tentang jurnal homeostasis
TRANSCRIPT

8/10/2019 Tentang Jurnal Homeostasis
http://slidepdf.com/reader/full/tentang-jurnal-homeostasis 1/9
Review
Peran natrium dalam cairan Homeostasis dengan latihan
Rick L. Sharp, PhD
Latihan Fisiologi laboratorium, departemen kesehatan & manusia kinerja, Iowa State University, Ames, Iowa
Kata kunci: natrium, cairan, Hiponatremia Gejala, latihan, aktivitas fisik, panas kelelahan
Makalah ini memberikan tinjauan terhadap sastra terkini mengenai efek interaktif natrium dan cairan
Penelanan dalam menjaga homeostasis fluida selama dan mengikuti paparan panas dan latihan. Berat berkeringat
selama latihan yang dikombinasikan dengan panas eksposur umumnya menghasilkan cairan defisit sesuai dengan 1 8% kerugian dalam
tubuh massa. Dengan demikian, banyak perhatian telah difokuskan pada pengembangan fluida penggantian panduan dan
produk untuk orang-orang yang aktif. Baru-baru ini, telah ada laporan lebih sering kasus Hiponatremia Gejala di antara
individu yang cenderung over-ingest air selama latihan yang berlangsung lebih dari empat jam, dan masuknya natrium
klorida dalam minuman fluida penggantian sering dianjurkan sebagai sarana potensi untuk mengurangi risiko
Hiponatremia Gejala. Meskipun Hiponatremia Gejala tidak cenderung menjadi faktor risiko utama untuk populasi umum,
daya tahan ultra-atlet dan orang-orang dengan aktivitas fisik pekerjaan dan eksposur panas mungkin akan mendapat keuntungan dari inirekomendasi. Penggantian fluida defisit setelah latihan dan panas eksposur daerah lain yang telah menerima
perhatian yang cukup besar. Penelitian di daerah ini menunjukkan bahwa jika air dikonsumsi, volume tertelan perlu
melebihi defisit fluida sekitar 150% untuk mengkompensasi kencing kerugian yang akan terjadi dengan air
Penelanan. Dimasukkannya natrium klorida dan lain larutan dalam minuman rehidrasi mengurangi kehilangan air kencing,
menuju pemulihan lebih cepat fluid balance. Data yang disajikan dalam makalah ini yang menyarankan diukur
interaktif hubungan antara natrium konten dan cairan volume dalam mempromosikan cepat sembuh dari fluid balance
setelah latihan dan dehidrasi termal-induced.
PENGENALAN
Dalam 1960 s itu tidak jarang untuk menemukan garam tablet
dispenser di ganti kamar di berbagai tempat olahraga. Ini adalahkarena dari keyakinan luas yang berlebihan kerugian sehingga-
dium keringat selama aktivitas fisik dapat menyebabkan pemiskinan
natrium dan mengakibatkan kram panas. Penelitian berikutnya,
Namun, menunjukkan bahwa keringat hipotonik dan natrium
konsentrasi lebih rendah daripada plasma. Temuan ini mengakibatkan
kesadaran bahwa nutrisi yang hilang dalam kelimpahan yang terbesar selama
latihan dalam panas adalah air daripada natrium. Lebih lanjut re-
pencarian dikonfirmasi menemukan ini dengan menunjukkan bahwa selama latihan
dalam kondisi panas dan lembab menyebabkan peningkatan dalam plasma
konsentrasi natrium [1], yang menyiratkan bahwa air penggantian mungkin
lebih penting daripada natrium penggantian selama exertional
stres panas.Dengan popularitas berjalan di 1970� s, itu menjadi
jelas bahwa penyakit panas merupakan risiko utama untuk orang-orang
berjalan di lingkungan yang panas dan lembab. Pedoman untuk fluida
penggantian dikembangkan dan bersama medis com-
munity, ras penyelenggara, dan untuk masyarakat umum. Khusus
minuman yang dikembangkan oleh perusahaan-perusahaan makanan untuk men
karbohidrat dan elektrolit penggantian dan dirancang untuk
digunakan sebelum, selama dan setelah latihan untuk membantu memenuhi
peningkatan tuntutan untuk nutrisi ini dalam melaksanakan publik.
Komposisi Olahraga minuman disesuaikan selama
30 tahun dalam menanggapi baik temuan-temuan penelitian dan rasa pref-
erences. Tujuan dari makalah ini untuk meninjau baru-baru ini
literatur ilmiah mengenai natrium keseimbangan dan hubungan-
kapal ke hidrasi selama dan setelah latihan, mi-
larly ketika dilakukan di bawah tekanan lingkungan panas.
AIR DAN NATRIUM KERUGIAN
SELAMA LATIHAN
Keringat produksi selama latihan dalam panas tergantung pada
latihan intensitas, durasi, pakaian, status hidrasi
Alamat cetak ulang permintaan: Rick L. Sharp, Ph.D., 250 Forker bangunan, departemen kesehatan & manusia kinerja, Iowa State University, Ames, IA 50011. E-mail:
Journal of American College of Nutrition, Vol. 25, No. 3, 231S 239S (2006)
Diterbitkan oleh American College of Nutrition
231S
Multilizer PDF Translator Free version - translation is limited to ~ 3 pages per translation.
Multilizer PDF Translator Free version - translation is limited to ~ 3 pages per translation.

8/10/2019 Tentang Jurnal Homeostasis
http://slidepdf.com/reader/full/tentang-jurnal-homeostasis 2/9
individu, panas-acclimation individu dan environmen-
Tal kondisi [2� 5]. Saat melakukan aktivitas fisik tinggi
lingkungan suhu, Penguapan keringat dari terkena
kulit adalah mekanisme utama untuk hilangnya panas. Apakah hilangnya panas
tidak cocok untuk tingkat metabolisme panas produksi (intensitas
latihan), penyimpanan panas tubuh naik dan inti suhu dapat
cepat mencapai tingkat berbahaya. Menjaga kapasitas tinggi untuk
keringat produksi karena itu penting dalam thermoregulation dan
pencegahan penyakit panas. Selama intensitas tinggi atletik,
keringat harga hingga 3 L\/hr mungkin di bawah panas dan lembab
kondisi [6,7]. Hal ini menyebabkan hilangnya tubuh air atau dehy-
dration setara dengan 1 8% dari tubuh massa. Digabungkan dengan keringat
konsentrasi natrium rata-rata berkisar antara 40� 60
mEq\/L [6 9], seperti keringat harga dapat mengakibatkan natrium pemiskinan
tingkat sekitar 150 mmol\/hr dengan natrium tambahan kerugian dalam
produksi air seni.
Sebuah studi oleh Mao et al. diukur elektrolit keringat dan
kencing elektrolit konsentrasi dan ekskresi dalam 13 remaja
Pemain sepak bola (16 18 thn) selama 1 jam sepak bola praktek con-
menyalurkan dalam panas (32 37C, kelembaban relatif 30 50%) pada delapan
hari [10]. Konsentrasi natrium berarti keringat adalah 55 mmol\/L.
Rata-rata keringat kerugian selama sesi 1 jam latihan adalah 1.54 l
(SD 2.06 L). Keringat dihitung hilangnya natrium rata-rata
mmol 82 (SD 62 mmol). Kencing hilangnya natrium rata-rata 110
mmol (SD 36 mmol). Dengan demikian rata-rata natrium ekskresi ac-
menghitung untuk oleh keringat dan saluran kemih ekskresi adalah 192 mmol (tabel
1). Karena tidak ada data dietary intake dilaporkan untuk mata pelajaran ini,
natrium dan fluid balance bisa tidak dihitung. Demikian pula, tidak ada
data yang diperoleh untuk menilai kinerja baik atau fisiologis
konsekuensi dari kerugian ini cairan dan elektrolit. Meskipun demikian,
observasi ini menyarankan kerugian besar natrium dan air
selama latihan dalam panas.Dimungkinkan bahwa metode pengumpulan keringat digunakan oleh Mao
et al. berlebihan seluruh tubuh natrium kerugian dalam keringat karena
untuk variasi regional dalam konsentrasi natrium keringat [11,12].
Belajar di Mao et al., keringat dikumpulkan dari punggung dan
dada subjek selama 5 menit selama sesi latihan.
Konsentrasi natrium diukur 55 mmol\/L mirip
konsentrasi Na keringat dikumpulkan oleh Shirreffs menggunakan
seluruh tubuh washdown metode [12]. Shirreffs et al. diukur
keringat konsentrasi natrium 51.6 mmol\/L selama latihan
memproduksi dehidrasi 2% dari subyek. Oleh karena itu tidak mungkin
data yang diperoleh oleh Mao et al. yang terlalu berlebihan.
Dalam sebuah studi oleh Sanders et al. [13], air dan natrium kerugian
diukur selama 4 hr bersepeda latihan pada 20 C pada latihan
intensitas setara dengan 55% dari puncak VO2. Selama latihan
mata pelajaran tertelan 3.85 l elektrolit karbohidrat 8 %
minuman yang mengandung 5, 50, atau 100 mmol\/L natrium. Keringat kerugian
rata-rata antara 3,7 dan 3,9 l untuk masing-masing dari cobaan. Natrium
konsentrasi keringat berkisar 43� 48 mmol\/L, memproduksi
kerugian natrium keringat antara 150 dan 190 mmol atas 4 hr
latihan. Dikombinasikan dengan natrium kencing kerugian, mata pelajaran
mengalami negatif natrium keseimbangan 198 mmol ketika
menelan 5 mmol\/L Na minuman, 36 mmol ketika menelan
50 mmol\/L Na minuman, dan mengalami natrium positif
keseimbangan 159 mmol ketika menelan minuman yang mengandung
mmol 100\/L natrium (Fig. 1). Selain untuk meyakinkan positif
natrium keseimbangan di seluruh latihan, konsumsi minuman
mengandung 100 mmol\/L natrium mengurangi total cairan yang hilang selama
latihan dibandingkan dengan minuman lain. Perhitungan
perubahan kompartemen air mengungkapkan kerugian signifikan fluida
dari ECF) 1.1 L) 5 mmol\/L sodium sidang, tidak ada perubahan dalam
ECF di 50 mmol\/L natrium pengadilan, dan perluasan ECF
volume) 0.5 L) sodium mmol 100\/L percobaan. Meskipun
lebih baik pemeliharaan hidrasi status di 50 dan 100
mmol\/L natrium cobaan, tanggapan kardiovaskular (misalnya denyut jantung
Respon) adalah serupa di antara tiga persidangan.
HIPONATREMIA GEJALA
Selama 20 tahun terakhir, orang-orang yang terlibat dalam durasi panjang
latihan daya tahan di panas telah disarankan untuk minum sebagai
banyak cairan mungkin selama latihan untuk mencegah dehydra-
tion, menjaga respon berkeringat dan dengan demikian memelihara
Pengatur suhu tubuh kapasitas [14]. Sayangnya, saran ini memiliki
mengakibatkan peningkatan atau setidaknya pengakuan Hiponatremia Gejala di banyak atlet bersaing dalam peristiwa ini [15 19]. Hyponatre-
Mia dapat menyebabkan karena hilangnya berlebihan natrium karena
berat berkeringat tanggapan, atau alternatif, karena yang pengenceran
plasma natrium sebagai konsekuensi dari terlalu bersemangat hidrasi [16].
Berbagai rekomendasi untuk mencegah Hiponatremia Gejala
dibuat dalam literatur dan termasuk mengurangi penekanan pada
fluida Penelanan [20] dan\/atau meningkatkan kandungan natrium bev-
erages tertelan selama latihan [21 24].
Prevalensi Hiponatremia Gejala
Beberapa penulis telah dijelaskan kasus Hiponatremia Gejala dur-
ing ketahanan latihan dalam panas. Speedy et al. telah menerbitkan
terbesar berbasis bidang studi terjadinya Hiponatremia Gejala
Tabel 1. Cairan tubuh dan natrium kerugian selama 1 jam sepak bola praktek di antara remaja laki-laki
Tubuh massa
(kg)
Kehilangan cairan
(L)
Keringat [Na]
(mmol\/L)
Keringat Na
Kehilangan
(mmol)
Kencing Na
Kehilangan
(mmol)
Total Na
Kehilangan
(mmol)
Berarti 62,5 1.54 55 82 110 192
SE 6,8 0,57 27 62 36 �
Data berasal dari Mao et al. [10].
Natrium dalam cairan Homeostasis dengan latihan
232S VOL. 25, NO. 3
Multilizer PDF Translator Free version - translation is limited to ~ 3 pages per translation.
Multilizer PDF Translator Free version - translation is limited to ~ 3 pages per translation.

8/10/2019 Tentang Jurnal Homeostasis
http://slidepdf.com/reader/full/tentang-jurnal-homeostasis 3/9
[18]. Dalam studi ini, 330 finishers perlombaan triathlon (6� 9
HR) dipelajari. Berdasarkan plasma natrium konsentrasi kurang
dari 135 mmol\/L, 58 (18%) dari finishers yang hyponatre-
Mikha sebelas mata pelajaran ini yang digambarkan sebagai sangat hy-
ponatremic) 130 mmol\/L) dan tujuh ini symp -
tomatic. Para penulis juga mencatat bahwa orang-orang subjek dengan
kasus-kasus yang paling parah Hiponatremia Gejala telah sedikit perubahan dalam tubuh
berat selama perlombaan, menyiratkan bahwa cairan yang berlebihan
menyebabkan Hiponatremia Gejala dalam sebagian besar kasus.
Penulis lain menyarankan Hiponatremia-Gejala itu hanya dapat
faktor risiko yang signifikan dalam luar biasa panjang durasi fisik aktivitas seperti maraton berlari dan triathlon berlangsung 4 jam
atau lebih. Noakes et al. [20] menunjukkan bahwa sebagian besar kasus
Hiponatremia Gejala diamati dalam para peserta kurang terlatih
Siapa yang mengambil jauh lebih lama untuk menyelesaikan lomba daripada atas
finishers. Durasi yang lebih lama dari latihan digabungkan dengan lebih besar
total fluida asupan sebagai akibat dari durasi yang lebih lama, karena itu
menempatkan orang-orang ini pada risiko lebih besar mengembangkan Hiponatremia Gejala.
Karena kasus Hiponatremia Gejala diinduksi latihan
sebagian besar terbatas pada upaya fisik luar biasa yang berlangsung lagi
dari 4 hr, Hiponatremia Gejala bukanlah cenderung sangat lebar-
menyebar di populasi umum yang terlibat dalam latihan
berlangsung kurang dari 2 jam per hari. Berbagai mekanisme telah
diajukan untuk menjelaskan pengembangan Hiponatremia Gejala dalam beberapa
individu. Penyebab ini termasuk cairan yang berlebihan atau pengenceran
efek [17], berlebihan natrium kehilangan selama latihan [21], dan
tidak pantas tanggapan dari arginin-vasopresin mengarah ke mantan
cessive retensi cairan tertelan [25]. Temuan lebih besar
prevalensi Hiponatremia Gejala di antara wanita menunjukkan baik
efek biologis seks pada fluida homeostasis atau perilaku berbeda-
ences antara pria dan wanita yang mungkin menyebabkan perempuan untuk dapat
lebih sesuai dengan saran untuk minum cairan sebanyak mungkin
selama latihan daya tahan [27].
Pencegahan Hiponatremia Gejala
Jika fluida overload adalah kontributor penting untuk mengembangkan-
ment Hiponatremia Gejala, orang akan berharap plasma natrium con-
centration jatuh selama latihan sebanding dengan volume
natrium rendah atau tidak ada cairan tertelan. Vrijens dan Rehrer [24]
memeriksa pertanyaan ini oleh merekrut subjek laki-laki 10 untuk exer-
cise untuk 3 hr di ruang lingkungan disimpan di 34 C. Themata pelajaran melakukan latihan ini pada dua hari yang terpisah; sekali
Sementara menelan bebas natrium air setiap 15 menit untuk mencocokkan
kehilangan cairan, dan sekali sementara menelan natrium komersial-
mengandung (18 mmol\/L Nakarbohidrat 63 g\/L, 3 mmol\/L
kalium) minuman untuk mencocokkan kehilangan cairan. Selama air
Penelanan konsentrasi natrium sidang, rata-rata plasma menolak
dari 140 mmol\/L sebelum latihan untuk 134 mmol\/L pada akhir
latihan (Fig. 2). Dalam sidang, karbohidrat-elektrolit plasma
konsentrasi natrium tidak mengurangi secara signifikan (140
mmol\/L sebelum latihan, 138 mmol\/L di akhir latihan). The
penulis menyimpulkan bahwa Hiponatremia Gejala diperbolehkan bahkan ketik
asupan cocok kehilangan cairan selama durasi panjang berolahraga ketikanatrium tidak termasuk dalam minuman pengganti fluida.
Penulis lain juga merekomendasikan dimasukkannya natrium
dalam minuman dikonsumsi selama latihan [7,22,23,26]. Gisolfi
[26] dianjurkan bahwa orang-orang yang berolahraga untuk 1 3 hr harus
mengkonsumsi antara 800 1600 ml\/hr cairan yang mengandung 10 20
mmol\/L natrium dan bahwa orang-orang yang berolahraga untuk lebih dari 3 jam
harus mengkonsumsi 500 1000 ml\/hr cairan yang mengandung 20 30
mmol\/L natrium. Lutkemeier et al. [22] menyarankan bahwa saline
Penelanan sebelum latihan dapat membantu melestarikan plasma volume
dan dapat mengakibatkan perubahan yang bermanfaat dalam latihan daya tahan
kinerja. Dalam review artikel yang diterbitkan oleh Rehrer [7] inclu-
Sion natrium dalam minuman pengganti fluida pada konsentrasi
berkisar antara 30 dan 50 mmol\/L disarankan sebagai kemungkinan
bermanfaat bagi orang-orang yang terlibat dalam panjang durasi latihan (3 hr ata
lebih) dalam panas.
Konsisten dengan hipotesis yang berlebihan natrium kehilangan
Gambar 1. Natrium keseimbangan di ujung 4-jam latihan bersepeda di 20 C
(kering-bohlam) lingkungan. Uji mengulangi dengan menelan 3.85 l
8% karbohidrat-elektrolit minuman dengan 5, 50, atau 100
mmol\/L natrium konsentrasi. Diadaptasi dari Sanders et al. [13].
Fig. 2. Konsentrasi natrium plasma sebelum dan setelah 3-jam latihan di
34 C (kering bohlam) lingkungan dengan menelan air baik polos
pertandingan kehilangan cairan atau minuman elektrolit karbohidrat komersial untuk
cocok kehilangan cairan. Diadaptasi dari Vrijens dan Rehrer [24].
Natrium dalam cairan Homeostasis dengan latihan
JOURNAL OF AMERICAN COLLEGE OF NUTRITION 233S
Multilizer PDF Translator Free version - translation is limited to ~ 3 pages per translation.
Multilizer PDF Translator Free version - translation is limited to ~ 3 pages per translation.

8/10/2019 Tentang Jurnal Homeostasis
http://slidepdf.com/reader/full/tentang-jurnal-homeostasis 4/9
the primary cause of exercise-induced hyponatremia, Hiller et
al. [21] suggested 1 2 g sodium ingestion per hour of exercise
to prevent hyponatremia. Assuming fluid ingestion of 1 liter per
hour to match fluid lost through sweating, this amount of
sodium requires a beverage containing 43 87 mmol/L sodium.
This recommendation is slightly higher than that recommended
by Rehrer and represents a sodium concentration roughly 2 4
times as high as that found currently in most commercial fluid
replacement beverages. Barr et al. argues that the reduced
palatability of such beverages would likely lead to less fluid
consumption among the general population and result in a
greater risk of dehydration [28].
There are also several studies that provide evidence that
sodium supplementation during exercise along with fluid re-
placement is not necessary [28 32]. Barr et al. had 8 subjects
perform 6 hr exercise at 55% VO2max in a heat chamber held
at 30C [28]. Each subject completed this exercise on separate
occasions to evaluate the possible effects of water ingestion,
water plus sodium (25 mmol/L), or no fluid. When the subjects
were not provided with fluid during the exercise, core temper-
ature and heart rate rose rapidly while plasma volume declined
throughout exercise. Under this condition, only one subject was
able to complete the full 6 hr exercise and the mean time of
exercise was 4.5 hr. The subjects who failed to complete the
exercise did so because heart rate exceeded 95% maximum
heart rate (n 1), core temperature exceeded 40C (n 1), or
volitional exhaustion (n 5). In the water and saline trials,
seven of the eight subjects completed the 6 hr of exercise.
There were no differences in either heart rate or core temper-
ature response between water and saline ingestion and both
trials resulted in smaller rise in these variables than was ob-
served when no fluid was ingested. Plasma volume droppedless when ingesting the saline beverage than when ingesting
water. Plasma sodium concentration decreased by small
amount in both the saline (change 3.0 mmol/L) and water
(change 3.9 mmol/L) trials but there were no significant
differences in plasma sodium concentration between these tri-
als. Calculation of overall sodium balance revealed a sodium
deficit in the water trial ( 207 mmol) that was significantly
larger than observed in the saline trial (91.3 mmol). Based on
these results, the authors concluded that sodium concentration
equivalent to that found in commercial sports drinks do not
prevent the fall in plasma sodium during exercise when fluid
intake matches fluid lost through sweating. They further sug-
gest that sodium replacement is not necessary in exercise
lasting less than 6 hr.
Based on these reviewed studies, it is apparent that inclusion
of sodium in fluid replacement beverages can offset some of
the losses of sodium that occur during prolonged and heavy
sweating. It is less clear that doing so will prevent hyponatre-
mia or that this improves either exercise performance or ther-
moregulation. As suggested by Sanders et al., however, sodium
ingestion likely preserves the plasma volume during exercise at
the expense of the intracellular fluid volume. What effect this
relative dehydration has on muscle metabolism and function
has not yet been studied. An additional finding common to
most of these studies is that even if sodium ingestion does not
affect plasma sodium concentration, it does reduce the sodium
deficit that occurs during prolonged exercise in the heat. This
may be significant for people who are involved in daily exer-
cise or occupations that involve prolonged physical activity in
hot, humid environments.
ROLE OF SODIUM INREHYDRATION AFTER EXERCISE
Despite efforts to replace fluid losses during exercise, mild
dehydration after exercise remains a common finding. Dehy-
dration equivalent to less than 2% loss of body mass is asso-
ciated with reduced performance and impaired thermoregula-
tion during subsequent exercise if the fluid deficit is not
corrected. Thus, considerable research has been devoted to
understanding the rehydration process and the role played by
sodium in restoring body fluids lost during prior exercise.
In studying rehydration after exercise-induced body water
loss, investigators have employed three models for rehydration:
allow subjects to drink fluids ad lib during the rehydration
period [33 35], prescribe fluid intake during the rehydration
period to match the fluid lost during the prior exercise [36 38],
and prescribe fluid intake in excess of the fluid lost in the prior
exercise [39 43]. The advantage of allowing ad lib rehydration
is that factors regulating thirst can be studied while the advan-
tage of prescribing fluid intake equal to fluid lost restores
plasma volume while total body water remains somewhat con-
tracted. The rationale for the approach that involves prescribingfluid intake in excess of that lost in the prior exercise is that
both plasma volume and total body water are restored by the
end of the rehydration period. Finally, there are also hybrid
models in which varied amounts of fluid and sodium content
are studied to allow for evaluation of independent effects of
sodium and fluid volume on the rehydration process.
Ad Libitum Rehydration
Nose et al. dehydrated six subjects by 2.3% using thermal
and exercise induced dehydration [34]. Over the next 3 hr,
subjects were seated in a thermoneutral environment and al-
lowed to rehydrate ad libitum using tap water (15C), placebo or
capsules containing NaCl to produce sodium concentration of
75 mmol/L. The purpose of this approach was to examine the
effect of sodium on drinking behavior and restoration of body
fluid compartments. Average fluid loss in the dehydration
period was 1550 ml and was followed by ingestion of 1100 ml
in the water trial and 1216 ml in the water plus sodium trial,
leaving the subjects in a fluid deficit after 3 hr of rehydration.
When urine production is subtracted from fluid ingestion, net
fluid gain during rehydration was 826 ml in the water trial and
Sodium in Fluid Homeostasis with Exercise
234S VOL. 25, NO. 3

8/10/2019 Tentang Jurnal Homeostasis
http://slidepdf.com/reader/full/tentang-jurnal-homeostasis 5/9
1045 ml in the water plus sodium trial. Despite the persistent
negative fluid balance even after 180 min, plasma volume had
returned to pre-dehydration by 90 min of recovery in the water
plus sodium trial while plasma volume remained slightly below
the pre-dehydration level even at 180 min of recovery. Calcu-
lation of fluid compartment recovery based on chloride space
showed that by the end of the rehydration period, total body
water had recovered by 52% in the water trial and by 76% in
the water plus sodium trial. Recovery of intracellular fluid was
not different between water and water plus sodium trials. Both
ECF and PV were more completely restored in recovery in the
water plus sodium trial (84% and 100%, respectively) com-
pared with water only (44% and 77%, respectively). These
findings illustrate the following points: 1) thirst is inadequate to
assure complete recovery of total body water deficits likely due
to early restoration of plasma volume, thereby removing the
volume dependent dipsogenic drive, 2) the presence of sodium
in the rehydration beverage stimulates greater drinking likely
due to greater osmotic dipsogenic drive, 3) the presence of
sodium in the rehydration beverage accelerates the recovery of
extracellular fluid and plasma volume in particular, and 4)
sodium in the rehydration beverage reduces urinary losses of
water, allowing a greater fraction of the ingested fluid to be
retained. These findings were later confirmed by Wemple et al.
using a similar dehydration and rehydration protocol [35].
Rehydration with Fluid Intake Sweat Loss
Several studies have examined recovery of body water
losses after exercise by providing an amount of fluid to subjects
that is equal to the amount of water lost during the exercise as
a consequence of sweating. Most of these studies attempted toachieve complete rehydration within a relatively short period
lasting between 2 and 4 hours. The early study by Costill and
Sparks [36] dehydrated eight male subjects using intermittent
exposure to dry heat (70C) until 4% of body mass was lost.
Once the prescribed dehydration was reached, the men returned
to a thermoneutral environment to begin the rehydration period.
At the beginning of rehydration and at 15-min intervals the
subjects drank a volume of fluid equal to 7.7% of the volume
lost during the dehydration. This was continued for 3 hr so that,
by the end of the 3 hr rehydration period, the subjects had
ingested the same total volume of fluid as lost in dehydration.
The procedure was repeated once when ingesting plain water as
the rehydration fluid and once using a carbohydrate-electrolyte
(CE) drink for rehydration. The CE drink contained 22 mmol/L
sodium, 17 mmol/L chloride, 2.6 mmol/L potassium, 3.9
mmol/L phosphate, and 10.6 g/100ml glucose with osmolality
of 444 mOsm/L.
Urine production was significantly higher when subjects
rehydrated with water (602 ml) than when using the CE bev-
erage (367 ml). Despite drinking a volume of fluid equal to that
which was lost in dehydration these subjects were only able to
recover 62% of their body mass loss during the rehydration.
This was mostly due to urinary and insensible loss of water
during the rehydration period. Plasma volume had dropped by
an average of 12% with dehydration and 38% of this loss was
recovered during rehydration with water while 67% of the loss
in plasma volume was recovered when drinking the CE bever-
age. The authors concluded that the presence of electrolytes and
carbohydrate in the rehydration favored a more complete re-
filling of plasma volume, but that neither beverage was ade-
quate for completely restoring either plasma volume or total
body water when 100% of the dehydration volume is consumed
overa3hr period.
Rehydration With Fluid Intake > Fluid Loss
Based on the earlier observations of incomplete body water
restoration when either thirst regulates fluid intake or fluid
intake matches the fluid lost in the prior dehydration, most
recent studies have provided fluid in excess of that which was
lost in dehydration [39 43]. Authors recognized that additional
fluid was needed to offset the obligatory urinary losses, con-
tinued sweat water loss, and water loss through respiration.
These studies fail to demonstrate complete body water resto-
ration during rehydration lasting up to 6 hours unless the
ingested fluid is coupled with sodium ingestion. A convenient
method of providing both fluid and sodium during rehydration is
to select a rehydration beverage or food providing both fluid and
sodium with other nutrients (carbohydrate and potassium, e.g.)
that may be vital in restoring normal function after dehydration.
Maughan and Leiper [39] examined the role of varied
concentrations of sodium in the rehydration beverage in achiev-
ing euhydration after mild dehydration of approximately 2%.
Their approach involved ingestion of 150% of the fluid lostduring a 30 minute period after a dehydration protocol consist-
ing of intermittent cycling exercise in a 32C environment.
Recovery of physiological markers of dehydration was fol-
lowed for 5.5 hr after ingesting the rehydration beverages. The
four beverages compared included sodium concentrations of 2,
26, 52, and 100 mmol/L. Although the fluid intake was con-
siderably larger than used in the prior research, neither the 2
mmol/L nor 26 mmol/L beverages resulted in complete recov-
ery of body water (66% and 82% recovery of body mass loss,
respectively) (Fig. 3). Both of the higher sodium beverages
resulted in complete (100%) rehydration by the end of the 5.5
hr monitoring period.
In an ambitious study designed to assess the interactive
effects of both sodium content and volume of fluid ingested in
rehydration, Shirreffs et al. [41] rehydrated subjects using
either 50%, 100%, 150%, or 200% of the volume lost and each
of these volumes contained either low sodium (23 mmol/L) or
higher sodium (61 mmol/L) concentration. Based on the net
fluid balance presented, body water recovery was nearly com-
plete (91% for both) with the lower sodium fluid when con-
sumed in both 150% and 200% excess but was incomplete with
either 50% volume (39% recovery) or 100% volume (60%
Sodium in Fluid Homeostasis with Exercise
JOURNAL OF THE AMERICAN COLLEGE OF NUTRITION 235S

8/10/2019 Tentang Jurnal Homeostasis
http://slidepdf.com/reader/full/tentang-jurnal-homeostasis 6/9
recovery) (Fig. 4). With the higher sodium content in ingested
fluid, recovery of the fluid deficit was complete with ingestion
of 150% of volume lost (107% recovery) while ingestion of
200% of volume lost resulted in a surplus of fluid (127%
recovery). Neither the 50% volume nor 100% volume fully
restored whole body fluid balance (38% recovery and 81%
recovery, respectively). Urine volume was positively related to
the volume of fluid ingested and inversely related to the content
of sodium in the rehydration beverage.
Multiple Regression of Sodium Concentration and
Fluid Volume
That recovery of total body water would depend on both the
sodium intake and the volume of fluid ingested may seem
intuitively obvious. The above reviewed studies provide an
evidentiary framework for quantifying this interactive effect.
Although each of these studies has compared rehydration be-
tween different volumes and between different intakes of so-
dium, there have been no attempts to use the combined data
from several studies in estimating the independent and interac-
tive contributions of fluid volume and sodium concentration to
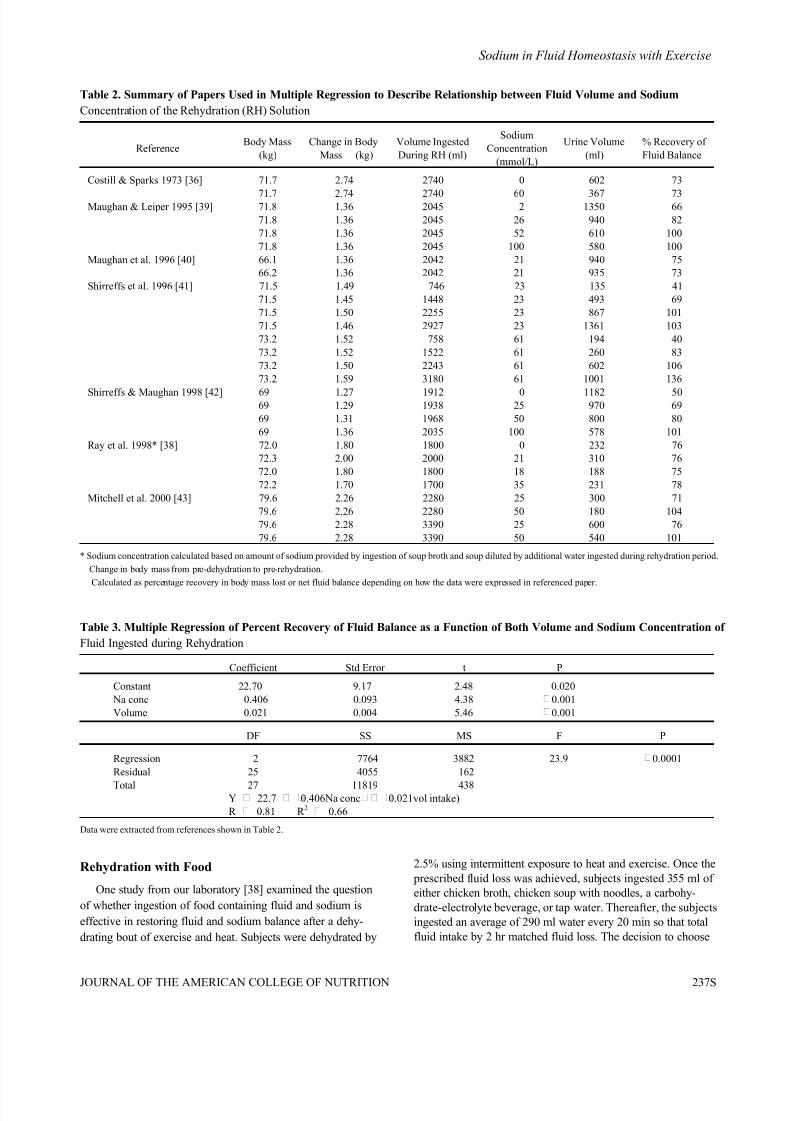
the rehydration process. The data displayed in Table 2 summa-rizing the findings of several rehydration studies were therefore
used in a multiple regression analysis to assess the relative
contributions of sodium concentration and fluid ingestion. In
each study, the data that were presented in the published paper
were either used directly (when provided by the authors) or the
relevant data were calculated from other results reported by the
authors. For the purpose of this analysis, whole-body rehydra-
tion (dependent variable) was expressed as the percentage
recovery of the fluid loss that had occurred during the dehy-
dration protocol. The reported sodium concentration of the
rehydration solution and the volume of this solution were used
as independent variables. Initially, additional variables wereentered into the regression model but none of the other vari-
ables achieved statistical significance (p 0.05). The variables
which did not significantly contribute to the prediction of fluid
recovery included urine volume during dehydration (likely due
to colinearity with sodium concentration), body mass (due to
low range of body mass in the reported studies), and duration
of rehydration period (which ranged from 2 6 hr).
The final regression model included both sodium concen-
tration (mmol/L) of the rehydration fluid and volume of this
solution consumed during the rehydration period (ml) as sig-
nificant predictors of percent recovery of fluid balance (Table
3). The resulting regression equation was
% rehydration 22.7 0.406 * Na 0.021 * volume
In the example of a 75 kg person who dehydrates by 2.5% and
ingests 100% of the volume lost during rehydration, a sodium
concentration of approximately 93 mmol/L would be required
to achieve fluid balance within 6 hr. On the other hand, if fluid
intake is increased to 150% of that lost in prior dehydration, the
regression model predicts that full rehydration could be
achieved with a sodium concentration of approximately 50
mmol/L. However, it must be noted that the regression model
accounts for only 66% of the variance in body water recovery.
It is likely that additional variables including temperature of the
ingested fluid, presence of other electrolytes (potassium, cal-
cium, magnesium) and nutrients (carbohydrate, amino acids),
arginine vasopressin and aldosterone, and osmolality of the
rehydration fluid also play important roles but are not included
in this regression model. Thus the present analysis is incom-
plete but does support the contention that both fluid volume and
sodium concentration are important considerations in the se-
lection and/or design of optimal rehydration solutions.
Fig. 3. Percent recovery of fluid balance during a 5.5-hr rehydration
period in which fluid was ingested at a volume equal to 150% of the
fluid deficit that was incurred. Rehydration was compared between
beverages containing 2 100 mmol/L sodium. Adapted from Maughan
and Leiper [39].
Fig. 4. Percent recovery of fluid balance during 6-hr rehydration period
in which both volume and sodium concentration of beverage were
varied. Adapted from Shirreffs et al. [41].
Sodium in Fluid Homeostasis with Exercise
236S VOL. 25, NO. 3
8/10/2019 Tentang Jurnal Homeostasis
http://slidepdf.com/reader/full/tentang-jurnal-homeostasis 7/9
Rehydration with Food
One study from our laboratory [38] examined the question
of whether ingestion of food containing fluid and sodium is
effective in restoring fluid and sodium balance after a dehy-
drating bout of exercise and heat. Subjects were dehydrated by
2.5% using intermittent exposure to heat and exercise. Once the
prescribed fluid loss was achieved, subjects ingested 355 ml of
either chicken broth, chicken soup with noodles, a carbohy-
drate-electrolyte beverage, or tap water. Thereafter, the subjects
ingested an average of 290 ml water every 20 min so that total
fluid intake by 2 hr matched fluid loss. The decision to choose
Table 2. Summary of Papers Used in Multiple Regression to Describe Relationship between Fluid Volume and Sodium
Concentration of the Rehydration (RH) Solution
ReferenceBody Mass
(kg)
Change in Body
Mass (kg)
Volume Ingested
During RH (ml)
Sodium
Concentration
(mmol/L)
Urine Volume
(ml)
% Recovery of
Fluid Balance
Costill & Sparks 1973 [36] 71.7 2.74 2740 0 602 73
71.7 2.74 2740 60 367 73Maughan & Leiper 1995 [39] 71.8 1.36 2045 2 1350 66
71.8 1.36 2045 26 940 82
71.8 1.36 2045 52 610 100
71.8 1.36 2045 100 580 100
Maughan et al. 1996 [40] 66.1 1.36 2042 21 940 75
66.2 1.36 2042 21 935 73
Shirreffs et al. 1996 [41] 71.5 1.49 746 23 135 41
71.5 1.45 1448 23 493 69
71.5 1.50 2255 23 867 101
71.5 1.46 2927 23 1361 103
73.2 1.52 758 61 194 40
73.2 1.52 1522 61 260 83
73.2 1.50 2243 61 602 106
73.2 1.59 3180 61 1001 136
Shirreffs & Maughan 1998 [42] 69 1.27 1912 0 1182 5069 1.29 1938 25 970 69
69 1.31 1968 50 800 80
69 1.36 2035 100 578 101
Ray et al. 1998* [38] 72.0 1.80 1800 0 232 76
72.3 2.00 2000 21 310 76
72.0 1.80 1800 18 188 75
72.2 1.70 1700 35 231 78
Mitchell et al. 2000 [43] 79.6 2.26 2280 25 300 71
79.6 2.26 2280 50 180 104
79.6 2.28 3390 25 600 76
79.6 2.28 3390 50 540 101
* Sodium concentration calculated based on amount of sodium provided by ingestion of soup broth and soup diluted by additional water ingested during rehydration period.
Change in body mass from pre-dehydration to pre-rehydration.
Calculated as percentage recovery in body mass lost or net fluid balance depending on how the data were expressed in referenced paper.
Table 3. Multiple Regression of Percent Recovery of Fluid Balance as a Function of Both Volume and Sodium Concentration of
Fluid Ingested during Rehydration
Coefficient Std Error t P
Constant 22.70 9.17 2.48 0.020
Na conc 0.406 0.093 4.38 0.001
Volume 0.021 0.004 5.46 0.001
DF SS MS F P
Regression 2 7764 3882 23.9 0.0001
Residual 25 4055 162
Total 27 11819 438Y 22.7 0.406Na conc 0.021vol intake)
R 0.81 R 2 0.66
Data were extracted from references shown in Table 2.
Sodium in Fluid Homeostasis with Exercise
JOURNAL OF THE AMERICAN COLLEGE OF NUTRITION 237S

8/10/2019 Tentang Jurnal Homeostasis
http://slidepdf.com/reader/full/tentang-jurnal-homeostasis 8/9
these products was based on commercial availability to
consumers as well as their varied amounts of electrolytes and
osmolality. With regard to sodium intake, chicken noodle soup
and chicken broth treatments provided a total sodium ingestion
of 50 mmol and 39 mmol, respectively. This is considerably
less than the sodium intake associated with the prior studies in
which subjects ingested 150% of the fluid loss with a sodium
concentration of 50 100 mmol/L. Using the regression model
from above, it is expected that the chicken broth and the
chicken noodle soup treatments would not fully restore the
fluid deficit in 3 hr (estimated % rehydration 73% for both).
Measured fluid recovery was 76% and 78% for the chicken
broth and chicken noodle soup, respectively. Although total
body fluid balance was not fully recovered in rehydration,
plasma volume was fully restored with the chicken broth and
the chicken noodle soup trials, but not with either a commercial
carbohydrate-electrolyte beverage or with water.
These findings illustrate the importance of ingestion of
sodium during the rehydration period not only for encouraging
increased retention of ingested fluids but also for restoration of
the plasma volume, which can be re-filled ahead of total fluid
balance when sufficient sodium is provided either in the rehy-
dration drink or in food consumed during rehydration. In ad-
dition, these findings show that it may not be necessary to
include sodium in every aliquot of fluid ingested during rehy-
dration if sufficient sodium is provided early in the rehydration
period either as a constituent of fluid or food.
SUMMARY AND CONCLUSION
Both sodium and fluid ingestion play important roles inmaintaining health and physiological function during physical
activity in hot environments. Whether people engage in pro-
longed endurance exercise such as marathons and triathlons or
if they are involved in occupational heat exposure during
physical activity, it is important that both fluid and sodium are
provided to offset the losses in both nutrients that occur as a
consequence of heavy sweating. People involved in vigorous
exercise in hot environments lose up to 3 liters of water and 3.5
grams of sodium per hour through sweating. Preventing these
fluid and sodium deficits helps to maintain both performance
and thermoregulation in such environments. The evidence from
published literature shows that fluid intake during exercise in a
warm environment is absolutely essential to attenuate the rise
in core temperature. These studies also demonstrate that unless
sodium is provided in the fluid replacement beverage, fluid
intake that matches or exceeds fluid loss may cause hypona-
tremia in some individuals participating in at least 4 hr of
exercise. Thus, many authors now recommend sodium concen-
tration of 20 50 mmol/L in beverages consumed during the
physical activity.
In designing a nutritional strategy for recovery from exer-
cise and heat exposure that results in mild dehydration, the dual
and interactive roles of fluid and sodium intake should be
considered. This synergistic association between fluid volume
and sodium intake is reflected in recommendations to consume
fluid in excess of that lost during the prior exercise and to
include sodium to increase the retention of the ingested liquids
by minimizing urine production. The papers reviewed here
suggest that plasma volume can be fully restored before total
body water deficits are fully corrected when sodium intake is
consumed either as a component of the rehydration beverage
with sodium concentration of approximately 20 mmol/L or
with food consumed in the early part of a rehydration period.
Using the meta-analysis presented in this paper, full recovery of
the fluid deficit within 6 hrs requires ingestion of a rehydration
solution containing 100 mmol/L sodium if consuming the same
volume of fluid that was lost in the prior dehydration. Alter-
natively, correction of the fluid deficit can also be achieved by
ingesting 150% of the volume lost if the rehydration solution
contains 50 mmol/L sodium.
REFERENCES
1. Senay LC Jr: Relationship of evaporative rates to serum [Na ],
[K ], and osmolarity in acute heat stress. J Appl Physiol 25:149
152, 1968.
2. Shapiro Y, Pandolf KB, Goldman RF: Predicting sweat loss re-
sponse to exercise, environment and clothing. Eur J Appl Physiol
48:83 96, 1982.
3. Allan JR, Wilson GG: Influence of acclimatization on sweat so-
dium concentration. J Appl Physiol 30:708 712, 1971.
4. Sawka MN, Toner MM, Francesconi RP, Pandolf KB: Hypohy-
dration and exercise: effects of heat acclimation, gender, andenvironment. J Appl Physiol 55:1147 1153, 1983.
5. Sawka MN, Montain SJ: Fluid and electrolyte supplementation for
exercise heat stress. Am J Clin Nutr 72(Suppl):564S 72S, 2000.
6. Costill DL: Sweating: its composition and effects on body fluids.
Ann NY Acad Sci 301:160 174, 1977.
7. Rehrer NJ: Fluid and electrolyte balance in ultra-endurance sport.
Sports Med 31:701 715, 2001.
8. Costill DL, Cote R, Fink W: Muscle water and electrolytes fol-
lowing varied levels of dehydration in man. J Appl Physiol 40:6
11, 1976.
9. Consolazio CF, Matoush LO, Nelson RA, Harding RS, Canham
JE: Excretion of sodium, potassium, magnesium and iron in human
sweat and the relation of each to balance and requirements. J Nutr
79:407 415, 1963.
10. Mao IF, Chen ML, Ko YC: Electrolyte loss in sweat and iodine
deficiency in a hot environment. Arch Environ Health 56:271 277,
2001.
11. Costa F, Calloway DH, Margen S: Regional and total body sweat
composition of men fed controlled diets. Am J Clin Nutr 22:52 58,
1969.
12. Shirreffs SM, Maughan RJ: Whole body sweat collection in hu-
mans: an improved method with preliminary data on electrolyte
content. J Appl Physiol 82:336 341, 1997.
13. Sanders B, Noakes TD, Dennis SC: Sodium replacement and fluid
Sodium in Fluid Homeostasis with Exercise
238S VOL. 25, NO. 3

8/10/2019 Tentang Jurnal Homeostasis
http://slidepdf.com/reader/full/tentang-jurnal-homeostasis 9/9
shifts during prolonged exercise in humans. Eur J Appl Physiol
84:419 425, 2001.
14. Convertino VA, Armstrong LE, Coyle EF, et al.: American Col-
lege of Sports Medicine position stand: exercise and fluid replace-
ment. Med Sci Sports Exerc 28:i vii, 1996.
15. Speedy DB, Campbell R, Mulligan G, et al: Weight changes and
serum sodium concentrations after an ultraendurance multisport
triathlon. Clin J Sport Med 7:100 103, 1997.16. Noakes TD: The hyponatremia of exercise. Int J Sport Nutr 2:205
228, 1992.
17. Irving RA, Noakes TD, Buck R et al.: Evaluation of renal function
and fluid homeostasis during recovery from exercise-induced hy-
ponatremia. J Appl Physiol 70:342 348, 1991.
18. Speedy DB, Noakes TD, Rogers IR, et al.: Hyponatremia in
ultradistance athletes. Med Sci Sports Exerc 31:809 815, 1999.
19. Hew TD, Chorley JN, Cianca JC, Divine JG: The incidence, risk
factors, and clinical manifestations of hyponatremia in marathon
runners. Clin J Sport Med 13:41 47, 2003.
20. Noakes T: Hyponatremia in distance runners: fluid and sodium
balance during exercise. Curr Sports Med Rep 1:197 207, 2002.
21. Hiller WDB, O Toole ML, Fortress EE, Laird RH, Imbert PI, Sisk
TD: Medical and physiological considerations in triathlons. Am J
Sport Med 15:164 167, 1987.
22. Luetkemeier MJ, Coles MG, Askew EW: Dietary sodium and
plasma volume levels with exercise. Sports Med 23:279 286,
1997.
23. Twerenbold R, Knechtle B, Kakebeeke TH, et al: Effects of
different sodium concentrations in replacement fluids during pro-
longed exercise in women. Br J Sports Med 37:300 303, 2003.
24. Vrijens DMJ, Rehrer NJ: Sodium-free fluid ingestion decreases
plasma sodium during exercise in the heat. J Appl Physiol 86:
1847 1851, 1999.
25. Montain SJ, Sawka MN, Wenger CB: Hyponatremia associated
with exercise: risk factors and pathogenesis. Exerc Sport Sci Rev
29:113 117, 2001.26. Gisolfi CV, Duchman SM: Guidelines for optimal replacement
beverages for different athletic events. Med Sci Sports Exerc
24:679 687, 1992.
27. Eichner ER: Exertional hyponatremia: why so many women.
Sports Med 24:54 56, 2002.
28. Barr SI, Costill DL, Fink WJ: Fluid replacement during prolonged
exercise: effects of water, saline, or no fluid. Med Sci Sport Exerc
23:811 817, 1991.
29. Brandenberger G, Candas V, Follenius M, Kahn JM: The influence
of the initial state of hydration on endocrine responses to exercise
in the heat. Eur J Appl Physiol 58:674 679, 1989.
30. Cade R, Spooner G, Schlein E, Pickering M, Dean R: Effect of
fluid, electrolyte, and glucose replacement during exercise on
performance, body temperature, rate of sweat loss, and composi-
tional changes of extracellular fluid. J Sports Med Phys Fitn
12:150 156, 1972.
31. Greenleaf JE, Brock PJ: Na
and Ca2
ingestion: plasma volume-
electrolyte distribution at rest and exercise. J Appl Physiol 48:838
847, 1980.
32. Powers SL, Lawler J, Dodd S, Tulley R, Landry G, Wheeler K:Fluid replacement drinks during exercise: effects on minimizing
exercise-induced disturbances in homeostasis. Eur J Appl Physiol
60:54 60, 1990.
33. Nose H, Mack GW, Shi X, Nadel ER: Involvement of sodium
retention hormones during rehydration in humans. J Appl Physiol
65:332 336, 1988.
34. Nose H, Mack GW, Shi X, Nadel ER: Role of osmolality and
plasma volume during rehydration in humans. J Appl Physiol
65:325 331, 1988.
35. Wemple RD, Morocco TS, Mack GW: Influence of sodium re-
placement on fluid ingestion following exercise-induced dehydra-
tion. Int J Sport Nutr 7:104 116, 1997.
36. Costill DL, Sparks KE: Rapid fluid replacement following thermal
dehydration. J Appl Physiol 34:299 303, 1973.
37. Gonzalez-Alonzo J, Heaps CL, Coyle EF: Rehydration after exer-
cise with common beverages and water. Int J Sports Med 13:399
406, 1992.
38. Ray ML, Bryan MW, Ruden TM, Baier SM, Sharp RL, King DS:
Effect of sodium in a rehydration beverage when consumed as a
fluid or meal. J Appl Physiol 85:1329 1336, 1998.
39. Maughan RJ, Leiper JB: Sodium intake and post-exercise rehydra-
tion in man. Eur J Appl Physiol 71:311 319, 1995.
40. Maughan RJ, Leiper JB, Shirreffs SM: Restoration of fluid balance
after exercise-induced dehydration: effects of food and fluid in-
take. Eur J Appl Physiol 73:317 325, 1996.
41. Shirreffs SM, Taylor AJ, Leiper JB, Maughan RJ: Post-exercise
rehydration in man: effects of volume consumed and drink sodiumcontent. Med Sci Sports Exerc 28:1260 1271, 1996.
42. Shirreffs SM, Maughan RJ: Volume repletion after exercise-
induced volume depletion in humans: replacement of water and
sodium losses. Am J Physiol 274(Renal Physiol 43):F868 F875,
1998.
43. Mitchell JB, Phillips MD, Mercer SP, Baylies HL, Pizza FX:
Postexercise rehydration: effect of Na
and volume on restoration
of fluid spaces and cardiovascular function. J Appl Physiol 89:
1302 1309, 2000.
Received January 9, 2006.
Sodium in Fluid Homeostasis with Exercise
JOURNAL OF THE AMERICAN COLLEGE OF NUTRITION 239S