the role of fentanyl on balance analgesia
Upload: department-of-anesthesiology-faculty-medicine-hasanuddin-university
Post on 13-Jul-2015
216 views
TRANSCRIPT

The Role of Fentanyl in Balance Anethesia
Muh. Ramli Ahmad
Department of Anesthesiolgy, IC and Pain Management
Faculty of Medicine, Hasanuddin University
Makassar, Indonesia
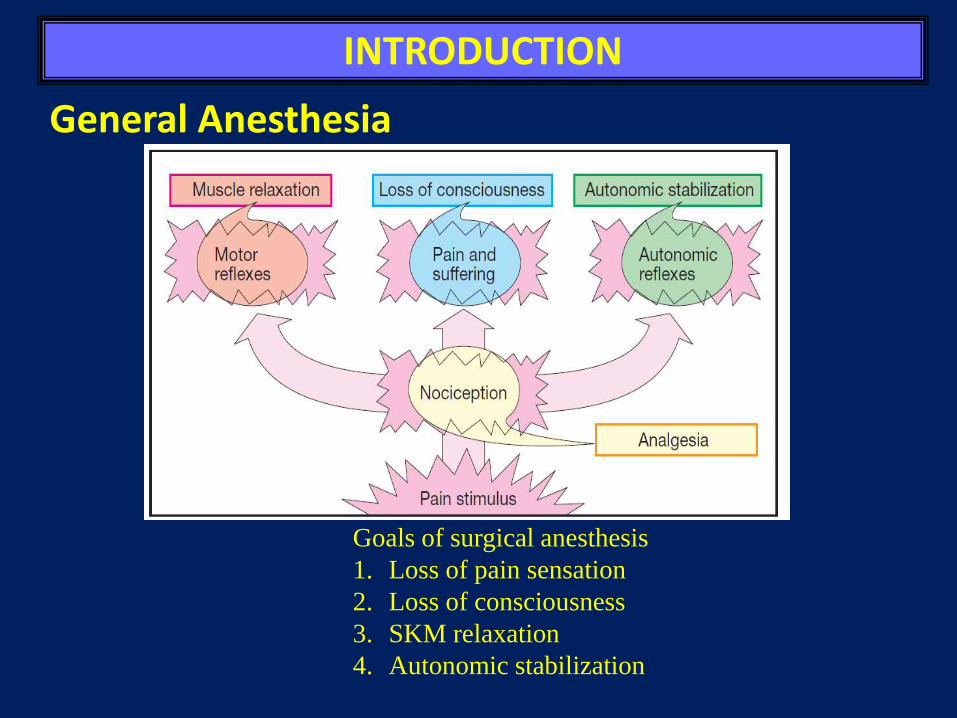
INTRODUCTION
Goals of surgical anesthesis
1. Loss of pain sensation
2. Loss of consciousness
3. SKM relaxation
4. Autonomic stabilization
General Anesthesia
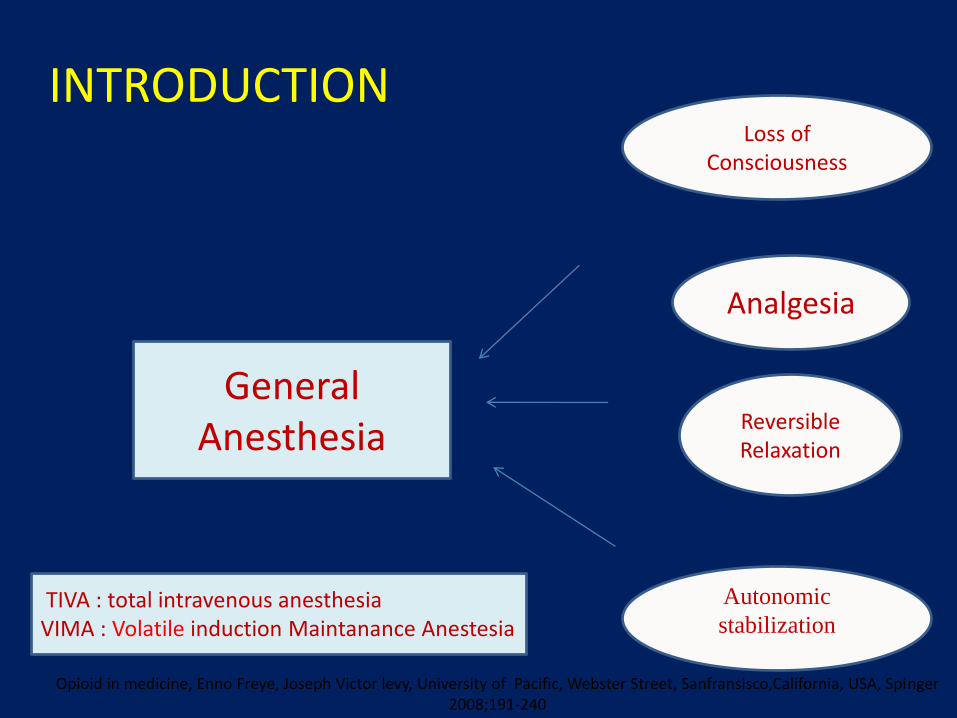
General Anesthesia
Loss of Consciousness
Analgesia
Reversible Relaxation
INTRODUCTION
Opioid in medicine, Enno Freye, Joseph Victor levy, University of Pacific, Webster Street, Sanfransisco,California, USA, Spinger 2008;191-240
Autonomic
stabilizationTIVA : total intravenous anesthesia
VIMA : Volatile induction Maintanance Anestesia

• Hypnosis (unconsciousness)
• Amnesia
• Analgesia
• Immobility/decreased muscle tone
– (relaxation of skeletal muscle)
• Inhibition of nociceptive reflexes MAC
• Reduction of certain autonomic reflexes
– (gag reflex, tachycardia, vasoconstriction) MAC-BAR ( blockade adrenergic response)
Goals of General Anesthesia

High dosage of Inhalation Anesthetic
Loss of Consciousness -Analgesia
Subcortical / Limbic System
Brain stem depression, Turmoil of Respiration and Hemodynamic ambiance
Opioid in medicine, Enno Freye, Joseph Victor levy, University of Pacific, Webster Street, Sanfransisco,California, USA, Spinger 2008;191-240
Traditional monoanesthesia

Inhalation Anesthetic Loss of consciousness + Analgesia
Fentanyl
Opioid in medicine, Enno Freye, Joseph Victor levy, University of Pacific, Webster Street, Sanfransisco,California, USA, Spinger 2008;191-240
Modern balanced anesthesia

• Furthermore in one study of 150 elective ASA I-III, surgical patients aged 65-92 years old showed that:
– Fentanyl reduced the rises in systolic, diastolic and mean arterial pressures, heart rate, and rate pressure product (P < 0.05)
– Fentanyl decreased the incidence of marked fluctuations in hemodynamic variables, often seen in geriatric patients (P < 0.05).
Opioid in Balanced Anesthesia
Splinter WM, Cervenko F. Haemodynamic responses to laryngoscopy and tracheal intubation in geriatric patients: effects of
fentanyl, lidocaine and thiopentone. CAN J ANAESTH 1989. 3 6; 4:3 7 0 – 6

Traditional monoanesthesia vs. modern
balanced anesthesia
Traditional monoanesthesia modern balanced anesthesia

FARMAKOEKONOMI
• Biaya opersional rumah sangat meningkatterutama kamar operasi
• Data biaya dikeluarkan RS 6% obatanestesi dari seluruh pembelian obat di RS Dari 6% 20% adalah obat inhalasi.
• Mulai dikembangkan Farmakoekonomi
FARMAKOEKONOMI
Farmakoekonomi adalah subdisiplin ilmu ekonomikesehatan yang membandingkan biaya danefektivitas suatu obat terhadap obat lain sertamelakukan analisis keduanya
Analisa ini untuk memberikan pelayanan kesehatanberdasarkan nilai yaitu mendapatkan hasil yang terbaik dengan biaya yang murah
Telah berkembang dinegara maju seperti Amerikaserikat, Jerman dan Australia

• Rapid induction
• Analgesia
• Inhibition of nociceptive reflexes
• Farmakoekonomi / cost effective
• Decrease the MAC
• Reduction of certain autonomic reflexes
– (gag reflex, tachycardia, vasoconstriction)
The Role of Fentanyl in Balance Anesthesia
The Potentiation of Anesthetic Agents with Fentanyl

Fentanyl
• Penggunaan paling sering dari fentanyl adalah sebagai agenanalgesik selama pemberian balanced anesthesia. Dosisfentanyl sebesar 0.5 – 2.5 mcg/kg dilakukan secara intermitendisesuaikan dengan intensitas pembedahan dan dapat diulangkurang lebih setiap 30 menit.
• Dosis alternatif, pemberian loading dose 5-10 mcg/kg daninfus kontinu fentanyl pada kecepatan antara 2-10 mcg/kg/jam dapat direkomendasikan.

Fentanyl
• Onset kerja fentanyl singkat, namun peak effect tercapai dalam waktu 5 menit.
• Pada praktek klinis secara umum, dosis fentanylyang digunakan sebelum dimulai induksi adalah1,5 sampai 5 mcg/kg.
• Titrasi fentanyl dilakukan sekitar 3 menit sebelumdilakukan laringoskopi karena efek puncaknyayang mengalami perlambatan sekitar 3-5 menituntuk mendapatkan efek yang maksimal.

Fentanyl Pharmacokinetics
• Intramuscular
Onset 7-15 minutes
Peak 15 minutes
Duration 1-2 hours
• Intravenous
Onset minutes
Peak minutes
Duration 30-60 minutes

Adverse Reactions:
MS: Muscle rigidity, particularly involving muscles of respiration.
CV: Bradydysrhythmias (common) or tachydysrhythmias, hypotension, orthostatic hypotension
Resp: Respiratory depression (common) or arrest.
CNS: Pupillary constriction. Sedation
GI: Nausea and Vomiting
Derm: Histamine release may cause local or general urticaria

Modern balanced anesthesia
Opioid in medicine, Enno Freye, Joseph Victor levy, University of Pacific, Webster Street, Sanfransisco,California, USA, Spinger 2008

The Potentiation of Anesthetic Agents with Fentanyl
Inhalation Agent Inhalation Agent + Opioid

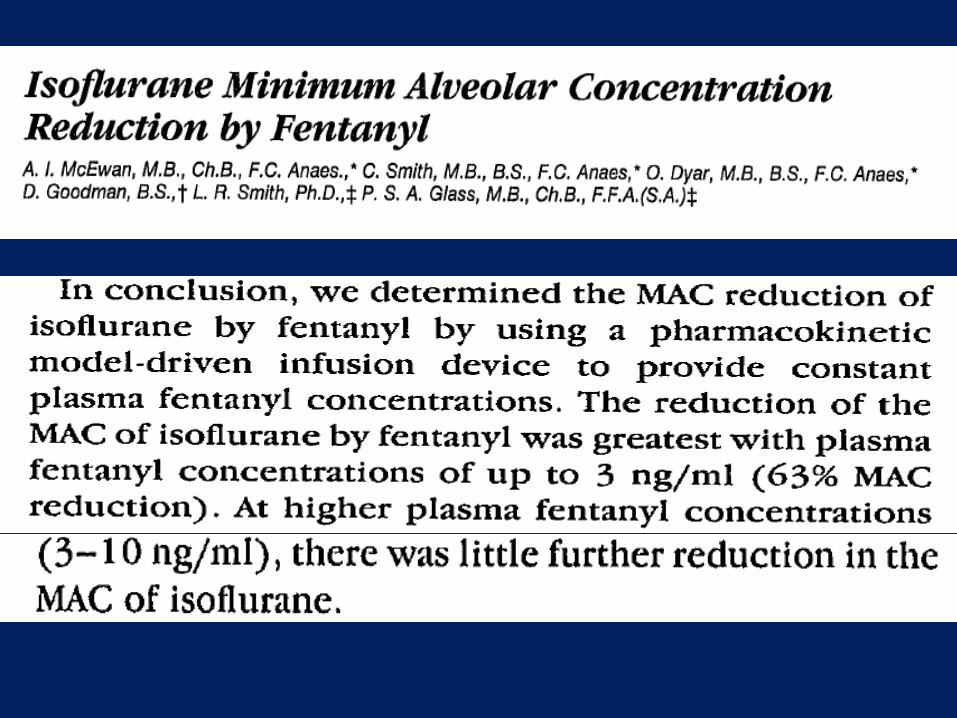
MAC Reduction of isoflurene by increasing concentrations of fentanyl
A.I. McEwan .Anestesiology 78T. 864-869 tahun 1993

MAC Reduction of isoflurene by increasing concentration of fentanyl




Fentanyl menurunkan MAC agenanestesi inhalasi
(From Katoh T et al: Sevoflurane Requirements for tracheal intubation with and without fentanyl. British Journal of Anesthesia 1999.)
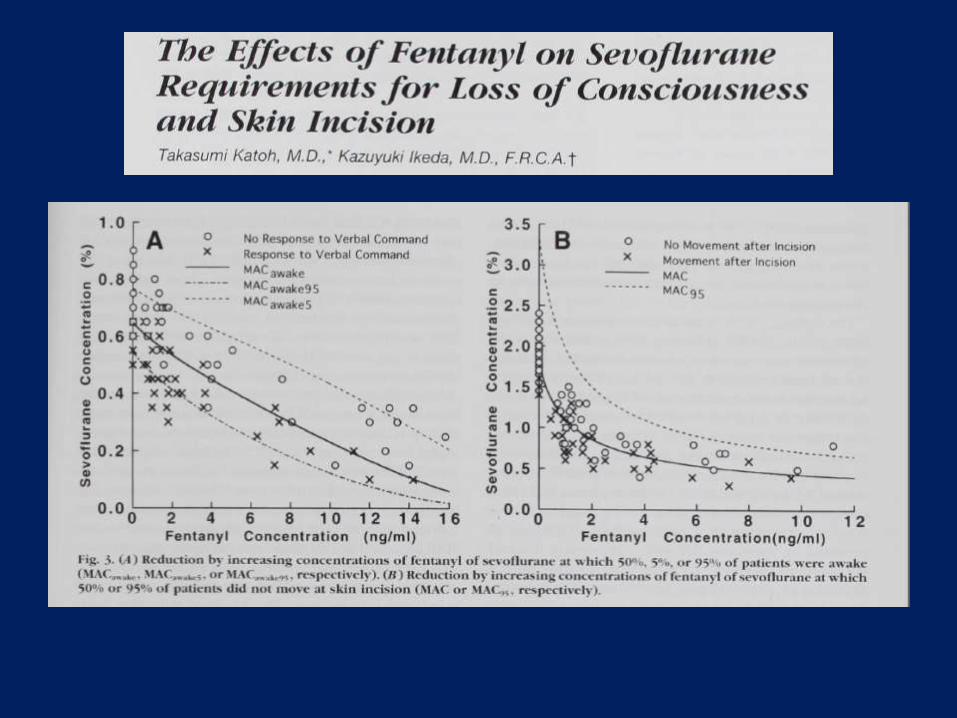

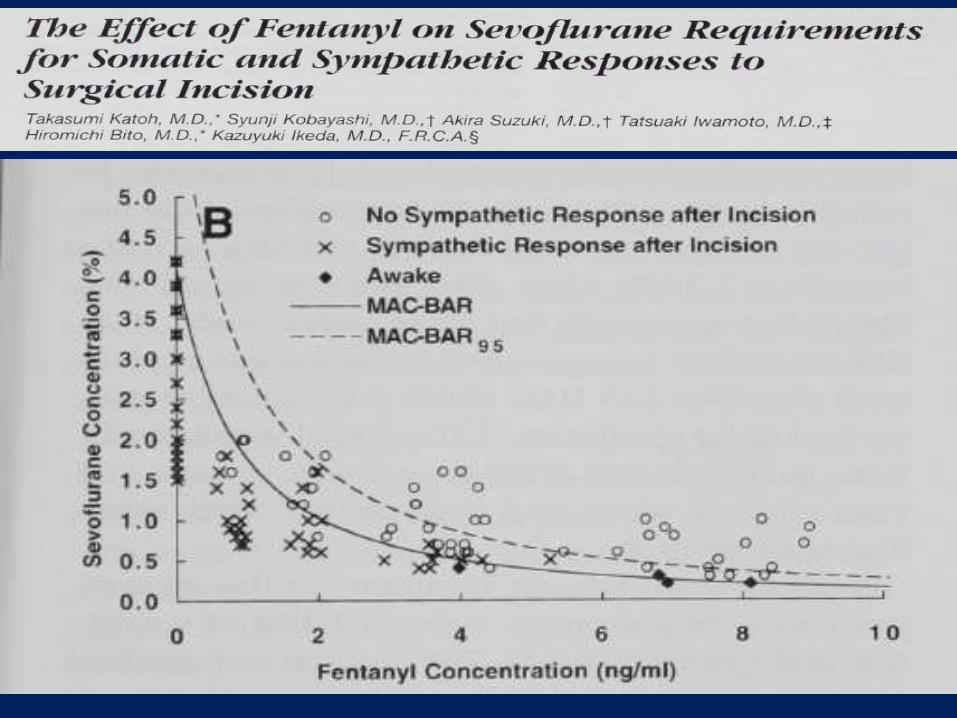
Reduction in MAC, MAC-BAR and MAC Awake of sevoflure by increasing concentration of fentanyl
Takasumi Katoh dkk 199
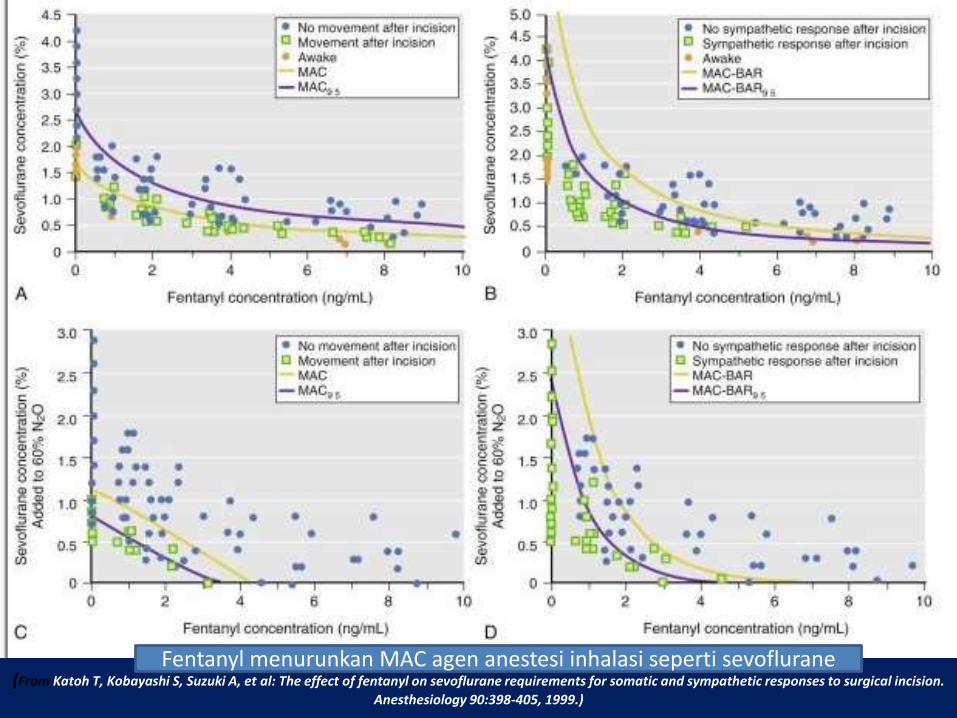
(From Katoh T, Kobayashi S, Suzuki A, et al: The effect of fentanyl on sevoflurane requirements for somatic and sympathetic responses to surgical incision.
Anesthesiology 90:398-405, 1999.)
Fentanyl menurunkan MAC agen anestesi inhalasi seperti sevoflurane



The Potentiation of Anesthetic Agents with Fentanyl
Katoh and Ikeda, 1999
The Potentiation of Sevoflurane and Fentanyl with Fentanyl Dosage Regiment of 0, 1, 2 and 4 µg/kg BWResult: Fentanyl 4 µg/kgBW was the most effective in decreasing autonomic stimulation along with decreasing Sevofluraneconsumption during operation
Xuan Wang2008
The Potentiation of Enflurane and Fentanyl on Pediatric PatientResult: Fentanyl group showed decreasing EnfluraneMAC level

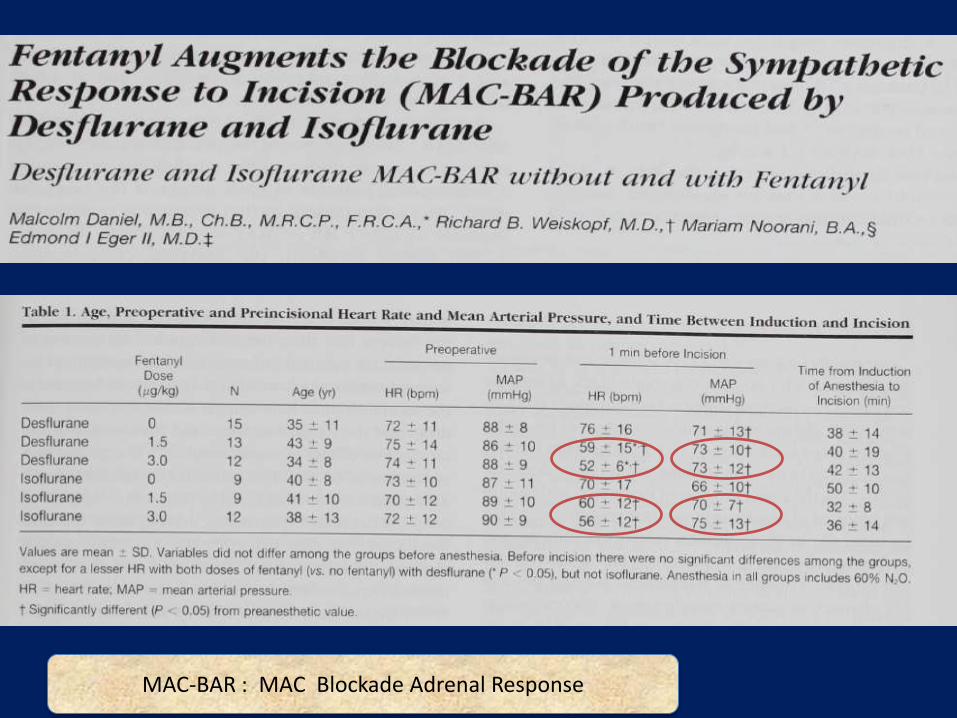
MAC-BAR : MAC Blockade Adrenal Response

MAC : MAC tracheal intubation




Fentanyl effect on MAP and HR
Fentanyl dosis 4 mcg/kg menurunkan denyut jantung dan MAP lebih efektif dari pada 1 atau 2 mcg/kg
(From Katoh T et al: Sevoflurane Requirements for tracheal intubation with and without fentanyl. British Journal of Anesthesia 1999.)

Fentanyl administration before intubation
• Most effective : 5 minutes before intubation
Ko SH et al. Small Dose Fentanyl Optimal Time of Injection for Blunting the Circulatory
Response to tracheal intubation. Anesth Analg 1998
(dosis pre-intubasi 2 mcg/kg)

Fentanyl administration before intubation
Channaiah et al. Low dose fentanyl : hemodynamic response to endotracheal intubation in
normotensive patients. Arch Med Sci Journal 2008
(dosis pre-intubasi 2 mcg/kg)

Premedication fentanyl added to the propofol regimen was shown able to reduce Systolic Blood Pressure (SBP) response due to airway manipulation (dosis pre-induksi 2 mcg/kg)
Fentanyl administration before intubation
*P <0.05
Adachi A, et al. Fentanyl Attenuates the
Hemodynamic Response to Endotracheal Intubation
More Than the Response to Laryngoscopy. Anesth
Analg 2002;95:233–7

• Premedication fentanyl also affected Diastolic Blood Pressure (DBP) response due to airway manipulation (dosis pre-induksi 2 mcg/kg)
Fentanyl administration before intubation
*P <0.05
Adachi A, et al. Fentanyl Attenuates the
Hemodynamic Response to Endotracheal Intubation
More Than the Response to Laryngoscopy. Anesth
Analg 2002;95:233–7

THE COMPARISION OF 4 µG/KgBW and 2 µG/KgBW FENTANYL to
HEMODYNAMIC STABILITY along with ISOFLURANE CONSUMPTION in LAPAROTOMY GYNECOLOGIC SURGERY
ABDUL MUTTALI . MUH.RAMLI AHMAD

Patient
2µg/kg BW FentanylGroup (N=14)
4µg/kg BW FentanylGroup (N=14)
Laparotomy Gynecology Procedure
Fit The Inclusion criteria
Intubation + Surgery
Response
IsofluraneConsumption
Premedication midazolam 0,05 mg/kgBW
Induction propofol 2-2,5 mg/kg BWAtracurium 0,5 mg/kgBW Maintenace
Monitoring HR,TD,BIS,TOF ETCO2,
(+) Isoflurane 0,5 %
Metode
Hemodynamic Fluctuation (+)
Rescue Fentanyl(--) Isoflurane 0,5%

Grafik perbandingan tekanan darah sistolik antara kedua kelompok
0
20
40
60
80
100
120
140
160
Sblmind
Sdhind
Sdhint
5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90 95 100 105 110 115
Kontrol
Perlakuan
0.9
24P =
0.3
87
0.1
01
0.0
02
0.0
26
0.0
04
0.0
08
0.0
23
0.0
26
0.0
35
0.0
71
0.0
02
0.0
11
0.0
40
0.0
08
0.0
23
0.0
48
0.2
08
0.0
02
0.0
00
0.0
02
0.0
02
0.0
00
0.0
01
0.0
93
0.0
28
teka
nan
dar
ah s
isto
lik (
mm
Hg)
TEKANAN DARAH SISTOLIK
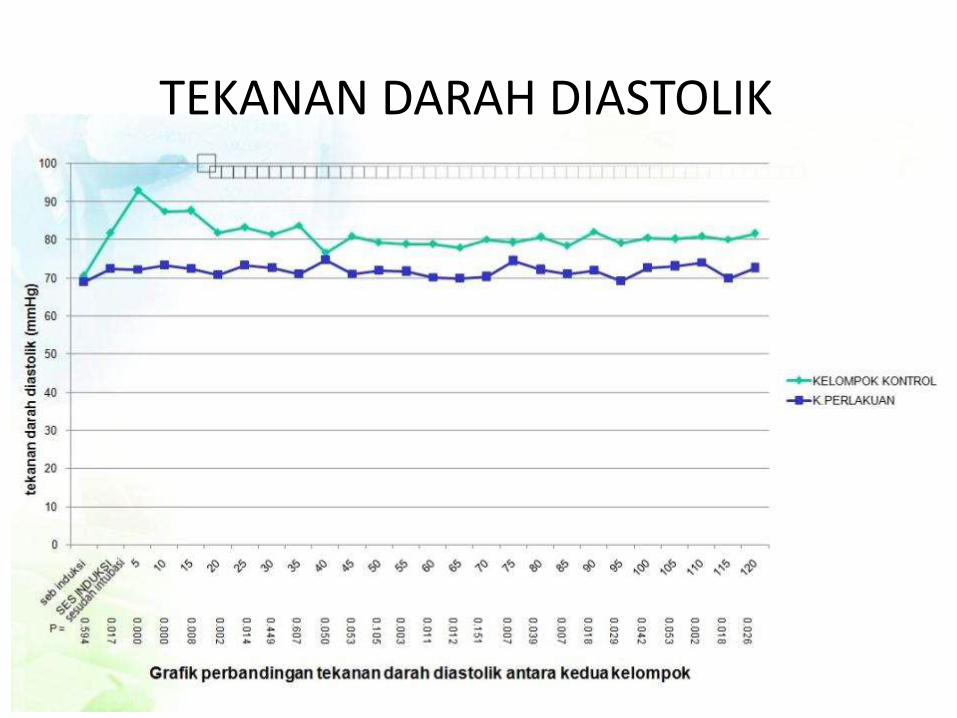
TEKANAN DARAH DIASTOLIK

LAJU JANTUNG

Comparison of Rescue Dose on Both Group
Comparison of Rescue Dose on Both Group
Control Group Experiment Group P
RESCUE DOSE 130.71 ± 45.987 24.64 ± 29.64 0,0000
All data was shown as mean value and tested with Mann Withney U test as significant was pronounced when p value less than 0.05

Comparison of Isoflurane Consumption
KEBUTUHAN ISOFLURAN
KELOMPOK KONTROL
K.PERLAKUAN
Figure 4. Comparison of Isoflurane consumption on both group
GROUP
Isoflurane Consumption Control Experiment p
47.0871 ± 2.43035.8736± .996
0,0000
All data was shown as mean value and tested with Mann Withney U test as significant was pronounced when p value less than 0.05

RESULT
Fentanyl 4 µg/kgBB Vs 2µg/kgBB
Better Hemodynamic Stability
Less Rescue Dose
Less Isoflurane Consumption

Conclusions
• Fentanyl produces a reduction in the minimum alveolar concentarion ( MAC) of isoflurene, sevoluren and desflurance
• Minimum alveolar concentarion (MAC) and Minimum alveolar concentarion blockade adrenergic response (MEC BAR)MAP and heart rate decreased similarly with creasing concentrations of fentanyl in plasma.
• Somatic and symphatetic responses to surgycal incision are clinical end points for assessing depth of anesthesia
• The intraction of fentanyl on the Cp50 of Propofol and Thiopental.

Thank you!FOR YOUR ATTENTION

• Isoflurane consumption was total of isofluranefor the whole operation (ml) and calculated with the following equation :
C:Mean concentration of the anesthetic volatile agent (vol%, T; Duration
of the operation, Flow O2: O2 flow (l/mnt), (Vapour pressure isoflurane : 240 )
Vol : C x Flow O2 x 1/ Vapour pressure x T