pain sub-department of neurology department · pdf filediagnosis yang paling mungkin? a....
TRANSCRIPT
PAIN
Yudiyanta Pain Sub-Department
of Neurology Department
Kasus 1
• 38 th• 1HSMRS LBP + kedua
bokong• Limitasi ROM terutama pada
gerakan fleksi dan rotasi.• NPS 6.• Neuro Exam: dbn• Suhu tubuh 37.8 C.• Nyeri tekan diatas vertebra
lumbal 4-5 dan dibokong (+).
Diagnosis yang paling mungkin?
A. Fraktur vertebra lumbal 4-5B. Spondilolistesis vertebra lumbal 4-5C. Hernia Nukleus Pulposus Lumbal 4-5D. Sprain MuskulerE. Referred Pain organ internal
Pemeriksaan Penunjang yang dianjurkan:
A. Lumbal X-RayB. Lumbal CT Scan C. Lumbal MRID. ENMGE. Belum perlu
Manakah terapi yang paling rasional?
A. Acetaminofen 3-4 x 1000 mgB. K-diclofenac 2x 50 mg C. Diazepam 3 x 2 mg D. Codein 3 x 20 mg E. Metilpredisolon 8 mg-8mg-0mg

Lumbar “strain” or “sprain”
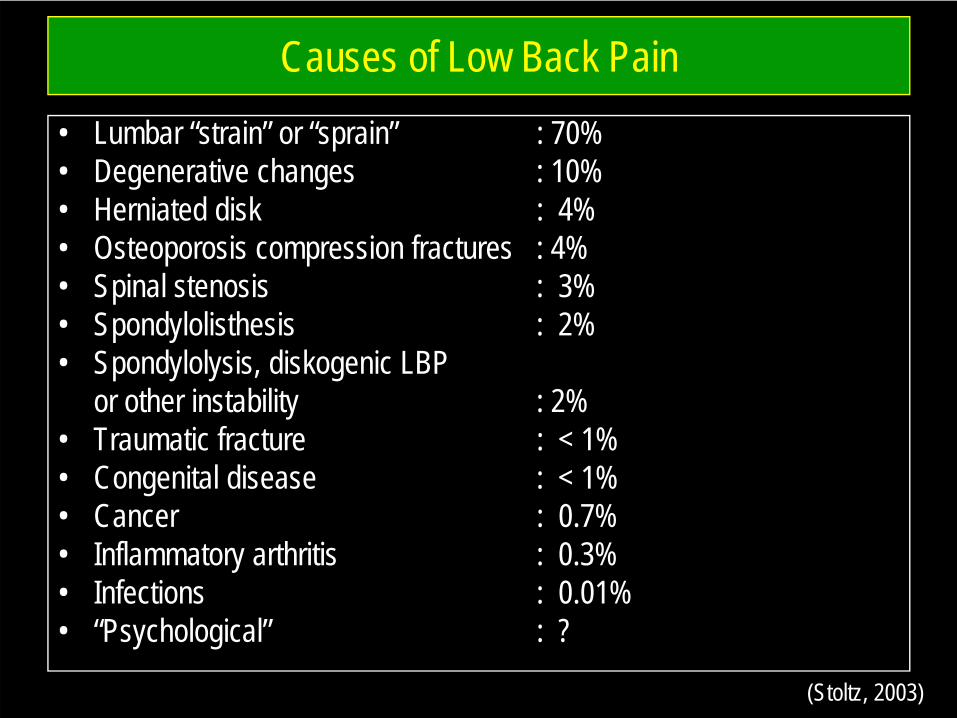
Causes of Low Back Pain• Lumbar “strain” or “sprain” : 70%• Degenerative changes : 10%• Herniated disk : 4%• Osteoporosis compression fractures : 4%• Spinal stenosis : 3%• Spondylolisthesis : 2%• Spondylolysis, diskogenic LBP
or other instability : 2%• Traumatic fracture : < 1%• Congenital disease : < 1%• Cancer : 0.7%• Inflammatory arthritis : 0.3%• Infections : 0.01%• “Psychological” : ?
(Stoltz, 2003)
Pemeriksaan Penunjang yang dianjurkan:
A. Lumbal X-RayB. Lumbal CT Scan C. Lumbal MRID. ENMGE. Belum perlu
Role of X-rays (Radiology)• Usually unnecessary and not helpful• Plain X-ray:
– Age > 50 years– No improvement after 6 weeks– Significant Trauma
• MRI :– After 6 weeks if have sciatica
Red Flags
• Significant trauma history, or minor in older adults• Nocturnal pain in supine position with history of cancer• Bladder or bowel incontinence or dysfunction• Constitutional symptoms:
• Fever / chills • Weight loss• Lymph node enlargement
• Risk factors for spinal infection• Recent infection• IV drug use• Immunosuppression
• Major motor weakness
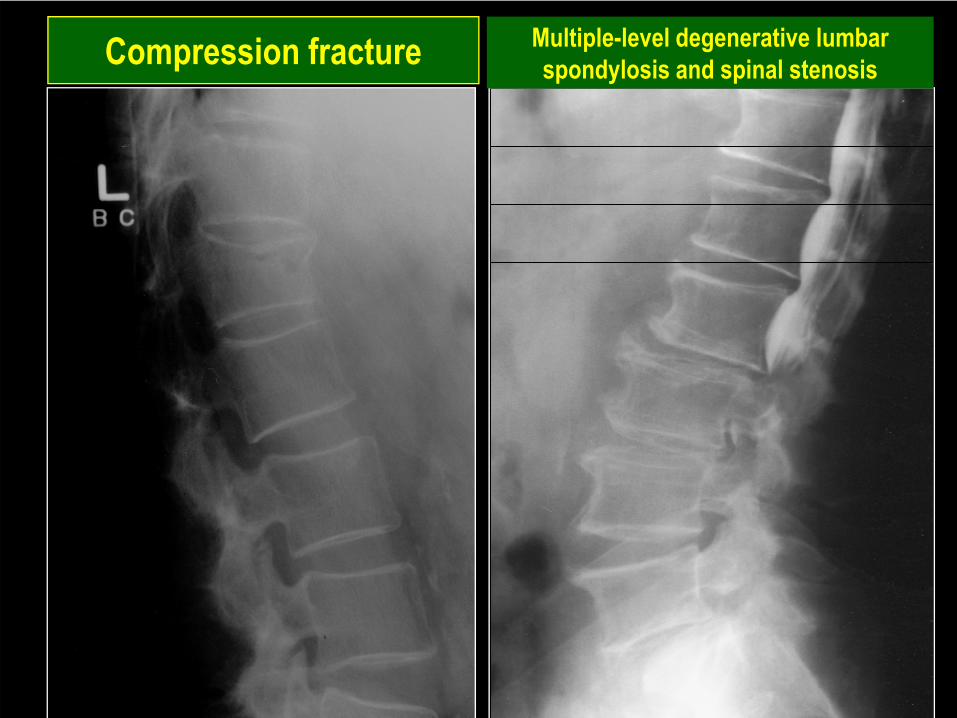
Compression fracture Multiple-level degenerative lumbar spondylosis and spinal stenosis

Spondylolisthesis
Manakah terapi yang paling rasional?
A. Acetaminofen 3-4 x 1000 mgB. K-diclofenac 2x 50 mg C. Diazepam 3 x 2 mg D. Codein 3 x 20 mg E. Metilpredisolon 8 mg-8mg-0mg
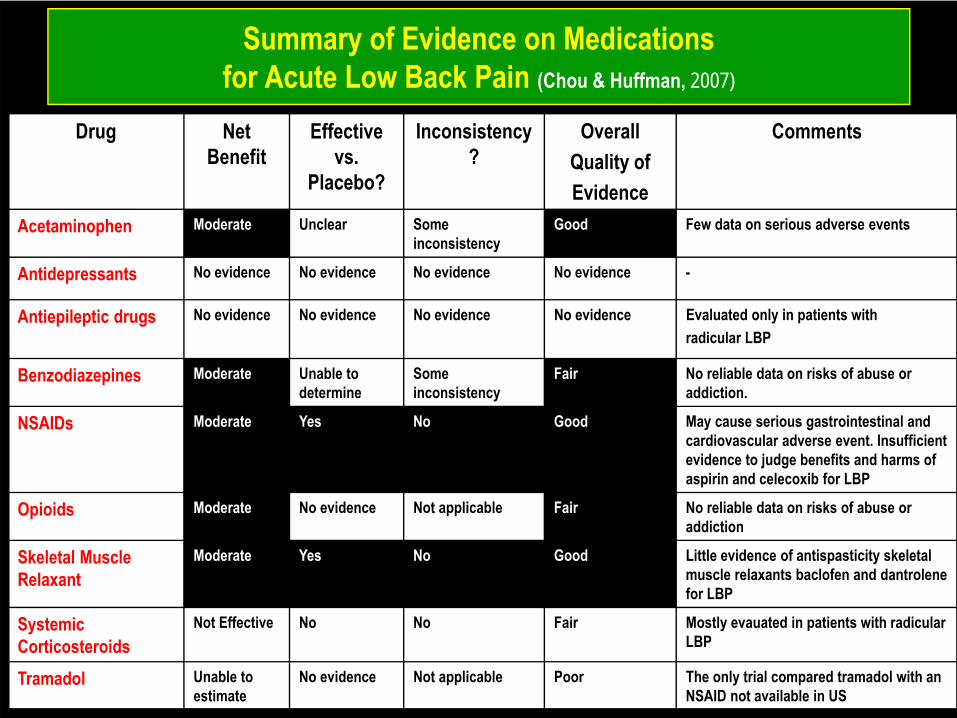
Summary of Evidence on Medications for Acute Low Back Pain (Chou & Huffman, 2007)
Drug Net Benefit
Effective vs.
Placebo?
Inconsistency?
OverallQuality ofEvidence
Comments
Acetaminophen Moderate Unclear Some inconsistency
Good Few data on serious adverse events
Antidepressants No evidence No evidence No evidence No evidence -
Antiepileptic drugs No evidence No evidence No evidence No evidence Evaluated only in patients withradicular LBP
Benzodiazepines Moderate Unable to determine
Some inconsistency
Fair No reliable data on risks of abuse or addiction.
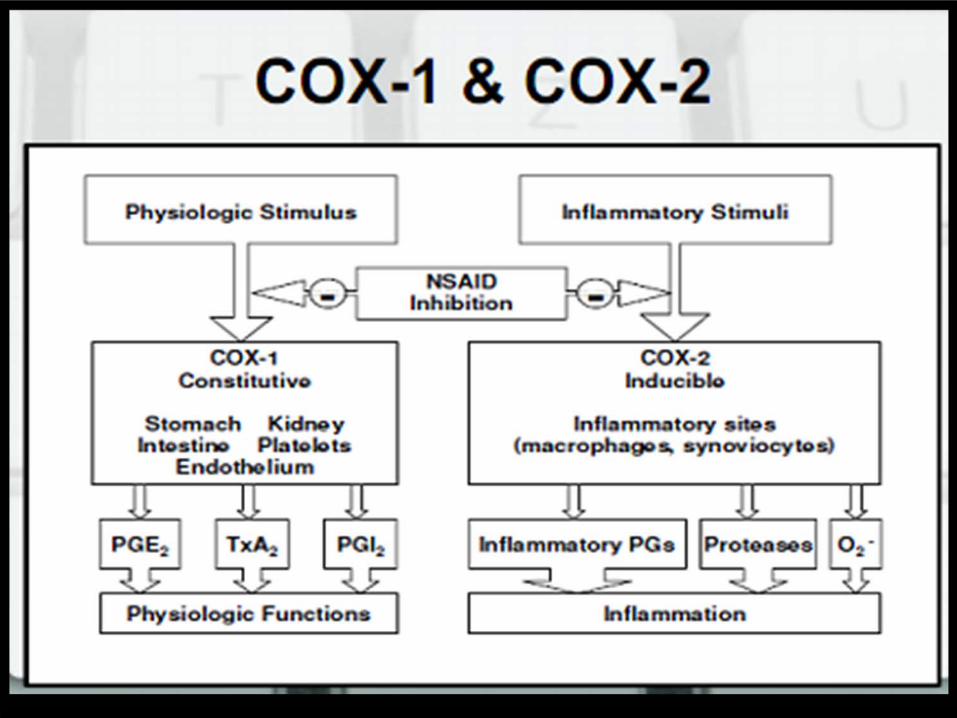
NSAIDs Moderate Yes No Good May cause serious gastrointestinal and cardiovascular adverse event. Insufficient evidence to judge benefits and harms of aspirin and celecoxib for LBP
Opioids Moderate No evidence Not applicable Fair No reliable data on risks of abuse or addiction
Skeletal Muscle Relaxant
Moderate Yes No Good Little evidence of antispasticity skeletal muscle relaxants baclofen and dantrolene for LBP
Systemic Corticosteroids
Not Effective No No Fair Mostly evauated in patients with radicular LBP
Tramadol Unable to estimate
No evidence Not applicable Poor The only trial compared tramadol with an NSAID not available in US
• Jika pada pemeriksaan ditemukan:– TD : 110/80– Ureum: 28– Creatinin : 1,1– SGOT: 30– SGPT: 28 – Nyeri tekan epigastrium (+).
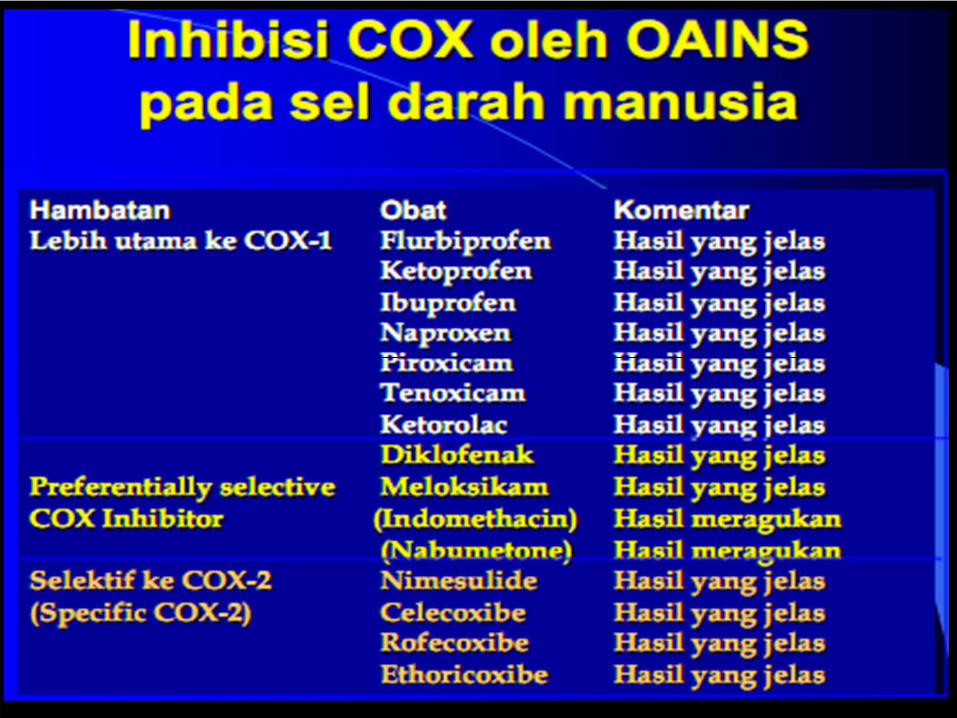
Pilihan NSAIDs yang paling rasional?
A. Ibuprofen 2-3 x 400 mgB. K-Diclofenac 2x50 mgC. Asam Mefenamat 3x500 mgD. Paracetamol 3x500 mgE. Celecoxib 2x200 mg
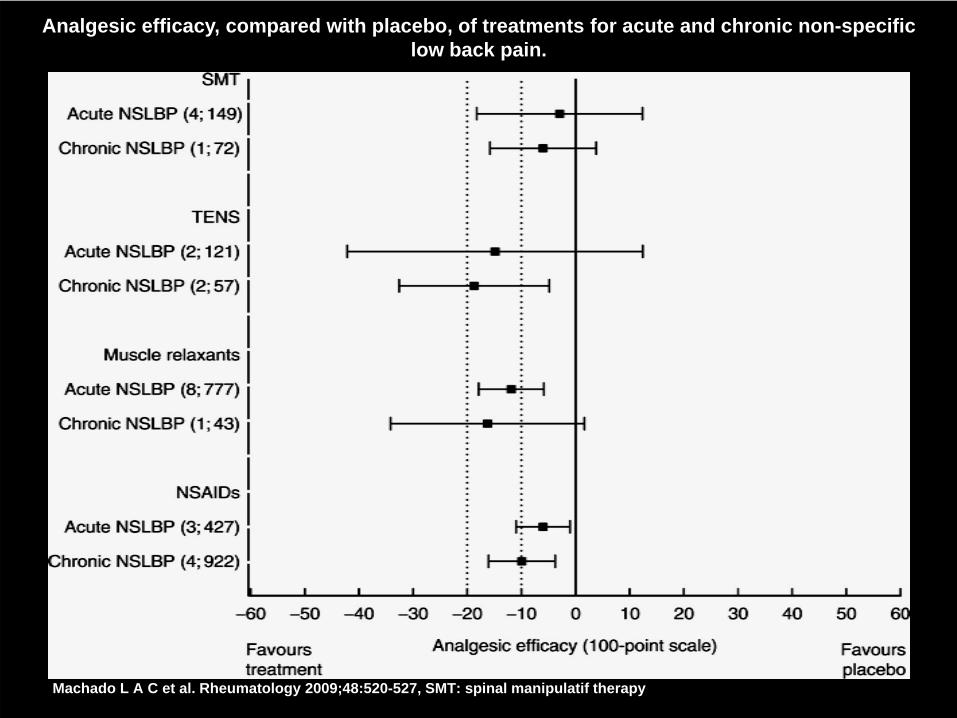
Analgesic efficacy, compared with placebo, of treatments for acute and chronic non-specific low back pain.
Machado L A C et al. Rheumatology 2009;48:520-527, SMT: spinal manipulatif therapy
Berapa lama saya bedrest?
A. 1-2 hariB. 5 hariC. 1 mingguD. 10 hari E. Tidak perlu bedrest, langsung aktifitas
Apakah boleh pijat?
A. BolehB. Tidak boleh
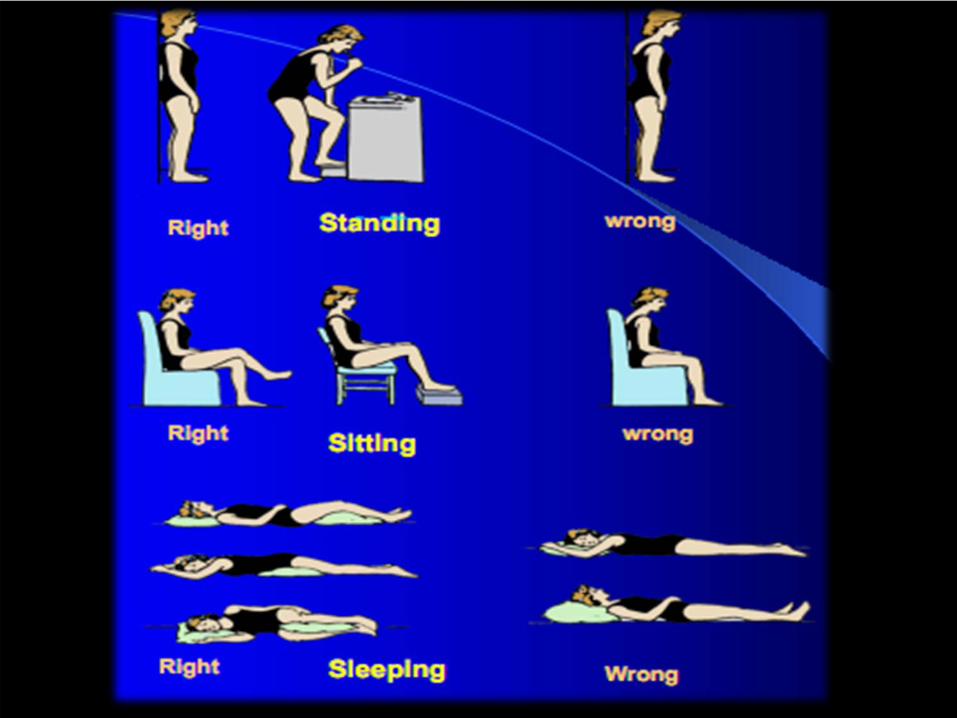
Exercise & Bed Rest• Advice to stay active:
– There is no evidence that advice to stay active is harmful for either acute low back pain or sciatica
• 1-2 days of bed rest if necessary• Light activity, avoiding heavy lifting, bending or twisting
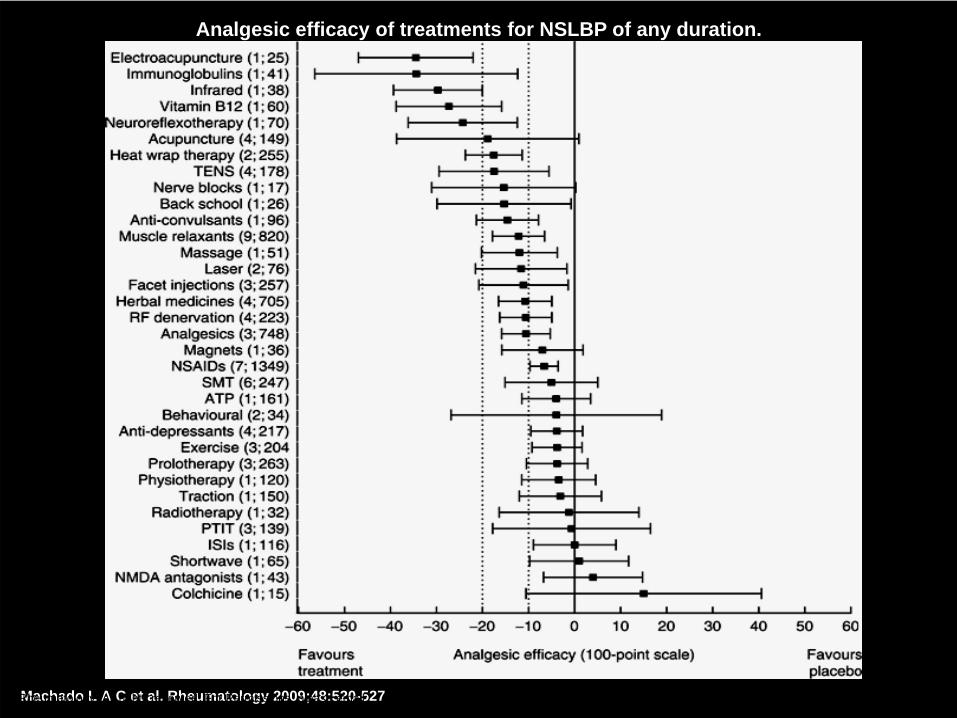
Analgesic efficacy of treatments for NSLBP of any duration.
Machado L A C et al. Rheumatology 2009;48:520-527© The Author 2008. Published by Oxford University Press on behalf of the British Society for
Rheumatology. All rights reserved. For Permissions, please email: [email protected]
KASUS 2
• Wanita 52 th dg keluhan nyeri punggung bawahmenjalar ke tungkai kanan. Riwayat angkat junjung(+), riwayat trauma (-). Pada pemeriksaan nyeriterutama dirasakan saat gerakan ekstensi badandan miring ke kiri, dan dirasakan lebih nyamandengan posisi badan fleksi dan menekuk ke kanan.Nyeri sudah dirasakan selama 2 bulan.
Diagnosis yang paling mungkin?
A. Fraktur vertebra lumbal B. Spondilolistesis vertebra lumbal C. Hernia Nukleus Pulposus Lumbal D. Sprain MuskulerE. Referred Pain organ internal
Pemeriksaan fisik yang paling sensitif mendukung diagnosis kerja anda:
A. Patrick signB. Kontra-Patrick SignC. Lasegue signD. Lasegue silang sign E. Babinski sign
Pemeriksaan Penunjang yang dianjurkan:
A. Lumbal X-RayB. Lumbal CT Scan C. Lumbal MRID. ENMGE. Belum perlu
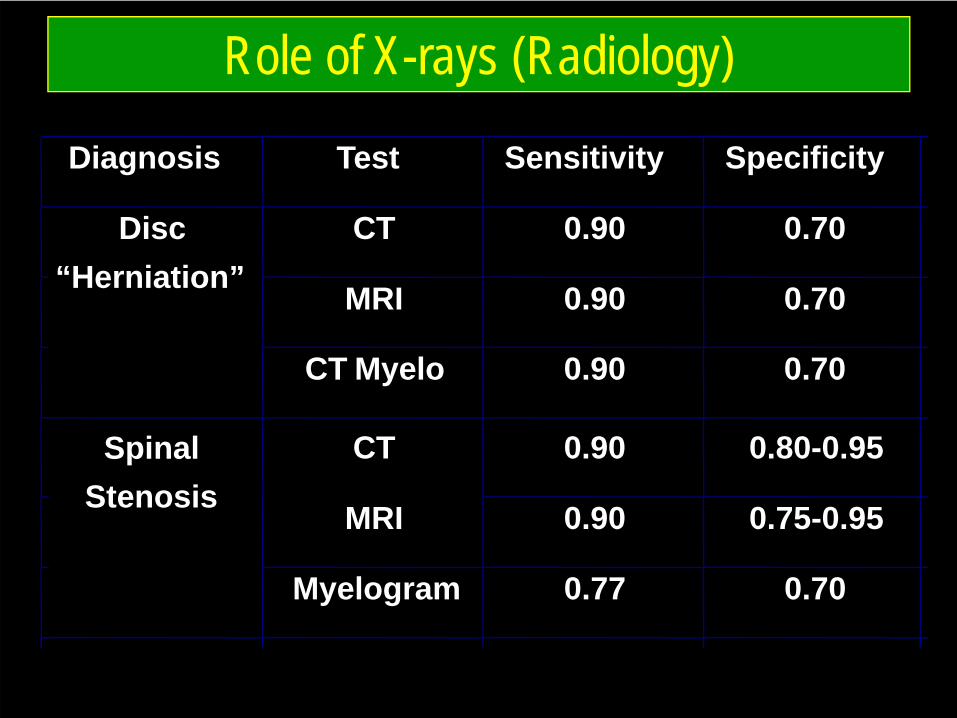
Role of X-rays (Radiology)
Diagnosis Test Sensitivity Specificity
CT 0.90 0.70
MRI 0.90 0.70
Disc“Herniation”
CT Myelo 0.90 0.70
CT 0.90 0.80-0.95
MRI 0.90 0.75-0.95
SpinalStenosis
Myelogram 0.77 0.70
• Pada evaluasi lebih lanjut, OS mengeluh nyeridengan rasa kemeng dan pegal, tidak berdenyut,disertai rasa terbakar, kadang-kadang jika salahposisi nyeri seperti tersetrum sampai ujung kaki.Kesemutan dan tebal2 juga dirasakan. NPS 6.
Terapi Farmakologi yang paling rasional?
A. Paracetamol 325 mg-tramadol 37,5 mg, gabapentin 100 mg, metikobalamin 500 mcg
B. Paracetamol 650 mg, amitriptilin 25 mg, gabapentin 100 mg
C. Tramadol 50 mg, amitriptilin 25 mg, codein 10 mg
D. Paracetamol 650 mg, tramadol 50 mg, carbamazepin 200 mg
E. Celecoxib 200 mg, amitriptilin 25 mg, metilprednisolon 8 mg po
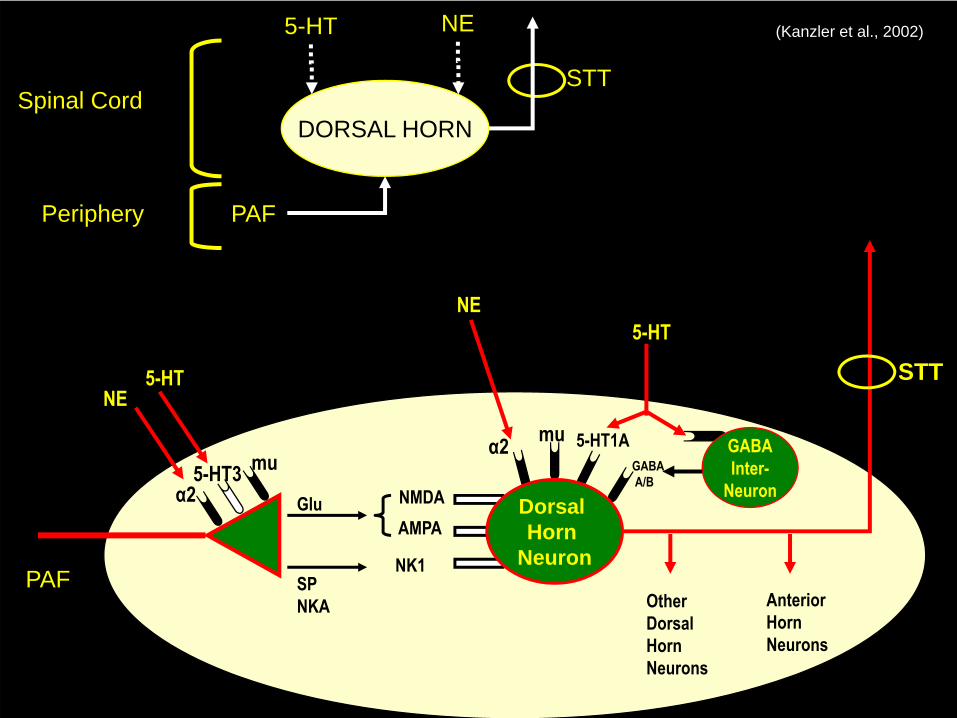
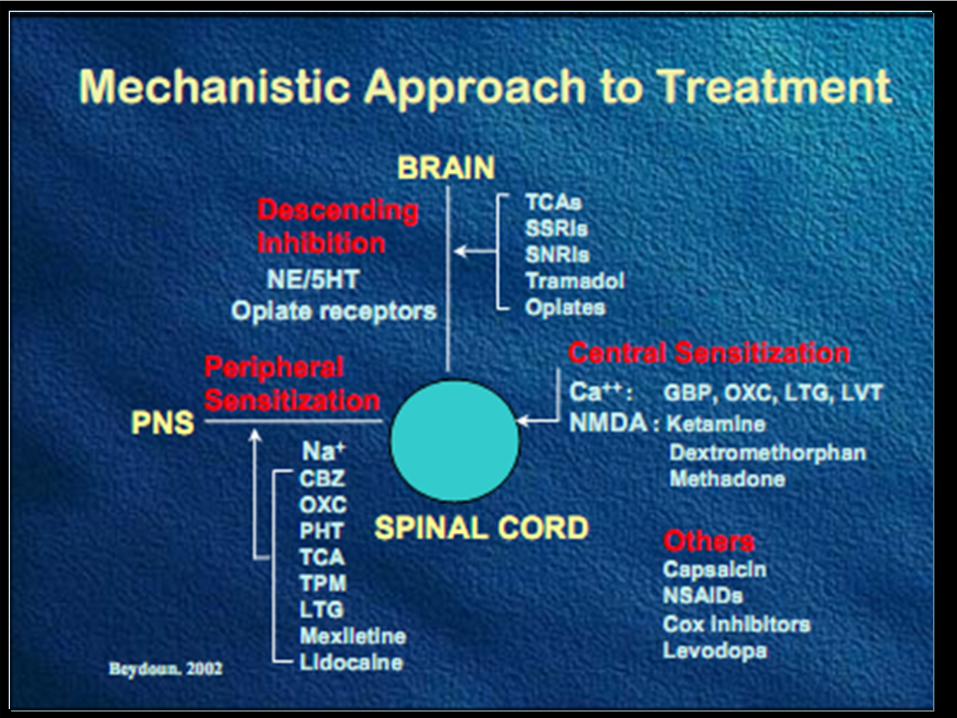
DORSAL HORN
NE5-HT
PAF
Spinal Cord
Periphery
STT
STT
Other Dorsal Horn Neurons
AnteriorHorn Neurons
α25-HT3 mu
5-HTNE
NMDAAMPA
NK1
Glu
SPNKA
Dorsal Horn
Neuron
α2 5-HT1AmuGABAA/B
GABAInter-
Neuron
5-HTNE
(Kanzler et al., 2002)
PAF
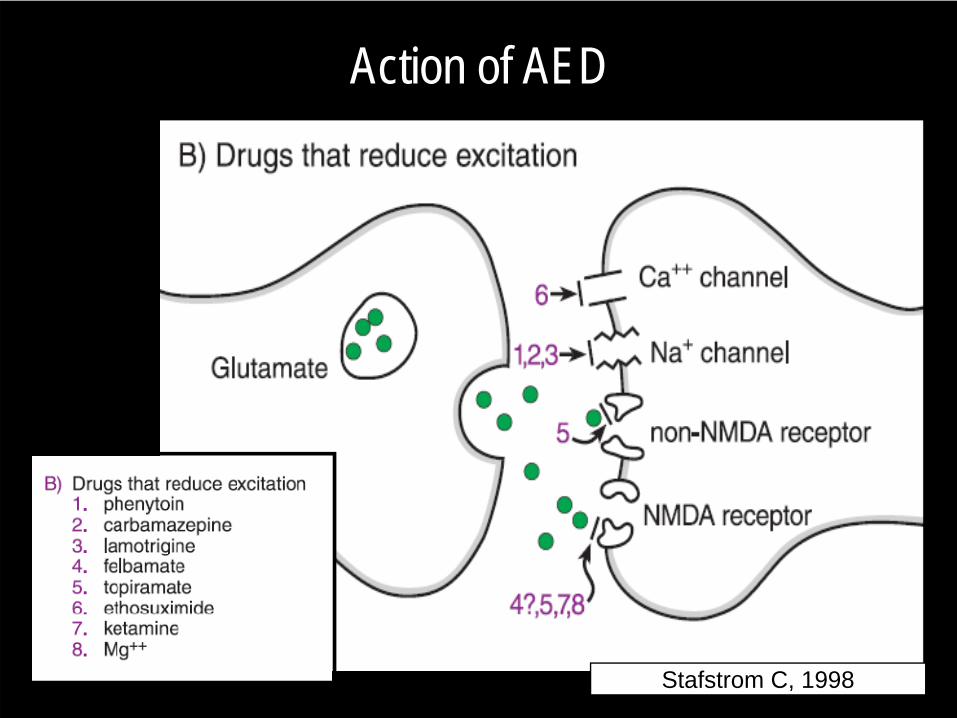
Action of AED
Stafstrom C, 1998
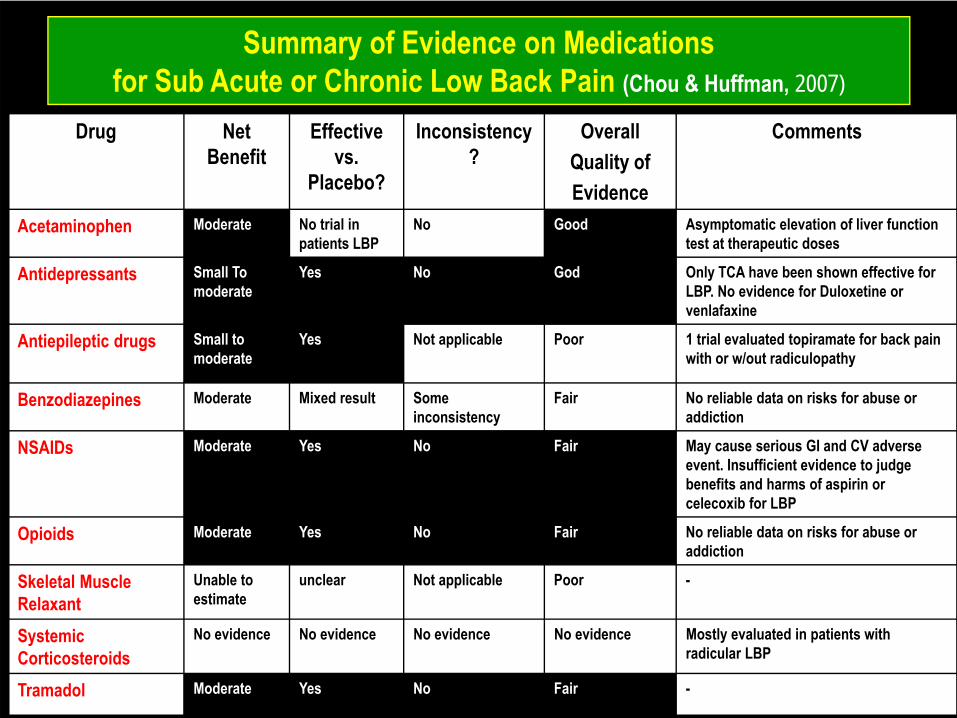
Summary of Evidence on Medications for Sub Acute or Chronic Low Back Pain (Chou & Huffman, 2007)
Drug Net Benefit
Effective vs.
Placebo?
Inconsistency?
OverallQuality ofEvidence
Comments
Acetaminophen Moderate No trial in patients LBP
No Good Asymptomatic elevation of liver function test at therapeutic doses
Antidepressants Small To moderate
Yes No God Only TCA have been shown effective for LBP. No evidence for Duloxetine or venlafaxine
Antiepileptic drugs Small to moderate
Yes Not applicable Poor 1 trial evaluated topiramate for back pain with or w/out radiculopathy
Benzodiazepines Moderate Mixed result Some inconsistency
Fair No reliable data on risks for abuse or addiction
NSAIDs Moderate Yes No Fair May cause serious GI and CV adverse event. Insufficient evidence to judge benefits and harms of aspirin or celecoxib for LBP
Opioids Moderate Yes No Fair No reliable data on risks for abuse or addiction
Skeletal Muscle Relaxant
Unable to estimate
unclear Not applicable Poor -
Systemic Corticosteroids
No evidence No evidence No evidence No evidence Mostly evaluated in patients with radicular LBP
Tramadol Moderate Yes No Fair -
• Hasil lab menunjukkan:– Hb 12 g%– Al 7.000– SGOT: 100– SGPT : 189– Ureum: 63– Creatinin 2,7
Berdasarkan Klinis dan Hasil Lab diatas, analgetik apa yang paling anda rekomendasikan?
A. Paracetamol 650 mgB. Paracetamol 500 mg + Celecoxib 100 mg C. Paracetamol 325 mg + tramadol 37,5 mgD. Celexocib 200 mg+ meloksikam 7,5 mg E. Piroxicam 20 mg + Paracetamol 300 mgF. Asam mefenamat 500 mg + paracetamol
500 mg
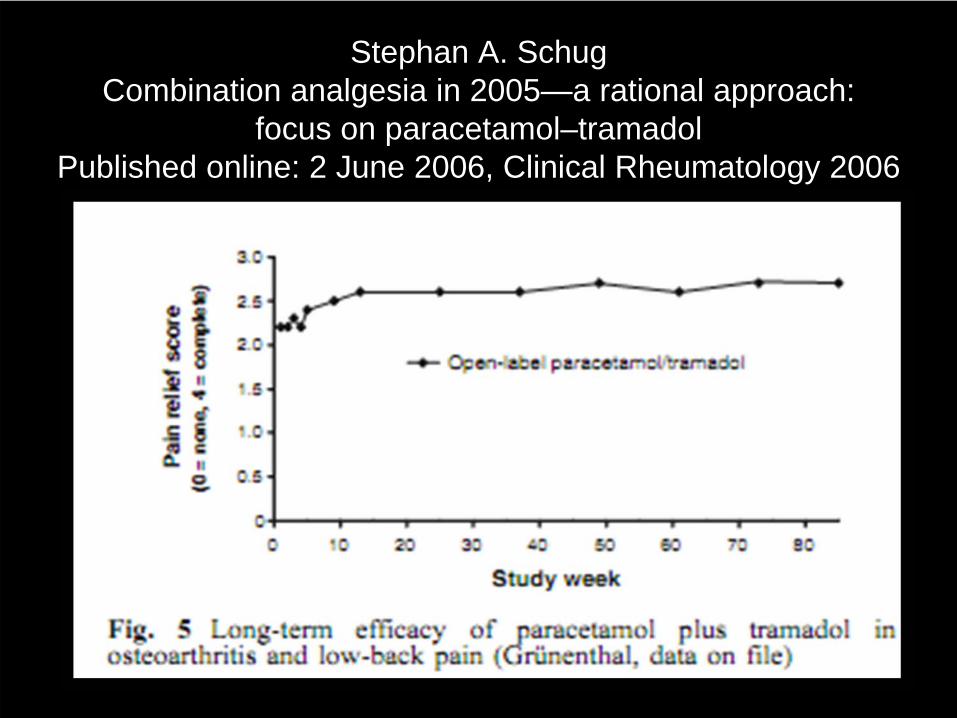
Stephan A. SchugCombination analgesia in 2005—a rational approach:
focus on paracetamol–tramadolPublished online: 2 June 2006, Clinical Rheumatology 2006
Cont’• safety concerns about long-term use:
– has demonstrated efficacy in the control of a variety of chronic pain states.
– long-term treatment up to 2 years’ duration.– well-tolerated and has reduction in adverse events– a useful add-on analgesic treatment if existing therapy is
insufficiently effective

Pemeriksaan MRI menunjukkan hasil seperti ini:
Anda merekomendasikan tindakan operatif jika:
A. Bacaan imaging HNPB. Sindrome cauda equinaC. Progressive Motor LossD. Intractable PainE. Klinis canalis stenosis spinalis
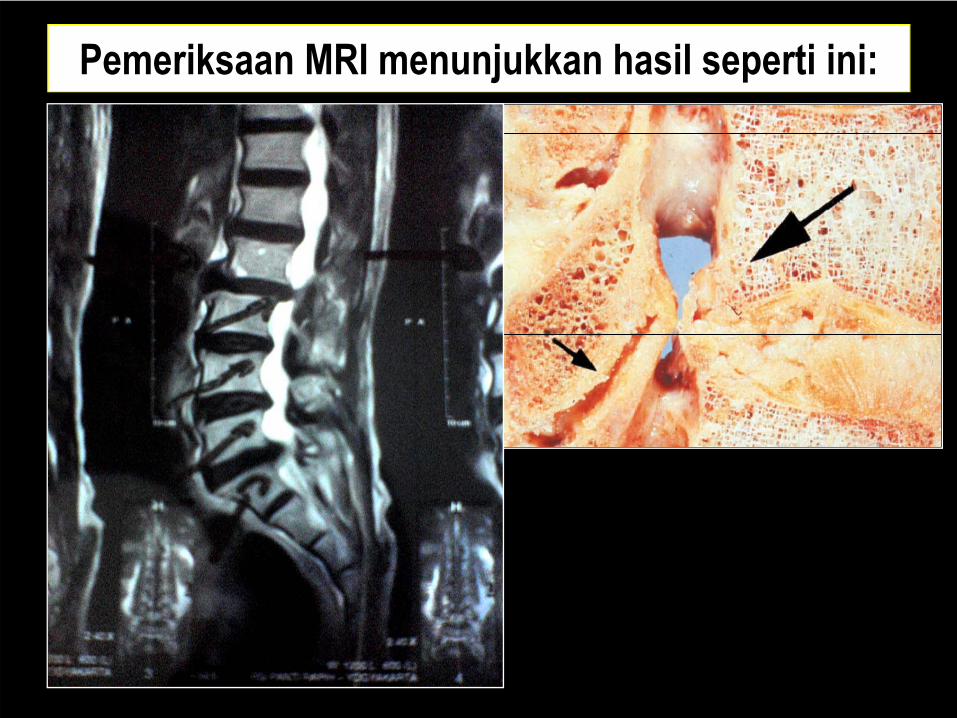
Pemeriksaan MRI menunjukkan hasil seperti ini:
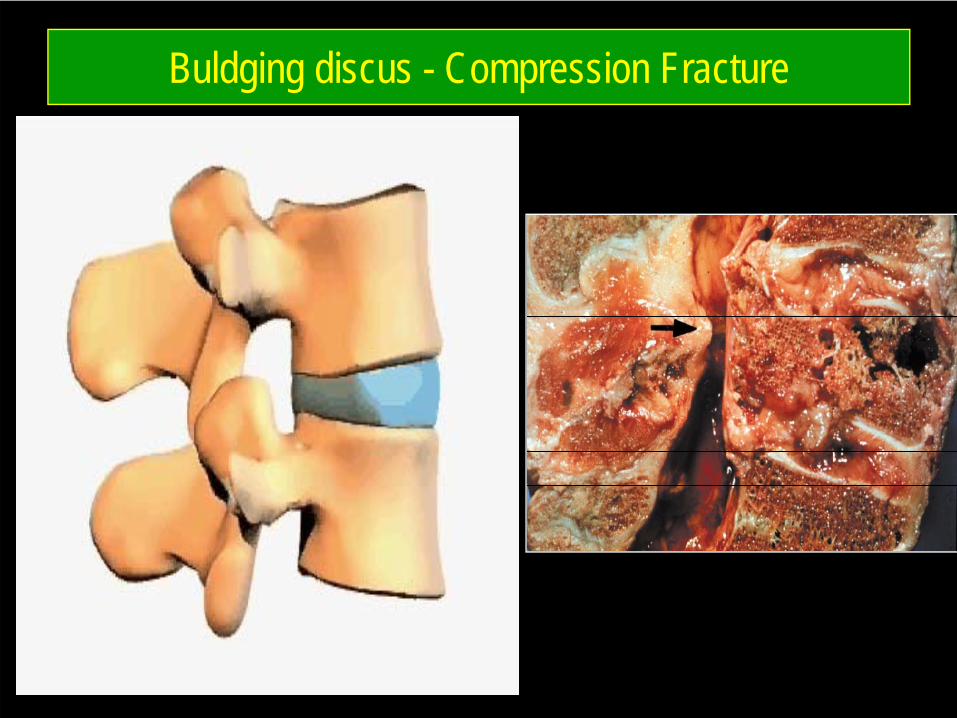
Buldging discus - Compression Fracture
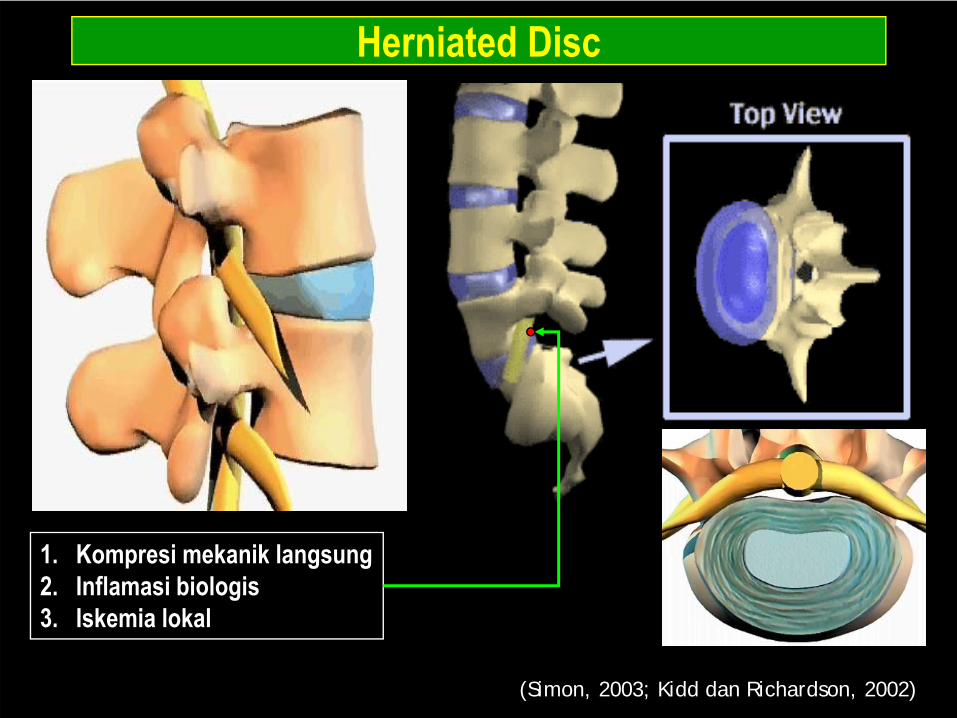
Herniated Disc
(Simon, 2003; Kidd dan Richardson, 2002)
1. Kompresi mekanik langsung2. Inflamasi biologis3. Iskemia lokal
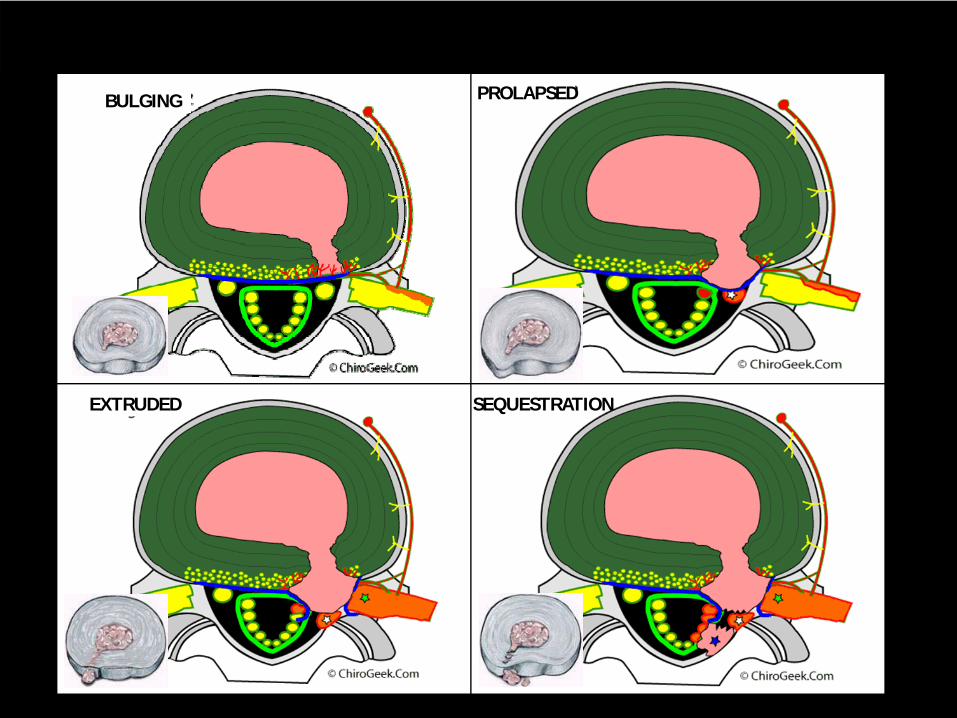
BULGING PROLAPSED
EXTRUDED SEQUESTRATION
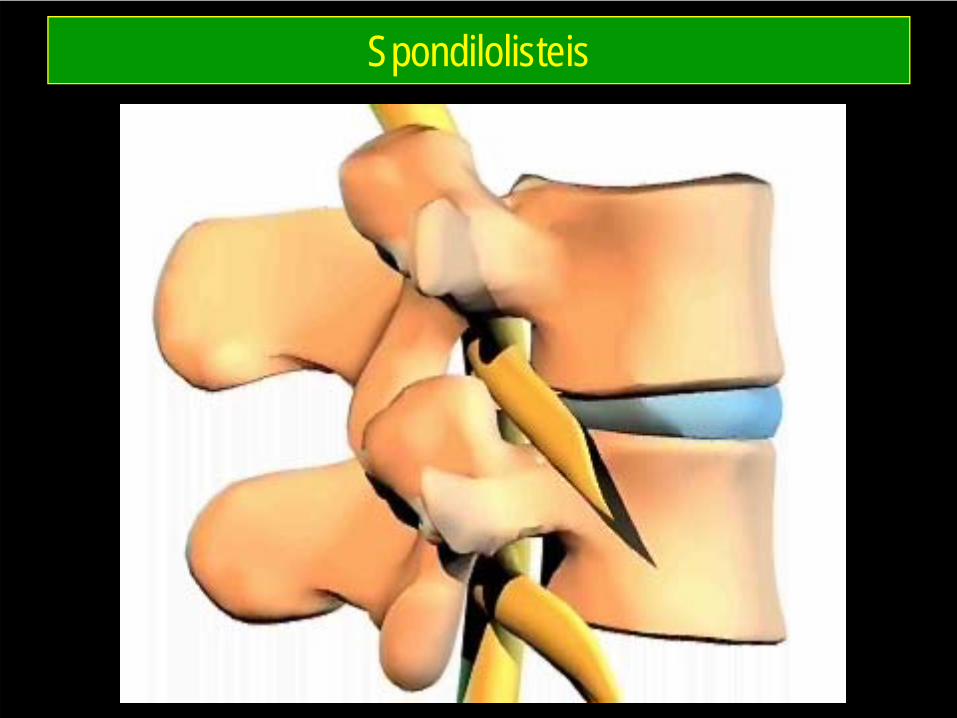
Spondilolisteis
SURGICAL
• Indications:– Cauda Equina– PROGRESSIVE Motor Loss– Intractable Pain– Spinal Canal Stenosis
Surgical Outcome (Weber et al)
• At 1 year:– 90% good outcome with Surgery as compared to 60% with Non-
Surgery• At 4 years:
– Surgery is slightly better (not statistical)• At 10 years:
– Same for both groups

Jika MRI seperti berikut:
Edukasi pada pasien ini yang paling tepat:
A. 62% herniasi diskus akan mengalami resorpsi spontan
B. Respons baik dengan operasi C. Prognosis jangka panjang > 10 tahun
lebih baik pada pasien yang dioperasiD. Harus minum obat seumur hidupE. Tidak akan bisa sembuh
• Treated the patient, not the diagnostic test• Recovery:
– 80 % 3 days to 3 weeks, with or without treatment– Up to 90 % resolved in 6-12 weeks– 86-90% satisfactory outcome in one year Saals et al, Bush et a
– 62% Disc Herniation Resorb Over Time• Large Compressive Discs symptomatic :
– Respond well to surgery – high rate of clinical improvement with non-operative treatment
(Saals et al)
PROGNOSIS on NON-SURGICAL
Other Modalities
• Back Brace/Corset/Lumbar Support• Traction• Injections: Inconclusive evidence• TENS• Hot/Cold• Ultrasound
Prevention
• Exercise:– Aerobic, back/leg strengthening
• Back braces and education about proper lifting techniques
• Weight loss and smoking cessation
Exercises• Improves pain and function• Many programs available, but difficult
to make any scientific recommendations for one type versus another
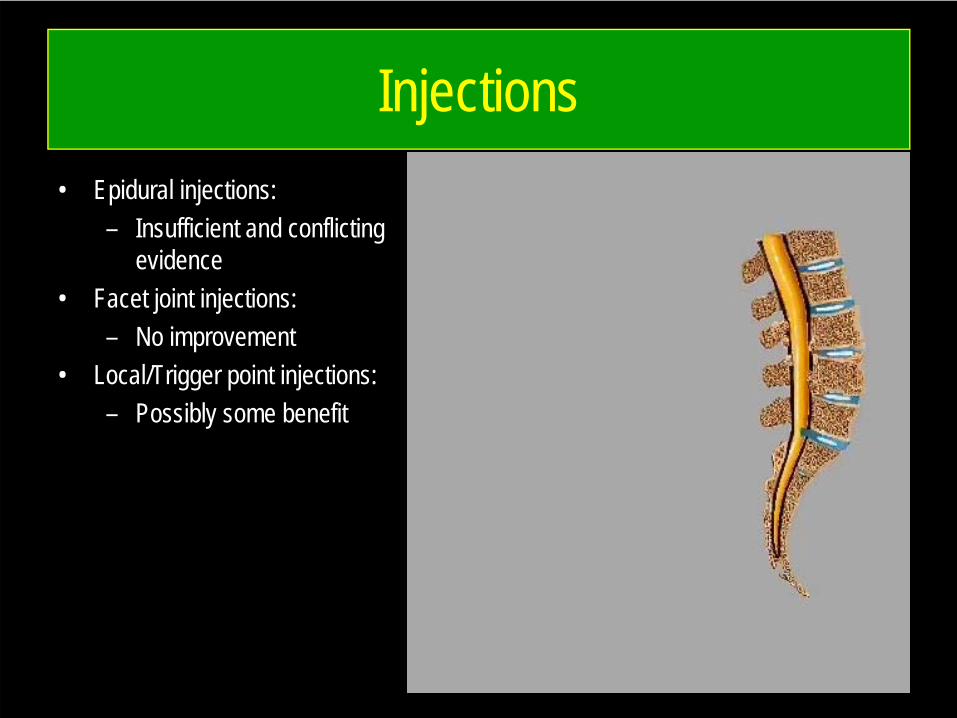
Injections• Epidural injections:
– Insufficient and conflicting evidence
• Facet joint injections:– No improvement
• Local/Trigger point injections:– Possibly some benefit
Symptom Magnification Examination:
• Waddell signs: signs suggesting symptom magnification and psychological distress– Superficial or non-anatomic distribution of tenderness– Non-anatomic or regional disturbance of motor or sensory
impairment – Inconsistency on positional SLR– Inappropriate/excessive verbalization of pain or gesturing– Pain with axial loading or rotation of spine
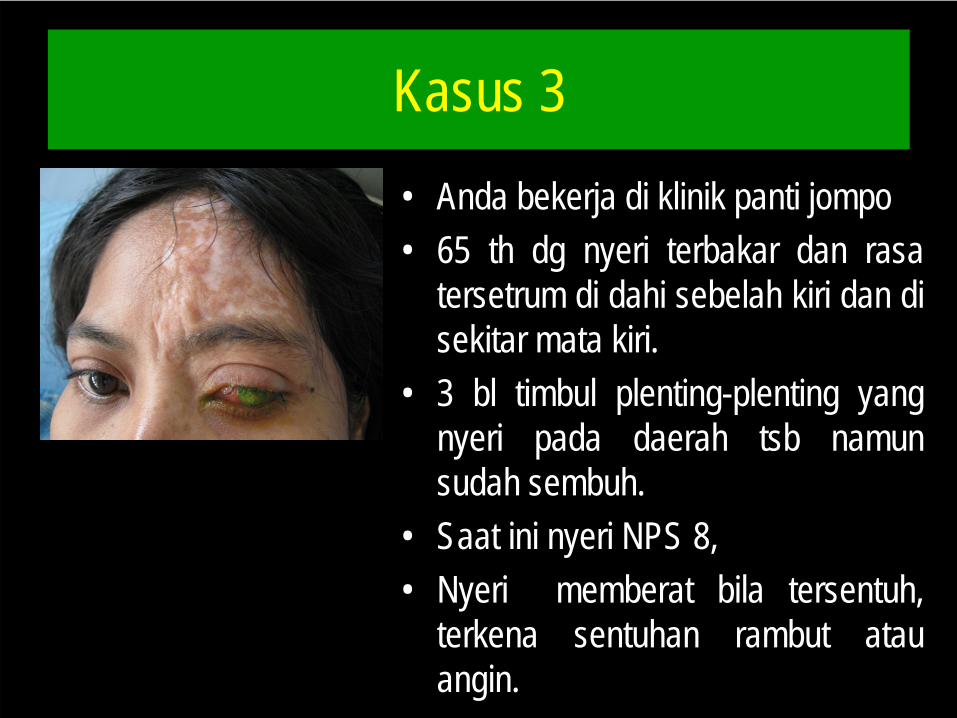
Kasus 3• Anda bekerja di klinik panti jompo• 65 th dg nyeri terbakar dan rasa
tersetrum di dahi sebelah kiri dan disekitar mata kiri.
• 3 bl timbul plenting-plenting yangnyeri pada daerah tsb namunsudah sembuh.
• Saat ini nyeri NPS 8,• Nyeri memberat bila tersentuh,
terkena sentuhan rambut atauangin.
OS hanya bersedia minum satu jenis obat. Obat mana yang paling anda rekomendasikan?
A. Meloksikam 1x15 mgB. Asam mefenamat 3x500 mgC. Metikobalamin 3x500 mcgD. Parasetamol 3x650 mgE. Amitriptilin 1x12,5 mg
Hasil EKG menunjukkan VES jarang, HHD, dan iskemik anterior. Obat mana yang anda
rekomendasikan ?
A. Gabapentin 2x75 mg B. Tramadol 2x50 mgC. Metikobalamin 3x500 mcgD. Parasetamol 3x650 mgE. Amitriptilin 1x12,5 mg
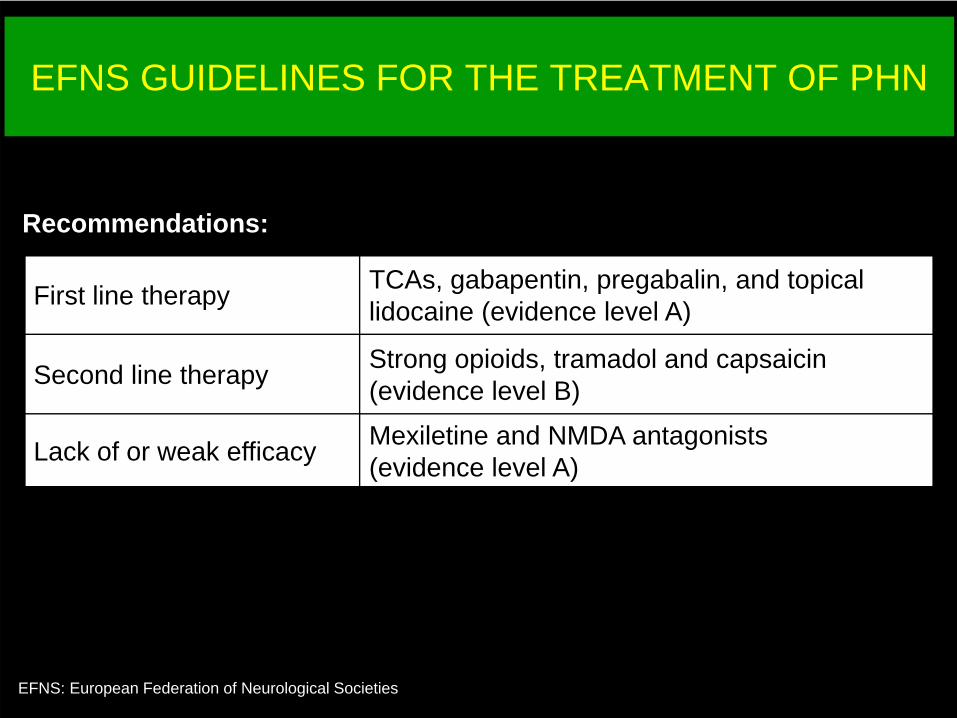
EFNS GUIDELINES FOR THE TREATMENT OF PHN
EFNS: European Federation of Neurological Societies
First line therapy TCAs, gabapentin, pregabalin, and topical lidocaine (evidence level A)
Second line therapy Strong opioids, tramadol and capsaicin (evidence level B)
Lack of or weak efficacy Mexiletine and NMDA antagonists(evidence level A)
Recommendations:
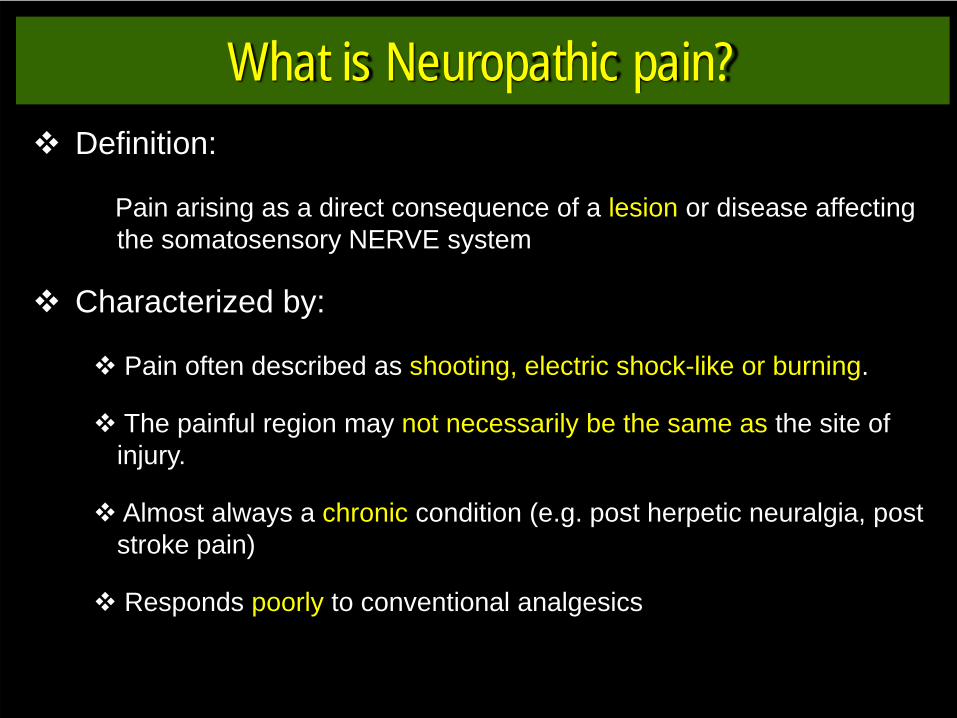
What is Neuropathic pain?Definition:
Pain arising as a direct consequence of a lesion or disease affecting the somatosensory NERVE system
Characterized by:
Pain often described as shooting, electric shock-like or burning.
The painful region may not necessarily be the same as the site of injury.
Almost always a chronic condition (e.g. post herpetic neuralgia, post stroke pain)
Responds poorly to conventional analgesics
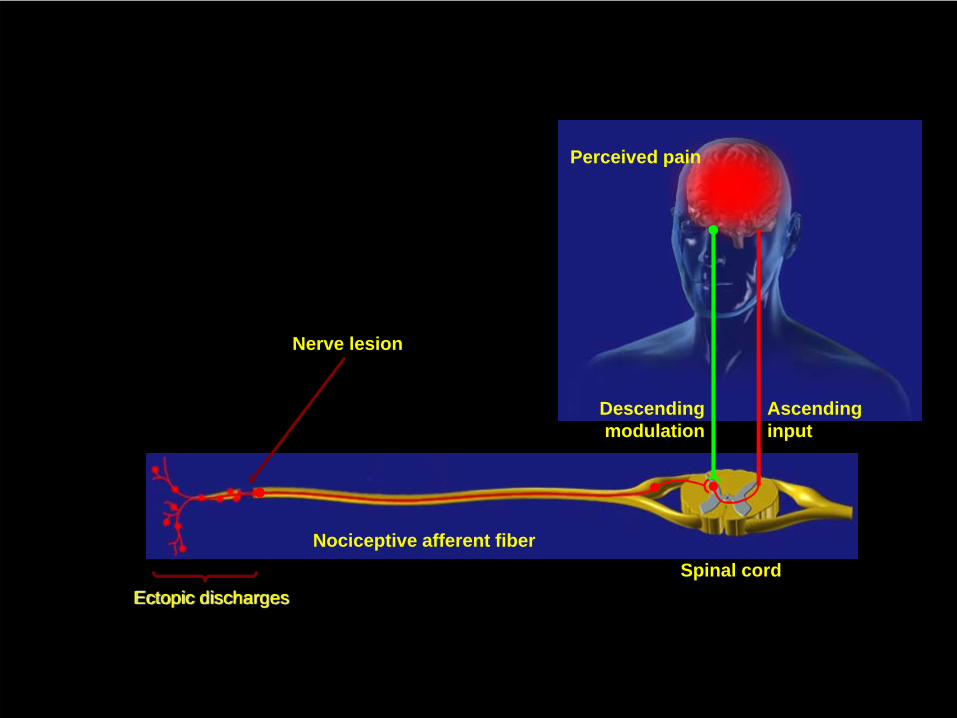
Ectopic discharges
Nerve lesion
Spinal cordNociceptive afferent fiber
Descendingmodulation
Ascendinginput
Perceived pain
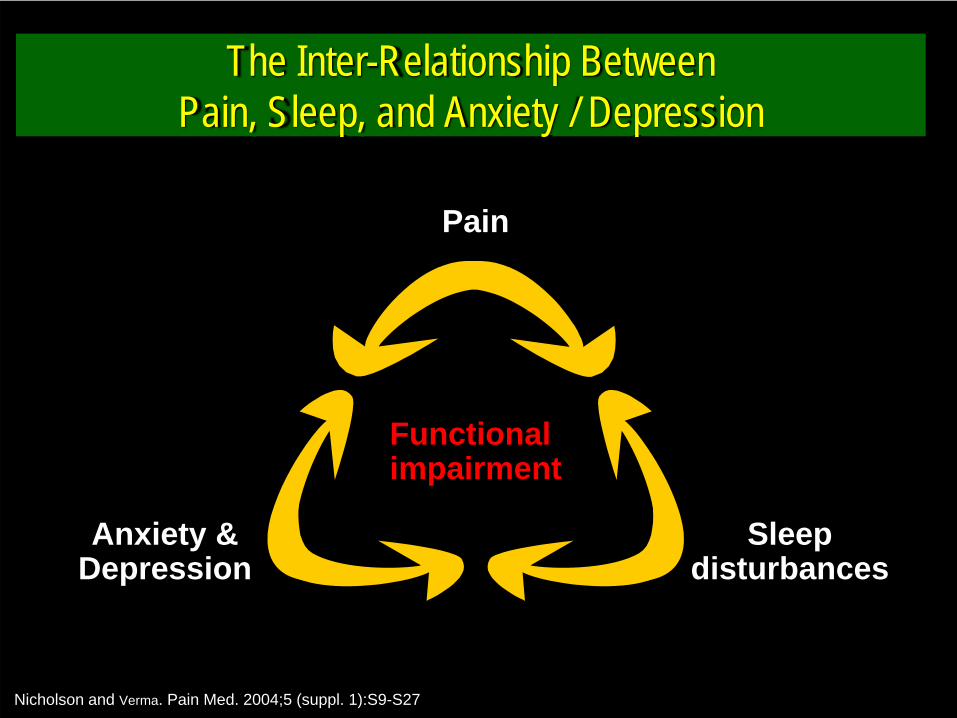
The Inter-Relationship Between Pain, Sleep, and Anxiety / Depression
Nicholson and Verma. Pain Med. 2004;5 (suppl. 1):S9-S27
Pain
Sleepdisturbances
Anxiety &Depression
Functional impairment
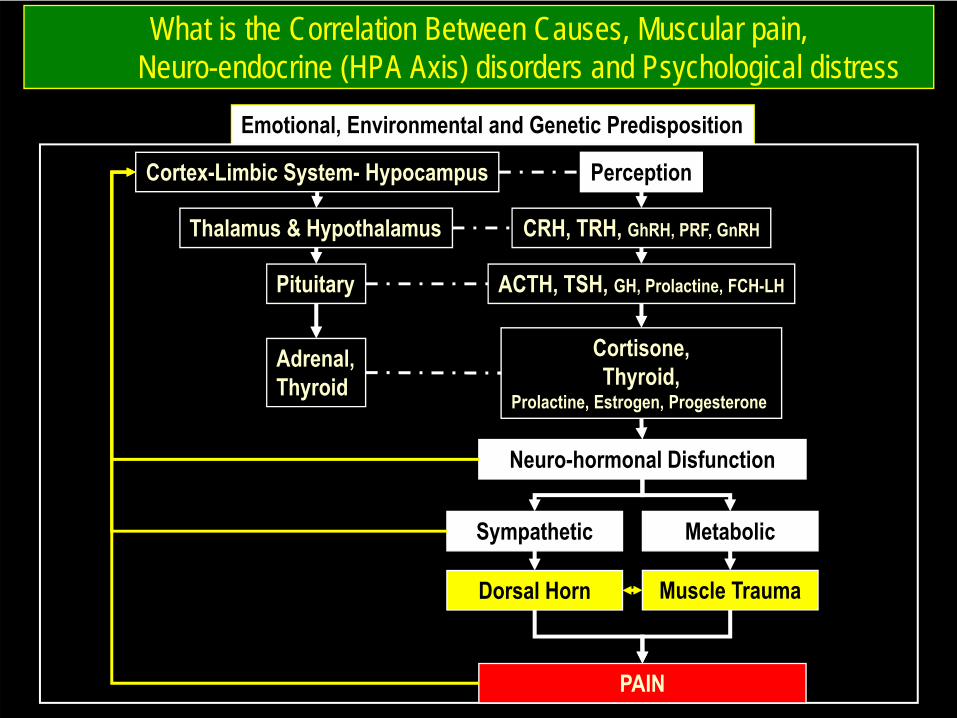
What is the Correlation Between Causes, Muscular pain, Neuro-endocrine (HPA Axis) disorders and Psychological distress
Emotional, Environmental and Genetic Predisposition
Cortex-Limbic System- Hypocampus
Thalamus & Hypothalamus
Pituitary
Adrenal,Thyroid
Perception
CRH, TRH, GhRH, PRF, GnRH
ACTH, TSH, GH, Prolactine, FCH-LH
Cortisone,Thyroid,
Prolactine, Estrogen, Progesterone
Neuro-hormonal Disfunction
Sympathetic Metabolic
PAIN
Muscle TraumaDorsal Horn
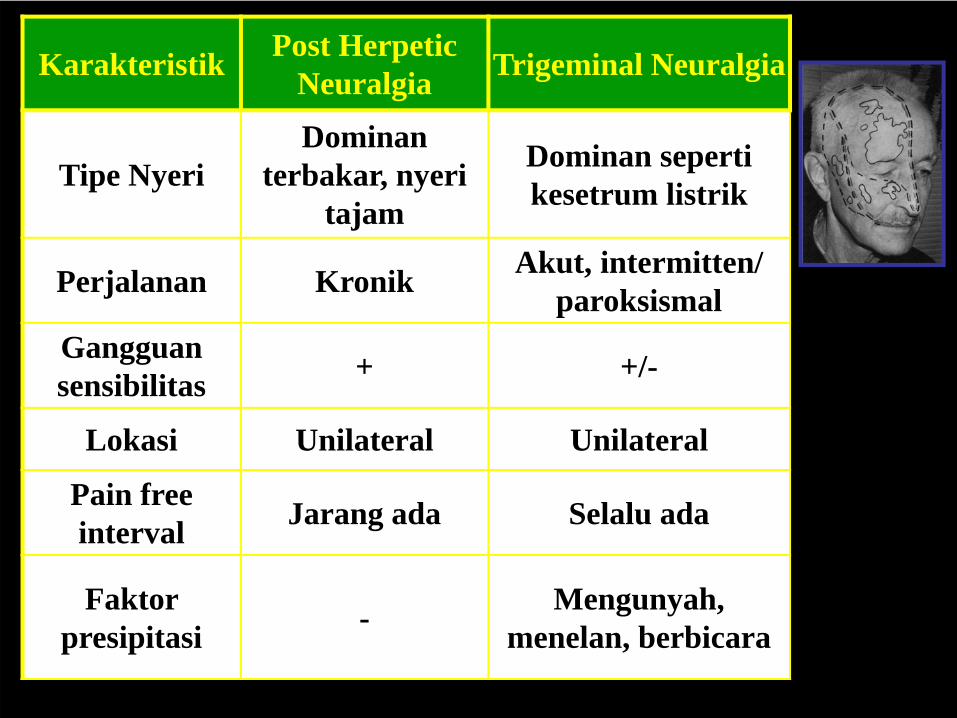
Karakteristik Post Herpetic Neuralgia Trigeminal Neuralgia
Tipe NyeriDominan
terbakar, nyeri tajam
Dominan seperti kesetrum listrik
Perjalanan Kronik Akut, intermitten/ paroksismal
Gangguan sensibilitas + +/-
Lokasi Unilateral Unilateral
Pain free interval Jarang ada Selalu ada
Faktor presipitasi - Mengunyah,
menelan, berbicara
Kasus 4 • Laki-laki, 60 tahun penderita Ca prostat, mengeluhkan
nyeri sangat hebat di tulang belakang, dirasakanseperti ditusuk-tusuk, dan kadang seperti terbakar.NPS 9. Nyeri ini muncul sejak sekitar 1 tahun yang lalusaat pasien pertama kali didiagnosis menderitakeganasan prostat. Nyeri ini dirasakan hilang timbulnamun semakin lama semakin berat dan konstan.Pemeriksaan neurologis didapatkan gangguan BABdan BAK, dengan anestesi dermatom L5S1.Pemeriksaan lab menunjukkan kadar PSA 125 mg/dldengan Ro terlampir.
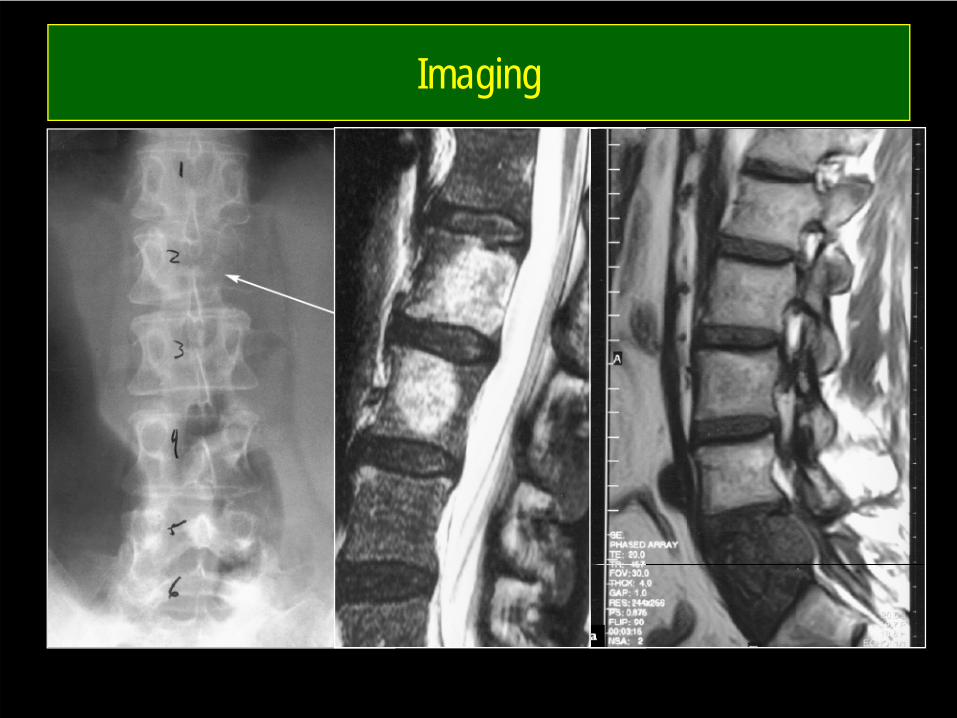
Imaging
Terapi yang paling anda pilih:
A. Tramadol 50 mg poB. Morfin sulfat 10 mgC. Risedronat sodium 60 mg D. Fentanil patch 25 mcgE. Ketorolac injeksi 1 amp
Primary or Metastatic Carcinoma
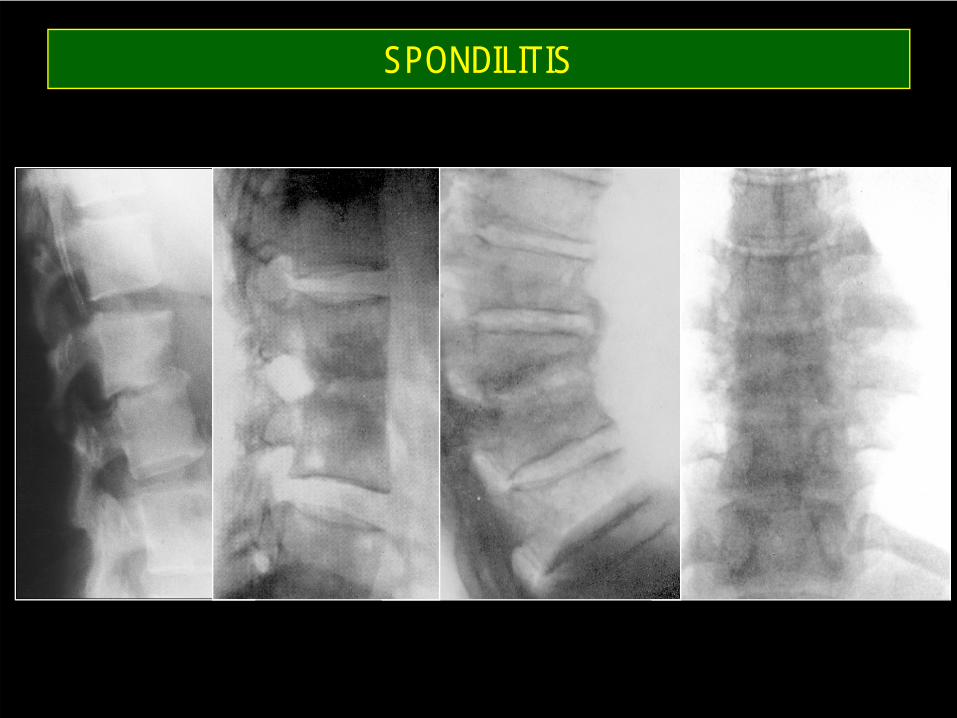
SPONDILITIS
Kasus 5 • Wanita 25 tahun, sekretaris, mengeluhkan nyeri kedua
tangan, sejak 8 HSMRS. dirasakan panas, tebal-tebaldan kemeng mulai dari sendi siku sampai dengantangan terutama pada jari telunjuk dan jari tengah.Tidak ada rasa tebal-tebal pada kelingking. NPS rata-rata 5. Rasa ini lebih parah pada saat tidur malam haribahkan menyebabkan pasien terbangun karena nyeri.Pekerjaan mengharuskan leher sering menunduk, dankadang-kadang merasakan nyeri leher terutama sorehari. Nyeri tekan epigastrium (-). Pemeriksaan fisik dbn.
Diagnosis yang paling mungkin?
A. HNP C5-6B. PolineuropatiC. MyelopathyD. MyalgiaE. Carpal tunnel syndrome
Nasehat Pertama ?
A. Splinting positionB. Tidak boleh angkat beratC. Kurangi makanan tinggi glukosaD. Tidak boleh makan tinggi kolesterolE. Minum obat secara teratur
Analgetik pilihan Anda:
A. Paracetamol 3x650 mgB. Metampiron 3x500 mgC. Tramadol 2x50 mgD. Paracetamol 325 mg + tramadol 33 mgE. Na-diclofenac 2x25 mg
Kombinasi terapi yang paling rasional?
A. Paracetamol+deksamethasonB. Na-diclofenac,
metilprednisolon+metikobalaminC. K-diclofenac + gabapentin +
metikobalaminD. Deksamethason injeksiE. Vit B injeksi, ketorolac injeksi
Terapi non farmakologi yang anda anjurkan:
A. Operasi dekompresiB. Fisioterapi exercise C. Ultrasound dan diatermiD. Layar komputer kerja sejajar mata
sehingga tidak menunduk saat kerjaE. Bedrest
CTS
• Normal pressure : 0–5mm Hg 30mm Hg at rest in CTS, and is 90mm Hg with wrist flexion or extension in patients with CTS.
• • Classic symptoms : – night pain that wakes the patient from sleep, – pain with maximal wrist flexion or extension, – decreased grip strength, and decreased
dexterity.
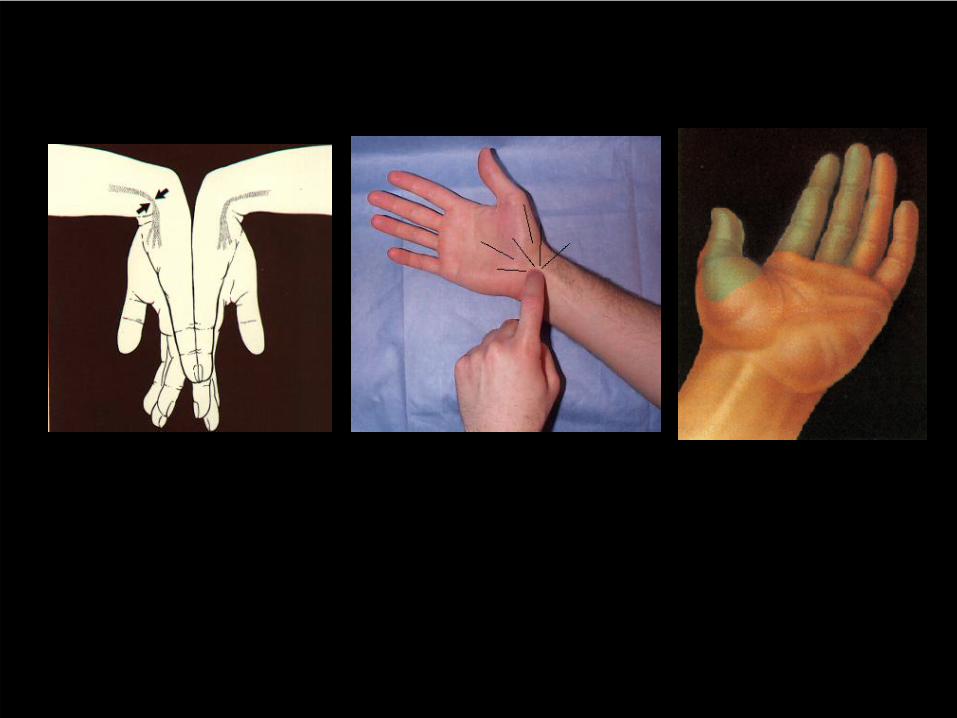
Summary of Tests
Test Sensitivity SpecificityPhalen’s 75% 62%Tinel’s 64% 71%Compression 87% 90%
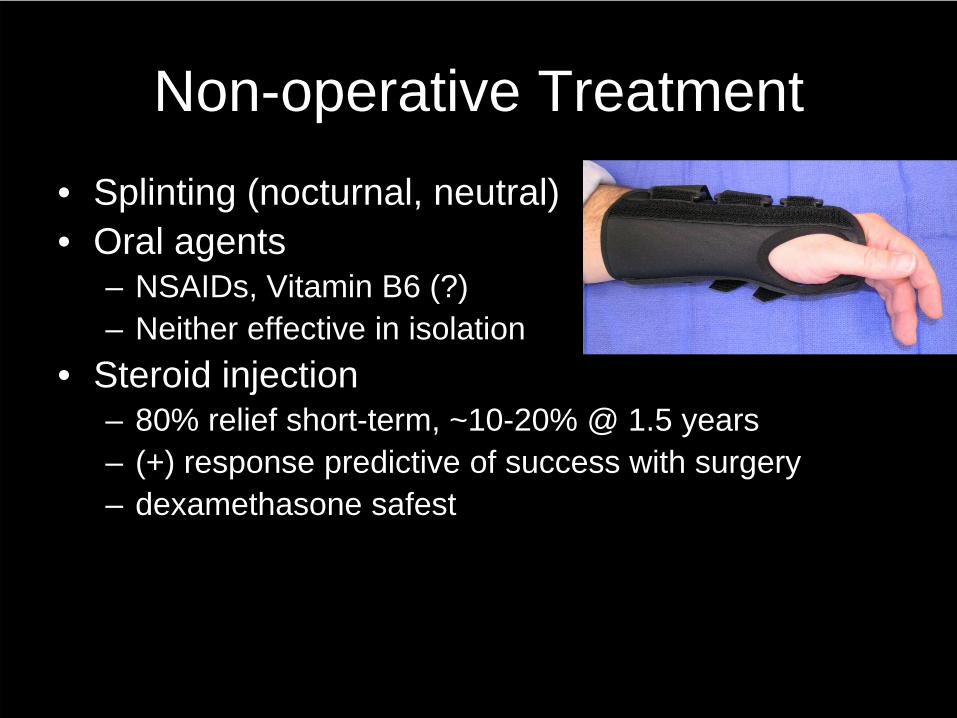
Non-operative Treatment• Splinting (nocturnal, neutral)• Oral agents
– NSAIDs, Vitamin B6 (?)– Neither effective in isolation
• Steroid injection– 80% relief short-term, ~10-20% @ 1.5 years– (+) response predictive of success with surgery– dexamethasone safest
Summary
• CTS is a clinical diagnosis– ED are confirmatory
• Non-operative treatment early• Operative treatment
– if denervation of APB– failure of non-operative treatment
Kasus 6
• Mahasiswi, 20 tahun datang dengan keluhan nyerikepala berdenyut, sejak 3 hari yang lalu, terutamadi frontal dan temporal. Pemeriksaan fisik danneurologis tidak ditemukan abnormalitas.Gangguan penglihatan (-). Pada pemeriksaan NPSberkisar 8. Pasien merasakan silau jika melihatsinar. Pasien sedang mengalami faringitis sejak 1hari , dan ada rasa mual.
Diagnosis yang paling mungkin
A. Migraine headacheB. Cluster headacheC. Tension type headacheD. Nyeri kepala terkait infeksi/inflamasiE. Galucoma
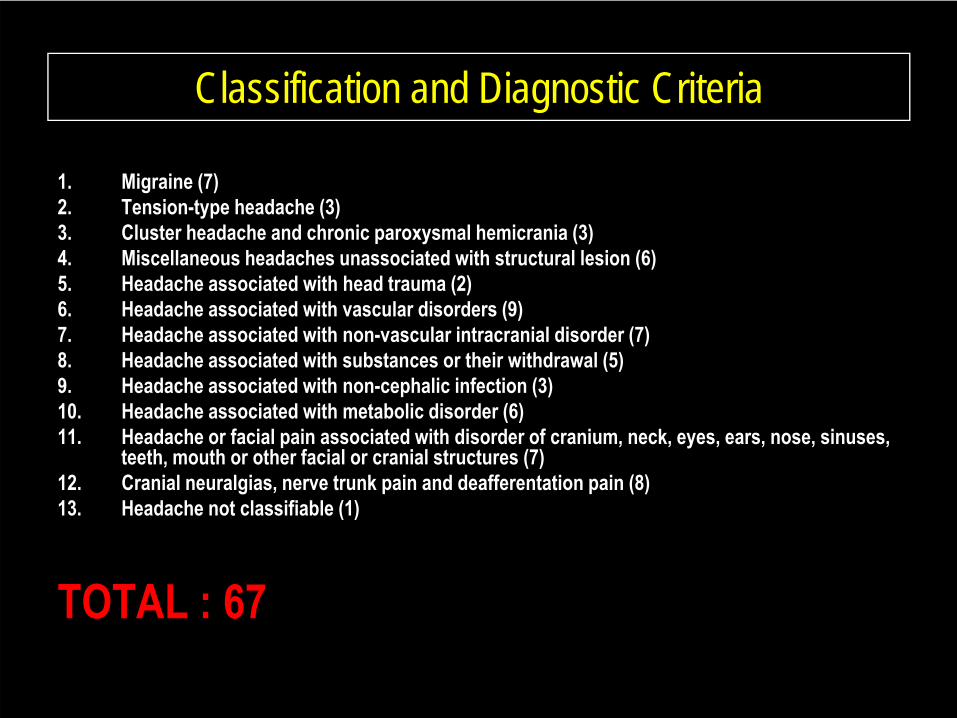
Classification and Diagnostic Criteria
1. Migraine (7)2. Tension-type headache (3)3. Cluster headache and chronic paroxysmal hemicrania (3)4. Miscellaneous headaches unassociated with structural lesion (6)5. Headache associated with head trauma (2)6. Headache associated with vascular disorders (9)7. Headache associated with non-vascular intracranial disorder (7)8. Headache associated with substances or their withdrawal (5)9. Headache associated with non-cephalic infection (3)10. Headache associated with metabolic disorder (6)11. Headache or facial pain associated with disorder of cranium, neck, eyes, ears, nose, sinuses,
teeth, mouth or other facial or cranial structures (7)12. Cranial neuralgias, nerve trunk pain and deafferentation pain (8)13. Headache not classifiable (1)
TOTAL : 67(Silberstein & Young, 2005)
BACKGROUNDHEADACHE
Primary Secondary
headache condition itself is the problem, and no
underlying or dangerouscause for it can be identified. The classification is based on
symptom profiles
headache are related to other conditions, and a
'secondary symptom'. They are classified according to their causes (e.g. vascular,
psychiatric, etc.).
Bajwa & Wootton, 209
History and examination• No ‘gold standard’ tests or biologic markers exist• A good history is the key to diagnosis. • Examination is usually normal in patients with primary
headache.• A systematic case history single most important
diagnosis, future work-up and treatment plan. • focus the physical examination and prevent
unnecessary investigation and imaging studies
Consider a diagnosis of migraine
• Patients with recurrent severe disabling headaches associated with nausea and sensitivity to light, and with a normal neurological examination (C).
Consider a diagnosis of tension-type headache
• in patients with recurrent, non-disabling bilateral headache and a normal neurological examination (C).
Consider the diagnosis of a trigeminal autonomic cephalalgia (cluster headache, paroxysmal hemicrania, short lived
unilateral neuralgiform headache with conjunctival injection and tearing (SUNCT))
• in patients with frequent, brief, unilateral headaches in a trigeminal distribution with ipsilateral cranial autonomic features (D)
New daily persistent headache
• Cresendo pattern in daily: exclude secondary causes (such as subarachnoid haemorrhage, meningitis, raised intracranial pressure, low pressure headache, giant cell arteritis) (D).
Investigation
• Neuroimaging is not indicated in patients who have a clear history of migraine, no “red flag” features, and a normal neurological examination(D).
• In stable migraine only 0.2% have relevant abnormalities on neuroimaging.
• Both magnetic resonance imaging and computed tomography can identify incidental abnormalities that may result in patient anxiety as well as dilemmas in practical and ethical management.
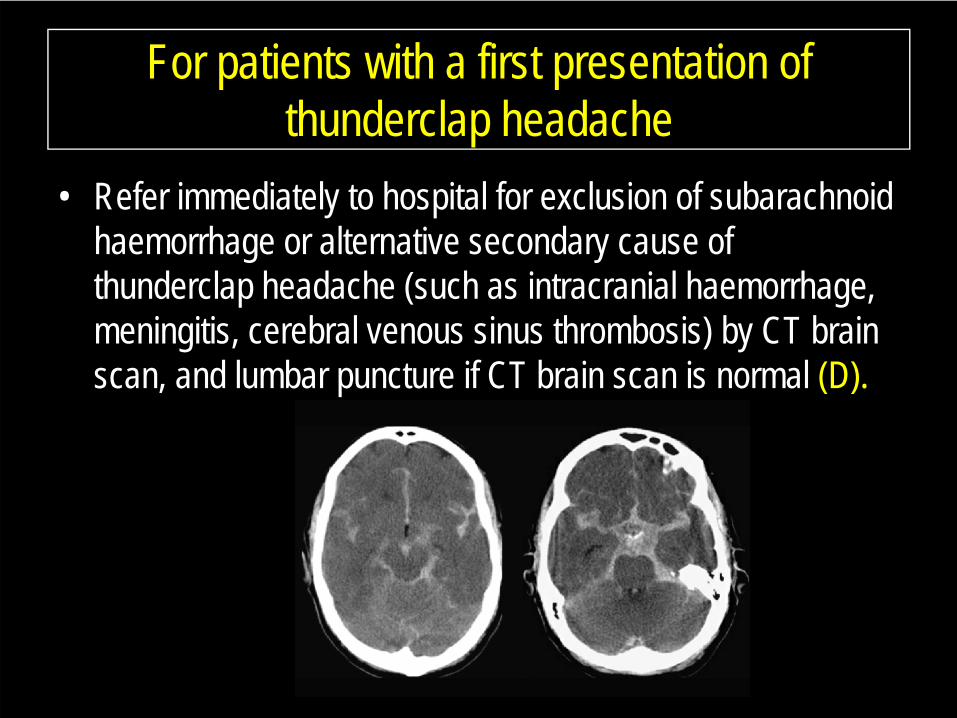
For patients with a first presentation of thunderclap headache
• Refer immediately to hospital for exclusion of subarachnoid haemorrhage or alternative secondary cause of thunderclap headache (such as intracranial haemorrhage, meningitis, cerebral venous sinus thrombosis) by CT brain scan, and lumbar puncture if CT brain scan is normal (D).
• The following are warning signs or “red flags” for potential secondary headache, based on observational studies (D): – new headache in a patient aged over 50; – thunderclap onset (that is, abrupt and severe); – focal and non-focal symptoms; – abnormal signs; – headache changing with posture;– valsalva headache (headache triggered by valsalva-type
manoeuvres such as coughing, sneezing, bending, heavy lifting, straining);
– fever– history of HIV; – cancer
Investigation
Indications for imaging studies• AAN, AAFP, ASIM:
– Patients with danger signs.– Non-acute headache and an unexplained abnormal finding on
neurologic examination. – In the remaining patients remain one of clinical judgment
• increased severity of symptoms or resistance to appropriate drug therapy;
• change in characteristics or pattern of headache• family history of an intracranial structural lesion
Bajwa & Wootton, 209
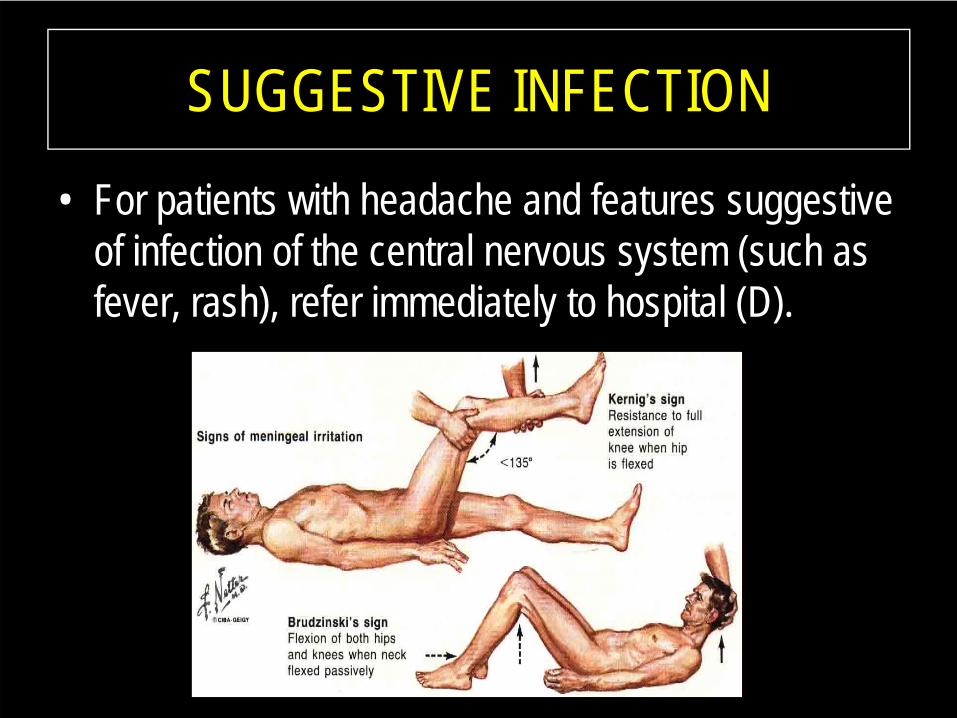
SUGGESTIVE INFECTION
• For patients with headache and features suggestive of infection of the central nervous system (such as fever, rash), refer immediately to hospital (D).
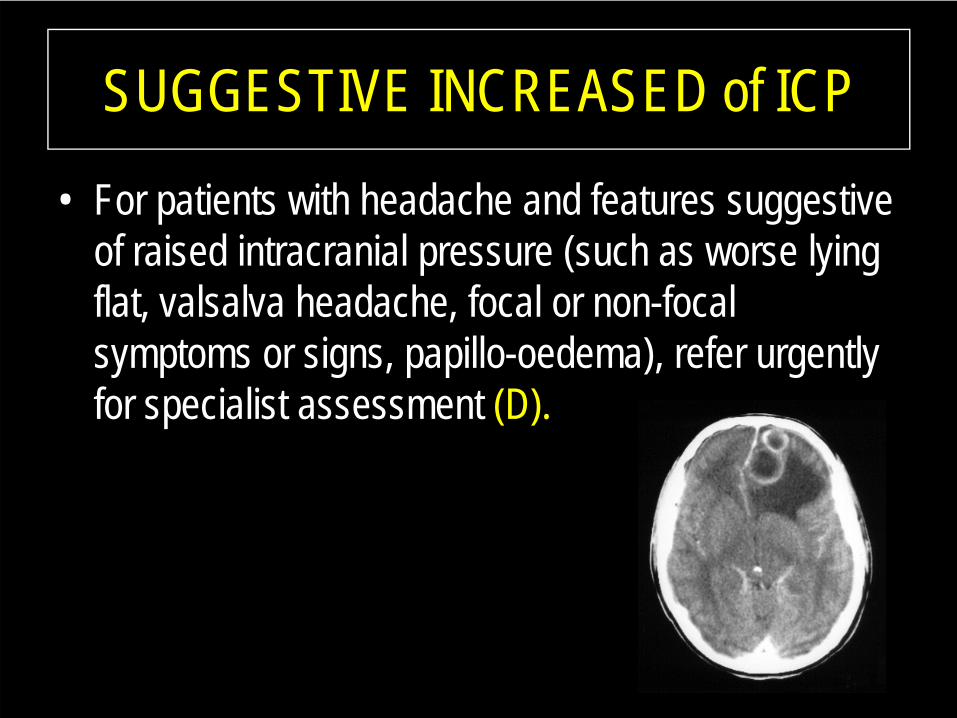
SUGGESTIVE INCREASED of ICP
• For patients with headache and features suggestive of raised intracranial pressure (such as worse lying flat, valsalva headache, focal or non-focal symptoms or signs, papillo-oedema), refer urgently for specialist assessment (D).
Consider intracranial hypotension
• in all patients with headache developing or worsening after assuming an upright posture (D).
• Refer such patients to a neurologist or headache clinic for specialist assessment (D)
Consider giant cell arteritis
• in any patient over the age of 50 presenting with a new headache or change in headache, and check erythrocyte sedimentation rate and C reactive protein levels (D).
SUMMARY• The appropriate evaluation of headache complaints includes the
following: – Rule out "Danger signs“. – Determine the type of primary headache using the patient history
as the primary diagnostic tool. – There may be overlap in symptoms (migraine and tension-type
headache; migraine and some secondary causes of headache (such as sinus disease)).
– An imaging study is warranted in "Indications for imaging studies“