telavancin
TRANSCRIPT
Nature Reviews | Drug Discovery
HN
NH
O
OH
OO
O OHOH
OH
NH
O
HN
OHN
NH
HN
NH
H2N
O
O
OOH
H
O
H
HO
HOHO
HN
O
P OHOH
OH
NH
HO2
7
C
O
ClO
OCl
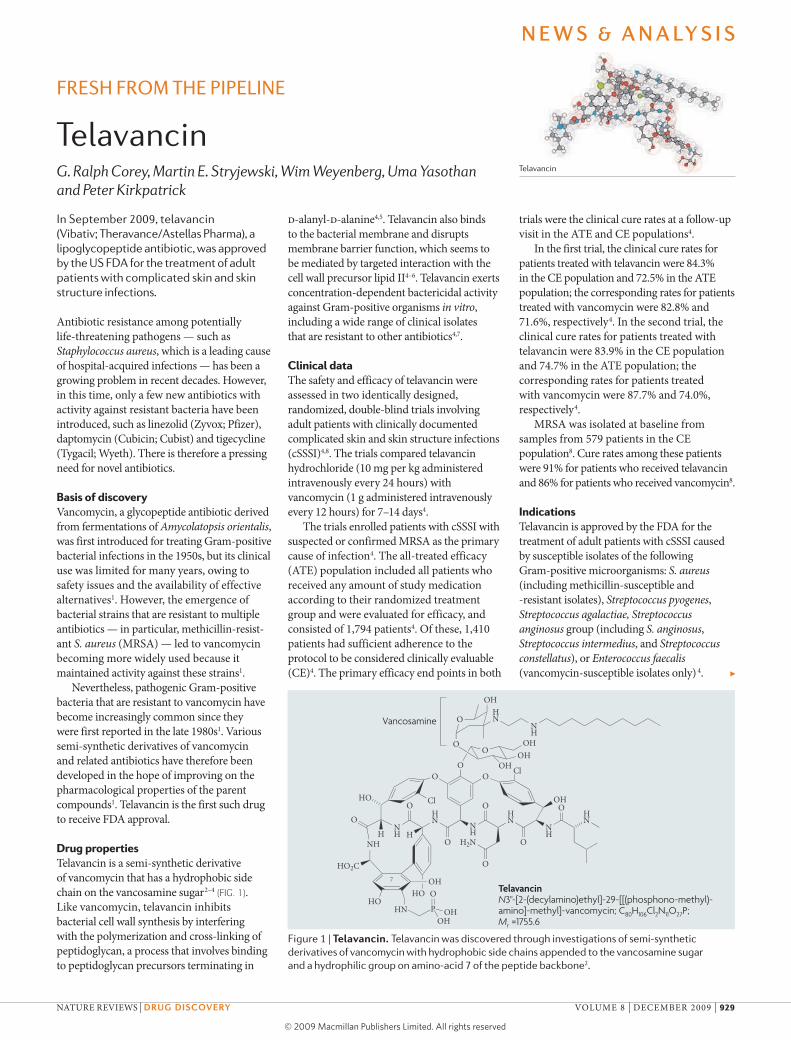
TelavancinN3''-[2-(decylamino)ethyl]-29-[[(phosphono-methyl)-amino]-methyl]-vancomycin; C80H106Cl2N11O27P; Mr =1755.6
Vancosamine
fresh from the pipeline
TelavancinG. Ralph Corey, Martin E. Stryjewski, Wim Weyenberg, Uma Yasothan and Peter Kirkpatrick
Telavancin
In September 2009, telavancin (Vibativ; Theravance/Astellas Pharma), a lipoglycopeptide antibiotic, was approved by the US FDA for the treatment of adult patients with complicated skin and skin structure infections.
Antibiotic resistance among potentially life-threatening pathogens — such as Staphylococcus aureus, which is a leading cause of hospital-acquired infections — has been a growing problem in recent decades. However, in this time, only a few new antibiotics with activity against resistant bacteria have been introduced, such as linezolid (Zyvox; Pfizer), daptomycin (Cubicin; Cubist) and tigecycline (Tygacil; Wyeth). There is therefore a pressing need for novel antibiotics.
Basis of discoveryVancomycin, a glycopeptide antibiotic derived from fermentations of Amycolatopsis orientalis, was first introduced for treating Gram-positive bacterial infections in the 1950s, but its clinical use was limited for many years, owing to safety issues and the availability of effective alternatives1. However, the emergence of bacterial strains that are resistant to multiple antibiotics — in particular, methicillin-resist-ant S. aureus (MRSA) — led to vancomycin becoming more widely used because it maintained activity against these strains1.
Nevertheless, pathogenic Gram-positive bacteria that are resistant to vancomycin have become increasingly common since they were first reported in the late 1980s1. Various semi-synthetic derivatives of vancomycin and related antibiotics have therefore been developed in the hope of improving on the pharmacological properties of the parent compounds1. Telavancin is the first such drug to receive FDA approval.
Drug propertiesTelavancin is a semi-synthetic derivative of vancomycin that has a hydrophobic side chain on the vancosamine sugar2–4 (FIG. 1). Like vancomycin, telavancin inhibits bacterial cell wall synthesis by interfering with the polymerization and cross-linking of peptidoglycan, a process that involves binding to peptidoglycan precursors terminating in
d-alanyl-d-alanine4,5. Telavancin also binds to the bacterial membrane and disrupts membrane barrier function, which seems to be mediated by targeted interaction with the cell wall precursor lipid II4–6. Telavancin exerts concentration-dependent bactericidal activity against Gram-positive organisms in vitro, including a wide range of clinical isolates that are resistant to other antibiotics4,7.
Clinical dataThe safety and efficacy of telavancin were assessed in two identically designed, randomized, double-blind trials involving adult patients with clinically documented complicated skin and skin structure infections (cSSSI)4,8. The trials compared telavancin hydrochloride (10 mg per kg administered intravenously every 24 hours) with vancomycin (1 g administered intravenously every 12 hours) for 7–14 days4.
The trials enrolled patients with cSSSI with suspected or confirmed MRSA as the primary cause of infection4. The all-treated efficacy (ATE) population included all patients who received any amount of study medication according to their randomized treatment group and were evaluated for efficacy, and consisted of 1,794 patients4. Of these, 1,410 patients had sufficient adherence to the protocol to be considered clinically evaluable (CE)4. The primary efficacy end points in both
trials were the clinical cure rates at a follow-up visit in the ATE and CE populations4.
In the first trial, the clinical cure rates for patients treated with telavancin were 84.3% in the CE population and 72.5% in the ATE population; the corresponding rates for patients treated with vancomycin were 82.8% and 71.6%, respectively4. In the second trial, the clinical cure rates for patients treated with telavancin were 83.9% in the CE population and 74.7% in the ATE population; the corres ponding rates for patients treated with vancomycin were 87.7% and 74.0%, respectively4.
MRSA was isolated at baseline from samples from 579 patients in the CE population8. Cure rates among these patients were 91% for patients who received telavancin and 86% for patients who received vancomycin8.
IndicationsTelavancin is approved by the FDA for the treatment of adult patients with cSSSI caused by susceptible isolates of the following Gram-positive microorganisms: S. aureus (including methicillin-susceptible and -resistant isolates), Streptococcus pyogenes, Streptococcus agalactiae, Streptococcus anginosus group (including S. anginosus, Streptococcus intermedius, and Streptococcus constellatus), or Enterococcus faecalis (vancomycin-susceptible isolates only) 4. ▶
Figure 1 | Telavancin. Telavancin was discovered through investigations of semi-synthetic derivatives of vancomycin with hydrophobic side chains appended to the vancosamine sugar and a hydrophilic group on amino-acid 7 of the peptide backbone2.
N e w s & a N a ly s i s
NATuRE REVIEWS | Drug Discovery VOLuME 8 | DECEMbER 2009 | 929
© 2009 Macmillan Publishers Limited. All rights reserved

AnAlysis | mrsa InfeCtIons
▶
Box 1 | the market for telavancin
Analysing the market for telavancin are Wim Weyenberg and Uma yasothan, ims health, london, UK.
the global market for drugs to treat methicillin-resistant Staphylococcus aureus (mrsA) was worth over Us$2.43 billion in 2008 (of which sales in the Us were $1.56 billion), and has shown a growth of more than 68% over the past 3 years14. the key antibiotics in this market are vancomycin, linezolid (Zyvox; pfizer), daptomycin (Cubicin; Cubist) and tigecycline (tygacil; Wyeth). the market leader in this mrsA subsegment is linezolid, with sales of $1.05 billion, followed by vancomycin, with sales of $838 million14.
telavancin (Vibativ; theravance/Astellas pharma), a lipoglycopeptide antibiotic that has recently been approved by the fDA for the treatment of complicated skin and skin structure infections, is the latest entrant to the mrsA subsegment of the antibiotics market. it has also shown non-inferiority to the standard of care treatment vancomycin in phase iii trials for the treatment of hospital-acquired pneumonia (hAp), and a new drug application for this indication was submitted in January 2009. Analysts estimate that telavancin sales will be $5 million in 2009, following a launch in the fourth quarter. these figures are predicted to reach $200 million by 2013, assuming that telavancin also gains approval for the hAp indication15,16.
Analysing issues in the treatment of infections due to MRSA are G. Ralph Corey, M.D., Professor of Medicine, and Martin E. Stryjewski, M.D., Adjunct Professor of Medicine, Division of Infectious Diseases, Duke university Medical Center, North Carolina, uSA.
Over the past decade, uS clinicians have observed an epidemic of cutaneous infections due to MRSA acquired in the community. This new MRSA (usually clone uSA300), together with its nosocomial-based relative, now produce the majority of invasive cutaneous infections that are seen in both healthy and hospitalized patients9,10. The treatment for these and other serious infections due to MRSA has centred on vancomycin, but this drug has several drawbacks: the need for intravenous administration, a slowly developing bactericidal effect and a gradually worsening resistance profile11,12. However, only linezolid, daptomycin and tigecycline have been approved for cSSSI due to MRSA in the past 10 years. The recent FDA approval of telavancin for cSSSI, particularly for infections due to MRSA, is therefore welcome.
Telavancin has several novel characteristics. It has rapid, concentration-dependent bactericidal activity against Gram-positive bacteria. Peak serum levels are several logs above the reported minimum inhibitory concentrations for MRSA5,13, which is important for the minority of patients with cSSSI (2–5%) who develop bacteraemia. Telavancin has a dual mechanism of action, which portends a slower rate of development of resistance5. Indeed, the development of resistance has not been detected in clinical
trials with telavancin. Furthermore, telavancin is not sequestered in the alveolar space, making it a potentially effective agent for pneumonic infections.
Two large, identically designed clinical trials involving patients with cSSSI treated with telavancin or vancomycin have been completed8. Co-primary outcomes included non-inferiority of telavancin to vancomycin in the CE population of each individual trial and superiority of telavancin over vancomycin in the ATE pooled population infected with MRSA from both trials. The first end point was met, but the second was not.
Clinicians must consider several safety issues when undertaking therapy with telavancin. First, telavancin is associated with reversible renal dysfunction in a small proportion of patients. Second, the efficacy of telavancin may be decreased in a small subgroup of patients with severe renal insufficiency. Third, all clinical trials in cSSSI have excluded very sick patients (for example, those with necrotizing fasciitis), and so the efficacy of new compounds in the treatment of life-threatening infections is unknown. Fourth, because of concern about fetal teratogenicity, a pregnancy test should be performed in women of child-bearing potential before prescribing telavancin. Finally, the role of antibiotics proven to be non-inferior to the standard of care in patients with cSSSI provides the physician with an alternative to standard therapy rather than a new first choice. Nevertheless, having new bactericidal agents to treat infections due to S. aureus, particularly MRSA, is important in the ongoing battle against this evolving, aggressive pathogen.
Important questions concerning the diagnosis and treatment of cSSSI remain: can
we effectively treat these infections for shorter periods (for example, 3 days) with higher doses of a rapidly bactericidal agent; which abscesses require only drainage with or without a single dose of antibiotic; and which patients require broader-spectrum therapy (or more invasive diagnostic efforts) because of their immune and/or circulatory status? Answering these questions will help to better delineate the role of new as well as old antibiotics in the treatment of patients with cSSSI.
G. Ralph Corey and Martin E. Stryjewski are at Duke University Medical Center, Durham,
North Carolina 27710, USA.
Wim Weyenberg and Uma Yasothan are at IMS Health, 7 Harewood Avenue, London, NW1 6JB, UK.
Peter Kirkpatrick is at Nature Reviews Drug Discovery.
e-mails: [email protected]; [email protected]; [email protected]
doi:10.1038/nrd3051
1. Van Bambeke, F. Glycopeptides in clinical development: pharmacological profile and clinical perspectives. Curr. Opin. Pharmacol. 4, 471–478 (2004).
2. Leadbetter, M. R. et al. Hydrophobic vancomycin derivatives with improved ADME properties: discovery of telavancin (TD-6424). J. Antibiot. 57, 326–336 (2004).
3. Hegde, S. S. et al. Pharmacodynamics of telavancin (TD-6424), a novel bactericidal agent, against Gram-positive bacteria. Antimicrob. Agents Chemother. 48, 3043–3050 (2004).
4. Food and Drug Administration. FDA labelling information. FDA website [online] <http://www.accessdata.fda.gov/drugsatfda_docs/label/2009/022110s000lbl.pdf> (2009).
5. Higgins, D. L. et al. Telavancin, a multifunctional lipoglycopeptide, disrupts both cell wall synthesis and cell membrane integrity in methicillin-resistant Staphylococcus aureus. Antimicrob. Agents Chemother. 49,1127–1134 (2005).
6. Lunde, C. S. et al. Telavancin disrupts the functional integrity of the bacterial membrane through targeted interaction with the cell wall precursor lipid II. Antimicrob. Agents Chemother. 53, 3375–3383 (2009).
7. Krause, K. M. et al. In vitro activity of telavancin against resistant Gram-positive bacteria. Antimicrob. Agents Chemother. 52, 2647–2652 (2008).
8. Stryjewski, M. E. et al. Telavancin versus vancomycin for the treatment of complicated skin and skin-structure infections caused by Gram-positive organisms. Clin. Infect. Dis. 46, 1683–1693 (2008).
9. King, M. D. et al. Emergence of community-acquired methicillin-resistant Staphylococcus aureus USA 300 clone as the predominant cause of skin and soft-tissue infections. Ann. Intern. Med. 144, 309–317 (2006).
10. Moran, G. J. et al. Methicillin-resistant S. aureus infections among patients in the emergency department. N. Engl. J. Med. 355, 666–674 (2006).
11. Wang, G. et al. Increased vancomycin MICs for Staphylococcus aureus clinical isolates from a university hospital during a 5-year period. J. Clin. Microbiol. 44, 3883–3886 (2006).
12. Tenover, F. C. Vancomycin-resistant Staphylococcus aureus: a perfect but geographically limited storm? Clin. Infect. Dis. 46, 675–677 (2008).
13. Sun, H. K. et al. Tissue penetration of telavancin after intravenous administration in healthy subjects. Antimicrob. Agents Chemother. 50, 788–790 (2006).
14. IMS MIDAS (IMS Health, 2009).15. Sanderson, I. et al. Specialty Pharmaceuticals (Cowen
and Company,14 Sep 2009).16. Urist, M. & Harr, S. JP Morgan North America Equity
Research Report (JP Morgan & Chase, 23 Jul 2009).
Competing interests statementG.R.C. and M.E.S declare competing financial interests: see web version for details.
N e w s & a N a ly s i s
930 | DECEMbER 2009 | VOLuME 8 www.nature.com/reviews/drugdisc
© 2009 Macmillan Publishers Limited. All rights reserved