penchun saenprasarnmedinfo.psu.ac.th/pr/pr2008/pr20080301_document.pdf · 2008-03-03 · errors and...
TRANSCRIPT

Copyright JCAHO 2001 1
PenchunSaenprasarn

Copyright JCAHO 2001 2
����������������� �� ��������� �������� �������������� �������������������� ����!��"� ����#�"����$ ������"���%���%!�&�' ��"(���%���"��.
Overall Req.
Multiple Req.
II 8 1.2 ��������������� �� ���������� ���������(Risk, Safety, and Quality Management System)
1
����� ����"������� ���������� ��H
! �����I���J�������J��K�������� ��
"J�� ���L�"���M��"� , �N ����,
��!����L��� �"��������� ����L�"���O������ ������ ����������
������ ������������������
������O����L�
�"!�PK��
�����������/���������� ������ KPI�����"#���$#%��������
". ��������������� ��������������
�. �����"���%���%!�&�2
3
4
1
2
34
6
5
��� "���%���%!�&� ��$ ������"���%���J�����"��Q���M�����
Monitor ��������������"��� "������������� ��
Copyright JCAHO 2001 3
��
���������������
����������� ��� ������� ��!�"� ��!���������������#���������$ %������%"����% �������� ����������&��'( �) ������
*���) +�������(���� �����&��&%��)�)��

Copyright JCAHO 2001 4
� ������������������� : ������ ��!"�#��$� %&�'%&�
$�('� �*���+,���$��$ "��� ���$��- �.&��/�����0%#'��%3� .���� �*4��%&� �* 2 6�� "!4 �%#'%(�7+(���6�� "!4 �%�8*�.�9:;<� 3�� >� .-"���4��%&� �* 2 9$+,���$��$ "��� �+'���6�� ".&�9$.4�+(6?#�� ��A;<�: >'��'���� ��� ����%�&� .&����$��B�+'���"��%'�'���� ��� 4'%#'%(�7+(!4 �9"� A���$%-��(��' A��%#'���$#��$� %&�'%&�:��4��%&� �* 2 ;8��� 4��%&� �*2 ��&�%$�"4��%&����� A6�","+,��-�'9($ ". '.�!4 �
Copyright JCAHO 2001 5
����������%��*��� A���A�&
� 4��%&� �* 4 (���A�&)!"���,�,�����A�&��$�? ' �����'('�'�>6?���%4FA#��$������%,'9�.&�9"� A����9�%:�-?������9#A�� %$8*�%(F'6�"%,''�>��$��,�,�����A�&4����.4�+(.� �%4�:��9:(�8�6?A��(��:��4��%&� �*4(��.) ��A ' �*%�8*�(� ��� ���(�8�%������+(;?���B�.�#���H��4��%&� �*4 (���A�&) $�9"+,���$��$ "��� �����%,'���A�&6?$���,�,��� '�<�$���$��- �.&��/�����0 4��%&� �* 4(���A�&)4<�$����$6�"4�����$I��

Copyright JCAHO 2001 6
� �� "6&& �B : the 5 “Ds”
DeathDiseaseDisabilityDiscomfort
Dissatisfaction

Copyright JCAHO 2001 7
� Patient Safety "#$%&()*$+,-./0+1,234$5"1673$+,-./0+1,8+8#$:;8/6=1++1,.1&>=?. +1,>@A46$B)6 5,C#+1,@;D>@A6 (A4>+E&F3*0,-5/1$+1,&;HI,)+J1 234$K/1"8I#&B)6F#$:;8/6L#$+1,,-..HI-+,-./0+1,(A48ME.)LE%&N0+1,8#$+)0>5LO+1,P%"R3$8,-@$K
� N0>SE$:II)RT K/1"8I#&B)6F#$:;8/65"1673$ +1,8,1U=1+#)0L,16(A4>+E&=1+#O.)LE>5LO,-5/1$>F1,).+1,.,E+1,@OB1R5,C#@B1/-+1,8,1U=1+B)6 #)0L,16 +1,.1&>=?. +1,>@A46$B)6 5,C#+1,@;D>@A6(A4=-+#N5>+E&+1,.1&>=?.L#:;8/6 K/1">@A6516L#(,)R6@E0
Copyright JCAHO 2001 8
- %(�7���09$�<�#��-�� (adverse event-AE) ��������������:����� �!"� #$��%&�'%$ (�)*+���,�#� �'%$���-�./0�123�*425�#6��7 ,1�2�38���!����� 9+����:� /&. ���& !��;�5�9�3<)=@/0N5D>+E&=1+K/1":E&RI1&N0+1,&;HI,)+J1 (medical errors)80% >+E&=1+K/1":E&RI1&F#$"0OJ6 K/1"I">5I/N0+1,L)&@E0N=@$:I:E&RI1&
- ������ (error) : ����C�2���������=2���.3!�����)�2+�� '�6#���%�D2E!.)�'�6#����C�2��E 7���./0����$����������%�#2��� #�!!*��& !��%�D2E!+�*./0%�D2E!

Copyright JCAHO 2001 9
� ����� �������������������������� ���� �� 2 � �!�� "����#
� +1,H+8D51>SE$.OKKI (person approach)� +1,H+8D51>SE$,-.. (System approach)
.OKKI +1,H+8D51>SE$,-..
- .+R,#$(1$=ELN= 5I$IC" >[C4#6S1 - "0OJ6(\1RI1&%&H"#6;N0#$K+1,K/.KO"R]LE+,," (A4"A+1,=)&+1,&A(A4@O&
- +^>+P_ ,->.A6. - >8IA460@E4$H/&I#".(.1(=;$N= I$`(J - ,-..$10

Copyright JCAHO 2001 10
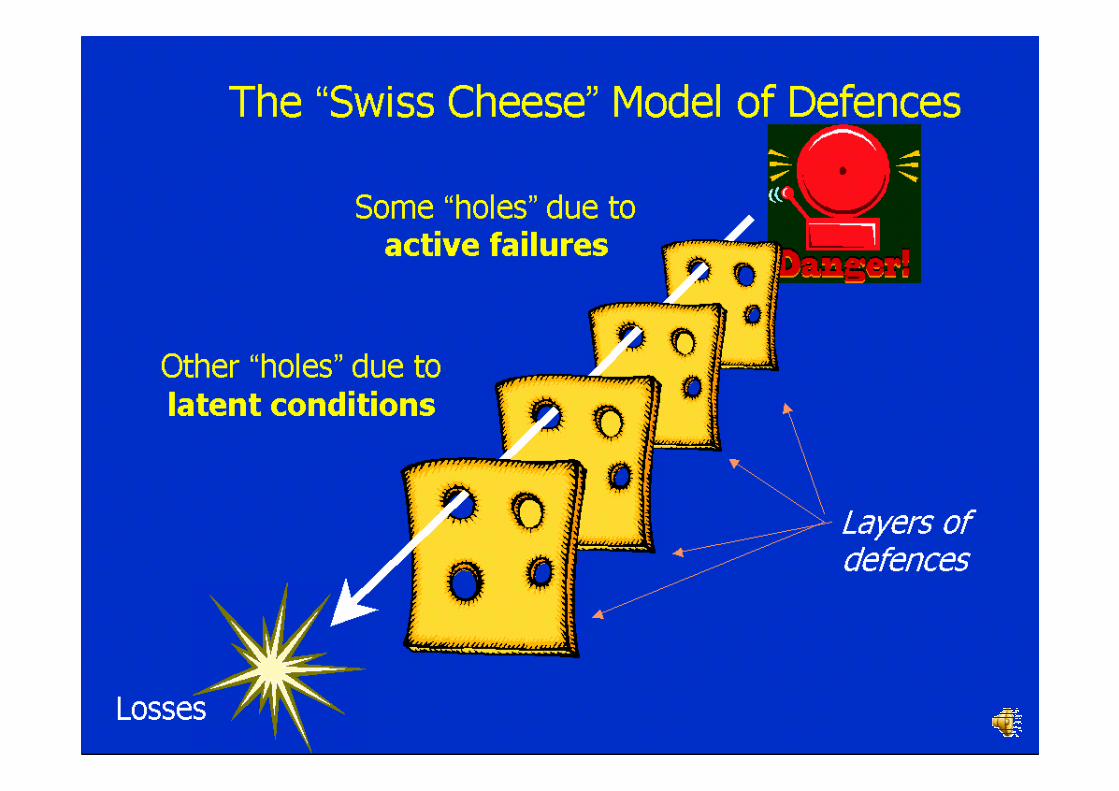
,��!(�:����AA���T %��"4�� 2 #44 �� K/1"I">5I/=,E$ (active failures) +1,+,-(\1%"8I#&B)6 `&6:;N5.,E+1,`&6L,$ >S0 K/1"RI)*$>:I#, :E&RI1& b0+^,->.A6.
� K/1"I">5I/Hb$ (latent failures) L#$/E>K,1-5 >+E&=1+,-..:E&RI1&F#$/EU/+, @7180E+ :;=)&,->.A6. F)*0L#08ME.)LE =073$:;.,E51, >S0 >/I1=\1+)& $10 #O8+,P%">RA6$R# K0>50C4#6 K0F1&8,-@.+1,P

Copyright JCAHO 2001 11
����� �* 1 4��'�':����%���'%�8*�����"?.&� �����(���# �.3. 2539 - 2543
182150967560��� (���)
138114676442����� �����������
393425915���� ������������������
42423������� !�"��
25432542254125402539#!��!��$�%��\ �'

Copyright JCAHO 2001 12
����� �� "�� ���������
N�����!� ��������K����"�

Copyright JCAHO 2001 13
��S ��T�T�����
����� ������%Q���L� ����� ���T�Q����"L��S

Copyright JCAHO 2001 14
�%��L�'�KQU T�Q�����" ��S L�V��� T� �Q�
�%�%' �W������ '�KQ��!���� � "���T�Q��X �� � 'I

Copyright JCAHO 2001 15
�Y! ���"ZQ���%�� %���� ��V� ��ZQ�����
Z!�T�Q�[M��%'�!��Z!�T�Q�[M��%'�!�� ��I�������"�� ���I�������"�� �
I�" near miss I�"�����X miss

Copyright JCAHO 2001 16
� Do Right Things� Do Them Well� Better Chance for Good Outcomes.
Accreditation Represents a Risk Reduction Strategy

Copyright JCAHO 2001 17
WHO WHO World Alliance World Alliance for Patient for Patient SafetySafetyto address the problem of to address the problem of
patient safety worldwidepatient safety worldwide

Copyright JCAHO 2001 18
� The problem of adverse events in health care is serious� 10% of hospital patients suffer an adverse event each year (UK, New Zealand, Canada and Europe)
� 16.6% of hospital patients suffer an adverse event (Australian study)
� 98,000 hospital deaths every year through medical error (USA)
� 1.4 million hospital patients worldwide acquire HAI (at any given time)
� UK: 100,000 cases of HAI lead to 5,000 deaths a year� USA: 1 out of every 135 hospital patients acquires HAI
Copyright JCAHO 2001 19
“Human beings make mistakes because the
systems, tasks and processes they work in
are poorly designed.”
Dr Lucian Leape, testifying to the US President’s Commissionon Consumer Protection and Quality in Health
Copyright JCAHO 2001 20
The Ubiquitous Patient Safety Challenge
• Denial and cover-up remains common• Systems awareness is limited and the capability to re-design systems to be safer is growing but still limited
• Health care is dynamic and ever changing with new drugs, technology and chronic diseases

Copyright JCAHO 2001 21
World Health Assembly Resolution 55.18• Develop global norms and guidance• Promote evidence-based policies• Encourage patient safety research• Share best practices• Promote cultures of safety in health care organizations

Copyright JCAHO 2001 22
Overview of the Alliance� The Alliance was set up to support countries improve their
safety of care� The Alliance:
� Generates awareness and commitment: political, clinical, patient
� Engages global and regional partners: private, public, NGO
� Develops and shares knowledge: guidelines, standards, research data, solutions, reporting & learning
� Provides technical expertise to countries� Mobilises resources to implement country projects

Copyright JCAHO 2001 23
World Alliance on Patient Safety Strands• Global Patient Safety Challenge• Patients for Patient Safety• International Patient Safety Events Taxonomy
• Reporting Systems• Research• Dissemination of Patient Safety Solutions

Copyright JCAHO 2001 24
First Global Patient Safety Challenge
Copyright JCAHO 2001 25
The Global Challenge: Clean Care is Safe Care
• Overarching strategy• Focus on hand hygiene• Comprehensive Guidelines on Hand Hygiene

Copyright JCAHO 2001 26
Patients

Copyright JCAHO 2001 27
Harvard Practice
Medical Study
1984
Utah Colorado
Study 1992
Australian Quality in Healthcare Study 1992
Adverse events in British Hospitals
1999-2001
Danish Adverse Event Study
2001
Adverse Events in New Zealand Study 2002
Canadian Adverse Event Study
2004
French Adverse Event Study
2004
The Commonwealth Fund Survey
2005
Research for Patient Safety

Copyright JCAHO 2001 28
Research• Project on measuring patient harm in data-poor environments
• Development of international patient safety research agenda
• Candidate studies• Funding issues

Copyright JCAHO 2001 29
Solutions for Patient Safety

30
Errors and adverse events can result from a variety of issues atErrors and adverse events can result from a variety of issues at different levels different levels
within health carewithin health care——for example, at the level of government support (e.g. funding), for example, at the level of government support (e.g. funding),
the level of a healththe level of a health--care facility or system (e.g. structure or processes), or at thecare facility or system (e.g. structure or processes), or at the
point of intervention between patients and practitioners (e.g. hpoint of intervention between patients and practitioners (e.g. human error). The uman error). The
Solutions from this initiative will not address the broad underlSolutions from this initiative will not address the broad underlying causes of ying causes of
patient safety problems (e.g. inadequate resources), but rather patient safety problems (e.g. inadequate resources), but rather will be directed at will be directed at
the specific level where good process design can prevent (potentthe specific level where good process design can prevent (potential) human ial) human
errors from actually reaching the patient. Solutions, therefore,errors from actually reaching the patient. Solutions, therefore, will be intended to will be intended to
promote an environment and support systems that minimize the rispromote an environment and support systems that minimize the risk of harm k of harm despite the complexity and lack of standardization in modern headespite the complexity and lack of standardization in modern health care.lth care.

Copyright JCAHO 2001 31
Confusing drug namesConfusing drug names is one of the most common causes of is one of the most common causes of
medication errors and is a worldwide concern. With tens of medication errors and is a worldwide concern. With tens of
thousands of drugs currently on the market, the potential for erthousands of drugs currently on the market, the potential for error ror
created by confusing brand or generic drug names and created by confusing brand or generic drug names and
packagingpackaging is significant. The recommendations focus on using is significant. The recommendations focus on using
protocols to reduce risks and ensuring prescription legibility oprotocols to reduce risks and ensuring prescription legibility or the r the use of preprinted orders or electronic prescribing.use of preprinted orders or electronic prescribing.

Copyright JCAHO 2001 32
The widespread and continuing failures to correctly identify patThe widespread and continuing failures to correctly identify patients ients
often leads to medication, transfusion and testing errors; wrongoften leads to medication, transfusion and testing errors; wrong person person
procedures; and the discharge of infants to the wrong families. procedures; and the discharge of infants to the wrong families. The The
recommendations place emphasis on methods for verifying patient recommendations place emphasis on methods for verifying patient
identity, including patient involvement in this process; standaridentity, including patient involvement in this process; standardization of dization of
identification methods across hospitals in a health care system;identification methods across hospitals in a health care system; and and
patient participation in this confirmation; and use of protocolspatient participation in this confirmation; and use of protocols for for distinguishing the identity of patients with the same name.distinguishing the identity of patients with the same name.

Copyright JCAHO 2001 33
Gaps in handGaps in hand--over (or handover (or hand--off) communication between patient care off) communication between patient care
units, and between and among care teams, can cause serious units, and between and among care teams, can cause serious
breakdowns in the continuity of care, inappropriate treatment, abreakdowns in the continuity of care, inappropriate treatment, and nd
potential harm for the patient. The recommendations for improvipotential harm for the patient. The recommendations for improving ng
patient handpatient hand--oversovers include using protocols for communicating critical include using protocols for communicating critical
information; providing opportunities for practitioners to ask aninformation; providing opportunities for practitioners to ask and resolve d resolve
questions during the handquestions during the hand--over; and involving patients and families in the over; and involving patients and families in the handhand--over process. over process.

Copyright JCAHO 2001 34
Considered totally preventable, cases of wrong procedure or wrong site surgery are largely the result of miscommunication and unavailable, or
incorrect, information. A major contributing factor to these types of errors is the lack of a standardized preoperative process. The
recommendations to prevent these types of errors rely on the conduct of a preoperative verification process; marking of the operative site by the practitioner who will do the procedure; and having the team involved in
the procedure take a “time out” immediately before starting the procedure to confirm patient identity, procedure, and operative site.

Copyright JCAHO 2001 35
While all drugs, biologics, vaccines and contrast media have a While all drugs, biologics, vaccines and contrast media have a
defined risk profile, concentrated electrolyte solutions that ardefined risk profile, concentrated electrolyte solutions that are used e used
for injection are especially dangerous. The recommendations for injection are especially dangerous. The recommendations
address standardization of the dosing, units of measure and address standardization of the dosing, units of measure and
terminology; and prevention of mixterminology; and prevention of mix--ups of specific concentrated ups of specific concentrated electrolyte solutions. electrolyte solutions.

Copyright JCAHO 2001 36
Medication errors occur most commonly at transitions. MedicatioMedication errors occur most commonly at transitions. Medication n
reconciliation is a process designed to prevent medication errorreconciliation is a process designed to prevent medication errors at patient s at patient
transition points.transition points. The recommendations address creation of the most The recommendations address creation of the most
complete and accurate list of all medications the patient is curcomplete and accurate list of all medications the patient is currently takingrently taking——also called the also called the ““homehome”” medication listmedication list;; comparison of the list against the comparison of the list against the
admission, transfer and/or discharge orders when writing medicatadmission, transfer and/or discharge orders when writing medication ordersion orders;;
and communication of the list to the next provider of care wheneand communication of the list to the next provider of care whenever the ver the patient is transferred or discharged.patient is transferred or discharged.

Copyright JCAHO 2001 37
The design of tubing, catheters, and syringes currently in use iThe design of tubing, catheters, and syringes currently in use is s
such that it is possible to inadvertently cause patient harm thrsuch that it is possible to inadvertently cause patient harm through ough
connecting the wrong syringes and tubing and then delivering connecting the wrong syringes and tubing and then delivering
medication or fluids through an unintended wrong route.medication or fluids through an unintended wrong route. The The
recommendations address the need for meticulous attention to recommendations address the need for meticulous attention to
detail when administering medications and feedings (i.e., the ridetail when administering medications and feedings (i.e., the right ght
route of administration), and when connecting devices to patientroute of administration), and when connecting devices to patients s (i.e., using the right connection/tubing).(i.e., using the right connection/tubing).
Copyright JCAHO 2001 38
One of the biggest global concerns is the spread of Human Immunodeficiency Virus (HIV), the Hepatitis B Virus (HBV), and the
Hepatitis C Virus (HCV) because of the reuse of injection needles. The recommendations address the need for prohibitions on
the reuse of needles at health care facilities; periodic training of practitioners and other health care workers regarding infection control principles; education of patients and families regarding transmission of
blood borne pathogens; and safe needle disposal practices.

Copyright JCAHO 2001 39
One of the biggest global concerns is the spread of Human Immunodeficiency Virus (HIV), the Hepatitis B Virus (HBV), and the
Hepatitis C Virus (HCV) because of the reuse of injection needles. The recommendations address the need for prohibitions on
the reuse of needles at health care facilities; periodic training of practitioners and other health care workers regarding infection control principles; education of patients and families regarding transmission of
blood borne pathogens; and safe needle disposal practices.
Copyright JCAHO 2001 40
Solutions in Development
1. Preventing Patient Falls2. Preventing Pressure Ulcers3. Look-Alike Packaging and Labeling of
Medications4. Response to the Deteriorating Patient5. Communicating Critical Test Results6. Healthcare-Associated Infections:
Central Lines7. Apology and Disclosure8. Patient and Family Involvement

Copyright JCAHO 2001 41
������������������� ���
Risk Identification Risk assessment
Risk TreatmentRisk evaluation
Wilson + Tingle 1999

Copyright JCAHO 2001 42
� �������� ��-+,�#�!�����%-�����!���-!!����-./������0�& ���� �
���������� �� ���������� ��-������ ��-�/�����-1"��*��-��"����-������(2������!"�����)�)�
�����'�����
������������������ ���������������������� ����
��������������������������������� RM:05

Copyright JCAHO 2001 43
Copyright JCAHO 2001 44

Copyright JCAHO 2001 45
������4������5���#��� Jo. Wilson,1999, P 31.
������Screening
��=>�� Assessing
����� Planning
�5�� Caring
��=>�� ��Evaluation
�5��F��/��H�Patient
Nursing* Medical Paramedical
Support*Services
Hotel*Services
Management*Services
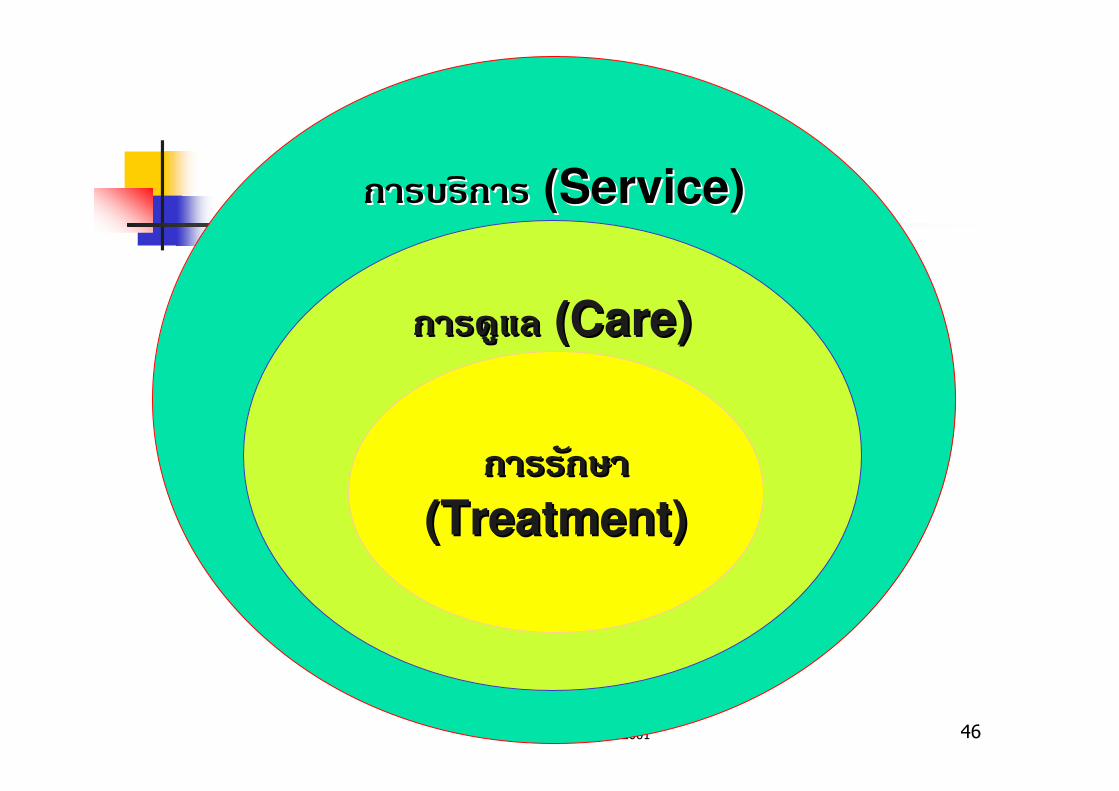
Copyright JCAHO 2001 46
������������������ ( (Service)Service)
����(������(�� ( (Care)Care)
������#�������#�
(Treatment)(Treatment)

Copyright JCAHO 2001 47
RMRMQAQA
CQICQI
Average ExcellenceBorderline
QUALITY OF CARE
ZONE OF QUALITY MANAGEMENT
# O
F H
OS
PIT
AL
SThe Total Quality Spectrum
lkdgf
�������&��������0��) �� %"��� ������������&��������0��) �� %"��� �����
��������������������������������� QualityProcess:01

Copyright JCAHO 2001 48
Customer
Driven

Copyright JCAHO 2001 49
• ����� ����� *������ !���������
- ������!9�/������
- �%�� ��
- ���%���
- ���0"��"���
- ��� Expose
• �����&������� ��
- ������ ����; ���� !�%��22��
����� �������0�

Copyright JCAHO 2001 50
������������� ���������������� ��� � ������� ������ �����������������������������������
�� !�"� FMEA �'�(���)�����*+����),���������"�������� !+"��
!���� ����-��������� �� ������������. -���*+����),���*�"������/�� *�/����0����������--��'�(* ��������1��23��
� ����'� Clinical CQI
� ������0 � RCA �/�����������*,*����*+���� �'���/������
�*+����),������!�� *�/�����0"������� �2/����0�����00!3����0��������=�2��0�3 ������1. ���������� ��
Copyright JCAHO 2001 51
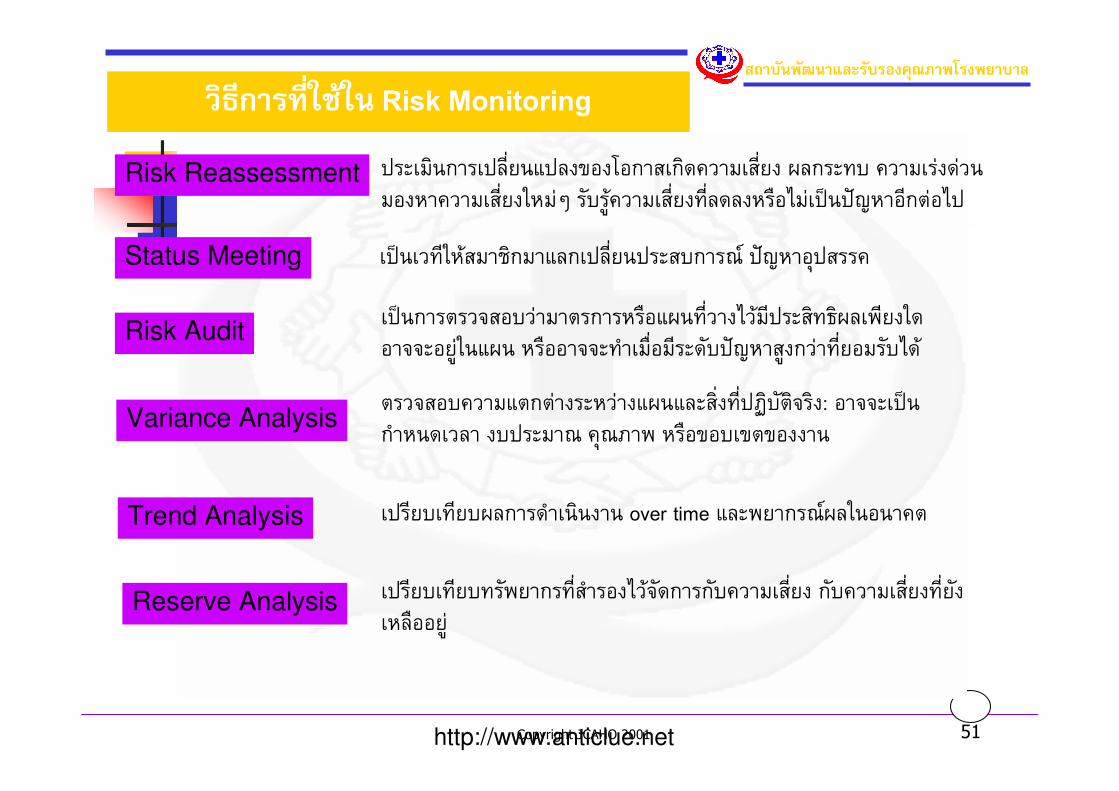
���������������� ���������������
��������������� Risk Monitoring
Risk Reassessment �����������#%��&���'(��(����������#%�� )����$* ���������� �(�������#%������+ ��*�,�����#%��$#%������-(.���/��01��(#���(.�
Status Meeting �/��$#�����������&����#%������*���2 �01��(�����
Risk Audit�/�������3�(*������������-(&)�$#%���.���#�����$"�)�4#����(�33�(�,���&)� ��-((�33�$���-%(�#����*�01���,�����$#%�(���*.��
Variance Analysis
Trend Analysis
���3�(*���&�������������&)�&����%�$#%�5�*���3���: (�33��/���������� �*�����2 �27�4 ��-('(*'�'(����
��#�*$#�*)������������� over time &��4����2 )���(���
Reserve Analysis ��#�*$#�*$��4����$#%����(�.��3�������*����#%�� ��*����#%��$#%�����-((�,�
http://www.anticlue.net

Copyright JCAHO 2001 52
���������������� ���������������Areas of Risk / Patient Safety
to be Monitored
General
Adverse Events
Mortality: Risk Adjusted, Standardized, Case Specific Fatality
SpecificHospital Associated Infection
Surgery & Anesthesia
Medication & Transfusion
By Services: ER, ICU, Maternal & Neonatal
High Risk Patients & Procedures
Environment & Equipment
Patient’s right, Ethic

Copyright JCAHO 2001 53
���������������� ���������������
Adverse Event & Error
Error (��� !�"��#�) �%�&��������������� &����%�&'(��������') ����*"�Adverse Event (&+,�����-���* %�.�'�����-) �%�&���������� ��,���
���&��"/.#����!0�'1�� &'(���� �%�&������!���-
ErrorAdverse
Event

Copyright JCAHO 2001 54
����� ����<�=����"�����������
1. P#�>P������>����4�#���������Q�>�R � ��!�S���!��� 2. ��=H�� ���>������PTS�P��!�S>�U�>���=��#�� ��� �� !����
��=�5��F��>�TS������ H�=� �H#���������Q�3. >P������V���������W�V#� ��=��!��������>P�S��
>�TS���������Q�4. 4�P��!������>�TS���������Q�5. ��������5�V������> � ��������Q�
Pronovost 2004 P. 59 - 68

Copyright JCAHO 2001 55
RM QA CQI is Power� �709"$����"��%'�'����'(����$%-�*��+, / 9$+,
� :0� �*�70 ����'+,$���s�'� +, / 9$+,
� +'��� ����' �70�����$#� A#�7���'%-$�� +, / 9$+,
� �70%(F'���$%#'9#9"+'���.�#t(� .&�����(���B����"�T+'����B�A��+(�'�8*'%:�+4��$$8�'��$���s�'$�+,� +, / 9$+,

Copyright JCAHO 2001 56
71K\1L#.F#$KOPKC# NS
�����A:���709".-"� +(%(F'�� �709"'��%��(& ����A������:��QA RM CQI$�+,.�#t(�+',����#��4��� '%���A���.&�

Copyright JCAHO 2001 57
RCA ANALYSIS
To get results, should we focus our behavior on the Y or X ?
“���������� X �� ���������������� Y ?”3.Analyze
4.Improve
���� Y
���� Dependent
���� Output
���� Effect
���� Symptom
���� Monitor
Y=1.Define
2.Measure
(�������)
f (X)
���� X1....Xn
���� Independent
���� Input-Process
���� Cause
���� Problem
���� Control
�������
(����)5.Control

Copyright JCAHO 2001 58
0
5
10
15
�.�. �.�. ��.�. ��.�. �.�. �.� �.�. .�. �.�. �.�. �.�. �.�.
VAP
0
50
100
�.�. �.�. ��.�. ��.�. �.�. �.� �.�. .�. �.�. �.�. �.�. �.�.
CQI
P Systemic Link Chart (Moor)Y = f( x1 +x2 +x3……xn)
������/��������*�"��RM/CQI/QA
X=CQIx13 ���/�x2�.����*�x33 �����
CY=VAP
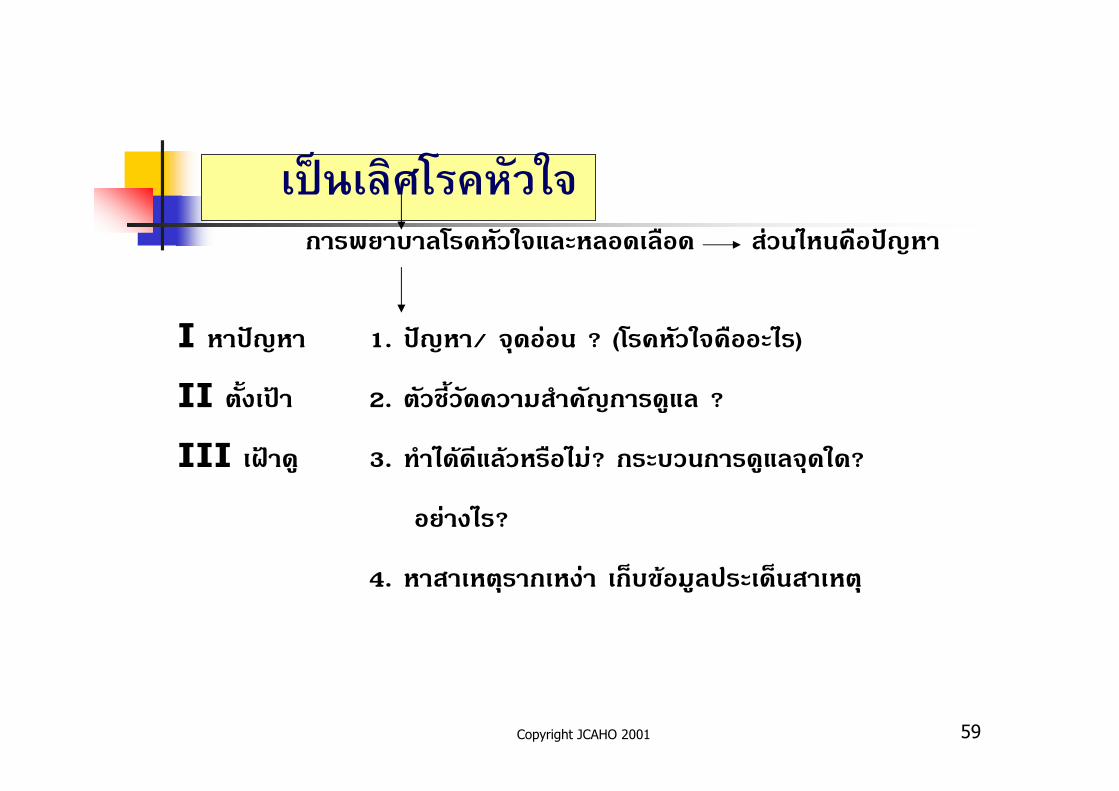
Copyright JCAHO 2001 59
$�(�$��)*��+��,-���������*������!����������� �"��0������-2��
I ���-2�� 1. �-2��/ !���"�� ? (*������!�����0�)
II %�$��/� 2. %��)�$�����������2����(�� ?
III ./��( 3. ���0� ���� �����0"? ����������(��!����?
��"��0�?
4. �����%������"� �9�& �(�����9����%�

Copyright JCAHO 2001 60
$�(�$��)*��+��,- (���)IV ������� �� 5. ��"���� )"������� 0&�-2�� ������
�G#H�/ ��!�� 3 �� ��
6. �������������� 0& (����)
Y=f(X1 X2 X3……XN)
7. ������K���%�
8. ���'������� 0&
9. ���������'����=;
10. &���'�*���������O��("���K���%��%�P��

Copyright JCAHO 2001 61
.'���"Root Cause Analysis (RCA)%#'����'(�#44 � �*%#'���:��#t(� (�8�-�%(�7�8>'s�':�����$.#�#��'+'���#H�A ����' ��$9#;<�-�%(�7:�����%��"�7A �����0 (�8�%(�7���0 �*9$�<�#��-�� �*�7'.��

62
Complying with the FMEA Requirements of the New Patient Safety Standards
Darryl S. Rich, Pharm.D., M.B.A., FASHP
Associate Director, Surveyor Development and ManagementJoint Commission

Copyright JCAHO 2001 63
New Patient Safety Standards
� It’s a leadership thing!� Manage variation in performance� Integrated patient safety program implemented
� Ongoing proactive program to identify risks to patient safety and reducing errors
� Patient safety is a high priority

Copyright JCAHO 2001 64
LD.5.2
� Leaders ensure that an ongoing, proactive program for identifying risks to patient safety and reducing medical/health care errors is defined and implemented.

Copyright JCAHO 2001 65
Requirements of LD.5.2
� At least annually, select at least one high-risk process for proactive risk assessment � such selection to be based, in part, on information published periodically by the Joint Commission that identifies the most frequently occurring types of sentinel events and patient safety risk factors

Copyright JCAHO 2001 66
High Risk Processes� PI.4.2 – Processes that involve risks or may result in sentinel events� Medication Use� Operative and other procedures� Use of blood and blood components� Restraint use� Seclusion, when a part of care� Care/services provided to high-risk populations� Resuscitation

Copyright JCAHO 2001 67
The Medication Use Process
Selection, Procurement, and Storage
Prescribing or Ordering, and Transcribing
Preparing and Dispensing
AdministrationMonitoring

Copyright JCAHO 2001 68
Requirements of LD.5.2
� Conduct a Failure Mode and Effects Analysis (FMEA)� Assess the intended and actual implementation of the process to identify the steps in the process where there is, or may be, undesirable variation (i.e., what engineers call potential "failure modes")

Copyright JCAHO 2001 69
RCA RCA RCA RCA ���� is a is a is a is a process,usually process,usually process,usually process,usually
reactive ,for identifying thereactive ,for identifying thereactive ,for identifying thereactive ,for identifying the
basic or causal factors that basic or causal factors that basic or causal factors that basic or causal factors that
underline variation in underline variation in underline variation in underline variation in
performance and which performance and which performance and which performance and which
can produce unexpected can produce unexpected can produce unexpected can produce unexpected
and and and and undesired adverse undesired adverse undesired adverse undesired adverse outcomes.outcomes.outcomes.outcomes.

70
Failure Mode and Effect Analysis

Copyright JCAHO 2001 71
Failure Mode and Effect Analysis
� ����������;���� �������& �����"�� ���'�������� !����&,$� Q, ��O���� ������ !�)"���������������"���O����� ��������� )�$�"� ������!�����%�&��& �����"���� ����*� �"�!����&,$�

Copyright JCAHO 2001 72
Failure :
���� ��� & �����"��&������ ������������������ ������������� ������� !������������ �O�0�%�& �������*��& ���������$�O�'��!������������; ��������'����!���O� ���% ����� �������������&���(�� �
Failure Mode: ����=����)��������
���#��&��& �����"���� ���&,$�(Failure))"����� �%� *�"� ��&���*%���0� ���� '�� ��& ���0�
����=����)�����������
���#��& �����"���� ���!����������� )"����%�����'������ ���!"����'������
Effect:'�&��& �����"���� �%"� ���� ���������1��0� ������ �� ��& �� '��%���R;���������� �(�� ������� ����(�� ������

Copyright JCAHO 2001 73
!���"����&��FMEA
� �����1,����*� &��& �����"���� ��!���&,$� ������%�&��& �����"����$�S
� �"�)�$1,������ 0&������� !����!��������*������������& �����"��
� �O�����������!��� �������<��'��%���R; ��������������"���O�����

Copyright JCAHO 2001 74
���������%;�) FMEA
� � ������� ������" '��%���R;��" ��������"��������������� ������0� ������������
� � �������� ������ ��������� '��%���R; ����������� � �'��%���R;�������������0� 1(����0��) ����� ����� �������=������ ��� �%�%"��!����%�
� ����!������� 0&�-2����9!��$� ����) �� ��/�����0"�� �-2�������"�����&,$����
� � �% ������������%�����/����������������������� �����("���-!!����
Copyright JCAHO 2001 75
��������� FMEA�� �������=����
� �O�������������& �������(Multi-disciplinary Teams)
� ��)��5-9 �� %������� �!���%"����"�����% ���O�'( ����������;%����#������� !��������������; �������1)�2��������;��& ��"��O���)��)� �����0�
� ���%1�������;����/������ )��!�
� ��)������ �����"��� ����) ���&���� �������� ������;

Copyright JCAHO 2001 76
FMEA Process Sequence
RPN
Detect
Occur
Sev
Actions Taken
12
Action Results 13Responsibility&Target Completion Date
11
Recommended Action(s)
10
RPN
9
Detec
8
Current Controls
7
Occur
6
Potential Cause(s) of Failure
5
Sev
4
Potential Effect(s) of Failure
3
Potential Failure Mode
2
Activity
1

Copyright JCAHO 2001 77
FMEA Basic Steps
1. ����1,��������������&�$�%���� % �����+,�#�(Flow chart)2. ����& �����"���� ��!!����&,$�(Potential Failure Mode)3. ����'�������� ��!!����&,$�(Potential Effects of
Failure)4. & �����"�������"���'������%"��� ��� ���������������������"
0��(Severity)5. ��0��O����%��� �O�0�0� �� ����� ���& �����"�� (Potential
Causes)6. *������������& �����"������ ������0�(Occurrence)7. ��=������ �) ����������& �����"�����-!!����(Current
Controls)8. �������1��������������%��!!��& �����"��(Detection)

Copyright JCAHO 2001 78
FMEA Basic Steps
9. ��������������� ���� ��!!����&,$�(Risk Priority Number)
10. ������������������/������� ���*���������������%��� !������
���& �����"�� ������������������=��������������(Recommended Actions)
11. ������'( ���'��)�� �������� ��������9! (Responsibility &Target Completion Date)
12. ��!����� 0� ����������� �(Actions Taken)
13. ���������� ������!�����������

Copyright JCAHO 2001 79
���%��� �O�0�0� �� !������ ���& �����"�������������
� 0"��������%��� )"��/�� T���� 0"�K���%�%����������K���%����
� 0"����������K���%����
� &�����#��� !���O��� ��!��0"0� ������.U����
� 0"����%��!���
� ���������K���%����'������
� �������� ��������������-2�� )"� ����� �������� ���0"�� ����������0�V�V
� &�$�%����"���� Q��Q �� ��������� ���������� ��� �

Copyright JCAHO 2001 80
���%��� �O�0�0� �� !������ ���& �����"�������������
� &����������� ���������� ����� ����'������� 0"�����,�����K���%����
� �-2���� �����&,$� 0"0� �������� 0&� ������;��-2�� )"�0"�� ��%�� �����("�������� �) ���0"0� V�V� �) ��� ����'�������
� 0"��������� ��� ������'��)�� ��������!�� )��!�� �*����0")��!�� V�V
Copyright JCAHO 2001 81
'�������� ��!!����!��& �����"��
� ����������� �������(�� ��� & ����������
� �-2���� �"�'�������������1��0� ��������������� �� ��& ��� ����������� ��������� ����������;%"��S
� �������������� �)���R;V�V

Copyright JCAHO 2001 82
��R;���������&��'������
� ����� A �%�����;Q, ��*������ !��"��� ������������� ��
� ����� B ������������� ��&,$� �%"���0"1,�'( �W��
� ����� C ������������� �����'( �W�� �%"0"����� '( �W��0� ������%���
� ����� D ������������� �����'( �W�� �"�'��� % ������./�������� ��� � ��!�"�0"������%���%"�'( �W��

Copyright JCAHO 2001 83
��R;���������&��'������
� ����� E ������������� �����'( �W���"�'��� ������%���)� ����� ���% ���������������#�
� ����� F ������������� �����'( �W���"�'��� ������%���)� ����� ���% �����*�������� ������("*�����������&,$�
� ����� G ������������� �����'( �W���"�'��� ������%���1�����"'( �W��
����� H ������������� �����'( �W���"�'��� % ��������)"��)���%

Copyright JCAHO 2001 84
FMEA is
� a team-base, systematic and proactive approach
� process or design can fail,why it might fail
� how it can be made safer.

Copyright JCAHO 2001 85
� Purpose FMEA for
JCAHO identify where
and when possible
system failures could occur
� To prevent those
problems before they happen

Copyright JCAHO 2001 86
FMEA *����������+&�� NASA ��)"���+���#�� 1950 0� ����&���0������%������ * � � � � �X � + .1972 � ��" � K� �� %� � � � North
American Automotive Operations &�����#�� Ford Motor !����$�0� ������'����"������0�������%;�) ��"������9� �����������+0��0� �� ����������%;�) FMEA ������"��%������
���X �+. 2002 0� �� �������������������� ��%�������&�� FMEA 0��) ���=����!���������
Copyright JCAHO 2001 87
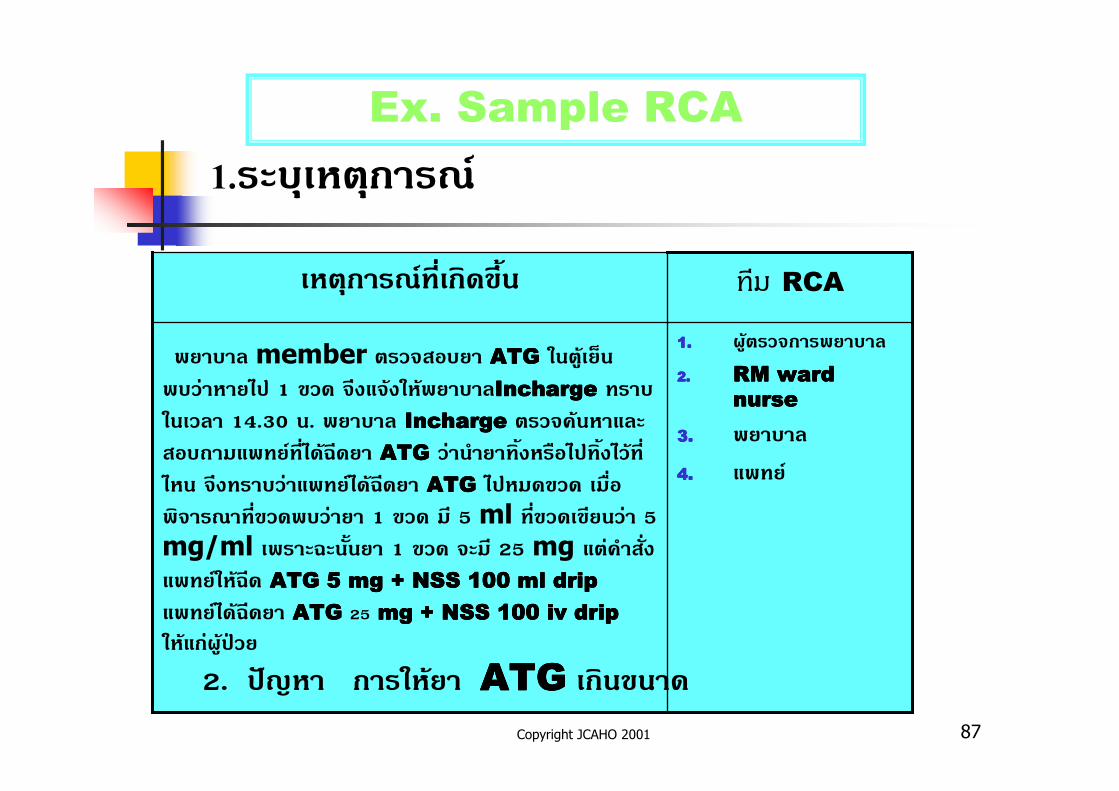
Ex. Sample RCA
1.�����%�����;
1.1.1.1. '( %��!���������
2.2.2.2. RM ward RM ward RM ward RM ward
nursenursenursenurse
3.3.3.3. ������
4.4.4.4. ����;
������ member %��!����� ATGATGATGATG ��%( �9����"����0� 1 &�� !,��! ��� ������InchargeInchargeInchargeIncharge ���� ����� 14.30 �. ������ InchargeInchargeInchargeIncharge %��!� ���������1�����;�� 0� T���� ATGATGATGATG �"��������$�����0���$�0� �� 0�� !,������"�����;0� T���� ATGATGATGATG 0���&�� � ���!������ &�����"��� 1 &�� � 5 ml �� &��&����"� 5mg/ml ����T���$��� 1 &�� !�� 25 mg �%"����� �����;�� T�� ATG 5ATG 5ATG 5ATG 5 mg + NSS 100 ml dripmg + NSS 100 ml dripmg + NSS 100 ml dripmg + NSS 100 ml drip ����;0� T���� ATG ATG ATG ATG 25 mg + NSS 100 iv dripmg + NSS 100 iv dripmg + NSS 100 iv dripmg + NSS 100 iv drip �� ��"'( �W��
��� RCA�%�����;�� ���&,$�
2. �-2�� ����� �� ATGATGATGATG ���&���

Copyright JCAHO 2001 88
4.������ Failure Mode
---- ---- -%��!���& �(��"�����%�����
����� MAR
----Q��1�������& ��!
----���%���������� MAR
----
���� Mode �� �'�%"��-2�� (Potential effect) 1 �� Y !�������
Y2 9$9"%����$��� A+A MAR
Y1 :�"������4-�A:�$?&���$;?������'���%����$��
I\1&).,/"1x2x3321Potential effect

Copyright JCAHO 2001 89
7. �����������'����=+��%�;(Analysis and Action planning for Critical Failure Mode
$����%����$�� �*;?���� ;?�:'�"
31/1/487/1/480.@.=)01.4 "+(( �('�%�����4-�A:'�"�� ATG ��$� A.� � 7��� >���'���%����$��
1.+1,L,/=@#.K/1"7;+L#$+#0+1,>L,A6"61
6& �*%��":<>'����%�&�%��*$�' -�>'-7"
6?� A6�",�A
��4���$
Critical Failure
Mode

Copyright JCAHO 2001 90
���#��� '�& "��(�&$+'6?-?����7
����������
%��!�"��������������������������%��!�� ���������% �����
����,�
�(��)"������
�� ������
�����'�
��V^�� /^5�H��� ��V^�� / ����Q� ��V^��
�����'����=;%��!�)������
%������!�����0 ��$�%���
�� & �(�'( �W��/2�%�!������'����%���
Copyright JCAHO 2001 91
��0� �* 1 � 6?#��,��9 ����7 30 # ��6�� "��$($��9� .� �- *���#H�,��'� ���A�&9#y�"��+(%�&� 10.00 '. %�&� 10.30 '. ( �+4%�', �&� 4'(�7"%�' %��8*�� alarm monitor #"9�
Copyright JCAHO 2001 92
��0� �* 2� 6?#��,�����7 72 # ��6�� "Tonsillectomy ' *���? �*�8>'%�&�02.00 '. ���"?�'�>�.&� Xygoma .��
� 6?#��,�����7 80 # $������- A-' &8*'&$+'(��'>�� 3����.��

93
-�7#.'� ����� �� RCA
1. %��"%�8*���7'.��, }>��A��T2. � >� �$ 6?%��*��:����$Flow3. ��A7#��%"F'#t(�4. ��%����(���A�'��� �*%��*��:��5. (�47"!(�/���������%��"#t(�6. (�-�%(�7:��#t(�+(;<����7. ���('"�7 B3�-�����.�9:8. ��"��$6&9. ���('"%#'.'� ��#H�A ��('� ����$+($)

Copyright JCAHO 2001 94
Flow �������������
������������ ���� ER
���������� �����������
����� �� �������� ��!
!� ��
����� �� NICU
Failure Mode
-�!������� ��"�
Failure Mode
-IC �!���� �� �����
-�#$��� �!�%��&�
Failure Mode
-��������!���� ��%��!��
-�!� ID �� �
Failure Mode
-NICU�!���� ��%��!��
-�!�� '�!���!� ��!&��� ������ #$��!#��!�� ��!&(�

Copyright JCAHO 2001 95
��)�g��=�
�)���3/���� ��1. h��*i������ 30 j +������k,! �
�2g��� �������k, 8 ��/�� l���m.����0����)�*3" -��
���2��0�3 � ����2��0�3 � �� ������0�+��*+��m
2��0�3����0�m��+,�"��+�� 1. ��0����m�"��+���� ��������
!3���i!-�m����m2��0�3�� �)������-�����(�
��3� 1 5 ���� �'�(* 1. h��!3������� m��!�"����

Copyright JCAHO 2001 96
ni*�
1. h��m��!�"�����)���3/���� �� (refer)

Copyright JCAHO 2001 97
Step 1
� Construct a Detailed Flow Chart of the Process� Multi-disciplinary participation of all those involved in the process
� Allocate plenty of time for this step� Be as detailed and complete as possible� Learn the flow chart process and symbols
� Flow charting software can help

Copyright JCAHO 2001 98
Step 2
� Determine each step that can “fail” and how it can “fail”
PhysicianWrites Order
MedicationOrder
Order PulledFrom Chart
Order TranscribedBy Unit Clerk into
MAR
Order TranscribedBy Pharm Tech
Into Pharmacy System
NCR copy oforder sent topharmacy
Writing illegibleOrder incompleteNon-formulary drugUsed felt penConfusion abbrev. usedLook-alike drug orderedContrary to approved clinical protocol
Order not pulled inTimely manner
Transcription error

Copyright JCAHO 2001 99
-���'����0��������������� ��
�+���� ��3/���� �� ��0�+��*+�
1. ����2� ������m *1. ������1. h�� ����), *1.��������0�+��*+�
��������3/���� ��
*2.����2� �����2��� 2. ��3/���� �������m2��0�3 *2.�.!31. h��
�����0�m
3. ����2� ��1. h�� *3. �/������ ��.3 *3. !� ni*���0�+��*+�
*4.�+��������),
A B C

Copyright JCAHO 2001 100
���*���
��0m ��/m.�+ �� m.�+ ��/3��k�� m.�+ ��/�����3�
Failure 2 1 1
Mode 4 3 2
3
A B C

Copyright JCAHO 2001 101
Requirements of LD.5.2
� For each identified "failure mode" identify the possible effects on patients (what engineers call the "effect"), and how serious the possible effect on the patient could be (what engineers call the "criticality" of the effect)
Copyright JCAHO 2001 102
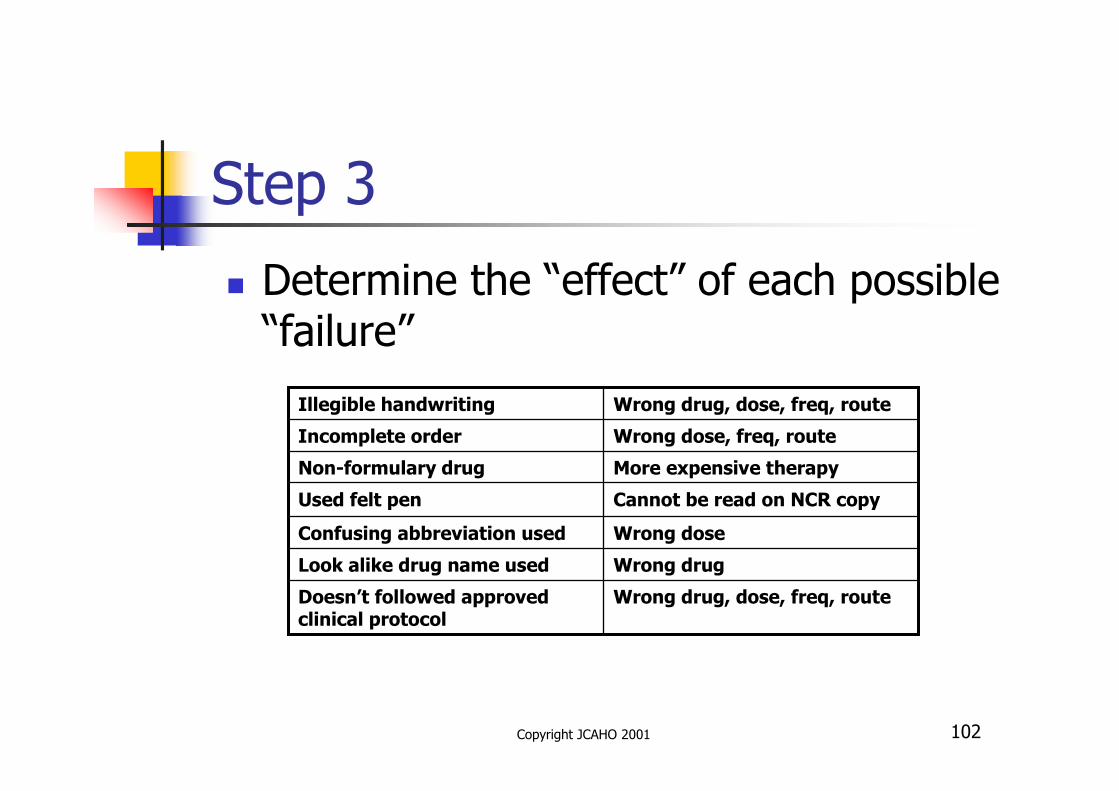
Step 3
� Determine the “effect” of each possible “failure”
Wrong drug, dose, freq, routeDoesn’t followed approved clinical protocol
Wrong drugLook alike drug name used
Wrong doseConfusing abbreviation used
Cannot be read on NCR copyUsed felt pen
More expensive therapyNon-formulary drug
Wrong dose, freq, routeIncomplete order
Wrong drug, dose, freq, routeIllegible handwriting
Copyright JCAHO 2001 103
Step 4� Determining how serious the possible effect(s) can have on the patient – criticality
� For each effect:� Estimate likelihood of failure (occurrence scale rank)� Estimate severity of failure (severity scale rank)� Estimate probability that failure is detected
(detection scale rank)
� Then compute criticality index � is product of above three or CI=OSR x SSR x DSR

Copyright JCAHO 2001 104
A�+����
1. ����2� ������m*2. ����2� �����2��������0�m3. ����2� ��1. h�� *4. �+��������),
���*��� ��0m ��/m.�+ ��
Failure mode 24
A

Copyright JCAHO 2001 105
Occurrence ScaleLikelihood Probability
� Remote (1) 1 in 10,000� No known occurrence
� Low (2, 3, 4) 1 in 5,000� Possible, but no known data
� Moderate (5, 6) 1 in 200� Documented but infrequent
� High (7, 8) 1 in 100 � Documented and frequent
� Very High (9, 10) 1 in 20 � Documented, Almost certain

Copyright JCAHO 2001 106
Severity ScaleOutcome possibilities
� Slight annoyance (1)� May affect the system
� Moderate System Problem (2, 3)� May affect the patient
� Major System Problem (4, 5)� May affect the patient
� Minor Injury (6)� Major Injury (7)� Terminal Injury or Death (8, 9)

Copyright JCAHO 2001 107
Detection ScaleLikelihood Probability
� Very High (1) 9 out of 10� Error always detected
� High (2, 3) 7 out of 10� Error likely to be detected
� Moderate (4, 5, 6) 5 out of 10� Moderate likelihood of detection
� Low (7, 8) 2 out of 10 � Low likelihood of detection
� Remote (9) 0 out of 10 � Detection not possible at any point

Copyright JCAHO 2001 108
Risk Priority Number: RPN
Severity = K/1",O0H,$ 0–10Occurrence = `#+1@>+E& 0-10Detection = K/1"@1"1,7N0+1,L,/==). 0-10
RPN = S x O x D= 7 x 3 x 5 = 105

Copyright JCAHO 2001 109
Step 4 (con’t)
� Rank prioritize the failure modes based on their criticality index.

Copyright JCAHO 2001 110
FMEA / RCA
5 >��.P���S2. �a�� ��5��V���W�V
2705-H��4>��S��P�V^������H������
6������H��4>��S�������P�Sa�>P��
9- ��Q��=�!��d��
1 >��.�������1. �a�� ��VV
- e����>fg��=��
- �VV>��S��
-��=>��
1473-H��4P�V���"���V��
7��������=>�� �=VV��!�S�5��F��"���V
7- ���H�"���#��
��=>�� �����"�#��V^��
�����=>�� �����
� !�S�h�VH�
�5������W�V
� �!�����"�RPND
E
T
�����V�����H�
OCC
Potential
Cause (S) of
Failure
S
EV
Potential
Effect(s)of
Failure
Potential
Failure
Mode
��4����
��������� ����/���������%� '( ���'��)�� FMEA No. _______Core Team Date !��%���*�� _________________
����� �� ___________________ ����� ����� __________________
Copyright JCAHO 2001 111
Example: Top 5 criticality-indexed failure modes*
� Having lethal drugs available on floor stock� Mistakes in math when calculating doses� Doses or flow rates for IV’s calculated incorrectly
� Not checking armbands before administration� Excessive drugs on nursing floor stock
*From: E. Williams and R. Talley “The Use of Failure Mode
Effects and Criticality Analysis in a Medication Error
Subcommittee” Hospital Pharmacy 1994 (Apr); 29(4): 331-338
Copyright JCAHO 2001 112
Requirements of LD.5.2
� For the most critical effects, conduct a root cause analysis to determine why the variation (the failure mode) leading to that effect may occur

Copyright JCAHO 2001 113
Step 5
� Conduct root cause analysis of top CI failure modesEquipment People
Environment Process
IllegibleHandwriting
Poor handwriting skills of MDMD not informed of need/P&P
No verification processNo list of unapproved abbrev.
Lack of MD order entryLack of Preprinted Order Sheets

Copyright JCAHO 2001 114
The three The three The three The three
levels of levels of levels of levels of causecausecausecause
Consequences
Action
Intent
Component Component Component Component
Causes Causes Causes Causes (Physical)(Physical)(Physical)(Physical)
Decision Roots (Human)
Deficiencies in
Organizational Systems (Latent)
The logic tree root system depicts the origin of failureThe logic tree root system depicts the origin of failureThe logic tree root system depicts the origin of failureThe logic tree root system depicts the origin of failure

115
P���� �!�����!a� RCA1. %��"%�8*���7'.��, }>��A��T2. � >� �$ 6?%��*��:����$Flow3. ��A7#��%"F'#t(�4. ��%����(���A�'��� �*%��*��:��5. (�47"!(�/���������%��"#t(�6. (�-�%(�7:��#t(�+(;<����7. ���('"�7 B3�-�����.�9:8. ��"��$6&9. ���('"%#'.'� ��#H�A �� ('� ����$
+($)

Copyright JCAHO 2001 116
Y = f (X1 X2 X3 X4sssXn)Dead = f (2��������0�m �+��������), ������1. h�� �/�����ssXn)
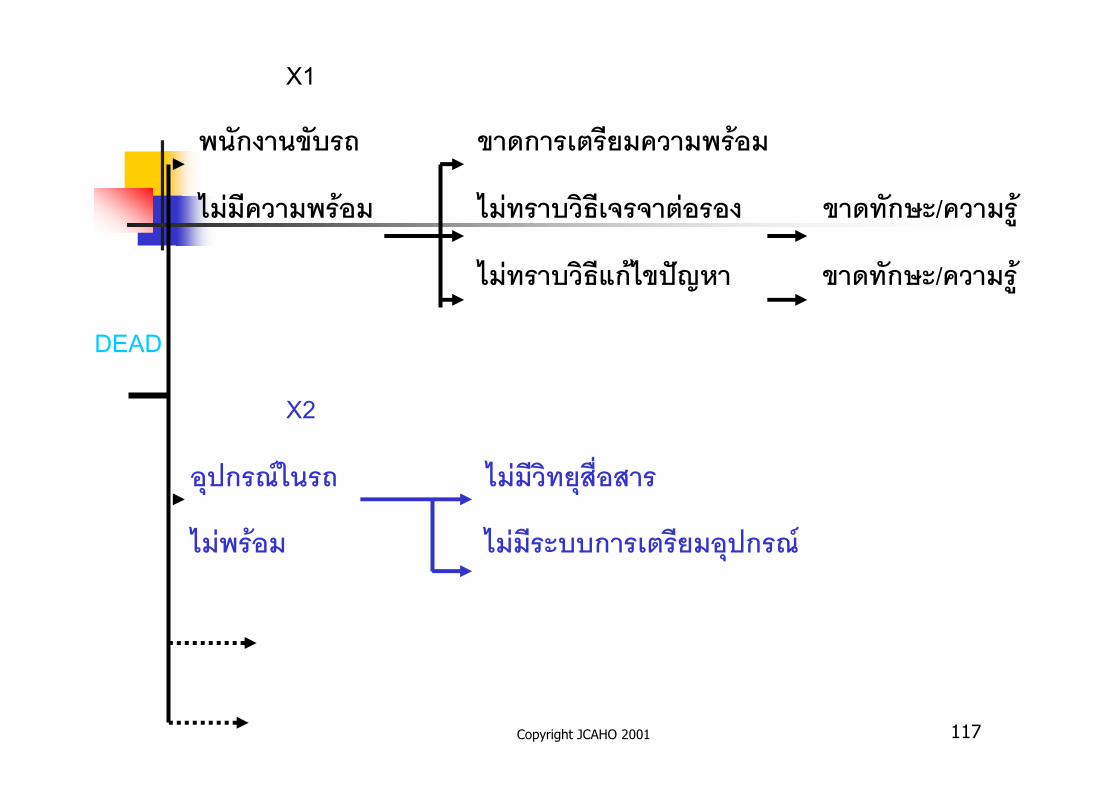
Copyright JCAHO 2001 117
X1
2��������0�m �������+��������2� ��
��"������2� �� ��"���0��t��-�-�+"���� ������=�/�����.
��"���0��t�!� ��ni*� ������=�/�����.
DEAD
X2
����),(��m ��"��������/�����
��"2� �� ��"����00����+��������),

Copyright JCAHO 2001 118
��" dead 2��������0�m -����00�+��������2� �� u�����g
refer ��� ������2� �� ������13
���0���=��-�-�+"���� v�/+��+��
���0���=�!� ni*� v�/+��+��

Copyright JCAHO 2001 119
�3���t ��-���� ������3� 1. ��01����0 ���/��������� 13
2�w������ 1. -��(* ����� ������������� ��3��� (**.) -'���� u�����g2� ����� u�����g ��0(*�" ��3��� (**.) �������� 2 �����2��������0�m -���'���)x, ���u� ��.�, ��.�
- �/����� ����g- ������13
2. -��(* �����������13
3. -���0����t��-�-�+"����/ !� ni*� --���0��-������13

Copyright JCAHO 2001 120
�3���t ��-���� ������3� 1. ��01����0 ���/��������� 13
2�w����00 1.+���������� 1 �.� *�. h�� ��+�����{�0�+�
����+����
����),�m 2.�����-�� 2-3 �.� *�. h�� +����)x,
|���|�� �'���)x,
3 ����g(� 1 �.� *�. h��
4.+��+����� 30 �.� �������}
�'��(�

Copyright JCAHO 2001 121
�3���t ��-���� ������3� 1. ��01����0 ���/��������� 13
2�w����00 -��3/���� �� -1. h���"�+"� -
Copyright JCAHO 2001 122
Requirements of LD.5.2
� Redesign the process and/or underlying systems to minimize the risk of that failure mode or to protect patients from the effects of that failure mode

Copyright JCAHO 2001 123
Step 6
� Brainstorm actions that could reduce the criticality index starting with failure modes that have the highest CI value that:� Decrease likelihood of occurrence� Decrease the severity of effects� Increase the probability of detection

Copyright JCAHO 2001 124
Requirements of LD.5.2
� Pilot test and implement the redesigned process.
� Identify and implement measures (indicators) of the effectiveness of the redesigned process.

Copyright JCAHO 2001 125
Requirements of LD.5.2
� Implement a strategy for maintaining the effectiveness of the redesigned process over time.
Copyright JCAHO 2001 126
Note similarities to PI
� PI.2 The new/modified process is designed well.� PI.2.1 Performance expectations are established for new/modified processes
� PI.2.2 The performance of new/modified processes is measured
� PI.5 Improved performance is achieved and sustained over time

Copyright JCAHO 2001 127
Remember
� Take small bites – keep it simple.� FMEA on PCA
� Think: “what could possibly go wrong”� Or what has gone wrong frequently in past
� Any modification to the process, creates new risk points.

Copyright JCAHO 2001 128
Parting Thought
� On survey, JCAHO is currently not evaluating how good your FMEA process is.
� JCAHO is evaluating whether you used a proactive process (that includes the elements of the intent) to determine risk points and then took action to reduce the risk
129
Questions?