kuliah nyeri kepala
DESCRIPTION
koas saraf sw, saraf sw, koas untar, nyeri kepala,TRANSCRIPT
Nyeri kepalaYang dimaksudkan di sini adalah rasa sakit / nyeri pada satu area atau lebih di kepala, muka, mulut, leher. Nyeri kepala bisa kronik, rekuren atau jarang. Nyeri bisa ringan atau cukup berat yang mengganggu aktifitas sehari-hari. Pada semua kasus, nyeri kepala menyangkut keterlibatan serabut saraf di jaringan, otot, dan pembuluh darah yang terletak di kepala dan dasar tengkorak.
Disini, nyeri kepala harus dibedakan dengan pusing (vertigo) dan perasaan melayang atau nggliyer (dizziness atau light headness). Dua hal terakhir tadi sifat dan latar belakangnya memang berlainan.
Bangunan peka nyeri
Bangunan peka nyeri di kepala apabila terstimulasi akan menimbulkan perasaan nyeri. Bangunan ini dapat dibedakan menjadi bangunan intrakranial dan ekstrakranial. Bangunan peka nyeri intrakranial meliputi sirkulus Willisi dan lanjutannya ke proksimal, arteri meninges, vena besar di otak dan dura, bagian duramater dekat pembuluh darah, nervi kraniales V, VII, IX,dan X, serta saraf spinal servikal bagian atas (C2,3). Sementara itu jaringan otak bukan merupakan bangunan peka nyeri.
Bangunan peka nyeri ekstrakranial meliputi Otot kepala dan leher, saraf kutaneus dan kulit kepala, mukosa sinus paranasalis dan hidung, mata dan orbita, telinga, gigi, saraf dan radiks serfikal, dan arteri karotis eksterna dan cabangnya.
Lokasi nyeri
Nyeri yang berasal dari bangunan intrakranial tidak dirasakan di dalam rongga tengkorak melainkan dirujuk ke bagian lainnya. Struktur supratentorial dipersarafi oleh N.V1 dan infratentorial oleh n.C2,3 sehingga lesi lobus oksipital direfer ke depan, Nyeri yang berasal dari duapertiga bagian depan kranium, di fosa kranium tengah dan depan, serta di atas tentorium serebeli dirasakan di daerah frontal, parietal dan temporal. dan lesi serebellum direfer ke belakang. Lagi pula bagian kaudal nukleus N V dari pertengahan pons sampai medulla spinalis segmen C3, juga menerima stimulus nyeri dari radiks serfikal atas selain dari N. Trigeminus. Nyeri ini disalurkan melalui cabang pertama nervus trigeminus.
Nyeri yang berasal dari bangunan di bawah tentorium serebeli di fosa posterior (misalnya di serebelum) biasanya diproyeksikan ke belakang telinga, di atas persendian serviko-oksipital atau di bagian atas kuduk. Nervi kraniales IX dan X dan saraf spinal C2, dan C3 berperan untuk perasaan di bagian infratentorial. Bangunan peka nyeri ini terlibat melalui berbagai cara yaitu oleh peradangan, traksi, kontraksi otot dan dilatasi pembuluh darah.Klasifikasi
Nyeri kepala primer mencakup 90 % kasus nyeri kepala, di mana tidak jelas kelainan sebagai penyebab yang mendasari.
Nyeri kepala sekunder didasari oleh suatu kelainan seperti penyakit serebrovaskuler, trauma kepala, infeksi, tumor, dan kelainan metabolik (mis., diabetes, penyakit tiroid ). Nyeri kepala juga bisa berasal dari sindrom yang mengenai mata, telinga, leher, gigi, atau sinus. Pada kasus-kasus seperti ini penyebabnya harus di cari dan diobati. Beberapa macam obat juga dapat menimbulkan sakit kepala sebagai efek samping.
Neri kepala sekunder yang berat, mendadak, dan mengganggu yang timbul setelah benturan di kepala, dan mengganggu aktifitas normal, atau disertai kelainan lain (mis., kejang, disorientasi, gangguan keseimbangan, hilang kesadaran, nyeri di mata atau telinga, demam) harus dievaluasi sesegera mungkin.
Nyeri kepala primer
1. Migren
Migren adalah nyeri kepala yang berdenyut yang sering unilateral dan disertai mual, muntah, sensitif terhadap cahaya, suara, bau-bauan; tidur terganggu; dan depresi. Serangan sering rekuren dan cenderung berkurang beratnya dengan bertambahnya usia.
1.1 Migren tanpa aura1.2 Migren dengan aura
1.2.1. Migren dengan aura tipik1.2.2. Nyeri Kepala non migren dengan aura tipik1.2.3. Migren dengan aura tipik tanpa sakit kepala1.2.4. Migren hemiplegi familial1.2.5. Migren hemiplegi sporadik1.2.6. Migren tipe Basiler
1.3. Sindrom periodik pada anak yang sering menjadi prekursor migren1.3.1. Muntah-muntah siklik
1.3.2. Migren abdominal 1.3.3. Vertigo paroksismal benigna pada anak
1.4. Migren retina1.5. Komplikasi migren
1.5.1. Migren kronik1.5.2. Status migren1.5.3. Aura persisten tanpa infark1.5.4. Migren infark1.5.5. Migren yang mencetuskan bangkitan
1.6. Probable migren1.6.1. Probable migren tanpa aura1.6.2. Probable migren dengan aura1.6.3. Probable migren kronik
2. Nyeri kepala tegang otot
Nyeri kepala tegang otot adalah bentuk yang paling sering dari nyeri kepala primer. Serangan biasanya mulai pada umur pertengahan dan sering disertai stres, kecemasan, dan depresi yang dapat timbul pada umur-umur tersebut.
2.1. Nyeri kepala tegang otot episodik yang jarang 2.1.1. Nyeri kepala tegang otot episodik dengan nyeri tekan perikranial 2.1.2. Nyeri kepala tegang otot episodik tanpa nyeri tekan perikranial 2.2. Nyeri kepala tegang otot episodik yang sering 2.2.1. Nyeri kepala tegang otot episodik dengan nyeri tekan perikranial 2.2.2. Nyeri kepala tegang otot episodik tanpa nyeri tekan perikranial 2.3. Nyeri kepala tegang otot kronik 2.3.1. Nyeri kepala tegang otot kronik dengan nyeri tekan perikranial 2.3.2. Nyeri kepala tegang otot kronik tanpa nyeri tekan perikranial 2.4. Probable tension type headache 2.4.1. Probable tension type headache episodik yang jarang 2.4.2. Probable tension type headache episodik yang sering 2.4.3. Probable tension type headache kronik
2. Nyeri kepala kelompok dan nyeri kepala trigeminal-otonom yang lain
Nyeri kepala kelompok berlangsung tiap hari selama masa berminggu-minggu bahkan kadang-kadang bulan. Serangan bisa menghilang kemudian muncul kembali pada musim yang sama pada tahun berikutnya.
3.1. Nyeri kepala kelompok 3.1.1. Nyeri kepala kelompok episodik 3.1.2. Nyeri kepala kelompok kronik 3.2. Hemikrania paroksismal 3.2.1. hemikrania paroksismal episodik 3.2.2. hemikrania paroksismal kronik 3.3. Nyeri kepala neuralgi unilateral singkat dengan injeksi konjungtifa dan lakrimasi 3.4. Probable sefalgia trigeminal otonomik 3.4.1. Probable nyeri kepala kelompok 3.4.2. Probable hemikrania paroksismal 3.4.3. Probable SUNCT
4. Nyeri kepala Primer lainnya 4.1. Nyeri kepala menusuk primer 4.2. Nyeri kepala akibat batuk primer 4.3. Nyeri kepala akibat olah raga primer 4.4. Nyeri kepala primer sehubungan aktifitas seksual 4.4.1. Nyeri kepala preorgasmik 4.3.2. Nyeri kepala orgasmik 4.4. Nyeri kepala hypnic 4.5. Nyeri kepala thunderclap primer

4.6. Hemikrania kontinua 4.7. Nyeri kepala harian persisten yang baru
Nyeri kepala sekunder
5. Nyeri kepala pada trauma 5.1. Nyeri kepala pasca trauma akut
5.1.1. Pada trauma kepala yang bermakna dan / atau gejala konfirmasi 5.1.2. Pada trauma kepala ringan dan / atau tanpa gejala konfirmasi
5.2. Nyeri kepala pasca trauma kronik 5.2.1. Pada trauma kepala yang bermakna dan / atau gejala konfirmasi
6. Sakit Kepala pada kelainan vaskuler 6.1. Penyakit serebrovaskuler iskemik akut 6.1.1. Serangan iskemik sepintas 6.1.2. Strok tromboemboli 6.2. Perdarahan intrakranial 6.2.1. Perdarahan intraserebral
6.2.2. Perdarahan subdural6.2.3. Perdarahan epidural
6.3. Perdarahan subarahnoid6.4. Malformasi vaskuler yang tidak ruptur 6.4.1. malformasi arterivena 6.4.2. aneurisma sakuler6.5. Arteritis 6.5.1. Arteritis sel raksasa (arteritis temporalis) 6.5.2. Arteritis sistemik lain 6.5.3. Arteritis intrakranial primer6.6. Nyeri arteri karotis atau vertebralis 6.6.1. Diseksi arteri karotis atau vertebralis
6.6.2. karotidinia (idopatik)6.6.3. Nyeri kepala pascaendarterektomi
6.7. Trombosis vena6.8. Hipertensi arteri
6.8.1. Efek peninggian tekanan darah akut terhadap bahan luar6.8.2. Feokromasitoma6.8.3. Hipertensi maligna6.8.4. Preeklamsi dan eklamsi
7. Nyeri kepala pada kelainan intrakranial nonvakuler7.1. Tekanan intrakranial yang tinggi
7.1.1. Peninggian tekanan intrakranial benigna7.1.2. hidrosefalus tekanan tinggi
7.2. Tekanan intrakranial yang rendah7.2.1. Nyeri kepala setelah pungsi lumbal7.2.2. Nyeri kepala pada fistula cairan serebrospinal
7.3. Infeksi intrakranial7.4. Sarkoidosis intrakranial dan penyakit inflamsi non-infeksi lainnya

7.5. Nyeri kepala sehubungan suntikan intratekal7.5.1. Efek langsung7.5.2. Karena meningitis kimia
7.6. Neoplasma intrakranial7.7. Nyeri kepala sehubungan kelainan intrakranial lain
8. Sakit kepala karena pemakaian bahan atau penghentiannya8.1. Nyeri kepala karena penggunaan bahan akut
8.1.1. Nyeri kepala akibat nitrat/nitrit8.1.2. Nyeri kepala akibat monosodium glutamat8.1.3. Nyeri kepala akibat CO8.1.4. Nyeri kepala akibat alkohol8.1.5. Nyeri kepala akibat bahan lain
8.2. Nyeri kepala akibat penggunaan bahan kronik8.2.1. Nyeri kepala akibat Ergotamin8.2.2. Nyeri kepala akibat analgetik8.2.3. Bahan lain
8.3. Nyeri kepala akibat penghentian bahan (penggunaan akut)8.3.1. Nyeri kepala akibat penghentian alkohol8.3.2. Bahan lain
8.4. Nyeri kepala akibat penghentian bahan (penggunaan kronik)8.4.1. Sakit kepala penghentian ergotamin8.4.2. Sakit kepala penghentian kofein8.4.3. Sakit kepala ketergantungan narkotik8.4.4. Bahan lain
8.5. Nyeri kepala karena bahan tetapi tanpa mekanisme jelas8.5.1. Pil antihamil atau estrogen8.5.2. bahan lain
9. Nyeri kepala pada infeksi di luar kepala9.1. Infeksi virus
9.1.1. Infeksi fokal9.1.2. Infeksi sistemik
9.2. Infeksi bakteri9.2.1. Infeksi fokal9.2.2. Infeksi sistemik
9.3. Sakit kepala pada infeksi lain
10. Nyeri kepala pada kelainan metabolik10.1. Hipoksia
10.1.1. Nyeri kepala pada ketinggian10.1.2. Nyeri kepala hipoksia10.1.3. Nyeri kepala apnu tidur
10.2. Hiperkapnia10.3. Campuran hipoksia dan hiperkapnia10.4. Hipoglikemi10.5. Dialisis10.6. Nyeri kepala pada kelainan metabolik lain
11. Nyeri kepala atau wajah pada kelainan kranium, leher, mata, telinga,

hidung, sinus, gigi, mulut, atau struktur wajah dan kepala yang lain11.1. Tulang kranium11.2. Leher
11.2.1. Vertebra serfikal11.2.2. Tendonitis retrofaringeal
11.3. Mata11.3.1. Glaukoma akut11.3.2. gangguan refraksi11.3.3.Heteroforia atau heterotropia
11.4. Telinga11.5.Hidung dan sinus
11.5.1. Nyeri kepala sinus akut11.5.2. Penyakit lain pada hidung dan sinus
11.6. Gigi, rahang, dan struktur yang berhubungan11.7. Penyakit pada sendi temporomandibular
12. Neuralgia kranial, nyeri trunkus saraf dan nyeri deaferensasi12.1.
Selanjutnya yang akan dibicarakan adalah nyeri kepala tegang otot, nyeri kepala kelompok, dan migren.
Nyeri kepala tegang otot dan kelompok
Insidens and Prevalensi
Di Amerika Serikat, lebih dari 45 juta orang —termasuk lebih dari 33 juta penderita asma, diabetes, dan sakit jantung —mengalami nyeri kepala kronik, rekuren. 28 juta dari padanya menderita migren setiap tahun.
Berkisar 75% to 90% dari semua orang yang mengeluh nyeri kepala kronik, atau sering, menderita nyeri kepala tegang otot. Nyeri kepala tegang otot lebih banyak pada wanita dari pria. Nyeri kepala kelompok utamanya pada pria berumur antara 20 dan 40 tahun.
Penyebab
Nyeri kepala tegang otot disebabkan oleh stres, ketegangan otot, dilatasi pembuluh darah, perubahan posisi, batuk atau bersin yang berlebihan, dan demam. Kondisi fisik dan mental yang dapat mengakibatkan ketegangan otot kronik dan sakit kepala :
kecemasan Artritis pada leher atau vertebra Penyakit degenerasi pada tulang atau diskus vertebra Depresi Gangguan sendi temporomandibular

Ada beberapa faktor pemicu yang diketahui menyertai nyeri kepala kelompok, termasuk obat-obatan yang menyebabkan dilatasi atau konstriksi pembuluh darah dan alkohol. Ini menimbulkan dugaan bahwa perubahan dalam dinding pembuluh darah di kepala mempunyai peranan sebagian.
Beberapa peneliti percaya bahwa kadar rendah endorphins dapat menyebabkan nyeri kepala yang sering, berat, atau kronik. Endorphins adalah bahan penghilang nyeri yang ditemukan di otak.
Symptoms
Nyeri kepala tegang otot Nyeri kepala tegang otot biasanya menimbulkan nyeri yang tumpul, menetap pada kedua sisi kepala. Nyeri biasanya meningkat dalam beberapa jam. Beberapa penderita nyeri kepala tegang otot mengatakan bahwa bila memburuk, nyeri berkembang dengan munculnya nyeri yang berdenyut.
Nyeri kepala tegang otot pernah diuraikan sebagai tekanan atau ikatan di sekeliling kepala, sepertinya tali yang ditarik kencang mengelilingi kepala atau kepala merasa dijepit.
Nyeri tekan pada otot didaerah leher, dasar tengkorak, kulit kepala, dahi, wajah, rahang, bahu, atau lengan atas bisa ditemukan pada penderita nyeri kepala tegang otot. Kulit kepala dan dahi mungkin terasa nyeri pada sentuhan. Beberapa orang nampak giginya terkatup.
Nyeri kepala kelompok Orang yang mengalami nyeri kepala kelompok bisa merasakan sampai 8 kali serangan sehari, setiap kali berlangsung 15- sampai 45 menit atau lebih lama. Serangan nyeri sering datang saat pagi-pagi buta dan membangunkan pasien dari tidur.
Nyeri pada nyeri kepala kelompok biasanya unilateral: terletak di sekitar satu mata dan hampir selalu pada satu sisi kepala. Bisa disertai hidung mampet dan mata berair.
Nyeri bisa terasa sangat hebat pada kebanyakan penderita, sering diuraikan seperti pisau atau paku ditusukkan ke dalam kepala. Berbaring bisa membuat nyeri kepala betambah parah. Beberapa orang mondar-mandir dan bergerak terus, tetapi tanpa perbaikan.
Diagnosis
Diagnosis nyeri kepala tegang otot dan kelompok didasarkan pada keluhan dan pemeriksaan medis yang menyeluruh pada pasien, seperti berikut:
Pemeriksaan mata Ciri-ciri nyeri kepala Kebiasaan tidur
Riwayat keluarga Riwayat medis Obat-obat yang diminum Pemeriksaan darah Pemeriksaan neurologis Pemeriksaan fungsi tiroid, hati , dan ginjal
Pemeriksaan Imaging otak mungkin dibutuhkan untuk menyingkirkan berbagai masalah medis serius yang mendasari, seperti tumor otak, strok, infeksi, and malformasi vaskuler (e.g., aneurisma).
Pemeriksaan imaging yang mungkin dilakukan :
EEG (electroencephalogram) untuk menilai aktifitas otak CAT (computer axial tomography) or MRI (magnetic resonance
imaging) scan untuk melihat jaringan dan struktur sekitar, pada , dan di dalam otak
Foto kepala, atau MRA (magnetic resonance angiography) untuk menilai pembuluh darah otak
Pemeriksaan laboratorium dan imaging dapat membantu menyingkirkan penyebab sekunder nyeri kepala, seperti berikut:
Tumor otak Aneurisma otak hipertensi infeksi (mis., meningitis, sinusitis, infeksi telinga) arteritis temporalis neuralgia trigeminus
Pengobatan
Nyeri kepala tegang otot Nyeri kepala tegang otot biasanya dapat diobati dengan baik dengan mengatur pola hidup dan penggunaan analgesik (mis., aspirin, ibuprofen, acetaminophen). Bila nyeri kepala berat atau sering, harus hati dengan penggunaan analgetik yang berlebihan, yang bisa menimbulkan nyeri kepala rebound.
Pada nyeri kepala rebound, kadar yang tinggi dari obat di dalam badan sebenarnya menyebabkan nyeri kepala. Pada kebanyakan kasus , nyeri kepala rebound membaik bila obat-obat di hentikan.
Nyeri kepala tegang otot yang tidak mempan obat penghilang nyeri dapat diberikan antidepresan atau obat mengurangi kecemasan, seperti amitriptylin, nortriptylin or desipramin.
Beberapa pasien nyeri kepala tegang otot merasakan membaik dengan pengobatan sekunder dengan mengurangi efek dari stres dan tegangan di badan, menggunakan pijat, meditasi dan biofeedback. Bila cocok,

psikoterapi dapat menolong beberapa pasien untuk belajar mengatasi lebih baik keadaan stres yang dapat menimbulkan sakit kepala.
Nyeri kepala kelompok Mengobati nyeri kepala kelompok terdiri atas mengurangi nyeri yang tak tertahankan, dan memutus atau memperpendek episode nyeri. Obat-obat untuk keadaan akut sama yang digunakan untuk migren:
sumatriptan (Iimitrex®)—suntikan atau sprai nasal. Triptan lain peroral juga bisa efektif.
DHE (Migranal®)—suntikan atau sprai nasal. Juga digunakan pada migren. Efek samping berupa mual dan dizziness.
100% oxygen—dihirup dari oksigen tangki. Diberikan bila obat-obat tidak memberikan perbaikan. Dapat digunakan di rumah.
Narkotik (e.g., codeine) —peroral. Tidak bekerja cukup cepat, mempersingkat nyeri kepala.
Prednison adalah kortikosteroid, merupakan bahan kimia yang poten yang dibentuk alamiah dalam badan. Diberikan dosis tinggi pada awalnya dan kemudian di tapering selama beberapa hari atau minggu, tergantung respons. Obat ini paling baik bila diberikan jangka pendek. Penggunaan jangka panjang dapat menimbulkan banyak efek samping serius sebab mempunyai banyak fungsi dalam badan. Efek samping potensial seperti peninggian tekanan intraokuler, osteoporosis, perubahan tingkah laku, ulkus, dan diabetes.
Lithium karbonat Lithium dapat meningkatkan kadar dopamin dan norepinefrin di otak. Diberikan peroral, biasanya 2 kali sehari, untuk memutus nyeri kepala kelompok. Konsentrasi lithium darah harus dimonitor ketat dengan pemeriksaan darah berulang. Efek samping seperti tremor, cepat haus, mual, dan sering kencing. Lithium karbonat khususnya digunakan untuk mengobati episode manik dari pasien manik depresi.
Verapamil melebarkan pembuluh darah. Bisa diminum 2 kali sehari. Efek samping berupa mual, dizziness, dan konstipasi. Verapamil khususnya untuk mengobati angina, hipertensi dan aritmia.
MIGREN
Migren adalah nyeri kepala yang berdenyut yang sering unilateral dan disertai mual, muntah, sensitif terhadap cahaya, suara, bau-bauan; tidur terganggu; dan depresi. Serangan sering rekuren dan cenderung berkurang beratnya dengan bertambahnya usia.
TipeKlasifikasi migren didasarkan pada keluhan yang timbul. Sudah diuraikan di atas.
Dua bentuk yang lazim adalah migren dengan aura dan migren tanpa aura yang akan diuraikan berikut.
Bentuk yang lebih jarang:
Migren basiler karotidinia migren tanpa sakit kepala migren oftalmoplegi status migren
Incidens and Prevalensi
Migren mengenai sekitar 24 juta orang di AS. Bisa pada setiap umur, tetapi biasanya mulai antara umur 10 dan 40 tahun dan berkurang setelah 50 tahun. Beberapa orang mengalamai beberapa kali serangan se bulan, sementara yang lainnya hanya mengalami beberapa kali seumur hidupnya. Berkisar 75% penderita migren adalah wanita.
Penyebab
Penyebab migren tidak diketahui. Kondisi ini bisa akibat dari satu rentetan reaksi dari SSP yang disebabkan oleh perubahan pada badan atau lingkungan. Sering ada riwayat keluarga menderita sakit tersebut, sehingga diduga penderita migren menerima warisan kepekaan terhadap pemicu yang menghasilkan inflamasi pada pembuluh darah dan saraf sekitar otak, menyebabkan nyeri.
Pemicu Pemicu adalah setiap stimulus yang memulai proses atau reaksi. Pemicu migren yang lazim dikenal :
Alkohol (mis., anggur merah) Faktor lingkungan (mis., cuaca, ketinggian, perubahan daerah waktu) Makanan yang mengandung kafein (mis., kopi, coklat), monosodium
glutamate (MSG; pada makanan Cina), dan nitrat (mis., makanan yang diproses, hot dogs)
Cahaya yang menyilaukan Perubahan hormon pada wanita Lapar Kurang tidur Obat-obatan (beli sendiri dan diresepkan) Parfum Stres
Gejala dan Keluhan

Nyeri migren sering diuraikan sebagai nyeri berdenyut yang bertambah dengan aktifitas rutin, batuk, mengedan, atau merendahkan kepala. Nyeri kepala sering begitu berat sehingga mengganggu aktifitas harian dan dapat membangunkan orang tersebut. Serangan nyeri membuat tidak berdaya, dan sering merasa lelah dan lemah terus begitu sakit kepala hilang.
Migren khasnya dimulai di satu area pada satu sisi kepala, kemudian meluas dan meningkat intensitasnya di atas 1 sampai 2 jam dan perlahan-lahan mereda. Bisa berakhir dalam 24 jam, dan pada beberapa kasus , beberapa hari.
Ada keluhan penyerta seperti mual, muntah, peka terhadap cahaya (fotofobia), atau peka terhadap suara (fonofobia). Tangan dan kaki dapat merasa dingin dan berkeringat dan bau yang tidak enak dapat tidak diterima.
Migren dengan aura ditandai oleh fenomena neurologis (aura) yang dirasakan 10 – 30 menit sebelum sakit kepala. Kebanyakan aura adalah visual dikatakan sebagai terang menyilaukan sekeliling benda atau pada bagian tepi lapangan pandang (disebut scintillating scotomas) atau garis-garis zigzag , bayangan berombak, atau halusinasi. Yang lain merasakan hilang penglihatan sementara.
Aura nonvisual seperti kelemahan motorik, kelainan bicara atau bahasa, dizziness, vertigo, and kesemutan atau baal (parestesia) wajah, lidah, or ekstremitas.
Migren tanpa aura adalah tipe yang paling sering dan bisa mengenai satu sisi kepala atau keduanya (bilateral). Kelelahan atau perubahan mood dapat dialami pada hari sebelum sakit kepala. Mual, muntah, peka cahaya (fotofobia) sering ada pada migren tanpa aura.
Migren arteri basiler menyebabkan gangguan pada arteri basiler di batang otak. Keluhan berupa nyeri kepala hebat, vertigo, penglihatan doubel, bicara pelo dan koordinasi otot yang terganggu. Bentuk ini terutama pada orang muda.
Karotidinia, juga disebut nyeri kepala separuh bawah atau migren wajah, menimbulkan nyeri dalam, tumpul, dan kadang-kadang nyeri menusuk di rahang atau leher. Biasanya ada nyeri tekan dan pembengkakan pada arteri karotis di leher. Episod bisa timbul beberapa kali seminggu dan berakhir beberap menit sampai beberapa jam. Tipe ini lebih lazim pada orang tua.
Migren tanpa nyeri kepala ditandai oleh adanya aura tanpa sakit kepala. Ini terjadi pada pasien dengan riwayat migren dengan aura.
Migren oftalmoplegia mulai dengan nyeri kepala di mata dan disertai muntah. Begitu nyeri kepala berjalan, kelopak mata jatuh (ptosis) dan saraf yang menggerakkan bola mata mengalami paralisis. Ptosis bisa menetap selama beberapa hari atau minggu.
Status migren adalah bentuk yang jarang dengan nyeri yang hebat yang biasanya berlangsung lebih dari 72 jam. Pasien mungkin membutuhkan perawatan.
Diagnosis
Diagnosis migren didasarkan riwayat keluhan, pemeriksaan fisik, dan pemeriksaan neurologis. Pemeriksaan dilakukan untuk menyingkirkan kelainan neurologis lain dan serebrovaskuler, seperti berikut:
Aneurisma serebri (pelebaran pembuluh darah di otak) Infark serebri (strok di otak) Trombosis sinus vena di otak (gumpalan darah dalam selaput yang
menutupi otak) hidrosefalus (kelebihan cairan otak) perdarahan intraserebral (perdarahan dalam tengkorak) cairan otak yang sedikit (CSF) Meningitis (peradagan selaput otak dan med.spinalis) blok sinus nasalis nyeri kepala pasca iktus (terjadi setelah strok atau bangkitan) Tumor
Pemeriksaan Computed axial tomography (CT scan) dilakukan untuk menyingkirkan kelainan otak yang mendasari bila migren masih baru atau bila ada perubahan ciri atau kekerapan. CT scan juga mencakup menyuntikkan kontras kemudian mengambil rentetan x-rays.
Electroencephalography (EEG) merekam signal listrik dalam otak menggunakan elektrode yang ditempatkan pada permukaan kulit kepala. Pemeriksaan ini untuk menemukan malfungsi aktifitas otak (mis., bangkitan).
Spinal tap (lumbar puncture) is dilakukan untuk menemukan infeksi dan menetapkan kadar sel darah putih, glukosa, dan protein dalam cairan otak. Pemeriksaan ini mencakup mengambil sejumlah kecil cairan dan memeriksa dibawah mikroskop.
Magnetic resonance imaging (MRI) scan and magnetic resonance angiography (MRA) dapat dilakukan untuk evaluasi lebih lengkap. MRI menghasilkan bayangan otak yang jelas yang memanfaatkan energi elektromagnetik. MRA menghasilkan bayangan pembuluh darah otak dan digunakan untuk menemukan aneurisma dan kelainan vaskuler lain.
Pengobatan
Perlu analisa riwayat migren pasien untuk memutuskan program pengobatan yang sesuai. Tujuan pengobatan adalah untuk mencegah atau mengurangi jumlah serangan migren (disebut pengobatan profilaksi) dan untuk

meredakan keluhan dan memperpendek lama migren (disebut pengobatan abortif.
Pengobatan profilaksi Obat-obat profilaksi (pencegahan) dapat diresepkan pada pasien dengan nyeri kepala yang sering (3 atau lebih sebulan) yang tidak mempan pengobatan abortif. Pertama dicoba satu obat (monoterapi), tetapi kombinasi obat-obat mungkin diperlukan. Banyak dari obat-obat ini mempunyai efek samping yang tidak diinginkan. Bila migren terkontrol, dosis obat dapat diturunkan atau dihentikan.
Beta blockers (e.g., propranolol [Inderal®], atenolol [Tenormin®]) adalah obat yang lebih disukai. Obat-obat ini mempengaruhi laju denyut jantung. Tidak boleh pada pasien asma dan harus digunakan dengan hati-hati pada pasien diabetes.
Efek samping terdiri atas gangguan gastrointestinal, insomnia, tekanan darah rendah (hipotensi), denyut jantung melambat (bradikardi), dan disfungsi seksual. Beberapa betablocker masuk ke dalam susu ibu dan dapat menyebabkan masalah pada bayi yang disusui.
Obat-obat antibangkitan seperti asam valproat (Depakote®), topiramat (Topomax®), and gabapentin (Neurontin®) mungkin efektif dalam pengobatan migren.
Efek samping meliputi mual, rasa tidak enak gastrointestinal, sedasi, kerusakan hati, dan tremor.
Calcium channel blockers (e.g., verapamil, amlodipine [Norvasc®]) menghambat dilatasi arteri dan meblok pelepasan serotonin. Tidak boleh diminum oleh pasien payah jantung atau blok jantung.
Efek samping mencakup konstipasi, muka merah (flushing), tekanan darah rendah, rash, dan mual.
Tricyclic antidepressants (TCAs; e.g., amitryptaline [Elavil®], nortryptaline [Pamelor®], desipramine [Norpramin®]) memblok reabsorbsi serotonin dan butuh minggu untuk efektif.
Efek samping meliputi:
konstipasi mulut kering hipotensi takhikardi retensi urine disfungsi seksual berat badan bertambah
Dosis tinggi TCA dapat menimbulkan bangkitan, strok, dan serangan jantung. Penghentian mendadak obat-obat ini dapat menyebabkan sakit kepala, mual, malaise,dan dapat memperberat efek samping.
Selective serotonin reuptake inhibitors (SSRIs; e.g., paroxetine [Paxil®], fluoxetine [Prozac®], sertraline [Zoloft®] biasanya lebih baik ditoleransi dari TCA, tetapi tidak seefektif TCA.
Efek samping mencakup mual, insomnia, disfungsi seksual,dan hilangnya nafsu makan.
Methysergide maleate (e.g., Deseril®, Sansert®) dapat diberikan pada pasien dengan migren yang sering, berat.
Efek samping terdiri atas insomnia, ngantuk, kepala ringan, dan rambut rontok. Obat tersebut tidak boleh pada pasien penyakit arteri koroner dan harus dihentikan selama 3-4 minggu setelah 3-4 bulan penggunaan sebab dapat menyebabkan fibrosis retroperitoneal, Keadaan di mana pembuluh darah di abdomen menebal, yang mengurangi aliran darah ke organ.
Pengobatan Abortif
Migren yang ringan dan jarang bisa membaik dengan obat-obat beli sendiri. Nyeri kepala berat disertai keluhan penyerta perlu diresepkan obat-obatan.
Selama migren, orang sering lebih suka beristitahat, atau tidur sendiri di ruang gelap, cukup tenang. Menempelkan bungkusan es di kepala atau menekan arteri yang menonjol di depan telinga pada sisi yang sakit dapat mengurangi sementara rasa sakit.
Analgesik (mis., aspirin, ibuprofen, acetaminofen) meredakan nyeri kepala sementara dan harus diminum saat gejala pertama migren. Obat-obat ini sangat efektif untuk migren yang jarang (kurang dari 3 perbulan) dan nyeri kepala yang tetap timbul dengan obat-obat profilaksi (breakthrough headaches.
Sering menggunakan analgesik (mis., lebih dari 4 kali seminggu) dapat menyebabkan nyeri kepala “rebound” dan dapat mengganggu pengobatan profilaski. Acetaminofen kadang dikombinasi dengan obat-obat lain untuk membuat bahan analgesik (mis., Midrin®).
Efek samping yang disebabkan oleh aspirin dan ibuprofen (mis., Advil®, Motrin®) adalah gangguan pencernaan dan perdarahan. Obat-obat ini harus diminum saat makan dan digunakan hati-hati. Ibuprofen tersedia dalam bentuk suppositoria, yang bisa berguna bila migren disertai mual dan muntah yang hebat.
Reseptor serotonin (mis, Imitrex®, Amerge®, Axert#&174) adalah obat yang bekerja cepat, biasanya ditoleransi dengan baik, lazim digunakan untuk

mengobati migren. Tersedia dalam bentuk oral, suntikan dan, dan bentuk semprotan hidung dan dapat digunakan setiap saat sakit kepala.
Efek samping adalah muka merah, perasaan tidak enak, kesemutan, dan mual.
Ergots (e.g., Cafergot®, Mioranal®) dapat digunakan oral atau suppositoria dan sering digunakan bersama obat anti mual, seperti prochlorperazine (Compazine®). Obat ini harus diminum saat gejala pertama migren muncul dan tidak efektif bila sakit kepala sudah berdenyut.
Efek samping adalah rasa tidak enak pencernaan, dizziness, strok, dan hipertensi. Ergots jangan diminum oleh pasien sakit jantung, vaskuler, hati, dan ginjal.
Pencegahan
Mencegah pemicu, menangani stres, dan minum obat profilaksi dapat mencegah migren. Dengan membuat catatan migren, dapat membantu mengetahui pemicu dan menilai efektifitas penanganan preventif. Pasien harus mencatat hal-hal berikut:
Aktifitas Faktor emosi (mis. Situasi stres) Faktor lingkungan (mis., cuaca, perubahan ketinggian) Makanan dan minuman Obat-obat (yang dibeli bebas dan diresepkan) Ciri-ciri migren (mis., beratnya, lamanya) Faktor fisik (mis., penyakit, kelelahan) Pola tidur
Tehnik penanganan stres (mis., biofeedback, hipnosis) dan aktifitas yang mengurangi stres (mis., meditasi, yoga, latihan) dapat membantu mencegah migren.
Tension-type headache
How to recognize this common condition
Loretta Mueller, DO
VOL 111 / NO 4 / APRIL 2002 / POSTGRADUATE MEDICINE
CME learning objectives
To review accurate diagnosis of tension-type headache To better understand the pathophysiology, precipitating factors, and societal
impact of tension-type headache
Preview:
Tension-type headache is the most prevalent headache type, affecting most women and men at some time in their lives, and can impair job productivity and interfere with family and social time. However, despite its impact, tension-type headache is also the most misunderstood headache type. Because of these misperceptions, many affected people are reluctant to seek medical treatment. In this article, Dr Mueller discusses possible triggers of tension-type headache, appropriate evaluation, and management with pharmacologic, nonpharmacologic, and alternative therapies.Mueller L. Tension-type, the forgotten headache: how to recognize this common but undertreated condition. Postgrad Med 2002;111(4):25-50
Up to 88% of women and 69% of men experience tension-type headache during their lifetime (1). The word "tension" implies that this type of headache can be attributed entirely to tension or stress, which may make people with this type of headache reluctant to consult a physician. Physician misperceptions that tension-type headaches are mild, benign, self-treatable conditions due solely to stress may further trivialize the problem. "Tension-type" is a headache classification developed in 1988 by the International Headache Society (IHS) (table 1). It refers to a condition characterized by bilateral mild to moderate pain and pressure that often is described as similar to that of having "a vise around the head." Some patients with tension-type headache may experience severe pain and marked disability.
Table 1. International Headache Society diagnostic criteria for tension-type headache Primary diagnosis1. Headache has at least two of the following characteristics: Bilateral pain Pressure Mild to moderate pain No increased pain with physical exertion2. And no more than one of the following: Sensitivity to light Sensitivity to sound3. And neither of the following*: Nausea Vomiting

4. And duration of 30 minutes to 7 days
Subdivision diagnosis1. Episodic (<15 days/mo) or chronic (>15 days/mo for >6 mo)2. Associated with or not associated with coexisting pericranial muscle tenderness**
*Chronic tension-type headache may include one of these symptoms.
**Diagnosed by manual palpation or electromyographic studies.
Adapted from Headache Classification Committee of the International Headache Society (2).
Tension-type headache usually is not associated with migrainelike symptoms, such as nausea, vomiting, increased pain with physical exertion, photophobia, and phonophobia. Stress may be one of many precipitating factors, but the underlying cause is unknown. Research advances into this nonvascular headache have not kept pace with exciting new migraine discoveries.
A central mechanism that is not unlike the mechanism of the serotonin abnormalities of migraine is one likely cause of tension-type headache, with muscular tenderness being either a contributing factor or an epiphenomenon. Physician and patient education directed at addressing the reduced quality of life and work productivity due to tension-type headache may stimulate further research and increase healthcare use by the 85% of people with tension-type headache who do not seek treatment (3).
Epidemiologic factors
Nearly 80% of the population will experience a tension-type headache at some time. An estimated 1-year prevalence of 86% in women and 63% in men means that it is more probable to have experienced a tension-type headache than not (1). Headache is one of the 10 chief complaints of patients seen in primary care practices, and 47% of headaches are tension-type (3). During childhood there is no male or female predominance for tension-type headache, but during adulthood it is more commonly experienced by women (female-male ratio, 5:4) (4). First onset of tension-type headache is before age 20 in 40% of affected persons, between ages 20 and 40 in 40%, and between ages 40 and 50 in 18% (3). Three percent of the general population (5% of women and 2% of men) experience chronic tension-type headache, defined as more than 180 headache days per year (1). Prevalence of chronic tension-type headache increases with age; the inverse is true for episodic tension-type headache.
Societal impact
Because of its high prevalence and wide spectrum of disability, tension-type headache has greater socioeconomic impact than any other headache type. About 820 annual workdays for every 1,000 persons are lost on account of tension-type headache (versus 270 days on account of migraine) (5). The reduced productivity of those who remain at work despite headache has an even greater impact. Overall, tension-type headaches have a negative effect on the emotional life of affected persons, resulting in marked reductions in quality of life and frequency of social and family activities. Despite this, less than 15% of people with tension-type headache seek medical attention (3). Proposed reasons for this disparity are lack of respect, empathy, and understanding by physicians; fear of not being taken seriously; trivialization of the disorder by media advertising and jokes; and the widespread misperception that the headaches have a purely psychological basis.
Diagnosis
There are no objective diagnostic markers for tension-type headache. An accurate diagnosis relies on comprehensive history taking, which is helpful in eliminating secondary, potentially life-threatening diagnoses (table 2). The principal feature of tension-type headache is mild to moderate pressure-type pain, usually on both sides of the head, often described as occurring in the frontal or occipital areas or as a band around the head. Associated symptoms may include fatigue, irritability, and difficulty concentrating, but migrainelike symptoms usually are absent. Tension-type headaches typically last 30 minutes to 1 week, but some people experience them daily.
Table 2. Differential diagnostic considerations in tension-type headache Primary diagnosisNonvascular: Tension-typeVascular: Migraine or cluster
Secondary (organic) diagnosisVascular disorders Subarachnoid hemorrhage Subdural hematoma Unruptured arteriovenous malformation or aneurysm Ischemic cerebrovascular disease Temporal arteritis Arterial hypertension Cerebral venous thrombosis
Nonvascular intracranial disorders Benign intracranial hypertension Intracranial hypotension after lumbar puncture Intracranial neoplasm Intracranial infection or meningitis

Substances that act as triggers Medications (eg, nitrates, over-the-counter drugs) Foods (eg, monosodium glutamate, alcohol) Exposures (eg, carbon monoxide) Rebound (eg, caffeine, analgesic, ergot)
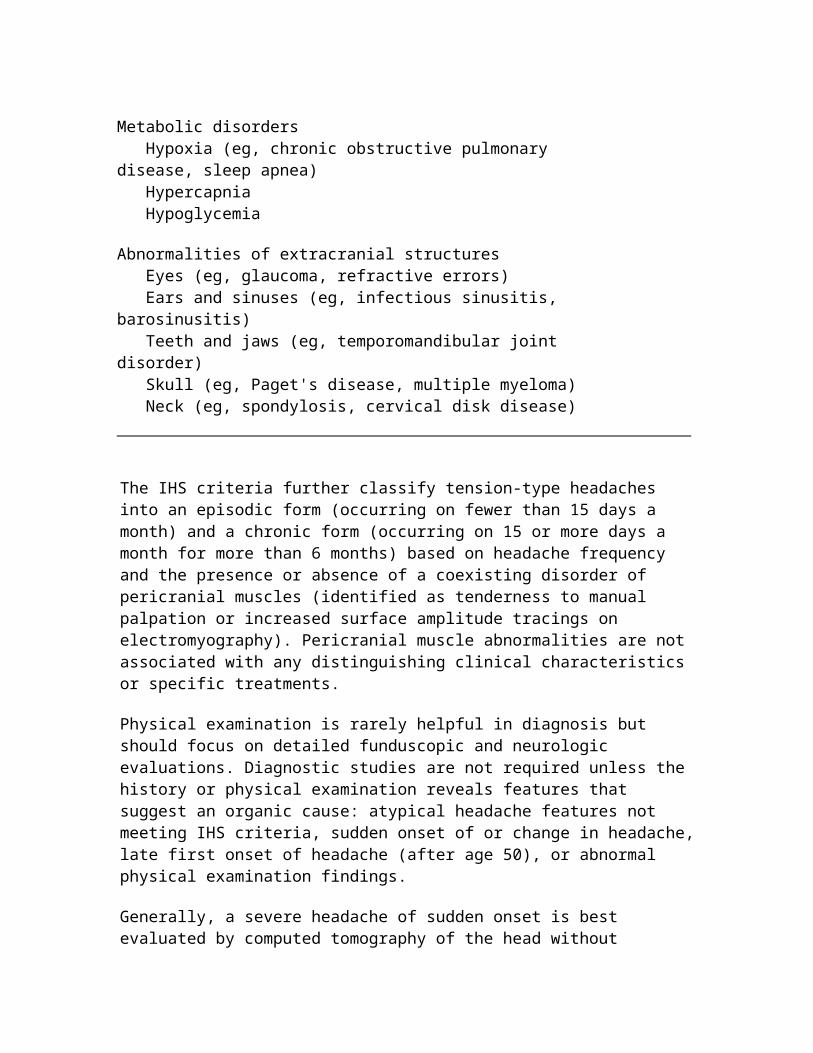
Metabolic disorders Hypoxia (eg, chronic obstructive pulmonary disease, sleep apnea) Hypercapnia Hypoglycemia
Abnormalities of extracranial structures Eyes (eg, glaucoma, refractive errors) Ears and sinuses (eg, infectious sinusitis, barosinusitis) Teeth and jaws (eg, temporomandibular joint disorder) Skull (eg, Paget's disease, multiple myeloma) Neck (eg, spondylosis, cervical disk disease)
The IHS criteria further classify tension-type headaches into an episodic form (occurring on fewer than 15 days a month) and a chronic form (occurring on 15 or more days a month for more than 6 months) based on headache frequency and the presence or absence of a coexisting disorder of pericranial muscles (identified as tenderness to manual palpation or increased surface amplitude tracings on electromyography). Pericranial muscle abnormalities are not associated with any distinguishing clinical characteristics or specific treatments.
Physical examination is rarely helpful in diagnosis but should focus on detailed funduscopic and neurologic evaluations. Diagnostic studies are not required unless the history or physical examination reveals features that suggest an organic cause: atypical headache features not meeting IHS criteria, sudden onset of or change in headache, late first onset of headache (after age 50), or abnormal physical examination findings.
Generally, a severe headache of sudden onset is best evaluated by computed tomography of the head without contrast and, possibly, lumbar puncture to rule out subarachnoid hemorrhage. Magnetic resonance imaging (MRI) of the brain is preferred for evaluating chronic progressive headaches because it has higher sensitivity for tumors, aneurysms, and posterior fossa lesions. Interestingly, nonspecific white matter abnormalities are an incidental finding on MRI scans in many patients with tension-type headache as well as in patients with migraine (32% and 34%, respectively, versus 7.4% in controls) (6). Laboratory studies may be indicated to identify suspected secondary causes of headache (eg, temporal arteritis, anemia, thyroid or metabolic abnormalities, Lyme disease) or to monitor for toxic effects from headache medication. Electrocardiography may be performed before prescribing of drugs that potentially alter conduction times (ie, tricyclic

antidepressants) or cause vasoconstriction. Standardized psychometric testing may identify comorbid psychiatric disorders, but these abnormalities may be the result of chronic headache pain.
Precipitating factors
Tension-type headache triggers are not always identifiable or consistent, and multiple triggers may have the additive effect of lowering the threshold of headache activation. In the past, studies have demonstrated few tension-type headache triggers other than emotional stress; more recent studies have found similar headache precipitants for both tension-type headache and migraine (table 3).
Table 3. Potential triggers of tension-type headache Stress (eg, everyday hassles, family crises, heavy workloads, unpleasant work or social situations)
Change in sleep regimen (eg, shift work, oversleeping)
Skipping meals
Certain foods (eg, caffeine, alcohol, cheese, chocolate)
Physical exertion
Environmental factors (eg, sun glare, odors, smoke, ambient noise, fluorescent lighting, sustained postures at video terminals or while driving)
Female hormonal changes (eg, menses, menopause, pregnancy, exogenous hormone use)
Medications used for concomitant medical conditions (eg, nitrates, selective serotonin reuptake inhibitors, antihypertensives)
Overuse of headache medication (eg, analgesic and caffeine combinations, butalbital compounds, opiates, ergot)
Information from Rasmussen (7).
Various medical conditions may exacerbate tension-type headache but rarely are an underlying cause. Tension-type headaches may be aggravated by barosinusitis from allergic or structural turbinate congestion or by functional disturbances of the masticatory
muscles around the temporomandibular joint from clenching, bruxism, or malocclusion. Head trauma--even a mild whiplash injury not associated with a blow to the head or loss of consciousness--may initiate or exacerbate tension-type headache, possibly on a chronic basis. That patients with first onset of tension-type headache after trauma have a genetic predisposition for the disorder is suspected but unproven (8).
Stress is undoubtedly the most common precipitant, triggering up to 80% of tension-type headaches. Emotions have biochemical effects in the body, and mental stress alone can elicit muscle contraction through the limbic system. Studies have demonstrated that, compared with control groups, patients with tension-type headache have similar major stressful life events but perceive more events as "hassles" and have less effective coping strategies (eg, avoidance, self-criticism, lack of use of social supports) (9). The increased prevalence of comorbid anxiety, depression, and somatoform disorders among people with tension-type headache is still debated. It is uncertain whether these disorders can initiate, contribute to, or maintain tension-type headaches; whether they are the result of a chronic pain condition; or whether they are due to a genetic susceptibility and serotonin abnormalities.
Pathophysiologic mechanisms
The cause of tension-type headache is unknown, but most research has focused on a peripheral mechanism pertaining to pericranial muscle tenderness, thus explaining the previous term "muscle contraction headache." Researchers who have attempted to find correlations between subjective complaints of pericranial muscle tension and electromyographic changes during a headache have had conflicting results. In fact, electromyographic readings indicating tenderness are usually greater in patients with migraine than in patients with tension-type headache during a headache (10). Sustained muscle contraction from physical or emotional causes may compress intramuscular arterioles, causing ischemia, accumulation of noxious metabolites, or both, which results in localized tenderness (9).
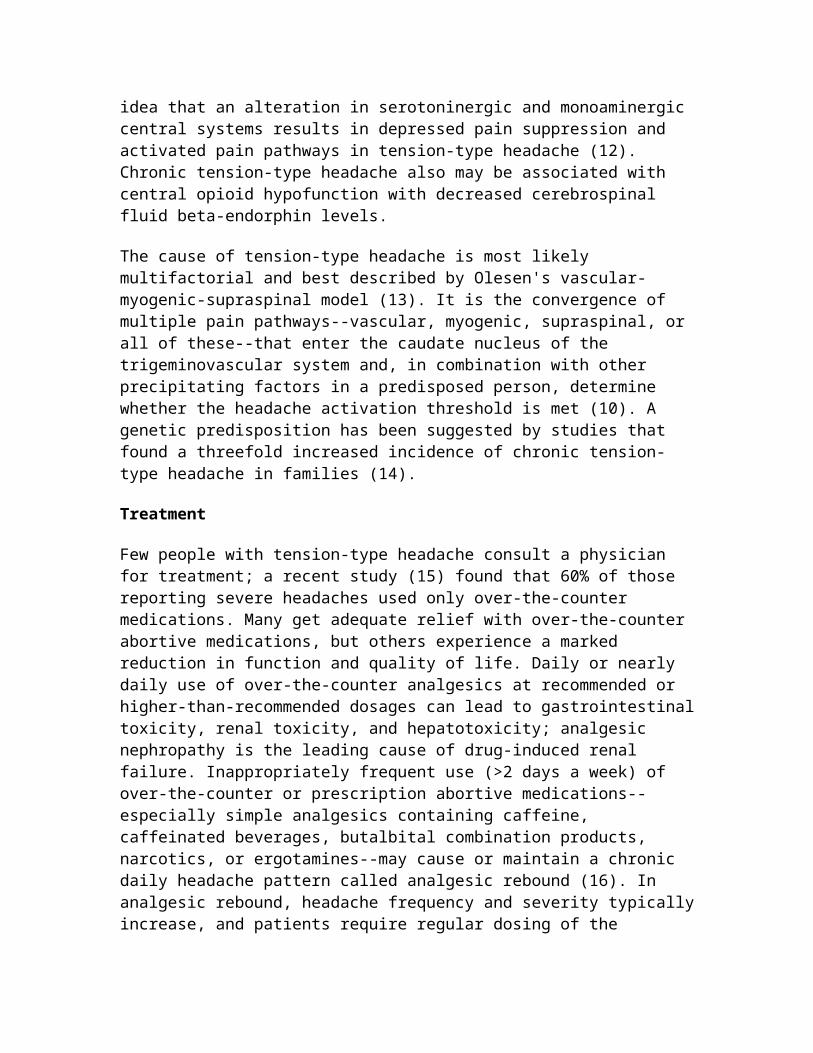
Another hypothesis, favored by physicians who believe migraine and tension-type headache are part of a continuum of the same underlying disorder, is that tension-type headache has a purely central mechanism and that muscle tension is an epiphenomenon (11). Studies that suggest a shared disorder with migraine have found reductions in platelet or serum serotonin, epinephrine, norepinephrine, and dopamine levels; these findings appear to support the idea that an alteration in serotoninergic and monoaminergic central systems results in depressed pain suppression and activated pain pathways in tension-type headache (12). Chronic tension-type headache also may be associated with central opioid hypofunction with decreased cerebrospinal fluid beta-endorphin levels.
The cause of tension-type headache is most likely multifactorial and best described by Olesen's vascular-myogenic-supraspinal model (13). It is the convergence of multiple pain pathways--vascular, myogenic, supraspinal, or all of these--that enter the caudate nucleus of the trigeminovascular system and, in combination with other precipitating
factors in a predisposed person, determine whether the headache activation threshold is met (10). A genetic predisposition has been suggested by studies that found a threefold increased incidence of chronic tension-type headache in families (14).
Treatment
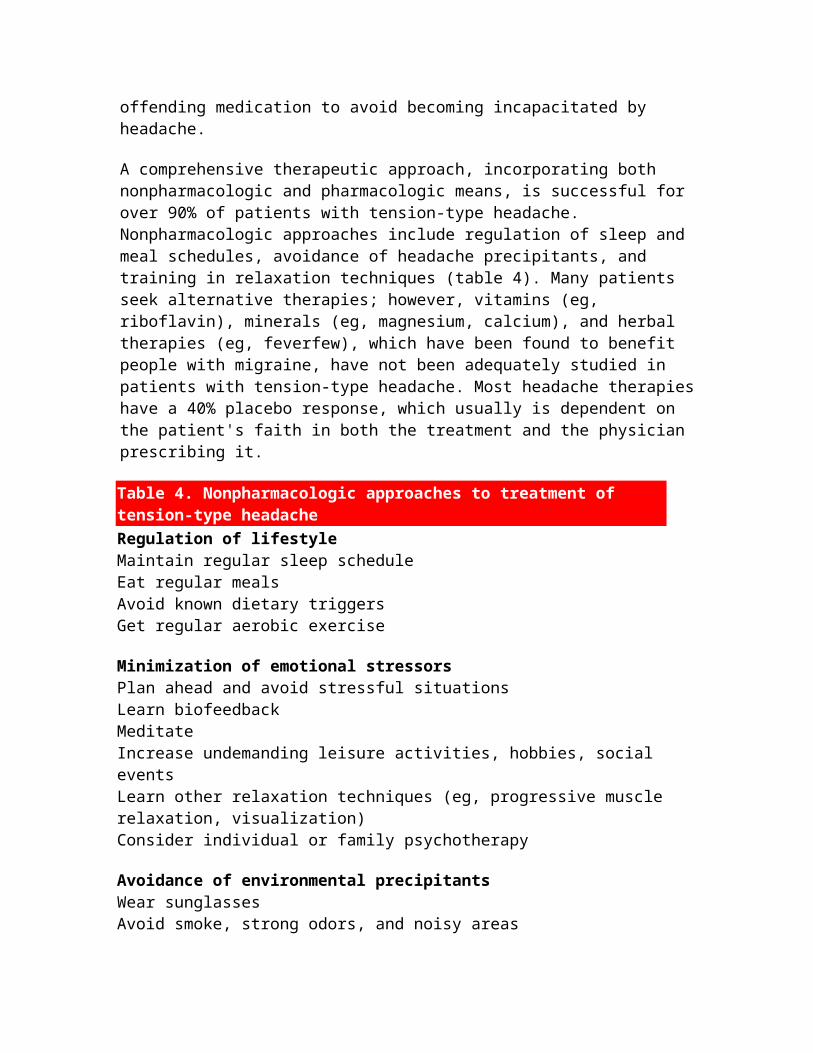
Few people with tension-type headache consult a physician for treatment; a recent study (15) found that 60% of those reporting severe headaches used only over-the-counter medications. Many get adequate relief with over-the-counter abortive medications, but others experience a marked reduction in function and quality of life. Daily or nearly daily use of over-the-counter analgesics at recommended or higher-than-recommended dosages can lead to gastrointestinal toxicity, renal toxicity, and hepatotoxicity; analgesic nephropathy is the leading cause of drug-induced renal failure. Inappropriately frequent use (>2 days a week) of over-the-counter or prescription abortive medications--especially simple analgesics containing caffeine, caffeinated beverages, butalbital combination products, narcotics, or ergotamines--may cause or maintain a chronic daily headache pattern called analgesic rebound (16). In analgesic rebound, headache frequency and severity typically increase, and patients require regular dosing of the offending medication to avoid becoming incapacitated by headache.
A comprehensive therapeutic approach, incorporating both nonpharmacologic and pharmacologic means, is successful for over 90% of patients with tension-type headache. Nonpharmacologic approaches include regulation of sleep and meal schedules, avoidance of headache precipitants, and training in relaxation techniques (table 4). Many patients seek alternative therapies; however, vitamins (eg, riboflavin), minerals (eg, magnesium, calcium), and herbal therapies (eg, feverfew), which have been found to benefit people with migraine, have not been adequately studied in patients with tension-type headache. Most headache therapies have a 40% placebo response, which usually is dependent on the patient's faith in both the treatment and the physician prescribing it.
Table 4. Nonpharmacologic approaches to treatment of tension-type headache Regulation of lifestyle Maintain regular sleep scheduleEat regular mealsAvoid known dietary triggersGet regular aerobic exercise
Minimization of emotional stressorsPlan ahead and avoid stressful situationsLearn biofeedbackMeditateIncrease undemanding leisure activities, hobbies, social eventsLearn other relaxation techniques (eg, progressive muscle relaxation, visualization)Consider individual or family psychotherapy
Avoidance of environmental precipitants
Wear sunglassesAvoid smoke, strong odors, and noisy areasMaintain proper posture; limit sustained positions
Physical therapy techniquesHeat, ice, ultrasound, transcutaneous electrical nerve stimulationMassage or cervical tractionStretching and strengthening exercises for cervical musculatureTrigger point stretching, compression, injection (any or all)
Osteopathic or chiropractic manipulation
Alternative therapiesAcupunctureAcupressure Therapeutic touchAromatherapy (eg, peppermint, green apple)Topical salves (eg, salicylic acid, piroxicam [Feldene], ketoprofen [Orudis, Oruvail])
Education and headache support groupsNational Headache Foundation (888-643-5552, www.headaches.org)American Council for Headache Education (800-255-ACHE, www.achenet.org)
Psychological stressors or comorbidities should be addressed for the best possible therapeutic outcome. A physician cannot change a patient's life circumstance but may be able to alter a patient's perspective about life events and the amount of stress they cause. Family or individual psychotherapy, or both, may help patients to modify perfectionistic standards, environmental demands, and maladaptive coping mechanisms; express their anger and emotions effectively; and develop a less critical self-perception. In some cases, family members should be involved in treatment to identify and address family behaviors that may unconsciously reinforce secondary gains and enabling behaviors in the patient. Generally, families should deemphasize concerns regarding headaches and encourage the patient to maintain as normal a lifestyle as possible.
If pharmacologic agents are indicated, abortive medications to relieve headaches may be used alone for infrequent headaches (occurring on 1 or 2 days a week) or in addition to a daily prophylactic medication for more frequent or severe headaches. Prophylaxis should be considered if significant disability occurs with attacks, if abortive medication cannot be used because of comorbid conditions or a history of substance abuse, or if preventive medication enhances the abortive medication effect. The mainstays of abortive therapy are analgesics and muscle relaxants (table 5). Simple over-the-counter analgesics and non-steroidal antiinflammatory drugs (NSAIDs) have been found to be effective in clinical trials. Little scientific evidence is available to support the effectiveness of muscle
relaxants. Butalbital analgesic combinations with or without codeine have been found to provide effective pain relief for tension-type headache (17); the barbiturate compound helps relieve the anxiety component of pain. Caffeine, used as an analgesic adjuvant in over-the-counter and prescription barbiturate combinations, increases the absorption, peak concentration, and analgesic potency of medication as much as 40%. The mild central nervous system stimulant effect of caffeine counteracts the sedative effects of barbiturates or opioids. A combination of isometheptene, dichloralphenazone, and acetaminophen also is indicated for tension-type headache. Interestingly, sumatriptan succinate (Imitrex), which typically is used for migraine, has been found to be effective in subgroups of patients with tension-type headache who experience frequent vascular headache qualities (ie, throbbing, increased pain with exertion, photophobia, and phonophobia) (18). Sumatriptan has not been found to be effective in patients with tension-type headache who do not report these vascular qualities.
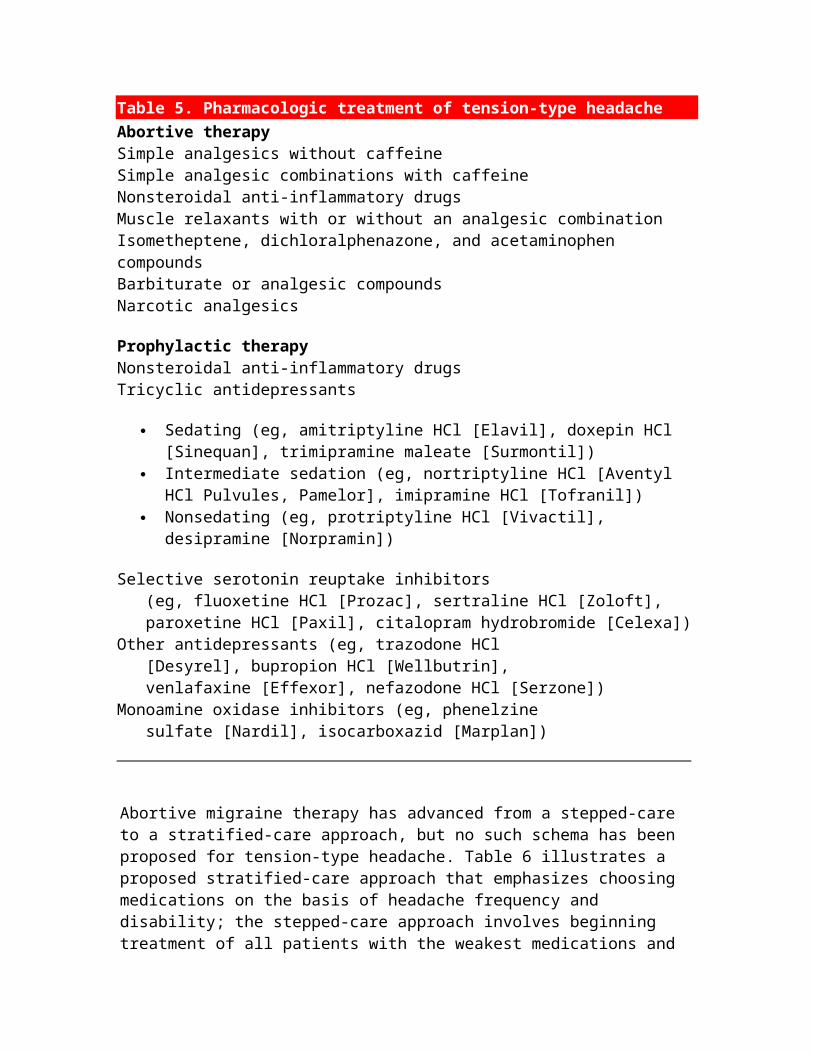
Table 5. Pharmacologic treatment of tension-type headache Abortive therapySimple analgesics without caffeineSimple analgesic combinations with caffeineNonsteroidal anti-inflammatory drugsMuscle relaxants with or without an analgesic combinationIsometheptene, dichloralphenazone, and acetaminophen compoundsBarbiturate or analgesic compoundsNarcotic analgesics
Prophylactic therapyNonsteroidal anti-inflammatory drugsTricyclic antidepressants
Sedating (eg, amitriptyline HCl [Elavil], doxepin HCl [Sinequan], trimipramine maleate [Surmontil])
Intermediate sedation (eg, nortriptyline HCl [Aventyl HCl Pulvules, Pamelor], imipramine HCl [Tofranil])
Nonsedating (eg, protriptyline HCl [Vivactil], desipramine [Norpramin])
Selective serotonin reuptake inhibitors (eg, fluoxetine HCl [Prozac], sertraline HCl [Zoloft], paroxetine HCl [Paxil], citalopram hydrobromide [Celexa])Other antidepressants (eg, trazodone HCl [Desyrel], bupropion HCl [Wellbutrin], venlafaxine [Effexor], nefazodone HCl [Serzone])Monoamine oxidase inhibitors (eg, phenelzine sulfate [Nardil], isocarboxazid [Marplan])

Abortive migraine therapy has advanced from a stepped-care to a stratified-care approach, but no such schema has been proposed for tension-type headache. Table 6 illustrates a proposed stratified-care approach that emphasizes choosing medications on the basis of headache frequency and disability; the stepped-care approach involves beginning treatment of all patients with the weakest medications and slowly advancing to stronger medications on the basis of response. In a stratified-care model, more effective medications, such as barbiturate or opioid combination analgesics, or both, may be considered first-line therapy for patients experiencing more disabling headaches; this is true as long as the headaches are not frequent (<2 days a week) and the patient is at low risk for habituation and has no history of substance abuse.
Table 6. Stratified-care approach to tension-type headache management based on frequency and degree of disability* InfrequentLow disability Nonpharmacologic approaches only Over-the-counter simple analgesics with or without caffeine (eg, Excedrin, Tylenol) Nonsteroidal anti-inflammatory drugs (eg, Anaprox, Motrin) No prophylaxis
High disability Narcotic analgesics (eg, Fioricet With Codeine Capsules, Vicodan) Nonsteroidal anti-inflammatory drugs with or without analgesic adjuvant (Anaprox, Motrin) Muscle relaxants Barbiturate and analgesic compounds Isometheptene compound Anxiolytics Consider prophylaxis
FrequentLow disability Nonpharmacologic approaches only Over-the-counter simple analgesics without caffeine Nonsteroidal anti-inflammatory drugs Consider prophylaxis
High disability** Muscle relaxants Nonsteroidal anti-inflammatory drugs Isometheptene compounds Prophylaxis indicated
*Headache frequency: infrequent, <2 days per week; frequent, >2 days per week. Low

disability means no to moderate impairment in function. High disability means moderate to severe impairment.
**High potential for analgesic overuse; avoid caffeine products, barbiturate compounds, anxiolytics, and narcotic analgesics.
Tricyclic antidepressants are the mainstay of prophylactic therapy for tension-type head-ache (19). Selection of a tricyclic antidepressant is usually based on the presence of sleep disturbances, with poor sleepers receiving the more sedating drugs. The average maintenance dose of most tricyclic antidepressants is 50 to 75 mg daily (except protriptyline hydrochloride [Vivactil], which is dosed differently). Effective dosage varies among patients and is unrelated to serum drug levels or antidepressant properties.
Despite their improved side effect profile, selective serotonin reuptake inhibitor antidepressants are less reliable for headache prophylaxis. Atypical antidepressant classes have potential but unproven benefits. Cyclobenzaprine hydrochloride (Flexeril), a muscle relaxant, has a chemical structure similar to that of the tricyclic antidepressants and has been found to be an effective prophylactic agent for tension-type headache but is not approved for long-term use (20). NSAIDs also may be used prophylactically.
Some physicians who feel strongly that migraine and tension-type headache are common entities propose that all migraine prophylactics are also effective for tension-type headache; however, few controlled studies of beta blockers, calcium channel blockers, or anticonvulsants used for tension-type headache are available. Botulinum toxin type A (Botox) has been studied as a potential headache treatment when injected into the frontalis muscle, but further studies are needed to identify the group of patients who are best suited for this treatment (21).
Efforts to foster a collaborative relationship with patients, making them active participants in their care, are likely to achieve higher treatment success rates. Patients should be educated about realistic treatment expectations. The physician should explain that a 4- to 8-week drug trial at full therapeutic doses may be required because of delayed effectiveness, that combinations of medications may be required, and that overuse of caffeine or analgesics negates treatment effect.
Preventive medications are not a cure; successful therapy is considered to be a 50% reduction in headache frequency, a reduction in headache intensity or duration, an enhancement of abortive medication effect, or all of these. Work around patient biases against certain drug classes or their potential for side effects (eg, weight gain, fatigue) while maintaining safety and efficacy.
Treatment is a balance between medication efficacy and adverse effects. Headache is a dynamic condition, and routine follow-up is required to reassess the need for medication

adjustments and to reinforce nonpharmacologic regimens. When patients are doing well, reduction of dosages of preventive medications should be attempted. Exacerbation of headache occurs at times regardless of potential triggers or medical regimens. The art of headache treatment is knowing when to maintain therapy and reassure patients, when to make minor adjustments in medications, and when to change the entire treatment regimen.
Conclusion
Recent advances in the treatment and understanding of migraine have overshadowed concerns about tension-type headache, the most prevalent headache disorder. Because of its high prevalence and wide spectrum of disability, tension-type headache is the most important headache type in regard to reduction in work productivity, quality of life, and socioeconomic impact.
Future research endeavors will address the pathophysiology of tension-type headache, whether peripheral, central, psychological, or multifactorial. Well-controlled clinical trials are needed to clarify the best treatment approaches and determine whether standard migraine medications may be used for tension-type headache. Patient education and more aggressive treatment regimens would likely increase use of the healthcare system and decrease the large indirect economic cost attributable to this often inadequately treated disorder.
References1. Rasmussen BK, Jensen R, Schroll M, et al. Epidemiology of headache in a
general population: a prevalence study. J Clin Epidemiol 1991;44(11):1147-57 2. Headache Classification Committee of the International Headache Society.
Classification and diagnostic criteria for headache disorders, cranial neuralgias and facial pain. Cephalalgia 1988;8(Suppl 7):29-34
3. A study of headache in North American primary care: report from the Ambulatory Sentinel Practice Network. J R Coll Gen Pract 1987;37(302):400-3
4. Friedman AP, de Sola Pool N, von Storch TJ. Tension headache. JAMA 1953;151:174-7
5. Rasmussen BK, Jensen R, Olesen J. Impact of headache on sickness absence and utilisation of medical services: a Danish population study. J Epidemiol Community Health 1992;46(4):443-6
6. De Benedittis G, Lorenzetti A, Sina C, et al. Magnetic resonance imaging in migraine and tension-type headache. Headache 1995;35(5):264-8
7. Rasmussen BK. Migraine and tension-type headache in a general population: precipitating factors, female hormones, sleep pattern and relation to lifestyle. Pain 1993;53(1):65-72
8. Yamaguchi M. Incidence of headache and severity of head injury. Headache 1992;32(9):427-31
9. Glass DE. Tension headache and some psychiatric aspects of headache. Headache Q 1992;3(3):262-9
10. Jensen R. Pathophysiological mechanisms of tension-type headache. Cephalalgia 1999;19(6):602-21
11. Olesen J, Jensen R. Getting away from simple muscle contraction as a mechanism of tension-type headache. (Editorial) Pain 1991;46(2):123-4
12. Castillo J, Martinez F, Leira R, et al. Plasma monoamines in tension-type headache. Headache 1994;34(9):531-5
13. Olesen J. Clinical and pathophysiological observations in migraine and tension-type headache explained by integration of vascular, supraspinal and myofascial inputs. Pain 1991;46(2):125-32
14. Russell MB, Iselius L, Ostergaard S, et al. Inheritance of chronic tension-type headache investigated by complex segregation analyses. Hum Genet 1998;102(2):138-40
15. Lipton RB, Diamond S, Reed M, et al. Migraine diagnosis and treatment: results from the American Migraine Study II. Headache 2001;41(7):638-45
16. Diener HC, Dichgans J, Scholz E, et al. Analgesic-induced chronic daily headache: long-term results of withdrawal therapy. J Neurol 1989;236(1):9-14
17. Friedman AP, DiSerio FJ. Symptomatic treatment of chronically recurring tension headache. Clin Ther 1987;10(1):69-81
18. Cady RK, Gutterman D, Saiers JA, et al. Responsiveness of non-IHS migraine and tension-type headache to sumatriptan. Cephalalgia 1997;17(5):588-90
19. Diamond ML, Solomon GD. Tension-type headache. In: Diamond ML, Solomon GD, eds. Diamond and Dalessio's the practicing physician's approach to headache. 6th ed. Philadelphia: WB Saunders, 1999:125-36
20. Lance JW, Anthony M. Cyclobenzaprine in the treatment of chronic tension headache. Med J Aust 1972;2:1409-11
21. Wheeler AH. Botulism Toxin A, adjunctive therapy for refractory headaches associated with pericranial muscle tension. Headache 1998;38(6):468-71
A fresh look at migraine therapyNew treatments promise improved management
Seymour Diamond, MD
VOL 109 / NO 1 / JANUARY 2001 / POSTGRADUATE MEDICINE
CME learning objectives
To become familiar with the pathophysiology and clinical features of migraine To learn the common signs of various types of migraine To understand the various options available for acute and prophylactic therapy of
migraine
Dr Diamond discloses financial interests in or connection with the following pharmaceutical companies: Glaxo Wellcome, Wyeth-Ayerst, Bayer, Merck, AstraZeneca, Carnrick, Bristol-Myers Squibb, and Abbott.
This is the second of four articles on headache
This page is best viewed with a browser that supports tables.
Preview: About 26 million Americans, nearly 70% of them women, are challenged by persistent, sometimes incapacitating migraine headaches. Although treatment has improved dramatically during the last decade, migraine headaches continue to raise diagnostic dilemmas and management questions among primary care physicians. In this article, Dr Diamond discusses diagnosis, current management, and prophylactic measures that can offer hope to many patients.Diamond S. A fresh look at migraine therapy: new treatments promise improved management. Postgrad Med 2001;109(1):49-60
The malady known as migraine was identified thousands of years ago and is known throughout all civilizations on earth. The earliest recorded description of headache dates to Mesopotamia in 4000 BC. Aretaeus of Cappadocia (130 to 200 AD) devised the first true description of migraine as a distinct entity because of its unilateral occurrence, association with nausea, regular recurrence, and paroxysms of pain separated by pain-free intervals. Because the pain was unilateral, Aretaeus called this type of headache "heterocrania." We now use the word "hemicrania," which literally means "half a head." Aretaeus also recognized the differences between acute headache attacks that lasted for days (cephalalgia) and chronic headaches (cephalea).
Classification of headache
Many elaborate classifications of headache have been formulated, including the 1962 recommendations of the Ad Hoc Committee on Classification of Headache of the National Institutes of Health (1). The most recent effort was published in 1988 by the International Headache Society (2). These classifications are complex and lengthy and are used primarily for research purposes. Therefore, they are difficult to translate into clinical practice.
My colleague Donald J. Dalessio, MD, and I devised a practical classification of headache for clinical use (3). We classified headaches into three primary categories (table 1): vascular (migraine, cluster) headache, tension-type (muscle contraction) headache, and organic (traction, inflammatory) headache. We also subdivided migraine into three types: migraine with aura (classic), migraine without aura (common), and complicated migraine (hemiplegic, ophthalmoplegic, and basilar artery migraine).

Table 1. Classification of headache VascularMigraine With aura Without aura Complicated •Hemiplegic •Ophthalmoplegic •Basilar artery Cluster (histamine)Toxic vascularHypertensive
Tension-type (muscle contraction)Depressive equivalents and conversion reactionsChronic anxiety statesCervical osteoarthritisChronic myositis
OrganicMass lesions (tumors, edema, hematomas, cerebral hemorrhage)Diseases of eye, ear, nose, throat, and teethArteritis, phlebitisOcclusive vascular diseaseAtypical facial painTemporomandibular joint dysfunctionCranial neuralgias (facial, glossopharyngeal)
A large number of patients have coexisting migraine and tension-type headache, which we consider an overlapping category. This combination headache is sometimes called mixed headache syndrome, transformed migraine, or chronic daily headache. Patients who have these headaches usually can differentiate the severe headache that has migraine characteristics and occurs two to five times a month from the chronic daily headache that is less severe (4).
Pathophysiology
Although the pathophysiology of migraine has not been firmly established, we owe a great deal of our knowledge about migraine pathophysiology to Harold G. Wolff, MD. During the 1930s, Dr Wolff did extensive research on migraine, including performing a craniotomy on a patient who was having an acute migraine attack. He observed initial cerebral vasoconstriction, followed by extracranial and intracranial vasodilation (5). He also noted that sterile inflammation surrounded the affected vessel and secondary muscle contraction was present.

On the basis of this information, Dr Wolff formulated the vascular theory of migraine. He also noted that certain vasoactive substances found in the inflamed tissue around the blood vessels contained catecholamines, histamine, serotonin, peptides, prostaglandins, and the slow-reacting substance of anaphylaxis, which is an acidic lipid. Dr Wolff speculated that prolonged migraine attacks (lasting 24 to 48 hours) seemed to be related to sterile inflammation. As a result of Dr Wolff's findings, corticosteroids were used for treating prolonged migraine headaches.
The work of Sicuteri and associates (6) and Curran and colleagues (7) confirmed the role of serotonin and its metabolites during all phases of a migraine attack. These investigations demonstrated that serotonin-releasing agents can induce migrainelike attacks. The fact that many of the newer drugs used for management of acute migraine are serotonin receptor agonists further implicates serotonin as a key player in migraine pathogenesis.
Neurologic theories of migraine have also been proposed. Studies by Olesen and associates (8) suggested that migraine results from an abnormal firing of a brain neuron. Spreading depression, a part of the neurologic theory, could explain the prodrome or aura of migraine. Moskowitz (9) identified the trigeminal ganglion as a factor in inducing neurogenic dural inflammation and the subsequent vascular pattern of the migraine attack. Other, more recent investigations suggested that substance P (10), calcitonin (11), and nitric oxide (12) are all active in the dural inflammatory cascade that occurs with or causes the vascular changes.
Definition of migraine
Although several definitions of migraine have been formulated, we rely on the definition developed by the World Federation of Neurology (13). It defines migraine as "a familial disorder characterized by recurrent attacks of headache widely variable in intensity, frequency, and duration. Attacks are commonly unilateral and are usually associated with anorexia, nausea, and vomiting. In some cases, they are preceded by, or associated with, neurological and mood disturbances."
The definitive characteristic of migraine with aura is the occurrence of a neurologic symptom complex 5 to 30 minutes before the onset of an acute migraine attack. Complicated migraine is described as a migraine attack associated with focal neurologic symptoms that may persist after the headache disappears. Ophthalmoplegic, hemiplegic, and basilar artery migraine are considered forms of complicated migraine.
Among adults who have migraine, about 70% are women and, of those, about 70% report a relationship between acute migraine attacks and menstruation. Menstrual migraine attacks can occur immediately before, during, or after menses. However, some women may also have attacks at other times of the month. Many women report a decrease in or complete remission of migraine attacks after the first trimester of pregnancy.
Clinical features
Migraine is not a daily headache. Frequency varies from a few headaches each week to one or two episodes each year. Most often, attacks occur two to eight times a month. Average duration is 4 to 24 hours, although some patients complain of headache lasting several days (status migrainosus). The degree of severity varies from moderate to incapacitating.
Patients who have migraine headaches often describe them as throbbing or pulsating. Although migraine pain is usually unilateral, it can occur on both sides of the head. Pain often affects the frontal and temporal regions but may be localized behind the eye. Also, pain can radiate across the head and to other regions of the face and neck.
Because of its association with nausea, vomiting, photophobia, phonophobia, dizziness, tinnitus, and blurred vision, migraine is often depicted as a "sick" headache. Symptoms can influence the selection of abortive and pain-relieving medication, as well as the route of administration. Migraine headaches are often exacerbated by physical activity.
Although migraine can first occur in childhood or as late as age 50, it usually starts during adolescence or young adulthood. In childhood migraine, boys and girls are affected equally until puberty, when the predominance shifts to girls (60% to 70%). Up to 70% of migraineurs report a family history of similar headaches.
The warning phaseAs stated earlier, the two major types of migraine are differentiated by the presence of an aura (prodromata). The aura consists of focal neurologic symptoms localized to the cerebral cortex or brainstem that may initiate or accompany the headache phase. Symptoms develop gradually over 5 to 20 minutes and are attributed to initial vasoconstriction. The aura typically lasts less than an hour.
The symptoms of the aura usually include such visual phenomena as flashing lights, zigzag or jagged lines, blind spots, difficulty in focusing, and distorted perception. Sometimes visual images are out of focus or appear to be unusually large or small.
Another occasional warning symptom is difficulty in speech, such as inability to find the right word or use of wrong words. A complete inability to speak occurs on rare occasions. Some patients are not able to understand what has been said. Also, headache may be preceded by motor aphasia.
Some patients who have migraine attacks, with or without aura, also have vague premonitory symptoms that start from 12 to 36 hours before the actual headache occurs. The symptoms usually begin imperceptibly and develop slowly. Premonitory symptoms vary and may range from one extreme to the other (eg, from euphoria to withdrawal, hyperactivity to sluggishness, extreme hunger to anorexia, diarrhea to constipation, frequent urination to fluid retention).

Other premonitory symptoms include yawning and fatigue, difficulty focusing, changes in personality, slurred speech, impaired concentration, irritability, agitation, sensitivity to light or sound, stiff neck, general muscle weakness, sensitive skin, and thirst. Some people have a feeling of well-being, become unusually talkative, and notice a surge of energy. The person's face may be pale, and the eyes may appear dark, heavy, or sunken. Although the migraine victim is not aware of these warning signs, friends or relatives may notice them.
Variations in hormone levels trigger headaches in many women, and fatigue, oversleeping, or skipping a meal can bring on migraine in some people. Medications have also been implicated in migraine attacks, including such agents as nitroglycerin, reserpine, indomethacin (Indocin), oral contraceptives, and cyclic estrogen replacement drugs. Psychological factors, such as anxiety, depression, repressed hostility, anger, and fear, can play a role as well.
Treatment
Migraine treatment can be divided into four types: general measures, abortive therapy, pain relief measures, and prophylactic therapy. Status migrainosus may require that additional strategies be tried.
General measuresAn important step in migraine management is identifying and avoiding headache triggers. Because migraine patients are particularly sensitive to changes in routine, regular sleep and meal schedules should be maintained. Although stress cannot be avoided, training in coping strategies or stress management may be beneficial. Similarly, a significant number of migraine sufferers appear to be obsessive, compulsive, and rigid, although this hypothesis has been debated. They may create environments that present enormous challenges. For example, a working mother returns to school and also participates in a number of volunteer activities. In many cases, a migraine sufferer endures a stressful period but then has a severe headache once the stress is alleviated.
Certain activities often trigger acute migraine attacks, such as looking at bright lights or the sun or watching a flickering or out-of-focus television program or film. I recommend use of tinted glasses during times of exposure to bright light for my migraine patients. In addition, flying or being at high altitudes, where the oxygen tension and concentration are usually lower than normal, can precipitate migraine attacks. Acetazolamide (Dazamide, Diamox), a diuretic and carbonic anhydrase inhibitor, taken the day before and the day of flying, may help patients who have migraine related to altitude changes. Changes in barometric pressure have also been identified as a migraine trigger, and migraine patients may be especially sensitive to weather conditions.
Abortive therapyUntil the early 1990s, only a few drugs were available for the acute treatment of migraine. Many physicians started with over-the-counter analgesics or prescription nonnarcotic nonsteroidal anti-inflammatory drugs (NSAIDs), progressed through the

ergotamine drugs, and used narcotics as a last resort in patients who had acute migraine attacks. Many times, management involved a litany of trial and error before a suitable drug was found. With the introduction of the triptans, early intervention with these migraine-specific drugs may act to reverse the migraine cascade.
Since then, advances have been made in pharmacologic therapy for migraine. Nevertheless, management of the migraine patient still requires frequent office visits, open communication between physician and patient, and an understanding by both physician and patient of the intricacies of drug treatment and interactions. For example, the route of administration is important in obtaining relief because it impacts the speed of action. Although oral administration is the simplest, it may not be appropriate for many of the 70% of migraineurs who have associated nausea and vomiting. Parenteral administration offers the quickest action, but self-injection may not be the optimal choice for many patients. A trip to the physician's office or emergency department delays the relief so badly needed.
Triptans: Discovery of the 5-hydroxytryptamine1 (5-HT1) receptor agonists ("triptans") has brought about remarkable advances in the treatment of migraine (14). These drugs have demonstrated efficacy in aborting migraine attacks and have variable affinity for the 5-HT1A, 5-HT1B, 5-HT1D, and 5-HT1F receptors. Their antimigraine effect is exerted by way of a receptor-mediated neural pathway in both the central nervous system and the trigeminal nerve, at which point neurogenic inflammation is blocked.
Sumatriptan succinate (Imitrex), the first triptan to be approved for migraine abortive therapy in the early 1990s, originally was available only for subcutaneous injections. Now sumatriptan can be given by oral or intranasal routes, as well as by injection. It is usually well tolerated and causes only minor side effects (eg, flushing, tingling, neck or chest tightness or pain, nausea, throat discomfort). If the first dose of sumatriptan offers at least partial headache relief, a second dose can be given an hour later or anytime within the next 24 hours if the headache recurs. However, a 5-day hiatus should be maintained between days of use. Sumatriptan should not be used in patients with basilar or hemiplegic migraine, ischemic heart disease, or Prinzmetal's angina and cannot be used concomitantly with ergotamine preparations or monoamine oxidase inhibitors (MAOIs).
Several oral second-generation 5-HT1B/1D agonists have been developed in the past few years. In 1998, the US Food and Drug Administration (FDA) approved naratriptan (Amerge), rizatriptan benzoate (Maxalt, Maxalt-MLT), and zolmitriptan (Zomig) for migraine therapy. It should be noted that none of the triptans can be used concomitantly with ergotamine derivatives nor should they be used in patients with basilar or hemiplegic migraine, ischemic heart disease, or Prinzmetal's angina.
Naratriptan has a longer half-life than the other triptans and remains active in the blood vessels for up to 6 hours. It has a low incidence of side effects, the most common of which are nausea and vomiting. Naratriptan holds promise for management of menstrual migraine because it has a long half-life. In addition, it can be used with MAOIs.
Rizatriptan is absorbed rapidly, and its effects can be noted within 30 minutes of ingestion. It is well tolerated but can cause a few mild side effects (eg, bitter taste, dizziness, fatigue, sleepiness, nausea). Rizatriptan is the only triptan currently available in an orally disintegrating tablet, which offers patients a convenient alternative if they prefer not to take water with their migraine medication. The formulation quickly dissolves on the tongue and is absorbed through the gastrointestinal tract. It does not exacerbate the nausea often associated with an acute migraine attack.
Zolmitriptan is also absorbed quickly and alleviates migraine attacks faster than some of the other triptans. It appears to be effective in alleviating associated symptoms, including nausea and sensitivity to light and sound. Its side effects are similar to those with sumatriptan and include nausea, dizziness, prickling or tingling of the skin, drowsiness, warm or cold sensations, jaw pain, and tightness of the neck or throat.
Three new triptans (eletriptan [Relpax], almotriptan, frovatriptan) may be available in the near future.
Ergotamine derivatives: Ergotamine tartrate preparations are vasoconstrictors that have been used in migraine abortive therapy for more than 50 years. These agents are available for oral administration in combination with caffeine. Ergotamine is also available for sublingual administration, but in the United States, it is no longer available in the parenteral form. An adequate dose should be taken as early as possible in a migraine attack to achieve a maximum response.
To prevent ergotamine rebound headaches or ergotism, care should be taken to remain within the limits of the recommended dosage. Ergotamine derivatives should not be used in patients with cerebrovascular, cardiovascular, peripheral vascular, ischemic heart, renal, or hepatic diseases; sepsis; or severe hypertension. In addition, ergotamine preparations should be used cautiously in patients with peptic ulcer and recent infection and should not be used in pregnancy.
Dihydroergotamine mesylate (D.H.E. 45, Migranal) has also been used safely and effectively in the abortive therapy of migraine, and it has recently been "rediscovered" because of its action as a 5-HT1D receptor agonist. It also has a potent effect at a number of other biogenic amine receptor sites. Unlike ergotamine tartrate, dihydroergotamine is associated with a lower incidence of nausea and is more of a venoconstrictor than an arterial vasoconstrictor. It can also be used to help patients who are ergotamine-dependent withdraw from ergotamine use.
Dihydroergotamine is available for intramuscular, subcutaneous, and intravenous injection and as a nasal spray. It also has been successfully used in repeated intravenous doses in patients with intractable migraine; a dose of 0.5 mg given as an intravenous push over 2 to 3 minutes, in combination with 10 mg of the antiemetic/antivertigo drug metoclopramide, may be repeated every 8 hours for 3 days in these cases.
Because of its vasoconstrictive properties, dihydroergotamine is contraindicated in patients who have peripheral vascular disease, ischemic heart disease, Prinzmetal's angina, uncontrolled hypertension, hemiplegic or basilar migraine, impaired hepatic or renal function, or sepsis, as well as in pregnant women. It should not be used concomitantly with other 5-HT1 agonists or ergotamine preparations. Also, dihydroergotamine should not be given to patients who have risk factors for coronary heart disease (CAD) unless a cardiovascular evaluation provides satisfactory clinical evidence that a patient is reasonably free of CAD, ischemic myocardial disease, and other significant cardiovascular disorders.
For patients with risk factors predictive of CAD who have a satisfactory cardiovascular evaluation, the first dose of dihydroergotamine should be given in a physician's office. Because cardiac ischemia can occur in the absence of clinical symptoms, consideration should be given to obtaining an electrocardiogram after the first dose is given to a patient with known risk for CAD.
Isometheptene mucate: In patients who cannot tolerate ergotamine or in whom ergotamine derivatives are contraindicated, isometheptene may be an effective alternative. Like ergotamine, isometheptene has cerebral vasoconstrictive actions. It is available in a preparation that also contains acetaminophen and dichloralphenazone, a mild sedative.
Aspirin and NSAIDs: Aspirin and other of the NSAIDs (eg, ibuprofen, naproxen sodium) have been used successfully in migraine abortive therapy. NSAIDs stabilize proteins and inhibit formation of active prostaglandins. They also inhibit inflammation through their effects on chemotaxis, phagocytosis, lysosomal enzyme release, and kinin generation.
Phenothiazines: The phenothiazines chlorpromazine hydrochloride (Thorazine) and prochlorperazine (Compazine) have been used effectively in the emergency department setting for the abortive treatment of acute migraine. Efficacy of these drugs is attributed to their antinauseant and sedative effects. In addition, their dopaminergic and adrenergic actions may trigger specific mechanisms involved in aborting migraine.
Lidocaine: A recent report (15) has suggested that use of intranasal lidocaine is helpful for abortive treatment of acute migraine. A 50% reduction in headache was noted by 55% of patients who used lidocaine. However, relapse was common and occurred early after treatment. In selected patients, this treatment has demonstrated significant benefit.
Pain relief measuresAbortive therapy may not completely resolve a migraine attack, and analgesics may be needed to alleviate pain. Over-the-counter analgesics (eg, aspirin, acetaminophen, ibuprofen, naproxen sodium, ketoprofen) may be effective. However, overconsumption of these analgesics, particularly those containing caffeine, can produce serious side effects. Withdrawal from caffeine-containing drugs may trigger caffeine withdrawal
headache. Therefore, these drugs should be avoided in patients who have frequent migraine attacks.
The first over-the-counter agent approved by the FDA for relief of migraine pain was the combination of aspirin, acetaminophen, and caffeine (Excedrin Migraine). This combination agent is suggested for the acute treatment of mild to moderate headache without associated vomiting and disability. Recently, two other nonprescription preparations of ibuprofen (Advil Migraine, Motrin Migraine) have also received approval for the relief of migraine pain. In addition, a parenteral NSAID, ketorolac tromethamine (Toradol), offers analgesia that is nonnarcotic and nonhabituating, and it has a low side-effect profile. The drug is given intramuscularly in a 60-mg dose.
Among the other options for pain relief are use of narcotic analgesics, antiemetics, phenothiazines, and cold packs. Narcotic analgesics (eg, codeine, meperidine hydrochloride [Demerol HCl], methadone hydrochloride [Dolophine HCl, Methadose]), preferably administered parenterally, are effective for pain relief but are potentially habituating. As with other pain syndromes, these drugs should not be used in patients with frequent migraine attacks and should never be used for daily headaches.
Antiemetics and phenothiazines, given parenterally or rectally, may be indicated in some migraine patients. The phenothiazines (including promethazine hydrochloride [Anergan, Phenergan], chlorpromazine, and prochlorperazine) are also useful because of their sedative and antinauseant action. Some antiemetics, such as trimethobenzamide hydrochloride and metoclopramide, have little sedative effect. However, metoclopramide, a 5-HT3 receptor agonist, enhances absorption of oral medications and has been used effectively in combination with intravenous dihydroergotamine. This use of metoclopramide occasionally causes nervousness and tremor.
Transnasal butorphanol tartrate (Stadol NS) is a totally synthetic mixed agonist-antagonist opioid analgesic that originally was available for parenteral administration. Its quick absorption through the nose is enhanced by its lipophilic nature. The highly vascular character of the nasal mucosa speeds uptake and absorption. Caution must be exercised because of the possibility of habituation to butorphanol, and it should not be prescribed for patients who have daily headaches.
Cold packs have been used by migraine patients for many years. Application of ice bags or commercially manufactured ice packs to the site of the pain, along with gentle pressure, may reduce the pulsating pain associated with acute migraine attacks.
Prophylactic therapyProphylactic drug therapy should be considered in patients who have more than two acute migraine attacks per month. It may also be considered in patients who have attacks that seriously compromise daily activities or that last several days.
Beta blockers: For the past two decades, the beta blockers have been recognized for their efficacy in migraine prevention. Researchers have suggested that beta blockers without

intrinsic sympathomimetic activity are more beneficial than those possessing such activity. Propranolol hydrochloride (Betachron E-R, Inderal), timolol maleate (Blocadren), and nadolol (Corgard), all of which lack intrinsic sympathomimetic activity, are recognized as effective migraine prophylactic agents. Each of these drugs is considered nonselective and should not be used in patients with pulmonary disorders.
For patients with asthma and other respiratory disorders, treatment with a cardioselective beta blocker, such as metoprolol (Lopressor, Toprol XL), is indicated. Beta blockers are also contraindicated in patients with congestive heart failure and atrioventricular conduction disturbances. In addition, beta blockers should be used cautiously in patients who use insulin, oral hypoglycemics, or MAOIs.
Anticonvulsant drugs: Divalproex sodium (Depakote) has shown efficacy in migraine prophylaxis. It may be of particular use in migraineurs with concomitant convulsive disorders, because it has the potential for preventing seizures. Divalproex should be avoided in patients who have a history of hepatitis or abnormal liver function. Recently, an extended-release formulation that can be used once a day received FDA approval.
NSAIDs: The use of NSAIDs has become increasingly common for prophylactic management of migraine. Acceptance of NSAID therapy was accelerated by the results of a randomized study of more than 22,000 male physicians who used low-dose aspirin or placebo every other day (16). About 6% of those on active medication had migraine attacks, compared with 7.4% of the placebo group. Although this decrease in headache frequency (20%) was modest, the results suggest that NSAID therapy may be effective in migraine prevention. Several NSAIDs have demonstrated prophylactic efficacy in decreasing the frequency and severity of migraine.
Calcium channel blockers: Calcium channel blockers may be considered in migraine prophylaxis, particularly in patients refractory to beta blocker therapy. The rationale for using these agents stems from their effect on intracranial vasoconstriction. Nimodipine (Nimotop) appears to have marked selectivity for the cerebral vasculature, and verapamil hydrochloride (Calan, Isoptin, Verelan) has also demonstrated antiplatelet effects.
Alpha-adrenergic blockers: For patients who experience food-related migraine, clonidine hydrochloride (Catapres) has demonstrated efficacy. Clonidine, an alpha agonist, has also been observed as beneficial for patients undergoing opiate withdrawal.
Antidepressants: Antidepressants have shown continued efficacy in migraine prophylaxis for several decades. The tricyclic drugs, particularly amitriptyline hydrochloride (Elavil), are believed effective in headache prevention because of analgesic actions independent of their antidepressant effects. Use of antidepressants is preferred for the treatment of coexisting migraine and tension-type headaches. Antidepressant therapy also may prove helpful in patients refractory to other standard forms of treatment. In these patients, a trial of the MAOIs should be considered.

Antihistamine and serotonin blockers: Cyproheptadine hydrochloride (Periactin) is the agent of choice in childhood migraine because it blocks both histamine and serotonin receptors. Side effects include drowsiness and weight gain. Efficacy in adults is minimal.
Methysergide: A lysergic acid derivative, methysergide maleate (Sansert) is closely linked to ergotamine. In addition to its vasoconstrictor actions, methysergide also appears to block the inflammatory mechanisms of serotonin. Although it has shown efficacy in migraine prevention, it is not widely used because of its serious side effects with prolonged therapy. When it is used, patients should be evaluated at monthly intervals to rule out pulmonary, coronary, or retroperitoneal fibrosis, as well as peripheral vascular disease. If a patient has been maintained on methysergide for 6 consecutive months, a 4- to 6-week drug hiatus must be ordered and an intravenous urographic study should be performed to rule out retroperitoneal fibrosis.
Status migrainosusIn patients who have this disorder, migraine attacks are unrelenting and refractory to conventional therapy. For some migraine attacks that persist for more than 24 hours, the treatment of choice is adrenocorticosteroid therapy, such as dexamethasone or methylprednisolone in dose packs. Sterile inflammation is considered the cause of these prolonged migraine attacks.
When migraine persists, the associated symptoms (eg, nausea, vomiting) may pose a threat to the patient's well-being. Dehydration can become a problem, and hospitalization may be needed for intravenous fluid replacement and to monitor serum electrolytes. Intravenous dihydroergotamine (0.5 mg) given with metoclopramide (10 mg) every 8 hours for 2 days has demonstrated efficacy in treating status migrainosus. This therapy avoids use of habituating narcotic analgesics.
Summary
Successful management of migraine headaches involves identifying and avoiding headache triggers and using appropriate abortive therapy once a headache is recognized. Pain relief measures include over-the-counter analgesics, parenteral NSAID therapy when needed, and use of antiemetics and cold packs. Narcotic analgesics are best used only as a "last resort" measure.
Prophylactic therapy should be considered for patients who have more than two acute migraine attacks each month or whose daily activities are seriously compromised by headaches. For the patient in whom status migrainosus threatens well-being, hospitalization and more intensive therapy may be needed.
References1. Classification of headache. Ad Hoc Committee on Classification of Headache.
JAMA 1962;179(6):717-8
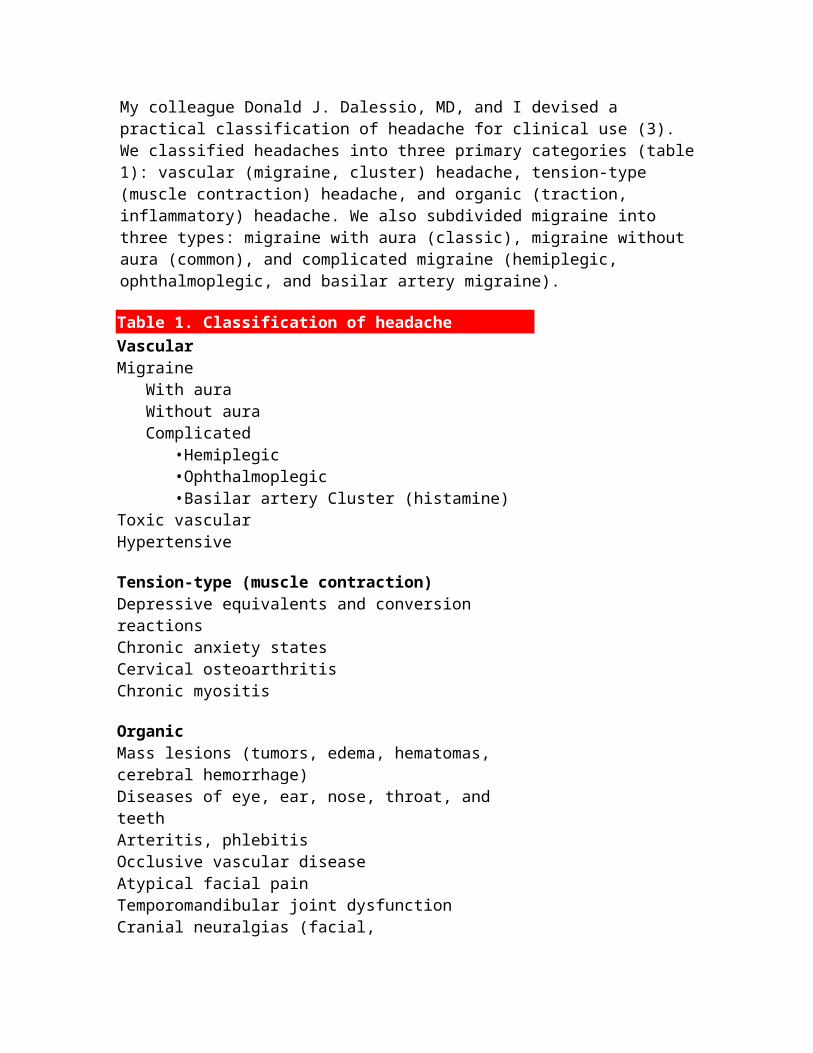
2. Classification and diagnostic criteria for headache disorders, cranial neuralgias and facial pain. Headache Classification Committee of the International Headache Society. Cephalalgia 1988;8(Suppl 7):1-96
3. Diamond S, Dalessio DJ. The practicing physician's approach to headache. New York: Medcom, 1973:2
4. Diamond S. Migraine headache. In: Diamond ML, Solomon GD, eds. Diamond and Dalessio's the practicing physician's approach to headache. 6th ed. Philadelphia: WB Saunders, 1999:46-70
5. Wolff HG. Headache and other head pain. 2d ed. New York: Oxford University Press, 1963
6. Sicuteri F, Testi A, Anselmi B. Biochemical investigations in headache: increase in hydroxyindoleacetic acid excretion during migraine attacks. Int Arch Allergy 1961;19:55-8
7. Curran DA, Hinterberger H, Lance JW. Total plasma serotonin, 5-hydroxyindoleacetic acid and p-hydroxy-m-methoxymandelic acid excretion in normal and migrainous subjects. Brain 1965;88(5):997-1010
8. Olesen J, Larsen B, Lauritzen M. Focal hyperemia followed by spreading oligemia and impaired activation of rCBF in classic migraine. Ann Neurol 1981;9(4):344-52
9. Moskowitz MA. The neurobiology of vascular head pain. Ann Neurol 1984;16(2):157-68
10. Goadsby PJ, Edvinsson L, Ekman R. Release of vasoactive peptides in the extracerebral circulation of humans and the cat during activation of the trigeminovascular system. Ann Neurol 1988;23(2):193-6
11. Goadsby PJ, Edvinsson L, Ekman R. Vasoactive peptide release in the extracerebral circulation of humans during migraine headache. Ann Neurol 1990;28(2):183-7
12. Buzzi MG, Moskowitz MA. The antimigraine drug, sumatriptan (GR43175), selectively blocks neurogenic plasma extravasation from blood vessels in dura mater. Br J Pharmacol 1990;99(1):202-6
13. Critchley M. Definition of migraine. In: Cochrane A, ed. Background to migraine: third migraine symposium. New York: Springer Verlag, 1970:181-2
14. Peroutka SJ. Developments in 5-hydroxytryptamine receptor pharmacology in migraine. Neurol Clin 1990;8(4):829-39
15. Maizels M, Scott B, Cohen W, et al. Intranasal lidocaine for treatment of migraine: a randomized, double-blind, controlled trial. JAMA 1996;276(4):319-21
16. Buring JE, Peto R, Hannekens CH. Low-dose aspirin for migraine prophylaxis. JAMA 1990;264(13):1711-3
Cluster headaches
Three enigmas surround cluster headaches:
Why do they begin? Why do they stop? Why do they start again?
No one has been able to explain the peculiar periodicity of cluster headaches, even though, as with all headache types, theories abound.
Goadsby (1) suggests that cluster headache should be termed neurovascular headache. He used a nitroglycerin spray to initiate typical cluster attacks in nine patients with chronic cluster headaches. The patients' brains were then studied by using positron emission tomography. He found that the cluster headaches affected three areas of the brain, two of which are associated with any painful stimulus. The area most activated by cluster headache was the ipsilateral hypothalamic gray matter. Because the hypothalamus can be associated with periodic illness of any sort, it could be postulated that an explanation for the intermittent nature of cluster headache is at hand.
Goadsby also noted that the vasodilation associated with cluster headache is a "secondary phenomenon," a result of activation of the trigeminal vascular system. It remains to be resolved whether this is correct or whether the vasodilation is primary and the other changes are secondary.
Clinical findingsCluster headaches are characterized by excruciating, sharp, penetrating pain that typically lasts 30 to 45 minutes (range, 10 minutes to 4 hours). They usually occur once or twice a day (but may occur up to 10 times per day) for 1 to 4 months. Most patients then experience a remission of months or years.
Cluster headaches and migraine have many similarities but also many differences. In contrast to migraine, cluster headaches are more prevalent in men, are not preceded by an aura, always occur unilaterally with pain recurring on the same side in subsequent headaches, and usually are not associated with a positive family history of cluster headache.
The headache often occurs during sleep (usually within 1 hour after falling asleep) and is severe enough to wake the patient. The mean age at onset is 27 to 30 years. Characteristically, cluster headache is associated with ipsilateral lacrimation, rhinorrhea, nasal congestion, and conjunctival injection. The pain is distributed unilaterally over the oculotemporal, oculofrontal, or temporal facial region. A partial Horner's syndrome with miosis and ptosis may occur on the ipsilateral side.
Short-term treatmentOxygen inhalation is effective and relatively safe for the symptomatic treatment of cluster headache (2). I generally prescribe it as first-line treatment. The mechanism of action is unknown but probably involves a marked reduction in cerebral blood flow that results in concomitant pain reduction. Patients should be told to begin therapy at the onset of an attack by administering 100% oxygen through a face mask at a rate of 7 to 8 L/min for 10

to 15 minutes. A nasal cannula should not be used because nasal congestion may impede inhalation. Patients should assume a sitting position, either upright or leaning forward, and should avoid hyperventilation, which may limit oxygen saturation.
Ergotamine preparations are more convenient than oxygen treatment, but the relatively slow onset of action of the oral products often limits their usefulness in cluster headache treatment (3). Sublingual ergotamine has a more rapid onset of action, which may render it useful for cluster headache treatment. A single dihydroergotamine meslyate (D.H.E. 45) injection may be useful in an emergency department or office setting.
Nonsteroidal anti-inflammatory drugs: Theoretically, many drugs used in the abortive or symptomatic treatment of migraine also should be effective in cluster headaches. However, because of the extremely brief nature of cluster headaches, most oral preparations do not provide relief. The nonsteroidal anti-inflammatory drug (NSAID) naproxen sodium given in a 550-mg dose at the onset of an attack may be of some use in these situations because of its relatively fast absorption. This drug's usefulness is limited, however, to those patients whose headaches last longer than 45 minutes. Because of NSAIDs' potential to cause serious gastrointestinal bleeding and ulcers, patients experiencing several attacks a day must carefully adhere to the manufacturer's recommendations for total daily dose.
Lidocaine nose drops: Some patients may feel relief with the local anesthetic lidocaine hydrochloride in the form of nose drops. Lidocaine 4% topical solution (Xylocaine) is available by prescription and may be dispensed in a dropper bottle (4). With the head tilted backward and turned toward the ipsilateral side, patients should instill 15 drops in the nostril on the affected side at the onset of headache. The dose may be repeated after 15 minutes, if needed.
Lidocaine may be used two times per headache, up to four times per day. To facilitate the administration of lidocaine, phenylephrine hydrochloride 0.5% nasal drops may be used to clear congested nasal passages. Side effects of lidocaine nasal drops may include nervousness and dizziness. Some patients allergic to lidocaine may show signs of hypersensitivity.
Triptans: The triptans, particularly sumatriptan succinate (Imitrex), are effective for short-term treatment of cluster headache (5). Generally, sumatriptan is used in patients who experience one or two cluster headaches each day.
Prophylactic treatmentBecause of both the limited usefulness of drugs for cluster headache pain and the intense nature of the pain, prophylactic treatment is essential. Cluster headaches that occur only during sleep may be treated with nightly administration of ergotamine. However, attacks that occur at various times of day or night may be prevented by routine use of methysergide maleate (Sansert), verapamil hydrochloride (Calan, Isoptin, Verelan), lithium, or prednisone, either alone or in combination (6-8). For example, I may prescribe a combination of prednisone (60 to 80 mg/day) and verapamil (240 mg/day) first (figure

1: not shown). I am careful to limit prednisone use to 7 to 14 days. It may be necessary to increase the verapamil dose or to continue the therapy through the cluster headache period.
If this combination fails, I usually try methysergide (2 mg three times daily), but again, I limit treatment to 1 to 2 months. Methysergide should not be given with other drugs except pain relievers such as hydrocodone bitartrate (Vicodin). If methysergide is ineffective, lithium or valproic acid (Depakene, Depakote), or both, can be used, often with verapamil. Treatment must be individualized if multiple drug failures occur.
Chronic cluster headache can be treated prophylactically with verapamil or lithium, or both. Valproic acid used alone or with verapamil often is effective. Occasionally, a patient responds to intranasal application of capsaicin five or six times per day. Occipital nerve blocks may relieve cluster attacks briefly, but I have found that subsequent injections become less effective. Patients with chronic cluster headache may become resistant to a previously successful prophylactic medication. These patients may require polypharmacy or, eventually, inpatient treatment.
For hospitalized patients with the rare intractable cluster headache, I use dihydroergotamine given intravenously every 8 hours. Some patients become headache-free during treatment, and remission is often sustained after discharge from the hospital. If hospitalization and all prophylactic efforts fail, neuroablative procedures may be considered. At this point, I sometimes refer patients to the Diamond Headache Clinic for histamine desensitization (9), a benign procedure that can produce striking results.
Surgical procedures include sphenopalatine ganglionectomy, radiofrequency thermocoagulation of the trigeminal ganglion, and section of the trigeminal nerve (10-12). However, the corneal anesthesia that results from these procedures puts the ipsilateral eye at risk. Use of glycerol injection into the trigeminal cistern to treat intractable cluster headache has resulted in significant pain relief and poses no risk to the cornea (10).