capd : pemilihan pasien,persiapan dan insersi kateter atma gunawan - kapan dan bagaimana... ·...
TRANSCRIPT
CAPD : pemilihan pasien,persiapan
dan insersi kateter
Atma Gunawan
Consultant Nephrologist
RSSA Malang
Pilihan terapi pengganti gagal ginjal
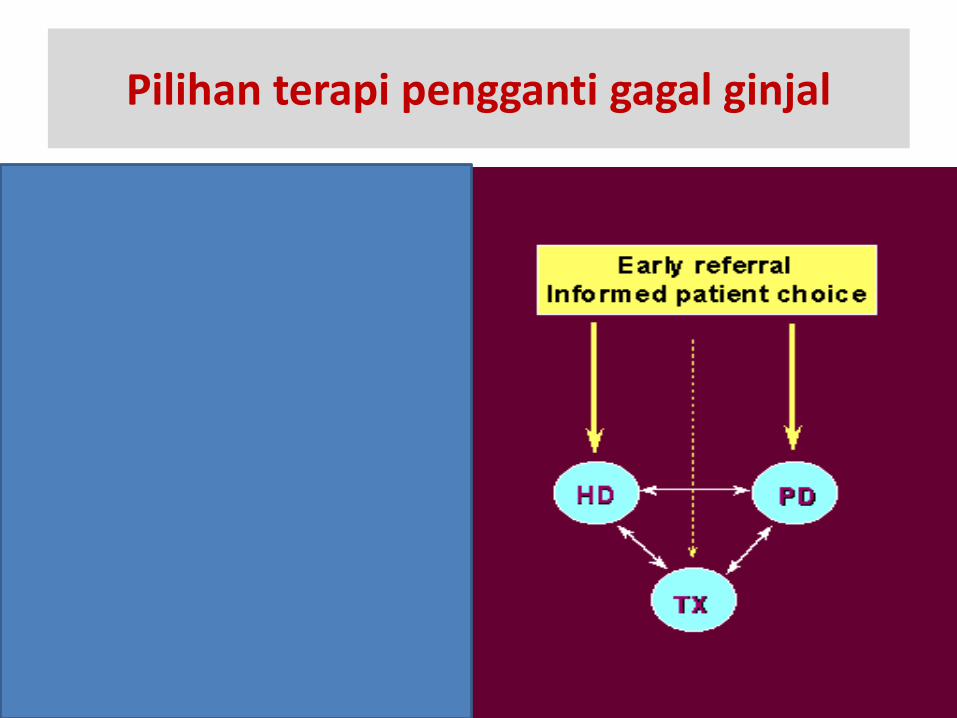
Pilihan terapi pengganti gagal ginjal
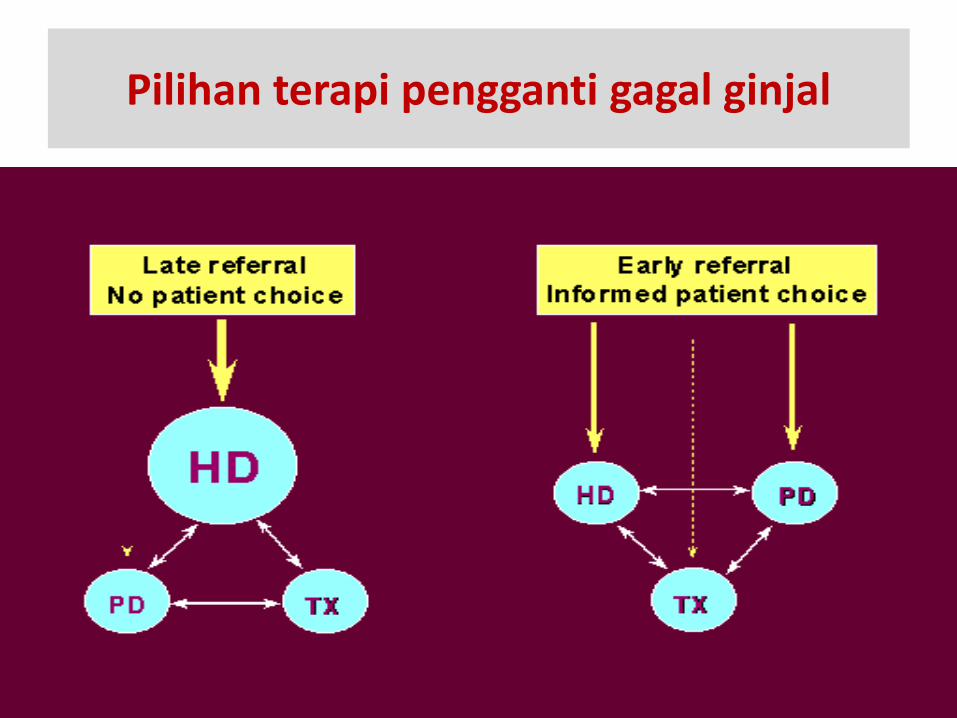
CAPD (continous ambulatory peritoneal dialysis)
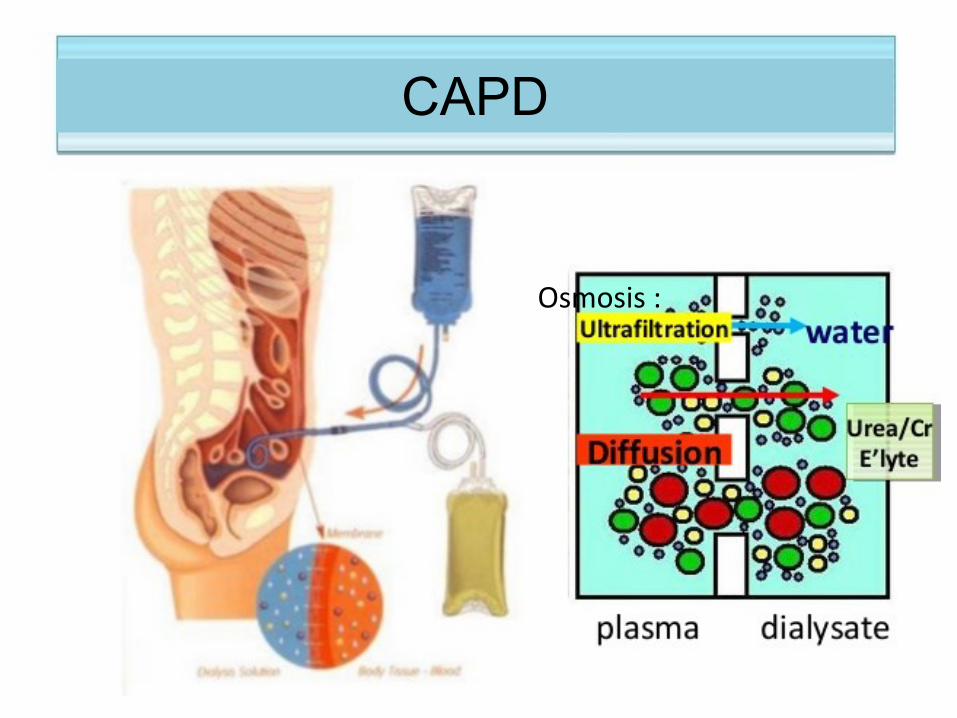
CAPD
Osmosis :
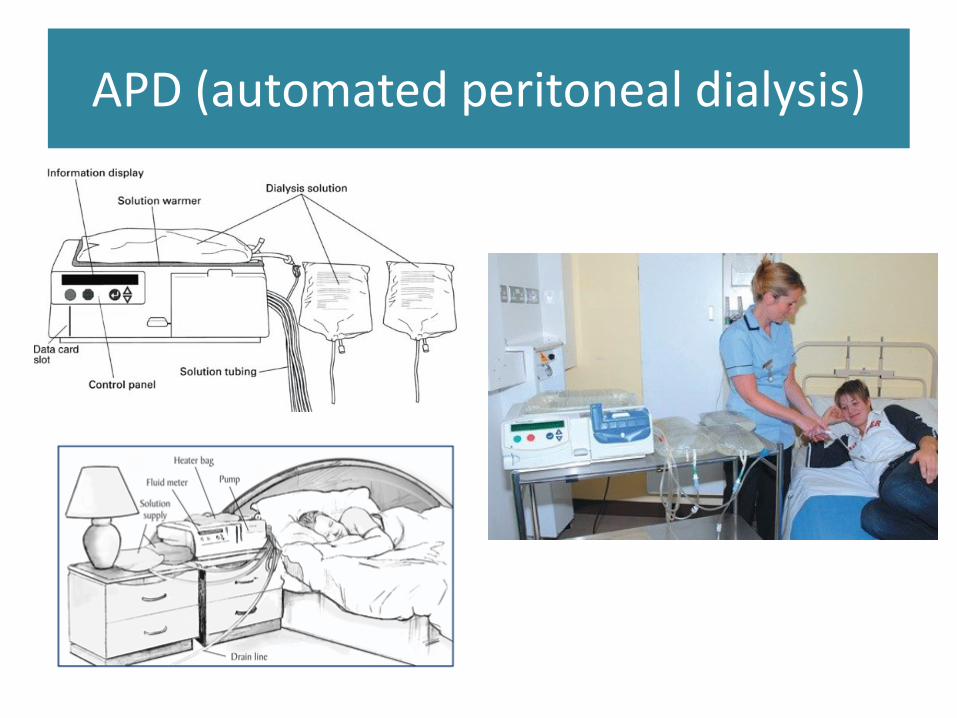
APD (automated peritoneal dialysis)
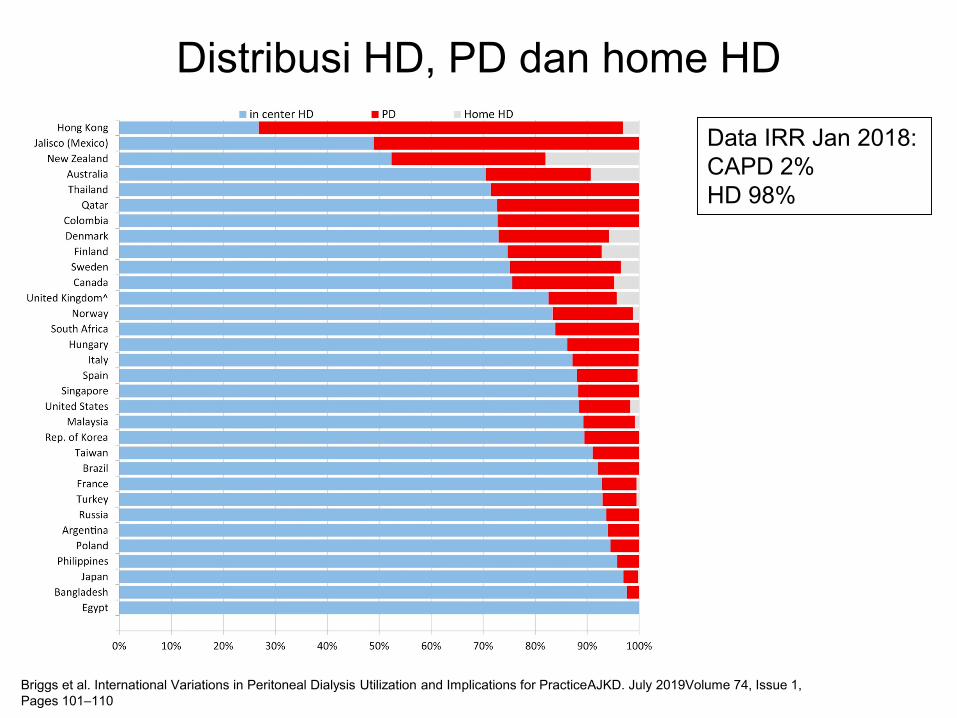
Distribusi HD, PD dan home HD
Briggs et al. International Variations in Peritoneal Dialysis Utilization and Implications for PracticeAJKD. July 2019Volume 74, Issue 1,
Pages 101–110
Data IRR Jan 2018:
CAPD 2%
HD 98%

PLB
CAPD Data per Des 2018
15
45 17
40
21
9
21
70
68
78
22
16
13
CAPD Px
Mapping
75
30
57
360
54
88
179
496
22
46
Solo
61
202
RSSA
Malang

ESRD ’S PATIENT (SEPT 2017)
Haemodialysis
CAPD
Renal Transplant
N = 688 (70%)
N = 296 (30%
N = 15 (1.5%)
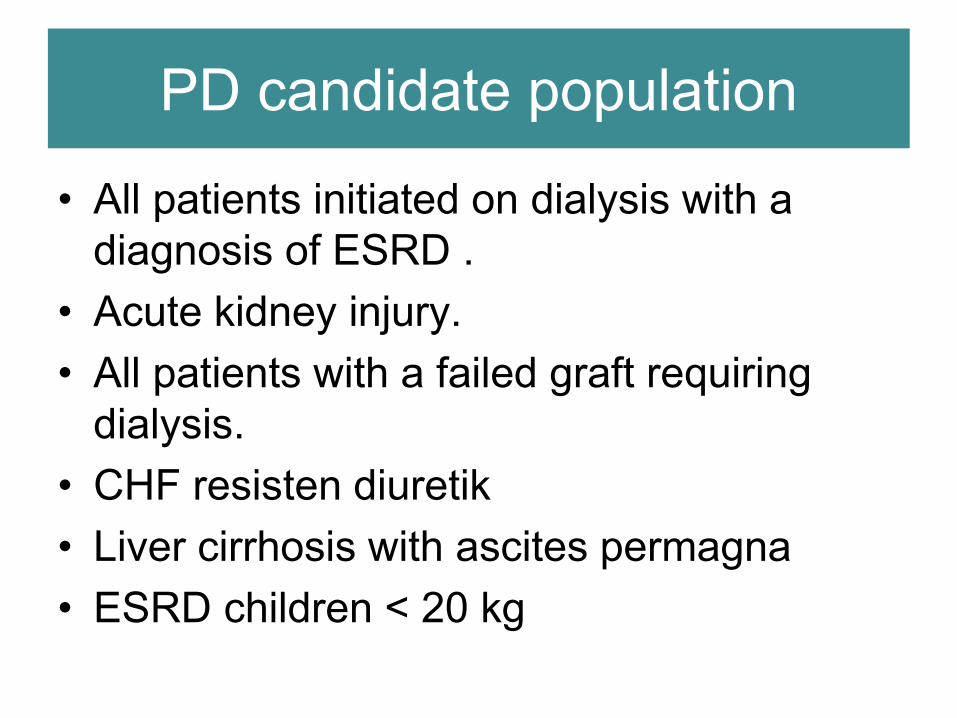
PD candidate population
• All patients initiated on dialysis with a
diagnosis of ESRD .
• Acute kidney injury.
• All patients with a failed graft requiring
dialysis.
• CHF resisten diuretik
• Liver cirrhosis with ascites permagna
• ESRD children < 20 kg

Surgical Contraindications to CAPD
• Absolute :
- severe peritoneal adhesions
- inflammatory bowel disease
- sepsis of anterior abdominal wall
- large unrepairable hernia of abdominal wall
• Relative :
- previous extensive pelvic or low abdominal surgery
- colostomy or ileostomy
- bleeding tendency
- post peritonitis
Benefit on PD ?
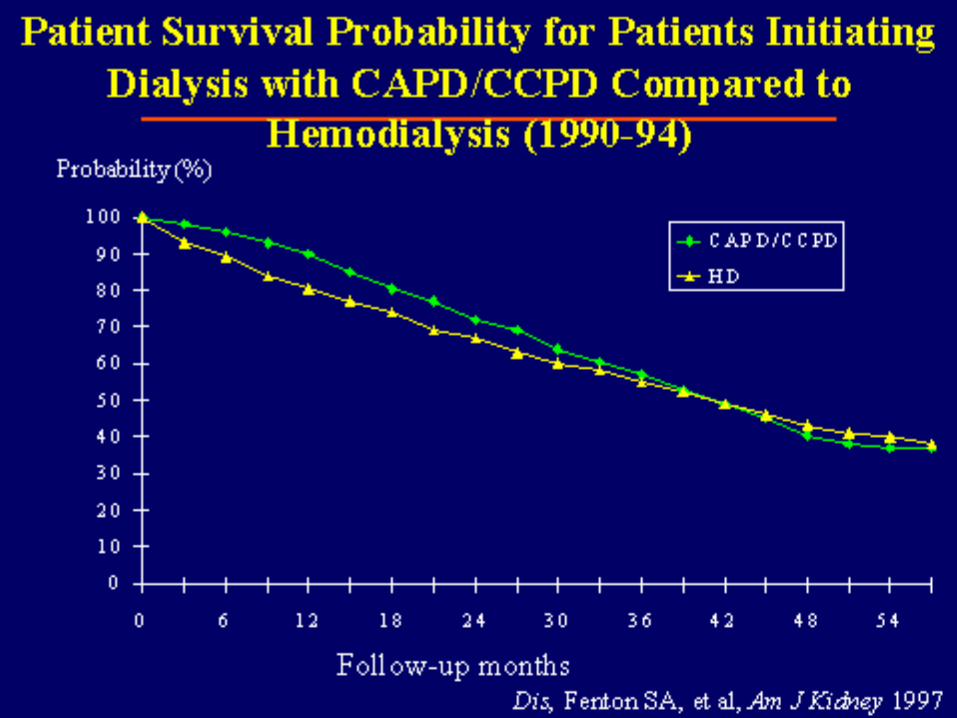
• Survival awal lebih baik
• Biaya lebih murah
• Preservasi RRF
• Logistik !
• Risiko hepatitis lebih rendah
• Clearance terhadap toxin makromolekul lebih baik
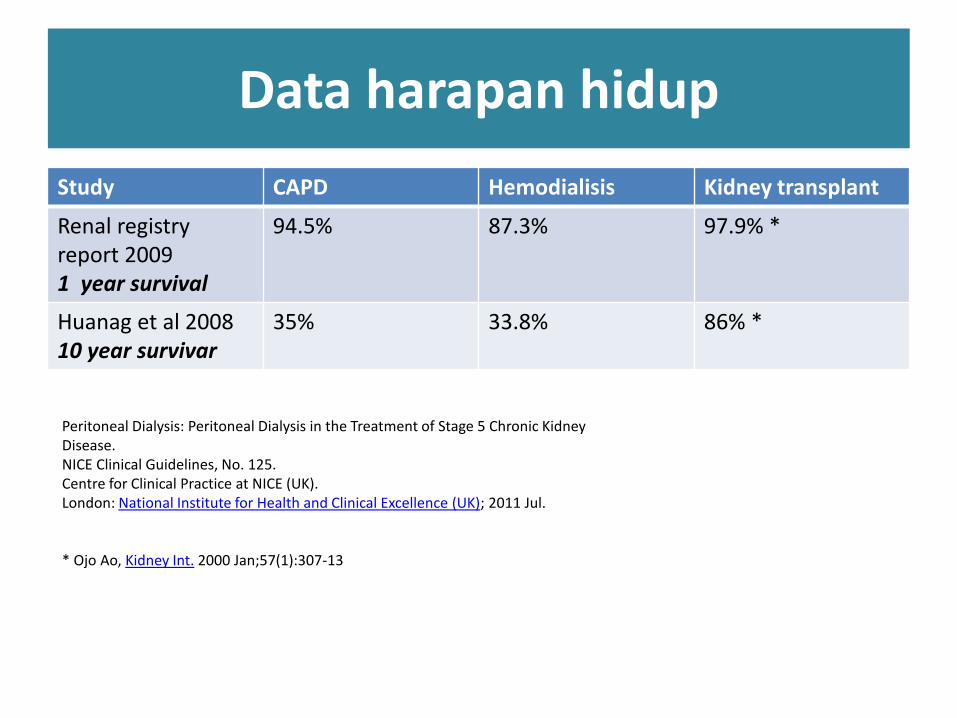
Data harapan hidup
Study CAPD Hemodialisis Kidney transplant
Renal registry report 20091 year survival
94.5% 87.3% 97.9% *
Huanag et al 200810 year survivar
35% 33.8% 86% *
Peritoneal Dialysis: Peritoneal Dialysis in the Treatment of Stage 5 Chronic Kidney Disease.NICE Clinical Guidelines, No. 125.Centre for Clinical Practice at NICE (UK).London: National Institute for Health and Clinical Excellence (UK); 2011 Jul.
* Ojo Ao, Kidney Int. 2000 Jan;57(1):307-13

Perbandingan biaya (mandiri)
Biaya 1x HD = Rp 879.000,-
Biaya HD perbulan (12x) =
Rp 10.548.000.-
NB; InaCBGs HD RSUD tipe
B
120 kantong CAPD bag
perbulan = Rp 7.500.000
Transplantasi ginjal RSUD
tipe A Rp 415.365.800 +
obat RP 50 jt satu tahun
pertama

Pembiayaan Mandiri 1 Pasien gagal ginjal kronik/ESRD
TahunKe-
KumulatifBiaya Hemodialisa
KumulatifBiaya C A P D
Kumulatif BiayaTransplantasi ginjal
1 93.600.000 79.200.000 300.000.000
2 187.200.000 158.400.000 330.000.000
3 280.800.000 237.600.000 360.000.000
4 374.400.000 316.800.000 390.000.000
5 468.000.000 396.000.000 410.000.000
6 561.600.000 475.200.000 440.000.000
7 655.200.000 554.400.000 470.000.000
8 936.000.000 633.600.000 500.000.000
9 1.029.600.000 712.800.000 530.000.000
10 1.123.200.000 792.000.000 560.000.000
HD = 1 pasien x 12/bulan x 650.000, CAPD 12 x 6.600.000, Renal transplant : biaya op 250.000.000, thn 1 obat 50 jt, tahun ke dua dan seterusnya obat 30 jt per tahun (RSSA)
HD 12x/bl ; CAPD 4 bag/hari


Clearance by normal kidneys HD and CAPD
Cle
aran
ce (
L/w
k)
0
200
400
600
800
1000
Kidney Hd CAPD
MW
Inulin 5200
Creatinine 113
Urea 60
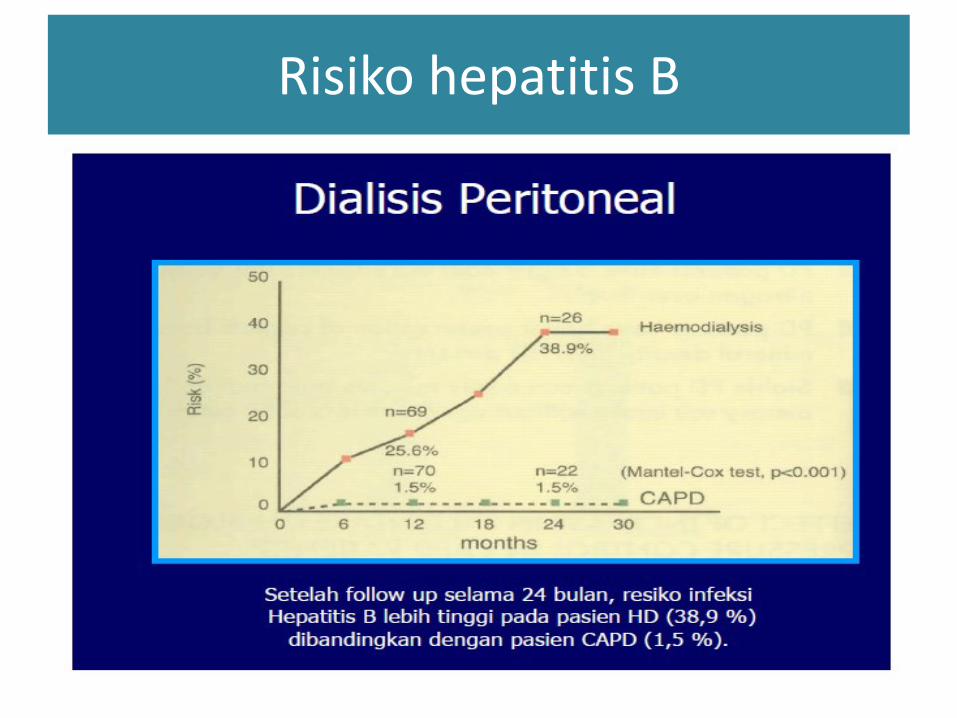
Risiko hepatitis B

Keuntungan segi logistik
• HD : 1 nurse per 3 pasien
PD : 1 nurse per 50 pasien
• Rasio kebutuhan bangunan terhadap pasien sangat kecil !
• Biaya transportasi sedikit

Methode Seldinger
technique
Peritoneuscopic Minilaparotomy Laparoscopic
Done by Nephrologist Nephrologist Surgeon/nephrolo
gist
Surgeon/nephrolo
gist
Setting Clean side-room Clean side-
room/operating
theater
Operating theater Operating theater
Anesthesia Local anesthesia Local/general
anesthesia
Local/general
anesthesia
General anesthes
Pros (i) Short learning
time
(ii) Low
complication rates
(i) Direct
visualization of
Peritoneum
(ii) Low leakage
rates
(i) Direct
visualization of
peritoneum
(ii) Allow purse-
string suture of
peritoneum
(iii) Low leakage
rates
(iV) Can
omentectomy
(i) Visualization of
intra-abdominal
structures
(ii) Allow
adjunctive
procedures for
example
Adhesiolysis,
omentopexy
Cons Relatively high
early
leakage rates
Short learning
time
Long learning time Long learning time (i) Very long
learning time
(ii) High cost
(iii) Specialized
equipment
needed
International Journal of Nephrology Volume 2013, Article ID 940106
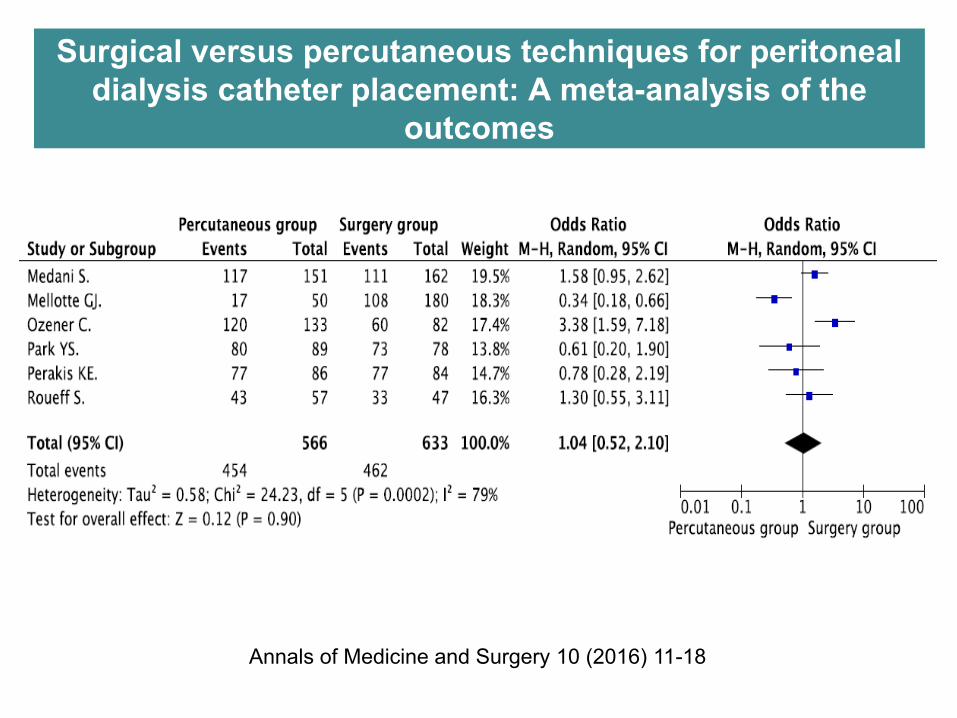
Surgical versus percutaneous techniques for peritoneal
dialysis catheter placement: A meta-analysis of the
outcomes
Annals of Medicine and Surgery 10 (2016) 11-18
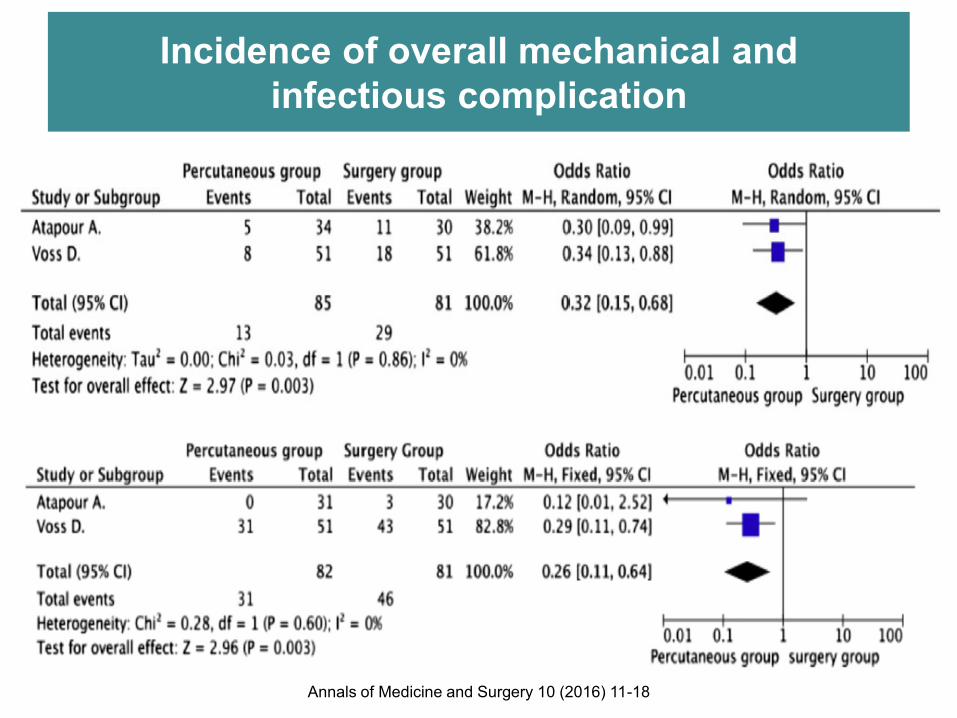
Incidence of overall mechanical and
infectious complication
Annals of Medicine and Surgery 10 (2016) 11-18

Who inserted PD catheter ?
KGH
Bedah umum
Bedah digestive
Bedah urologi

Competency of nephrologist consultant

Methode of insertion PD catheter

Methode of PD insertions by nephrologist
Methodes Hospital
Laparatomy RSSA (Malang) ; RSUD Zainul Abidin
(Banda Aceh)
Peritoneuscopic
Seldinger technique
RSSA (Malang)
RSSA (Malang) ; RSHS (Bandung),
RS Gatot Subroto (Jakarta) ; RSUP
M.Hoesin (Palembang)
• PD catheter inserted by nephrologist start on 2006.
• Started at Malang, by laparatomy methode
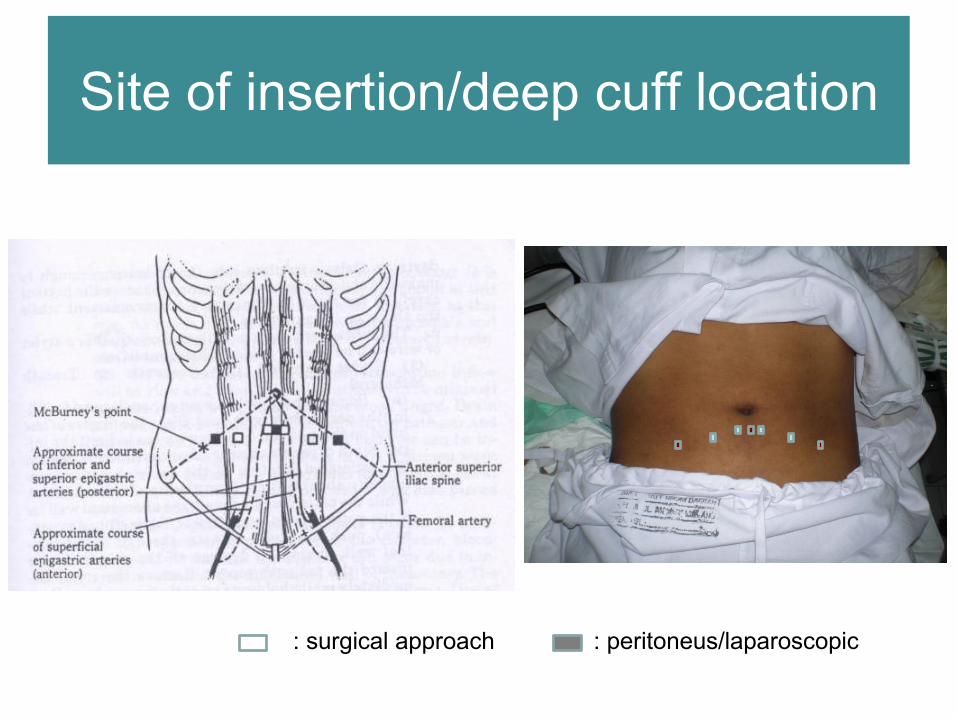
Site of insertion/deep cuff location
: surgical approach : peritoneus/laparoscopic

Catheter anatomy
Extra-Peritoneal
standard Tenckhoff
Swan neck
Cuff
double cuffs
single cuff
Intra-Peritoneal
straight
coiled tip
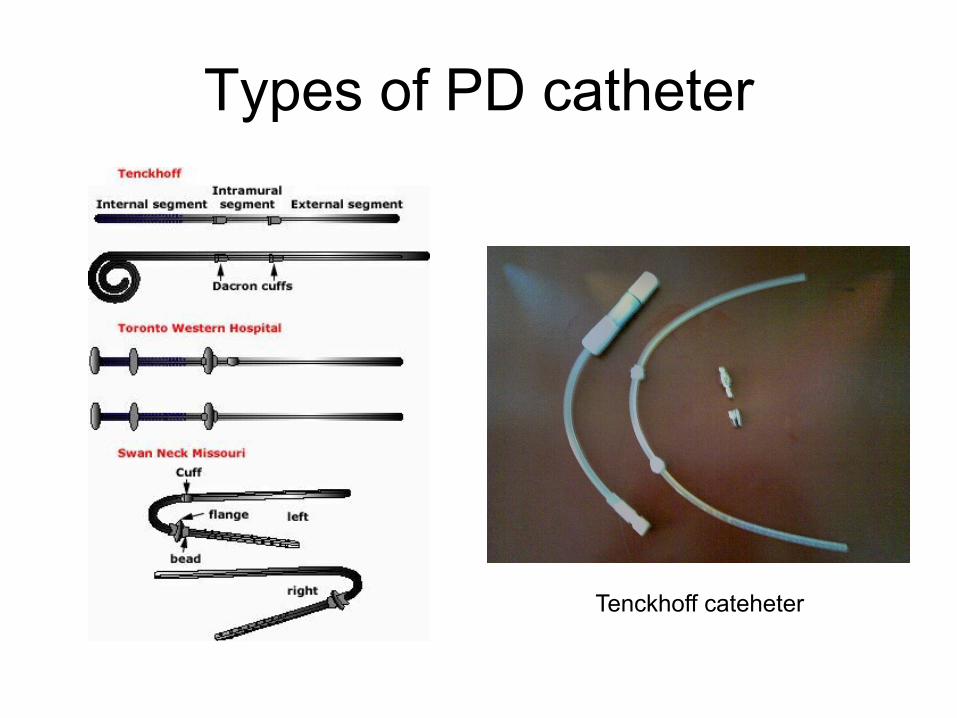
Types of PD catheter
Tenckhoff cateheter

Deep cuff location
• Deep cuff should be burried inside muscle or posterior fascia
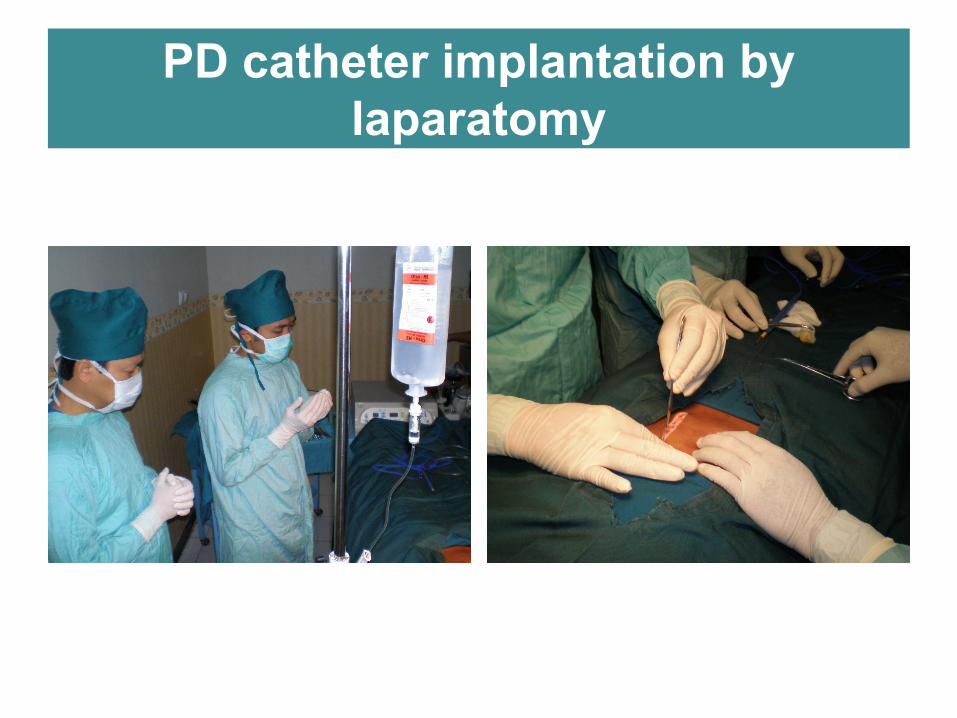
PD catheter implantation by
laparatomy
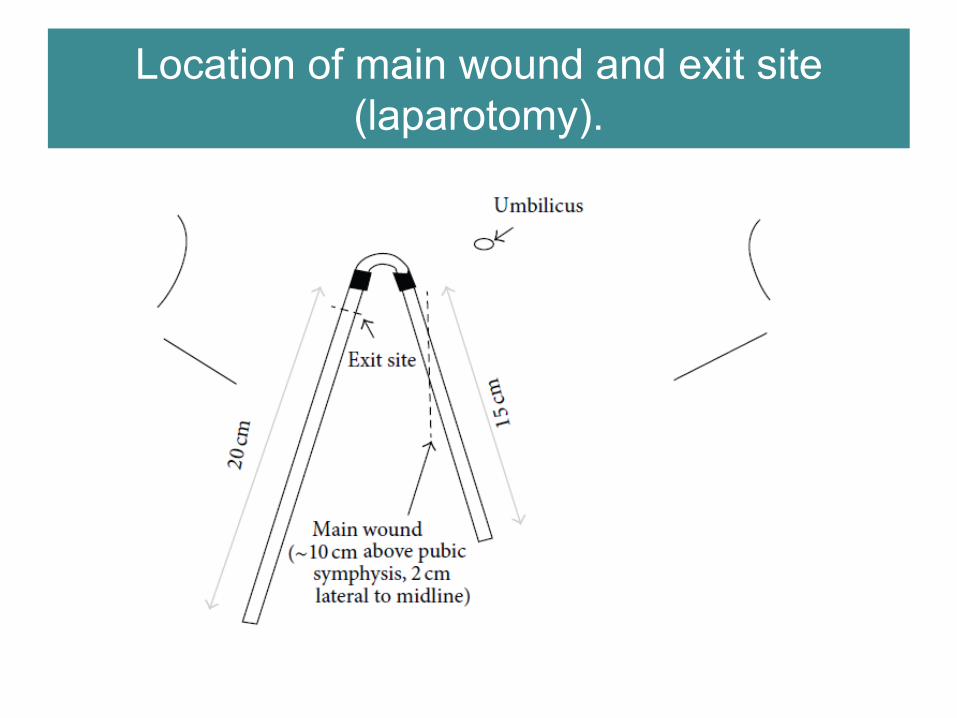
Location of main wound and exit site
(laparotomy).

Skin incision, the subcutaneous tissue is
dissected till the reach of the anterior
rectus sheath
The rectus muscle is bluntly split
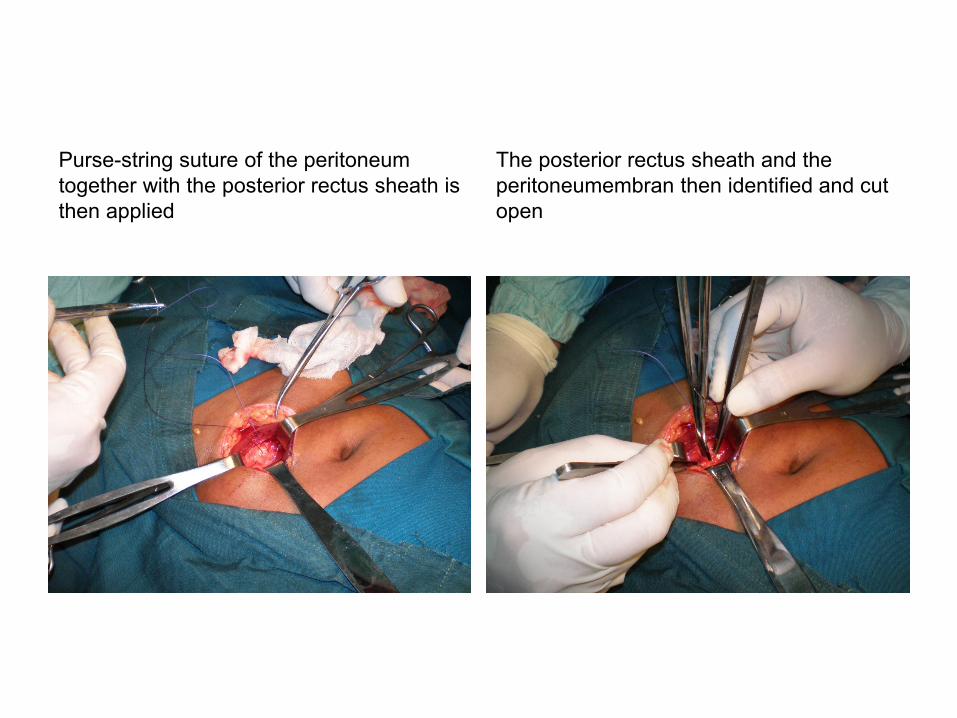
The posterior rectus sheath and the
peritoneumembran then identified and cut
open
Purse-string suture of the peritoneum
together with the posterior rectus sheath is
then applied
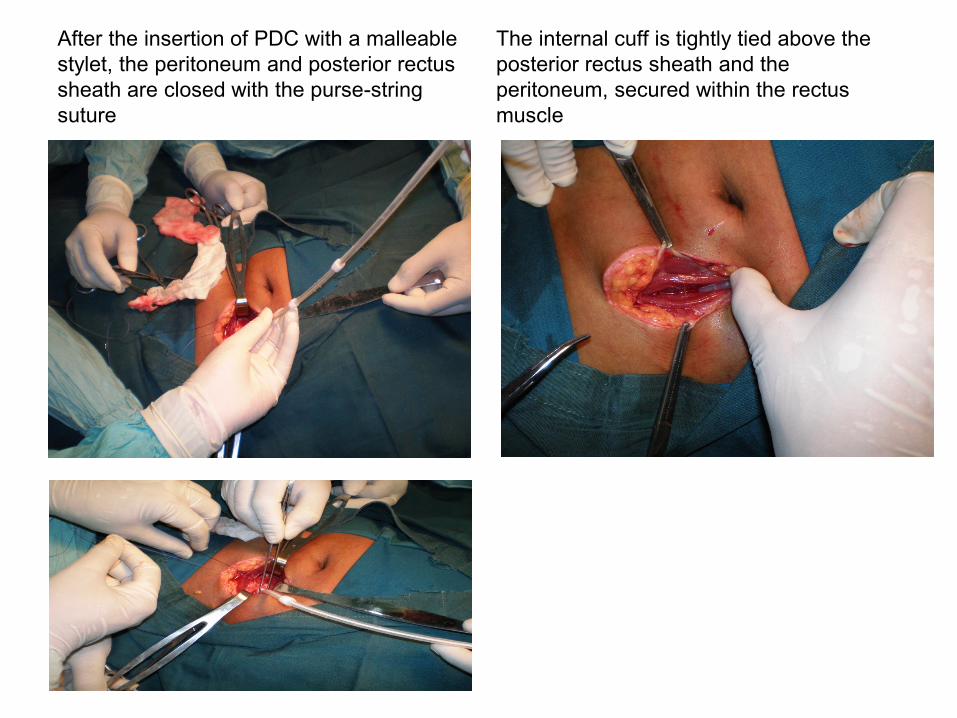
After the insertion of PDC with a malleable
stylet, the peritoneum and posterior rectus
sheath are closed with the purse-string
suture
The internal cuff is tightly tied above the
posterior rectus sheath and the
peritoneum, secured within the rectus
muscle
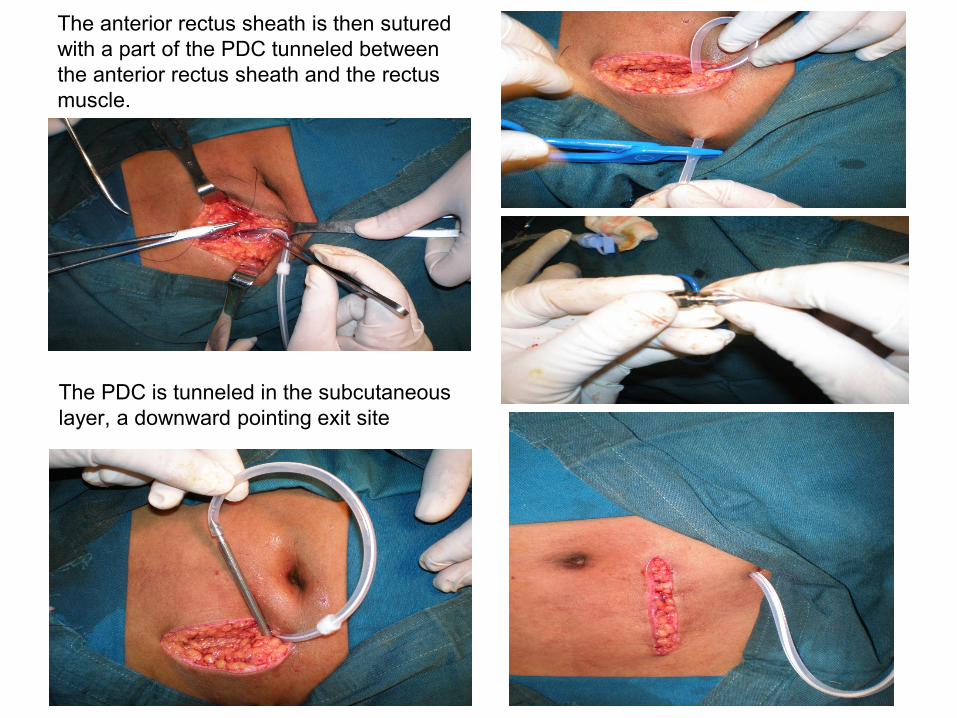
The anterior rectus sheath is then sutured
with a part of the PDC tunneled between
the anterior rectus sheath and the rectus
muscle.
The PDC is tunneled in the subcutaneous
layer, a downward pointing exit site
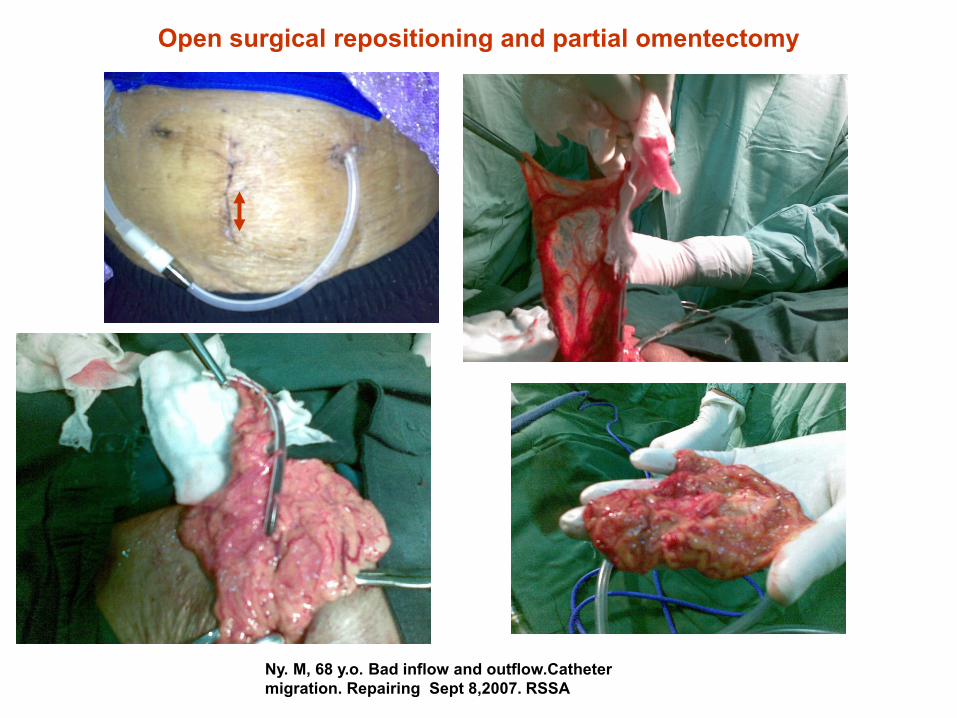
Open surgical repositioning and partial omentectomy
Ny. M, 68 y.o. Bad inflow and outflow.Catheter
migration. Repairing Sept 8,2007. RSSA

Kaplan–Meier plot of Tenckhoff catheter survival in
the present study. 2 yr sr 87,2 %
TENCKHOFF CATHETER
INSERTION BY 6
NEPHROLOGISTS:OPEN
DISSECTION TECHNIQUE in
Hongkong. N=250 (2005-2008)
Perit Dial Int 2010; 30:524-527
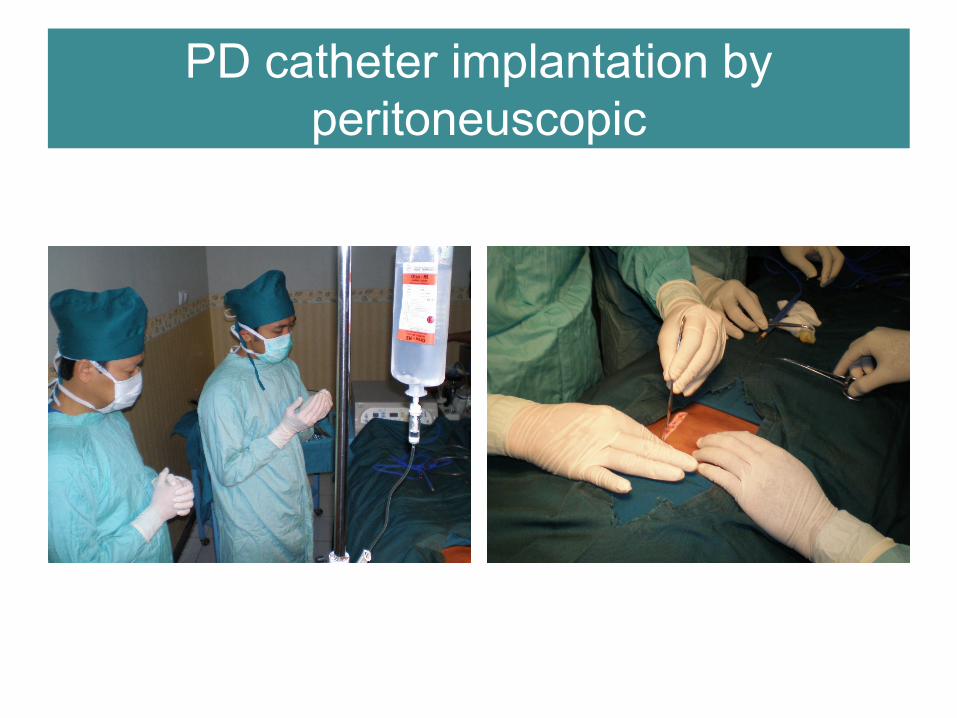
PD catheter implantation by
peritoneuscopic
Peritoneuscope

Site of insertion
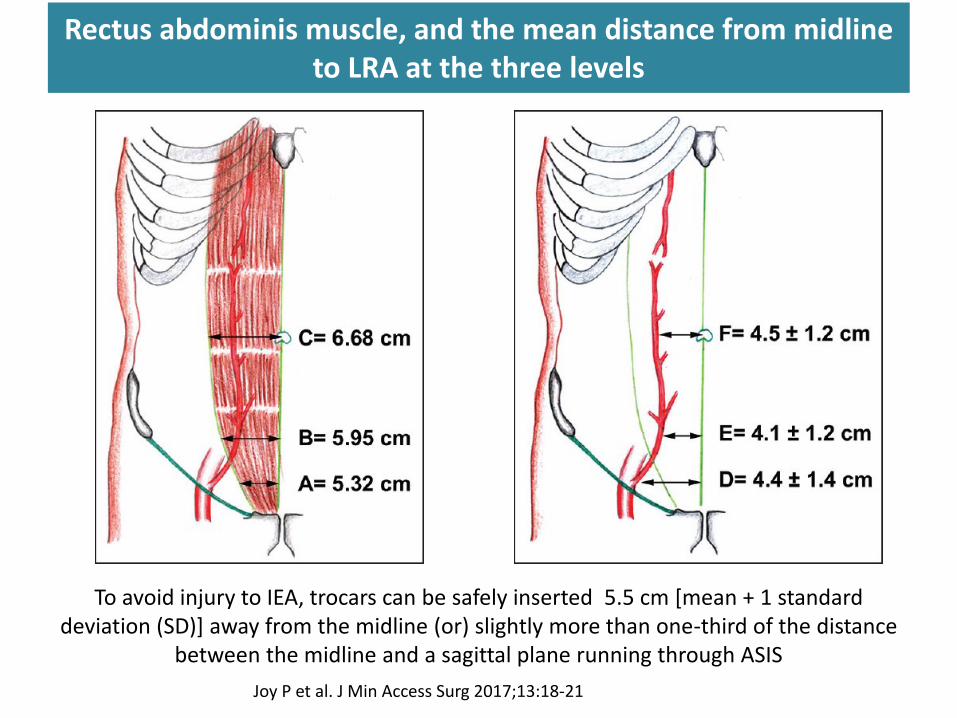
Rectus abdominis muscle, and the mean distance from midline to LRA at the three levels
To avoid injury to IEA, trocars can be safely inserted 5.5 cm [mean + 1 standard deviation (SD)] away from the midline (or) slightly more than one-third of the distance
between the midline and a sagittal plane running through ASIS
Joy P et al. J Min Access Surg 2017;13:18-21

Make 3-5 cm long horizontal skin incision.
Perform blunt dissection with hemostats to the anterior surface of the rectus sheath.
Insert Quill® Catheter Guide Assembly at 20o - 30o angle toward coccyx into the
peritoneum
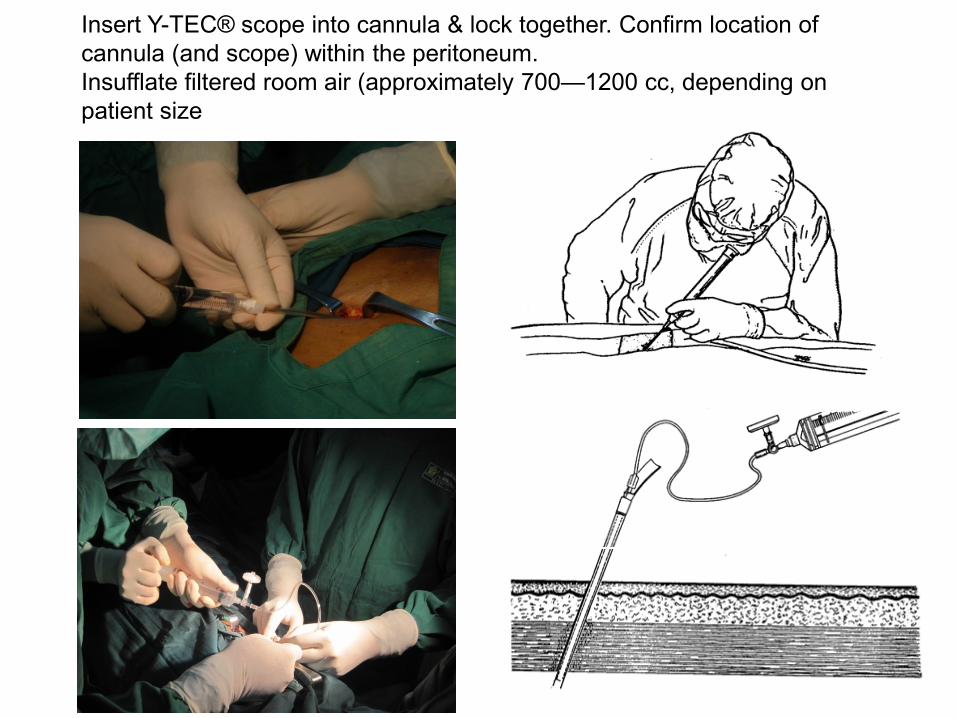
Insert Y-TEC® scope into cannula & lock together. Confirm location of
cannula (and scope) within the peritoneum.
Insufflate filtered room air (approximately 700—1200 cc, depending on
patient size
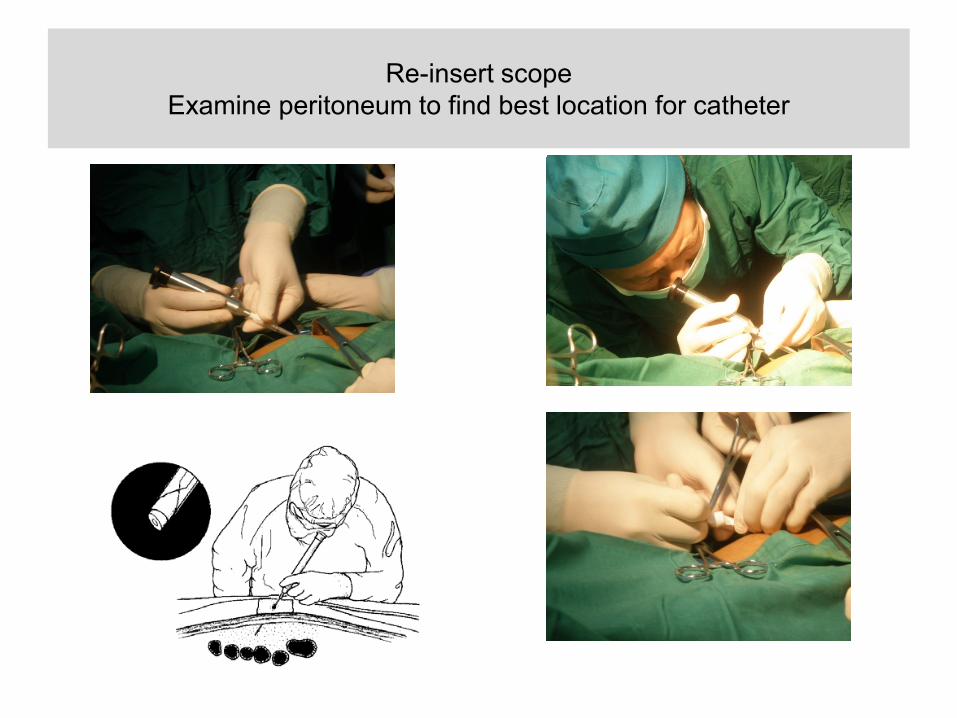
Re-insert scope
Examine peritoneum to find best location for catheter

Remove the cannula from the Quill® Guide with a slight twisting motion and
retraction of the cannula
Insert and dilate the Quill® Guide with the small and large dilator (goal is to
dilate rectus muscle).
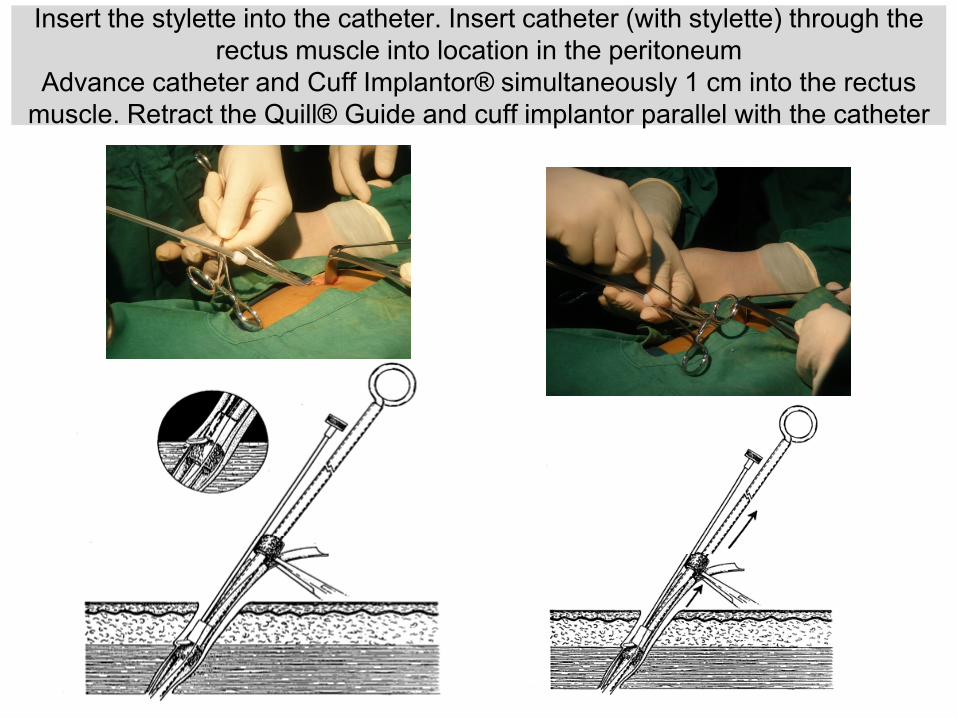
Insert the stylette into the catheter. Insert catheter (with stylette) through the
rectus muscle into location in the peritoneum
Advance catheter and Cuff Implantor® simultaneously 1 cm into the rectus
muscle. Retract the Quill® Guide and cuff implantor parallel with the catheter

Create tunneling : incision exite site, inserting tunnelor with
catheher to exite site

Perbandingan open surgery vs peritoneuskopi di RSSA
Open Surgery (n=108) Peritoneouscopy (n=64)
Usia (tahun) (p=0.053) 50±13.4 47±10.3
Jenis Kelamin (L/P) (p=0.331) 74/34 41/23
Lama CAPD (bulan) (p=0.548) 45±40.9 19±15.5
≤ 6 bulan 9(8.3%) 7(10.9%)
7-12 bulan 25(23.1%) 21(32.8%)
>12 bulan 74(68.5%) 36(56.3%)
Tingkat Pendidikan (p=0.001 )
≤ SD 25(23.1%) 34(53.1%)
SMP 27(25.0%) 8(12.5%)
SMA 37(34.3%) 12(18.8%)
≥ S1 19(17.6%) 10(15.6%)
Komplikasi non mekanik (p=0.015)
Perdarahan 5(4.6%) 2(3.1%)
Infeksi Exit Site 7(6.5%) 0
Peritonitis 4(3.7%) 0
Masalah Mekanik (p=0.182)
Malposisi 4(3.7%) 2(3.1%)
Kateter Tertekuk 0 1(1.6%)
Bocor 8(7.4%) 0
Outflow Failure 6(5.5%) 3(4.7%)
Outcome Catheter (p=0.947))
Meninggal 31(28.7) 18(28.1%)
Off Catheter 5(4.6%) 1(1.6%)
Peritonitis 9(8.3%) 8(12.5%)

LAPAROSCOPIC
(for catheter reposition)
OMENTOPEXY
Break in periode
• Time to start dwelling
• Depend on methode of insertion.
• Optimally 2 weeks post-operation.
• Peritoneuscopic : 1 week
Laparascopic : 10 days
Seldinger technique : 2 weeks
Laparotomi : 2 weeks
• However, peritoneal dialysis can be started within hours of
placement of a catheter if needed; using low-volume, supine
exchanges.
• The break-in period may need to be longer in patients in whom there
is concern about impairment in wound-healing (diabetes, on steroid).
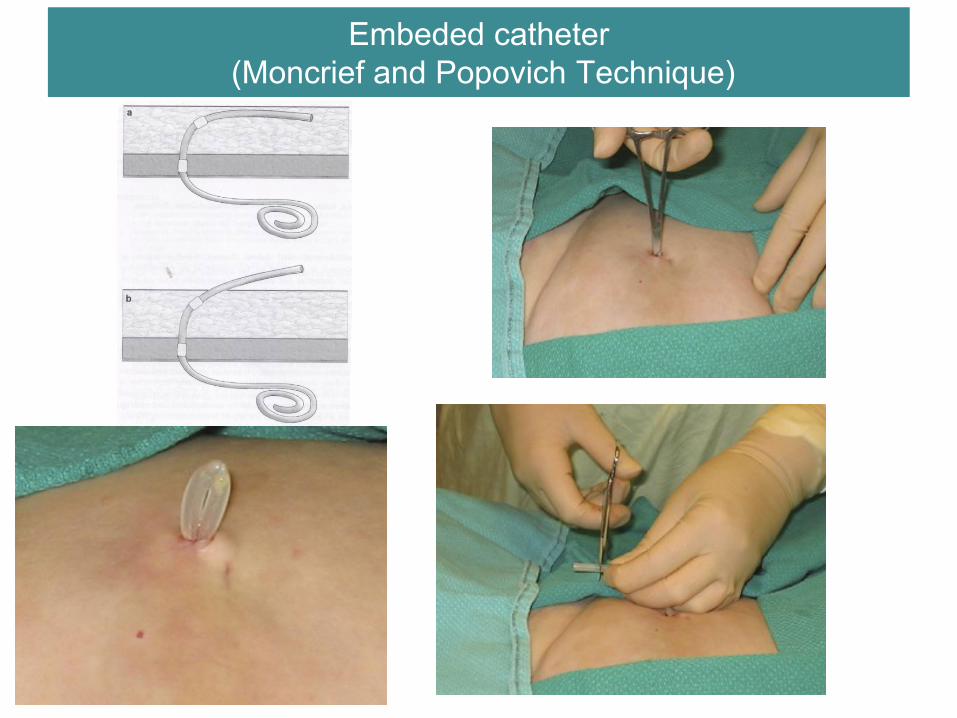
Embeded catheter
(Moncrief and Popovich Technique)
Perawatan kateter PDpasca insersi
• Antibiotik profilaksis diberikan sebelum insersi kateter PD
• Dressing exite site dilakukan setiap minggu, sampai luka kering.
• Dressing tambahan dilakukan bila kasa basah atau berdarah.
• Belum boleh kena air selama luka belum kering.
• Mandi/shower boleh setelah luka kering (2-3 minggu post-op).
ISPD Guideline.Perit Dial Int 2012; 32:S29–S86 ; Oxford Univ. Hospital , NHS Found Trust
Perawatan kateter PDpasca insersi
Lakukan teknik aseptik, masker dan handschoen steril:
• Bersihkan luka sekitar exite site dengan kasa steril yang dibasahi cairan antiseptik.
• Kerak luka dibersihkan dengan kasa dibasahi NS.
• Gunakan kasa lain untuk membersihkan tubing kateter, dari arah tubuh keluar
• Gunakan kasa kering steril beberapa lapis untuk menutup luka. Lalu difiksasi
• Selang kateter difiksasi, sesuai posisinya, untuk mencegah pergerakan.
ISPD Guideline.Perit Dial Int 2012; 32:S29–S86
Perawatan kateter harian untuk pencegahan infeksi
• Setiap hari dioleskan antibiotik cream/zalf pada exite site.
• Exite site dibersihkan minimal 2x seminggu atau setiap selesai mandi/shower
• Bila terjadi exite site infection : bersihkan exite site setiap hari.
ISPD CATHETER-RELATED INFECTION RECOMMENDATIONS: 2017 UPDATE

Antibakteri Topical , Antiseptik, dan cairan antiseptik untuk pencegahan infeksi terkait kateter
• Povidone-iodine • Chlorhexidine solution • Amuchina solution/hypochlorite solution • Mupirocin cream • Gentamicin cream or ointment • Ciprofloxacin otologic solution • Antibacterial honey • Polysporin triple ointment • Polyhexanide
Ringkasan
• CAPD adalah pilihan terapi pengganti ginjal
yang mempunyai beberapa kelebihan
dibandingkan HD
• Metode insersi percutaneus memberikan hasil
lebih superior dibandingkan laparotomi
• Lama break in periode tergantung metode
insersi
• Dressing dan exite site care adalah penting
paska operasi
