sesi_6,_7a_blok_i
TRANSCRIPT
8/12/2019 Sesi_6,_7A_Blok_I
http://slidepdf.com/reader/full/sesi67abloki 1/19
8/12/2019 Sesi_6,_7A_Blok_I
http://slidepdf.com/reader/full/sesi67abloki 2/19
ISU-ISU SISTEM PELAYANANKESEHATAN DI BERBAGAI NEGARA
• PEMERATAAN• PENINGKATAN BIAYA
PEL.KES• EFISIENSI
• KUALITAS• AKUNTABILITAS&
SUSTAINABILITAS
(Neg.berkembang)
8/12/2019 Sesi_6,_7A_Blok_I
http://slidepdf.com/reader/full/sesi67abloki 3/19
Sistem Asuransi di
Negara• USA
• Kanada• Jerman
• Filipina• Thailand
• Indonesia
8/12/2019 Sesi_6,_7A_Blok_I
http://slidepdf.com/reader/full/sesi67abloki 4/19
Sistem Asuransi
Kesehatan di Amerika• Multipayer Umumnya komersial dan
lebih percaya pada mekanismepasar
• 38 Juta tidak terasuransi, 85%
diantaranya kelompok perkerja.
• Medicare
• Medicaid
• HMO Act 1973
8/12/2019 Sesi_6,_7A_Blok_I
http://slidepdf.com/reader/full/sesi67abloki 5/19
Sistem Asuransi
Kesehatan di Kanada• Tidak seperti Inggris, tidak seperti
Amerika• Dana pemerintah Pusat diberikan ke
badan publik independen yg
berorientasi nirlaba dan bertg jawab
pada PEMDA PROPINSI (50:50)
sekarang block grant• Mulai dari rawat inap
8/12/2019 Sesi_6,_7A_Blok_I
http://slidepdf.com/reader/full/sesi67abloki 6/19
Si t A i di
8/12/2019 Sesi_6,_7A_Blok_I
http://slidepdf.com/reader/full/sesi67abloki 7/19
Sistem Asuransi di
FilipinaDi mulai 1997 dg UU
Asuransi Kesehatan Nasional
penyelenggara PHIC
Monopoli
Paket rawat inap
Cakupan 60% (wajib)
H lth I I
8/12/2019 Sesi_6,_7A_Blok_I
http://slidepdf.com/reader/full/sesi67abloki 8/19
Health Insurance In
Thailand• Medical Welfare Scheme (MWS) : cover indigence,
health card for community leaders and health
volunteer
• Civil Servant Medical Benefit Scheme(CSMBS)
• Compulsory Health Insurance : Social SecurityScheme(SSS), Workmen Compensation Scheme
(WCS), and Traffic Accident Insurance (TA).• Voluntary Health Insurance : Private Insurance (PI),
Voluntary Health Card (VHC).
8/12/2019 Sesi_6,_7A_Blok_I
http://slidepdf.com/reader/full/sesi67abloki 9/19
• Objective : fringe benefits for government workers
and to compensate their low salaries.
• Basic concepts of these scheme are public welfare
for government workers; retrospective FFS
payment, free choices of access without co-payment.
• Beneficiaries include government workers and theirfamilies, estimated millions.
• Beneficiaries are free to choose public or private
care but limited payment to private care.
The Civil Servants Medical Benefit Scheme
8/12/2019 Sesi_6,_7A_Blok_I
http://slidepdf.com/reader/full/sesi67abloki 10/19
Compulsory Health Insurance
• The Workmen Compensation Scheme (WCS):
cover sickness and injuries due to work-related.
Contributions are paid by employers based onexperience-rate.
• The Social Security Scheme (SSS) : started infor enterprises with and more workers
and expanded to those with or more workers in
. In , it aims to extend to those or
more workers.
• The Traffic Accident Insurance (TA) : compulsoryfor all car owners.
8/12/2019 Sesi_6,_7A_Blok_I
http://slidepdf.com/reader/full/sesi67abloki 11/19
H lth I I
8/12/2019 Sesi_6,_7A_Blok_I
http://slidepdf.com/reader/full/sesi67abloki 12/19
Health Insurance In
Thailand
• % public subsidized
scheme; MWS, CSMBS• % public subsidized scheme;
VHC
• % public subsidized scheme:SSS
• unsubsidized scheme; WCS,TAI, PI
8/12/2019 Sesi_6,_7A_Blok_I
http://slidepdf.com/reader/full/sesi67abloki 13/19
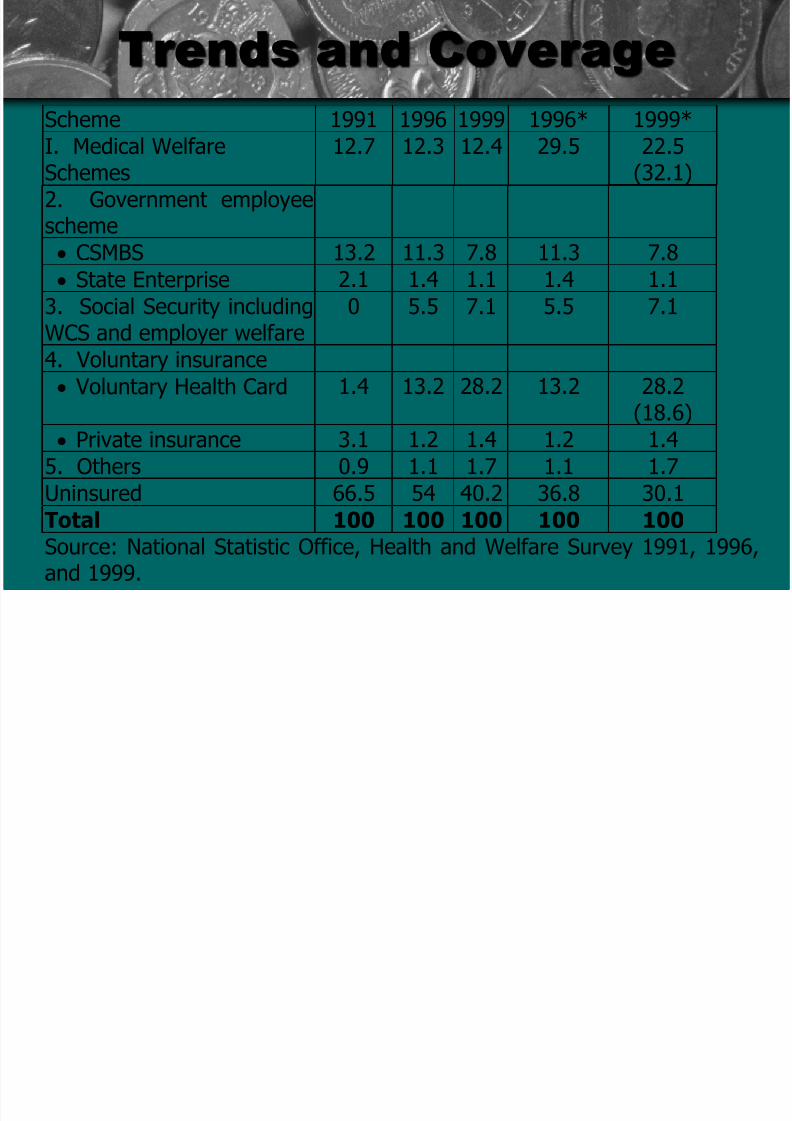
Trends and Coverage
Scheme 1991 1996 1999 1996* 1999*
I. Medical WelfareSchemes
12.7 12.3 12.4 29.5 22.5(32.1)
2. Government employeescheme
• CSMBS 13.2 11.3 7.8 11.3 7.8
• State Enterprise 2.1 1.4 1.1 1.4 1.1
3. Social Security includingWCS and employer welfare
0 5.5 7.1 5.5 7.1
4. Voluntary insurance
• Voluntary Health Card 1.4 13.2 28.2 13.2 28.2
(18.6)• Private insurance 3.1 1.2 1.4 1.2 1.4
5. Others 0.9 1.1 1.7 1.1 1.7
Uninsured 66.5 54 40.2 36.8 30.1
Total 100 100 100 100 100Source: National Statistic Office, Health and Welfare Survey 1991, 1996,and 1999.
Fi i M d l d id
8/12/2019 Sesi_6,_7A_Blok_I
http://slidepdf.com/reader/full/sesi67abloki 14/19
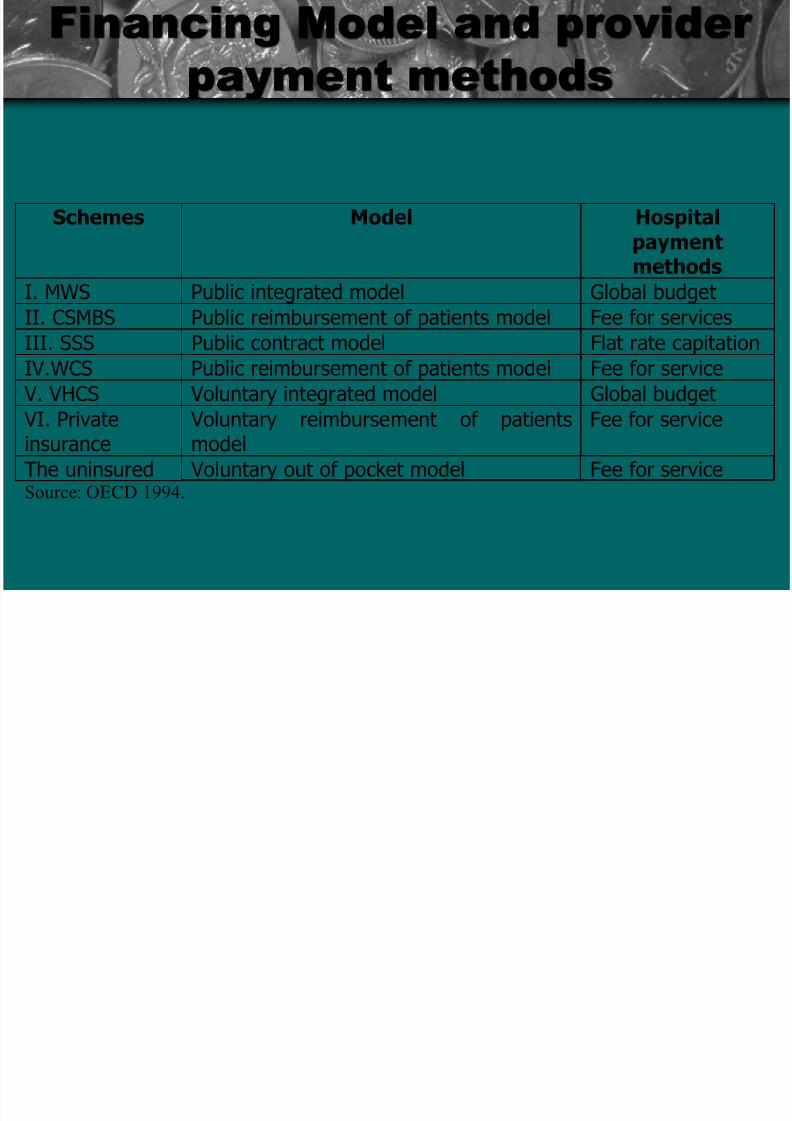
Schemes Model Hospital
paymentmethods
I. MWS Public integrated model Global budget
II. CSMBS Public reimbursement of patients model Fee for servicesIII. SSS Public contract model Flat rate capitation
IV.WCS Public reimbursement of patients model Fee for service
V. VHCS Voluntary integrated model Global budget
VI. Privateinsurance
Voluntary reimbursement of patientsmodel
Fee for service
The uninsured Voluntary out of pocket model Fee for serviceSource: OECD 1994.
Financing Model and provider
payment methods
8/12/2019 Sesi_6,_7A_Blok_I
http://slidepdf.com/reader/full/sesi67abloki 15/19
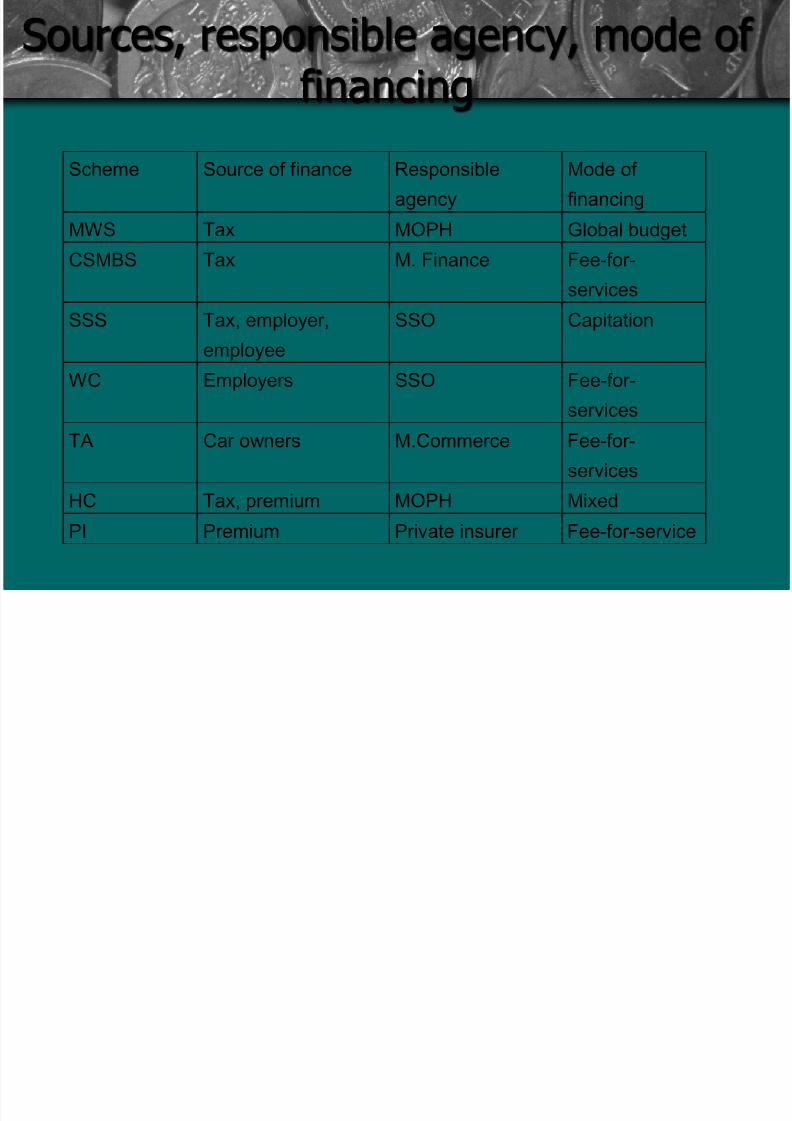
Sources, responsible agency, mode of
financingScheme Source of finance Responsible
agency
Mode of
financingMWS Tax MOPH Global budget
CSMBS Tax M. Finance Fee-for-
services
SSS Tax, employer,
employee
SSO Capitation
WC Employers SSO Fee-for-
servicesTA Car owners M.Commerce Fee-for-
services
HC Tax, premium MOPH Mixed
PI Premium Private insurer Fee-for-service
8/12/2019 Sesi_6,_7A_Blok_I
http://slidepdf.com/reader/full/sesi67abloki 16/19
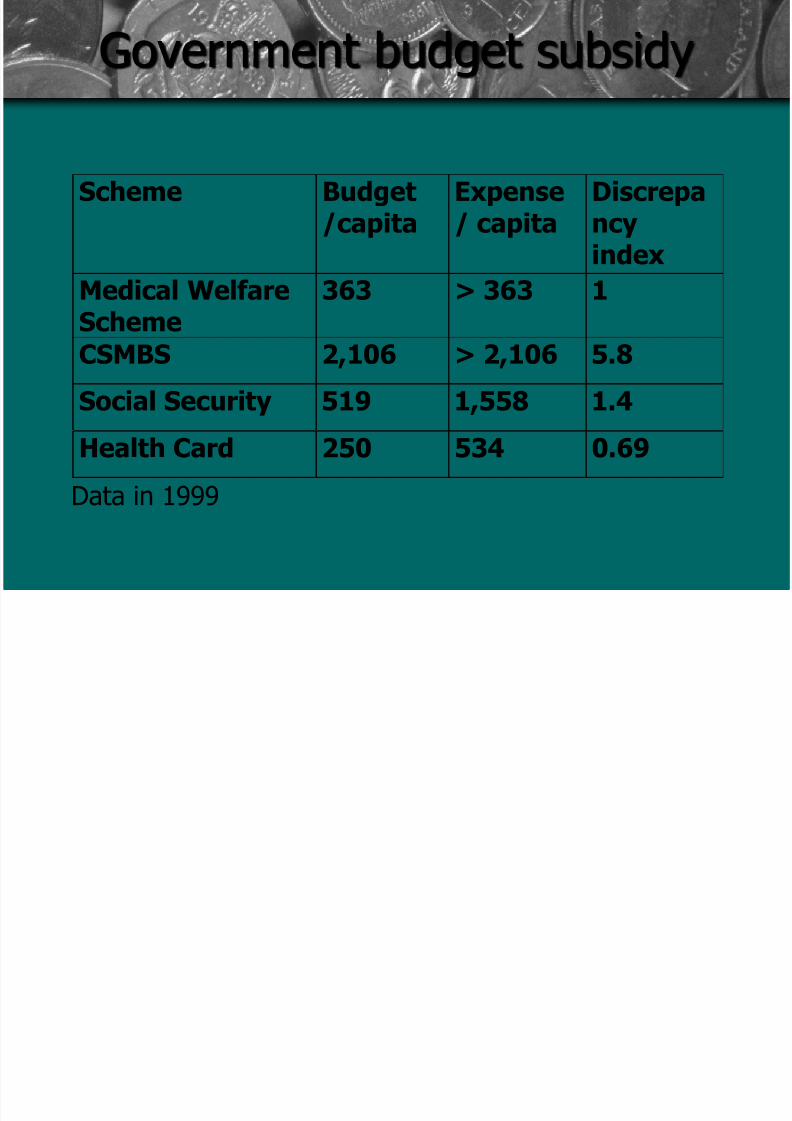
Government budget subsidy
Scheme Budget/capita
Expense/ capita
Discrepancyindex
Medical Welfare
Scheme
363 > 363 1
CSMBS 2,106 > 2,106 5.8
Social Security 519 1,558 1.4
Health Card 250 534 0.69
Data in 1999
8/12/2019 Sesi_6,_7A_Blok_I
http://slidepdf.com/reader/full/sesi67abloki 17/19
P i A i i
8/12/2019 Sesi_6,_7A_Blok_I
http://slidepdf.com/reader/full/sesi67abloki 18/19
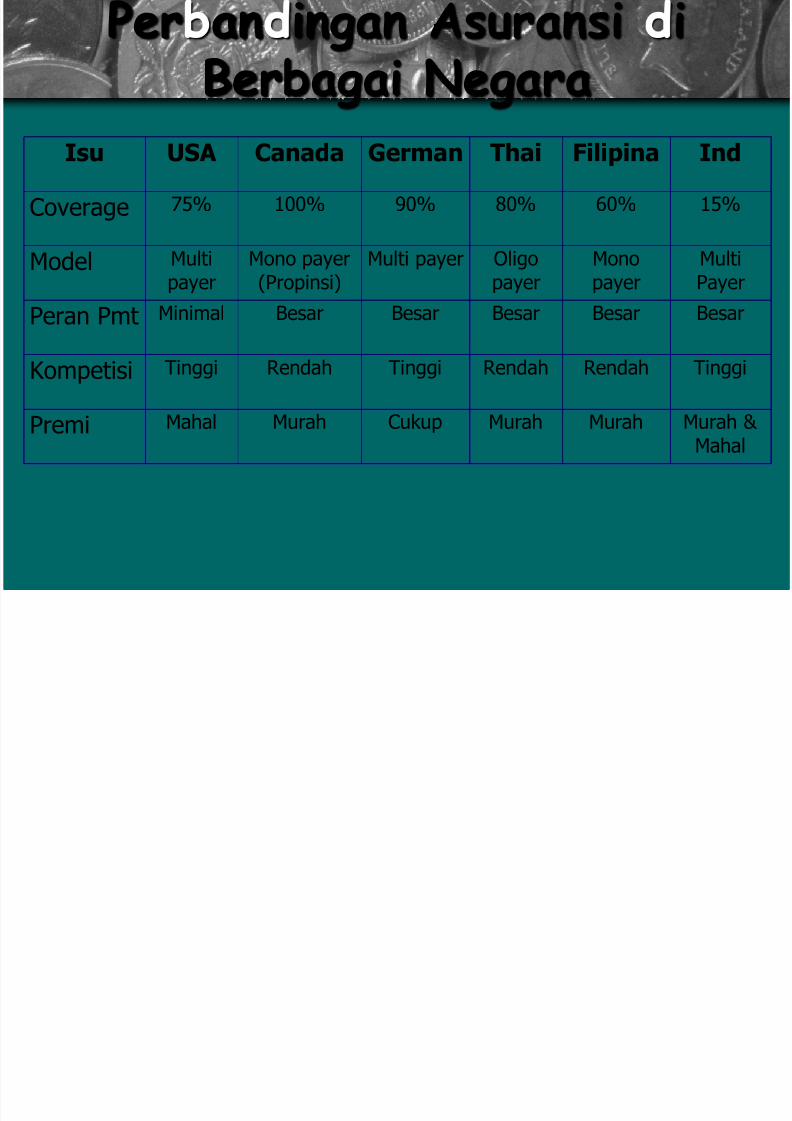
Per an ingan Asuransi i
Berbagai NegaraIsu USA Canada German Thai Filipina Ind
Coverage 75% 100% 90% 80% 60% 15%
Model Multipayer
Mono payer(Propinsi)
Multi payer Oligopayer
Monopayer
MultiPayer
Peran Pmt Minimal Besar Besar Besar Besar Besar
Kompetisi Tinggi Rendah Tinggi Rendah Rendah Tinggi
Premi Mahal Murah Cukup Murah Murah Murah & Mahal
8/12/2019 Sesi_6,_7A_Blok_I
http://slidepdf.com/reader/full/sesi67abloki 19/19
Kesimpulan
• Umumnya Sifat asuransi kesehatan not-
for profit, kecuali USA
• Cakupannya tinggi
• Beberapa dikelola oleh badan independen
• Satuan terkecil Badan pelaksana bukandistrik tetapi propinsi
• Ada keterkaitan sistem asuransi
kesehatan dan tingkat kesehatan
penduduk