kuliah clp 2015 april. fk unlam.ppt
TRANSCRIPT
CCLEFT LIP AND PALATELEFT LIP AND PALATECELAH BIBIR DAN PCELAH BIBIR DAN PALATUMALATUM
Departemen Ilmu Bedah/Divisi Bedah Plastik FK Unlam/RSUD Ulin Banjarmasin
Dr. Sulandri Gusasi, SpBP-RE
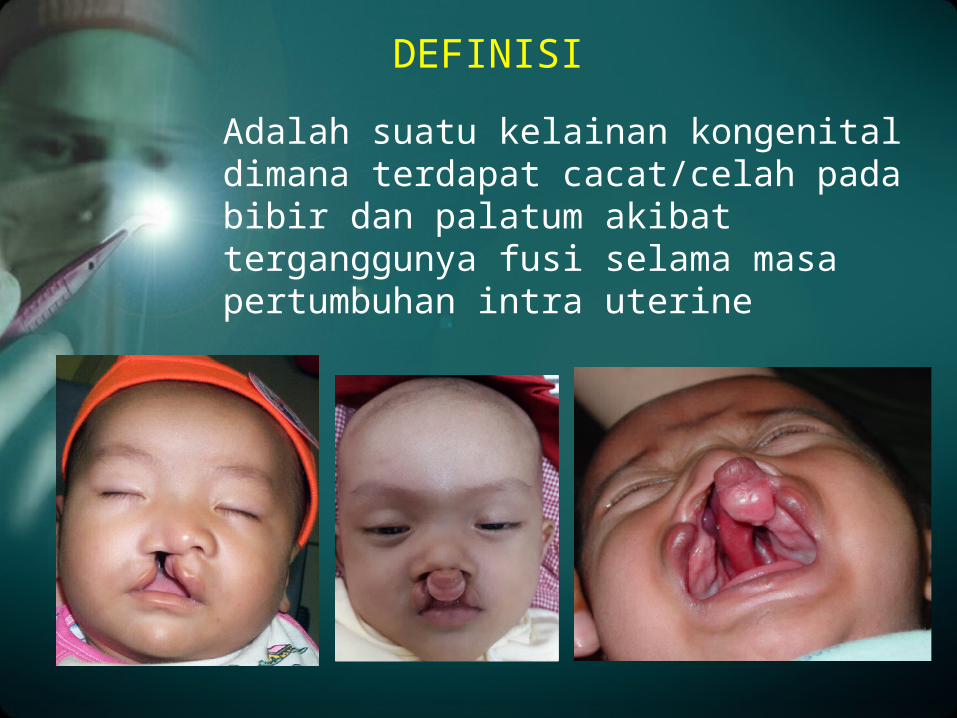
Adalah suatu kelainan kongenital dimana terdapat cacat/celah pada bibir dan palatum akibat terganggunya fusi selama masa pertumbuhan intra uterine
DEFINISI
Sejarah
• Fabricus ab Aquapendente (1537-1619) • CLP disebabkan oleh gangguan
embriologis
• Pada akhir tahun 1950, Ralph millard mengembangkan teknik yang dinamakan “cut as you go”.
• Tenssion (1952) mengembangkan tehnik operasi CLP dengan melakukan flap dengan membuat “figure of Eight” yang mengkaitkan tepi dari bibir ke tepi seberang sisi bibir yang mengalami pembelahan
• Peter Raandal (1960) menciptakan teknik standar dalam rekonstruksi CLP, dengan membuat flap segitiga
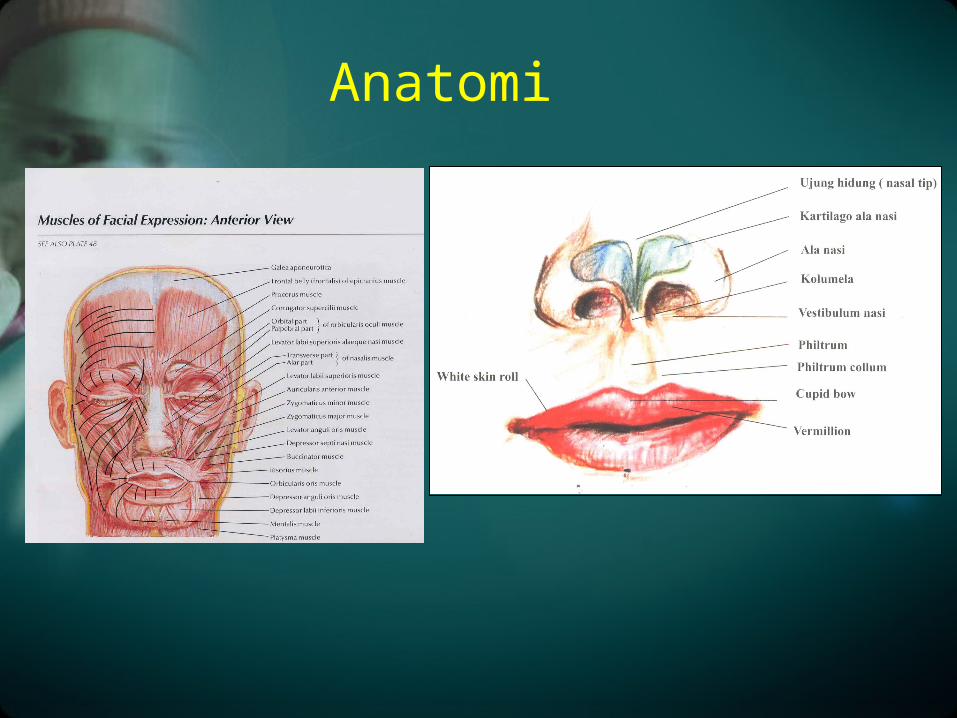
Anatomi
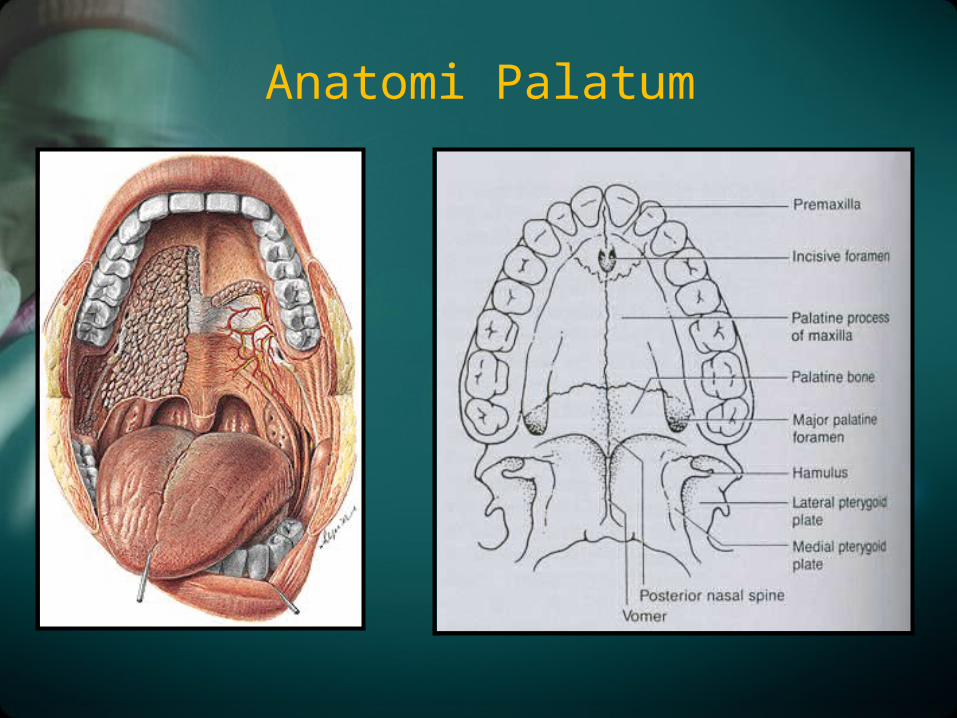
Anatomi Palatum
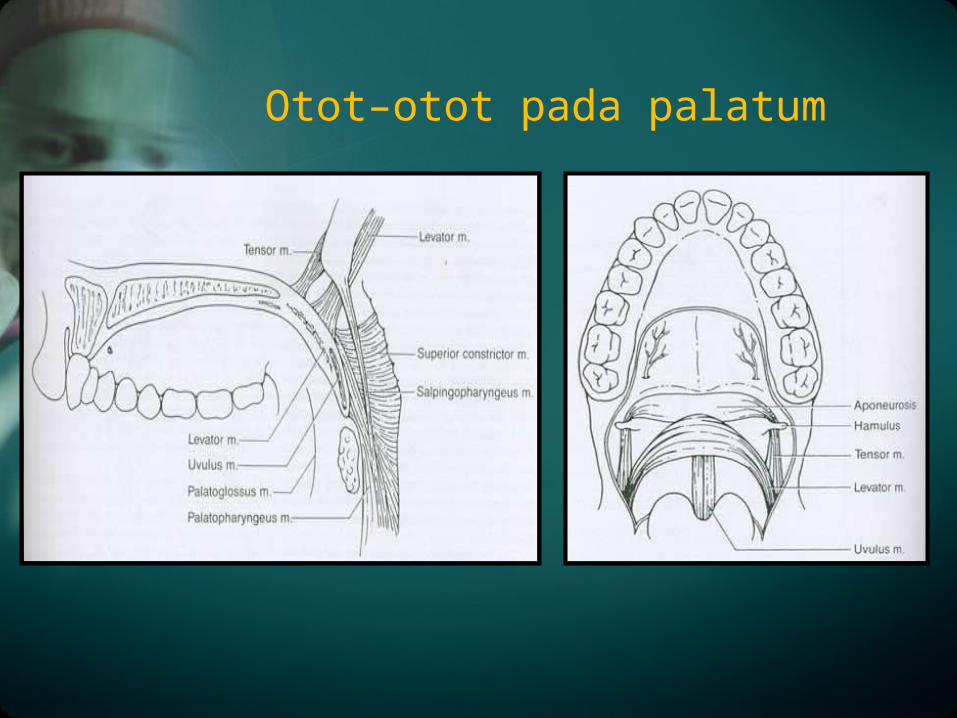
Otot–otot pada palatum
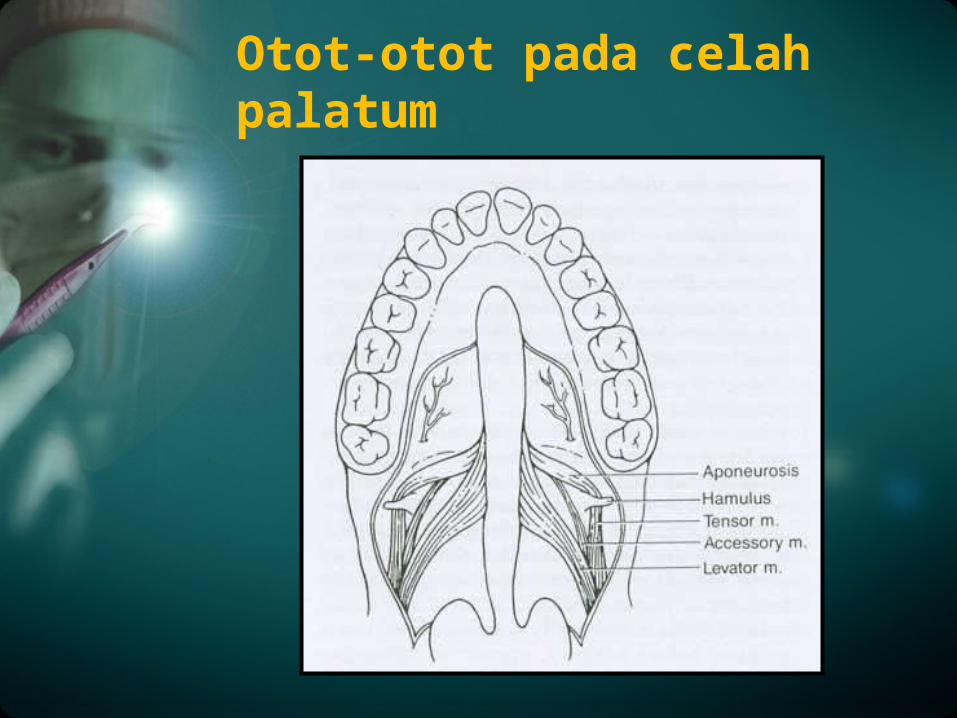
Otot-otot pada celah palatum
1939 FOGH-ANDERSON : 1:750 dari kelahiran hidup
1950 MILLARD-LA ROSSA : 1:760 di PENSYLVANIA
BURDY dan HABIB : Berdasarkan ras ; Pada bangsa Asia, sekitar 2,1 anak dari tiap 1000 kelahiran mengalami CLP. Pada ras kulit putih prevalensi mencapai 1 kasus/ 1000 kelahiran, pada ras kulit hitam mencapai 0,4 kasus tiap 1000 kelahiran.
Prevalensi jenis kelamin ; laki-laki lebih banyak menderita dibanding wanita dengan rasio 3:1.
Epidemiology
Bisa syndromik atau non syndromik.
Syndromik : bila terdapat lebih dari satu malformasi dan
menyangkut lebih dari satu daerah perkembangan.
Non syndromik : hanya terdapat satu malformasi atau terdapat
beberapa anomali yang berasal dari satu daerahperkembangan.
Sebagian besar kasus celah bibir dan langit-langit adalah non syndromik.
ETIOLOGI :
A. Faktor HEREDITERSebagai faktor yang sudah dipastikan.Gilarsi : 75% dari faktor keturunan resesif dan 25% bersifat dominan.
1. Mutasi gen.
2. Kelainan kromosom
FAKTOR PENYEBAB :
Faktor GenetikExtra Cellular Molecules (ECM), yang berperan
sebagai faktor pertumbuhan dan induksi terhadap molekul protein :
• Bone Morphogenic Protein : berperan membentuk palatum
• Sonic Hedgehog:membentuk primordial wajah dan epitel
• Fibroblast Growth factor :membentuk matrix ekstraseluler palatum
• Gen TBX 22 adalah gen yang berperan penting dalam pembentukan mesoderm jaringan. Mutasi pada gen ini akan menyebabkan adanya gangguan spesifikasi mesoderm sehingga menyebabkan CLP
B. FAKTOR EKSTERNAL / LINGKUNGAN :
1. Faktor usia ibu.
2. Obat-obatan. ( asetosal atau aspirin sebagai obat analgetik, rifampisin, fenasetin, sulfonamide, aminoglikosid, indometasin, asam flufetamat, ibu profen dan penisilamin, diazepam, kortikosteroidm, antihistamin )
3. Nutrisi Alkohol
5. Penyakit infeksiSifilis, virus rubella
6. Radiasi
7. Stres emosional
8. Trauma, (trimester pertama)
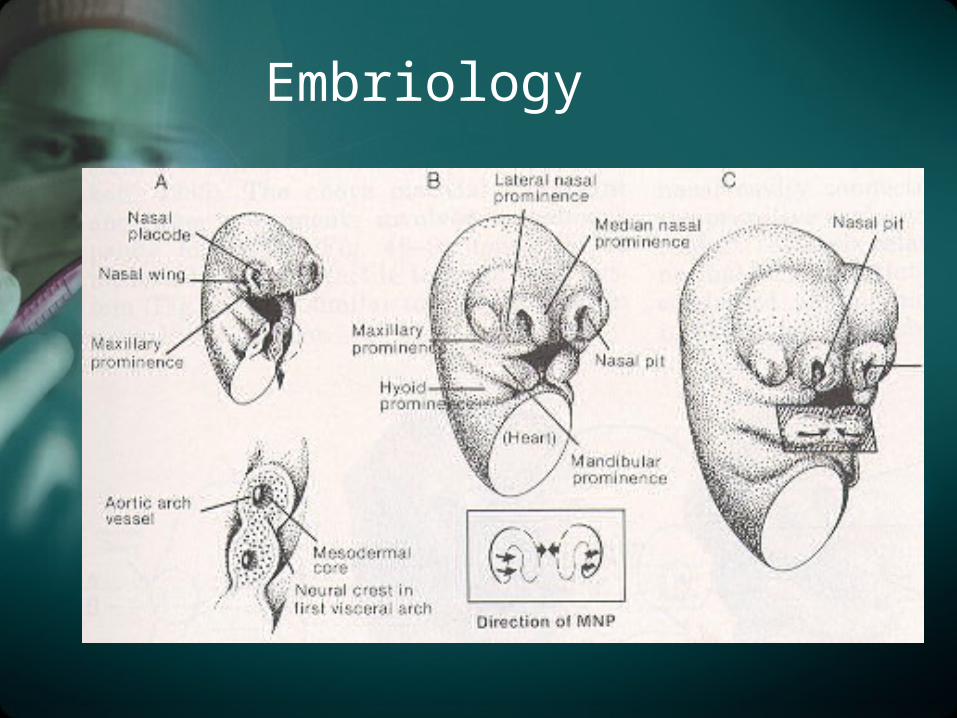
Embriology
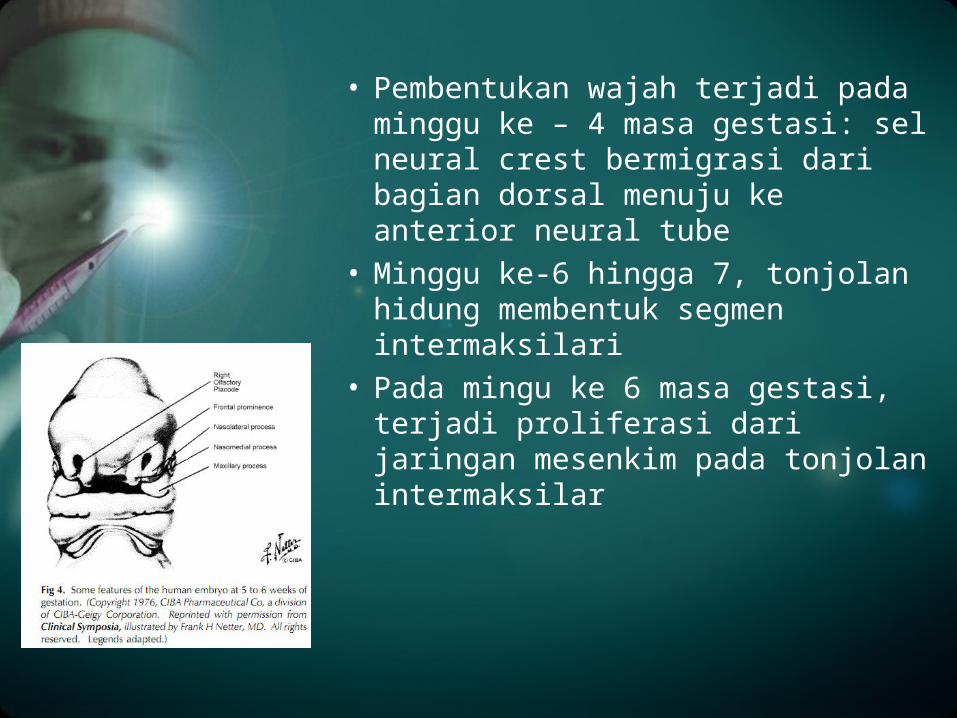
• Pembentukan wajah terjadi pada minggu ke – 4 masa gestasi: sel neural crest bermigrasi dari bagian dorsal menuju ke anterior neural tube
• Minggu ke-6 hingga 7, tonjolan hidung membentuk segmen intermaksilari
• Pada mingu ke 6 masa gestasi, terjadi proliferasi dari jaringan mesenkim pada tonjolan intermaksilar
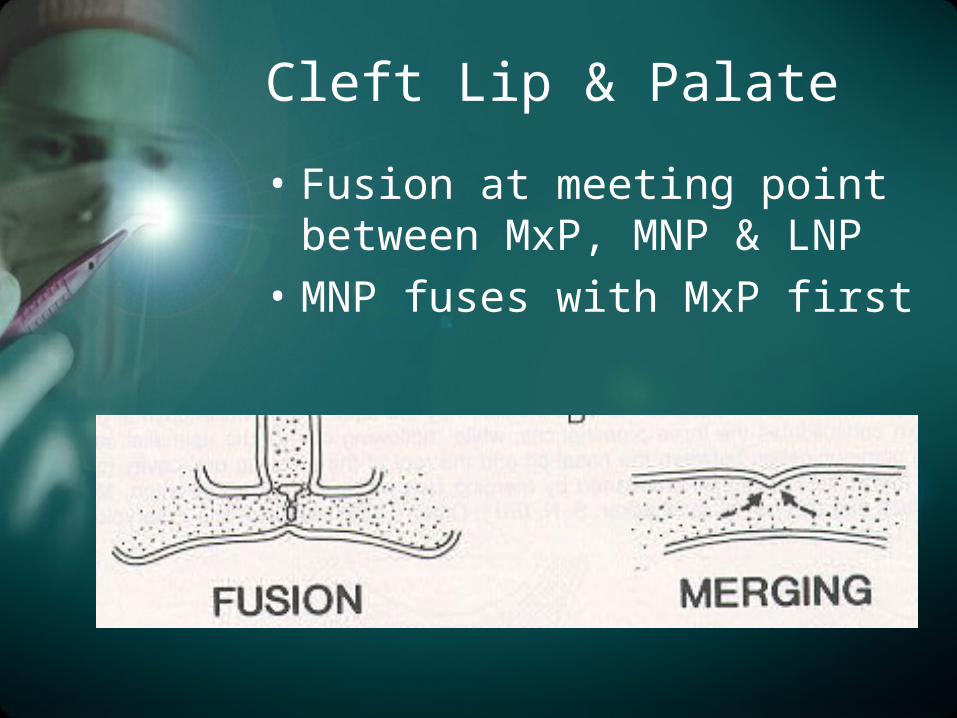
Cleft Lip & Palate
• Fusion at meeting point between MxP, MNP & LNP
• MNP fuses with MxP first
Klasifikasi dan morfologi
• Klasifikasi Davis and Ritchie ; tahun 1922 mengklasifikasikan ke dalam 3 grup sesuai posisi celah dalam hubungannya dengan proses alveolar.
• Klasifikasi Veau ; Sistem klasifikasi veau membagi cleft lip and palate ke dalam 4 grup.
• Klasifikasi Arturo Santiago ; menggunakan 4 angka untuk mengindikasikasikan adanya celah dan lokasinya. Masing masing angka diikuti oleh huruf yang mengindikasikan kondisi celah (komplit, inkomplit, submukosa).
• Tahun 1962, American Commitee for Cleft Palate Rehabilitation membuat standarisasi yang kemudian diadopsi oleh Cleft Palate Association
• Kernahan dan Stark membuat klasifikasi yang lebih simple dan lebih jelas. Pada tahun 1971, Kernahan menghasilkan klasifikasi berdasarkan huruf Y (Stripped Y Method ) yang menggunakan foramen incisivus sebagai titik panduan
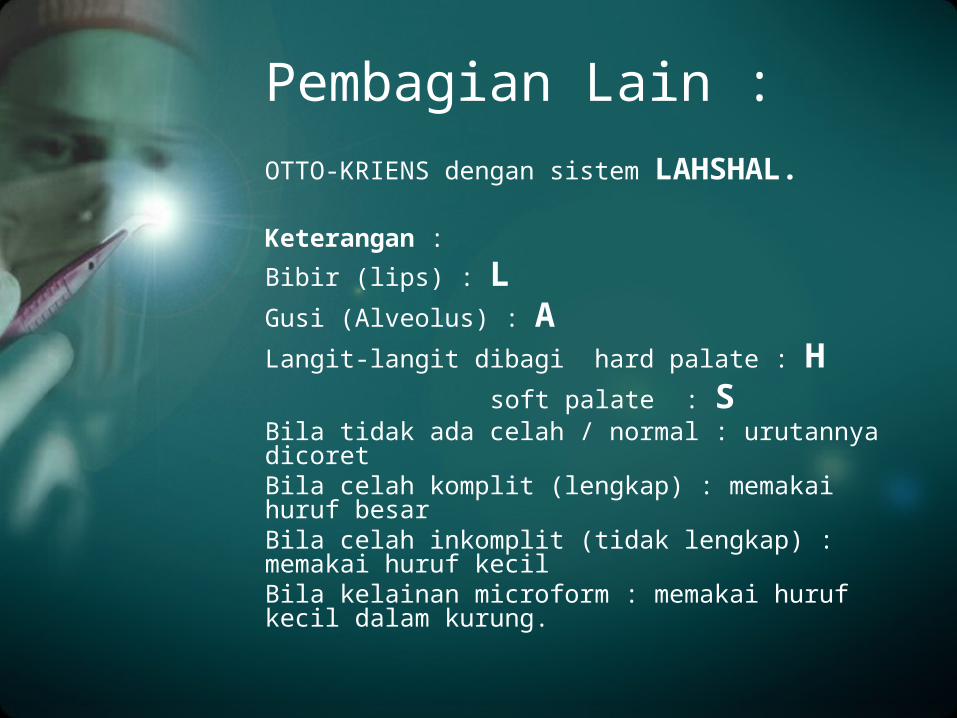
OTTO-KRIENS dengan sistem LAHSHAL.
Keterangan :
Bibir (lips) : LGusi (Alveolus) : ALangit-langit dibagi hard palate : H
soft palate : SBila tidak ada celah / normal : urutannya dicoretBila celah komplit (lengkap) : memakai huruf besarBila celah inkomplit (tidak lengkap) : memakai huruf kecilBila kelainan microform : memakai huruf kecil dalam kurung.
Pembagian Lain :
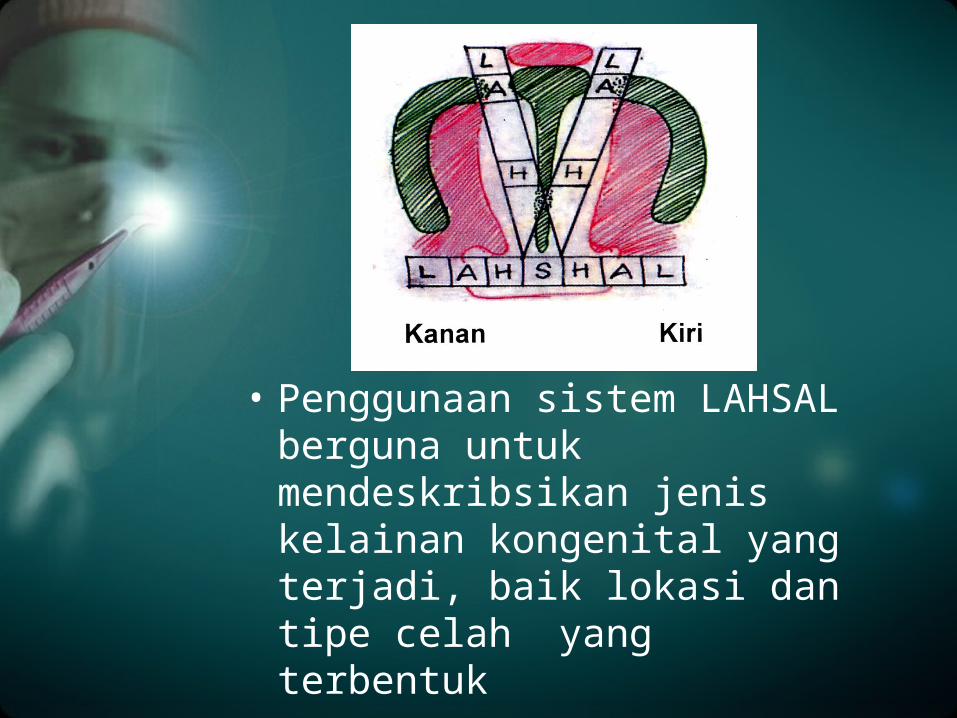
• Penggunaan sistem LAHSAL berguna untuk mendeskribsikan jenis kelainan kongenital yang terjadi, baik lokasi dan tipe celah yang terbentuk
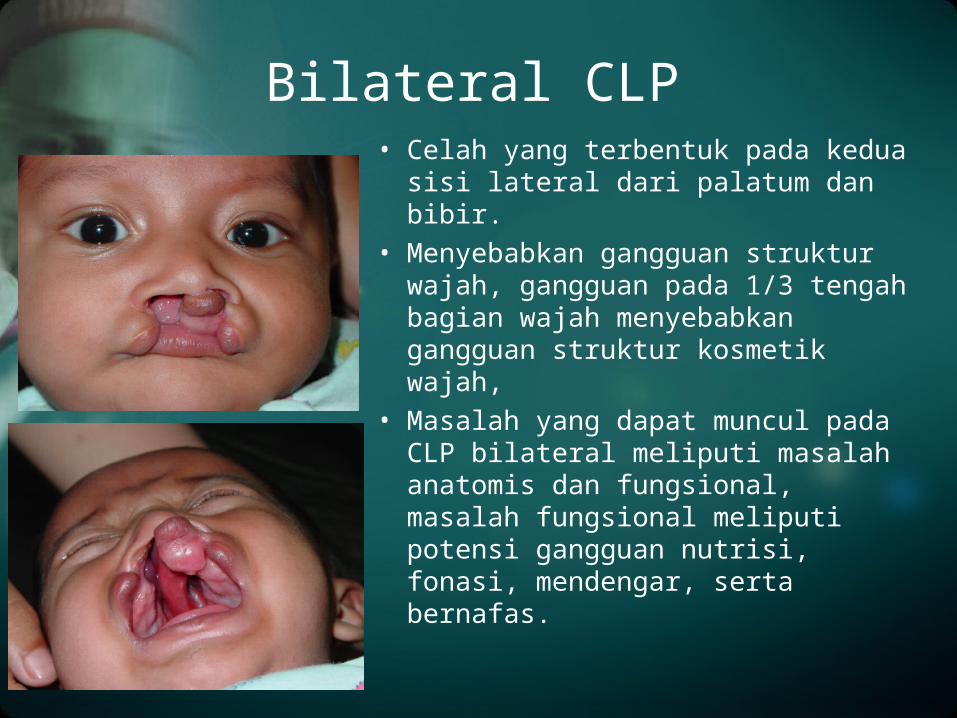
Bilateral CLP • Celah yang terbentuk pada kedua sisi
lateral dari palatum dan bibir.
• Menyebabkan gangguan struktur wajah, gangguan pada 1/3 tengah bagian wajah menyebabkan gangguan struktur kosmetik wajah,
• Masalah yang dapat muncul pada CLP bilateral meliputi masalah anatomis dan fungsional, masalah fungsional meliputi potensi gangguan nutrisi, fonasi, mendengar, serta bernafas.
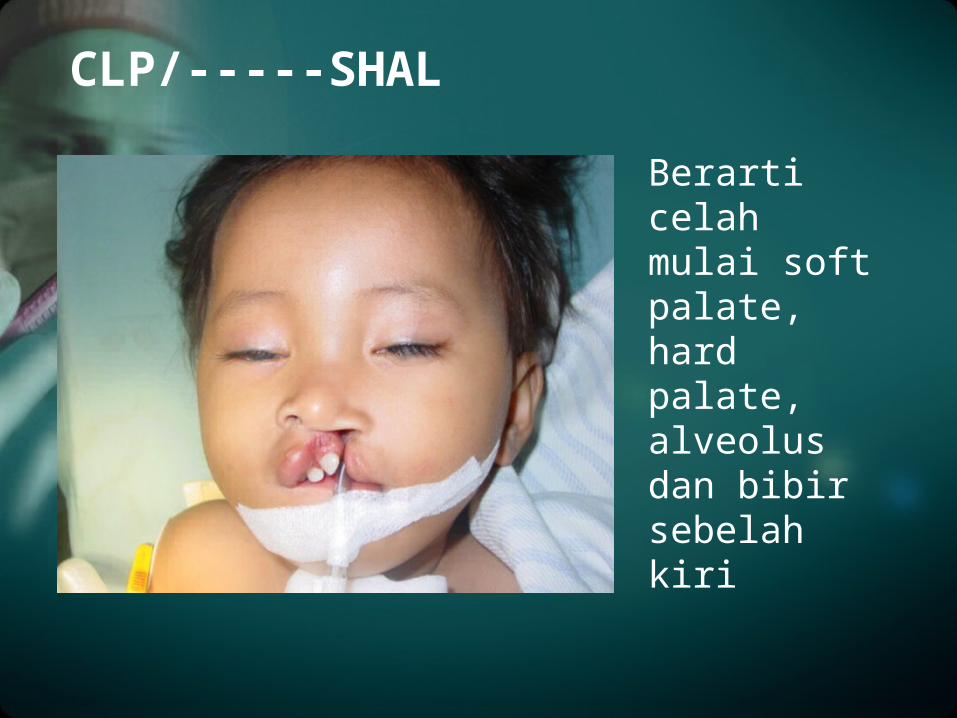
CLP/-----SHAL
Berarti celah mulai soft palate, hard palate, alveolus dan bibir sebelah kiri
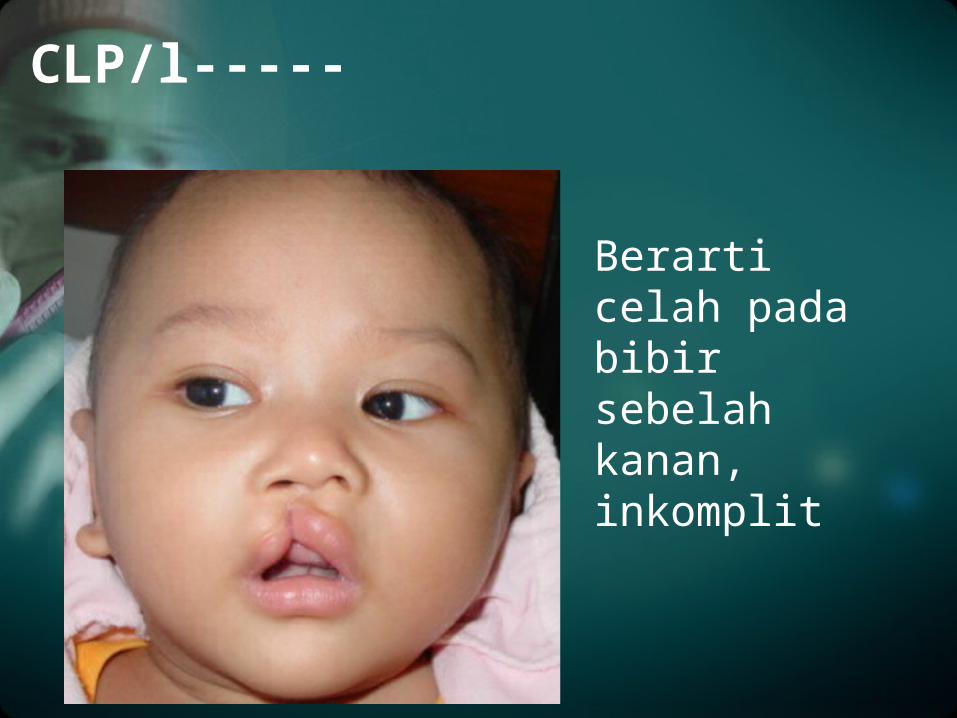
CLP/l-----
Berarti celah pada bibir sebelah kanan, inkomplit
Rule over ten :
1. Berat badan > 10 pon
2. Hemoglobin > 10 gr%
3. Umur > 10 minggu
Timing Operasi
1. Psikologis orangtua & anak
2. Nutrisi dan gizi
3. Infeksi (OMP)
4. Suara sengau : rhinolalia
5. Pertumbuhan gigi
6. Pertumbuhan tulang muka 1/3 tengah yang tidak normal
MASALAH YANG DIHADAPI
Meliputi :
1. Ahli bedah plastik.
2. Ahli THT
3. Dokter gigi/Orthodontist
4. Speech therapist.
5. Psikolog/Psikiater
6. Social worker
Penanganan Multidisiplin
1. Penjelasan kepada orangtuanya
2. Umur 3 bulan (rule over ten)Operasi bibir dan alanasi, evaluasi telinga.
3. Umur 10-12 bulanOperasi palato/celah langit-langit. Evaluasi pendengaran dan telinga.
4. Umur 1-4 tahunEvaluasi bicara. Speech theraphist setelah 3 bulan pasca operasi
5. Umur 4 tahunDipertimbangkan repalatoraphy atau/dan Pharyngoplasty
PROTOKOL PENANGANAN :
6. Umur 6 tahunEvaluasi gigi dan rahang. Evaluasi pendengaran.
7. Umur 9-10 tahunAlveolar bone graft
8. Umur 12-13 tahunFinal touch, perbaikan-perbaikan bila diperlukan.
9. Umur 17 tahunEvaluasi tulang-tulang muka.Bila diperlukan advancement osteotomy Le FORT I
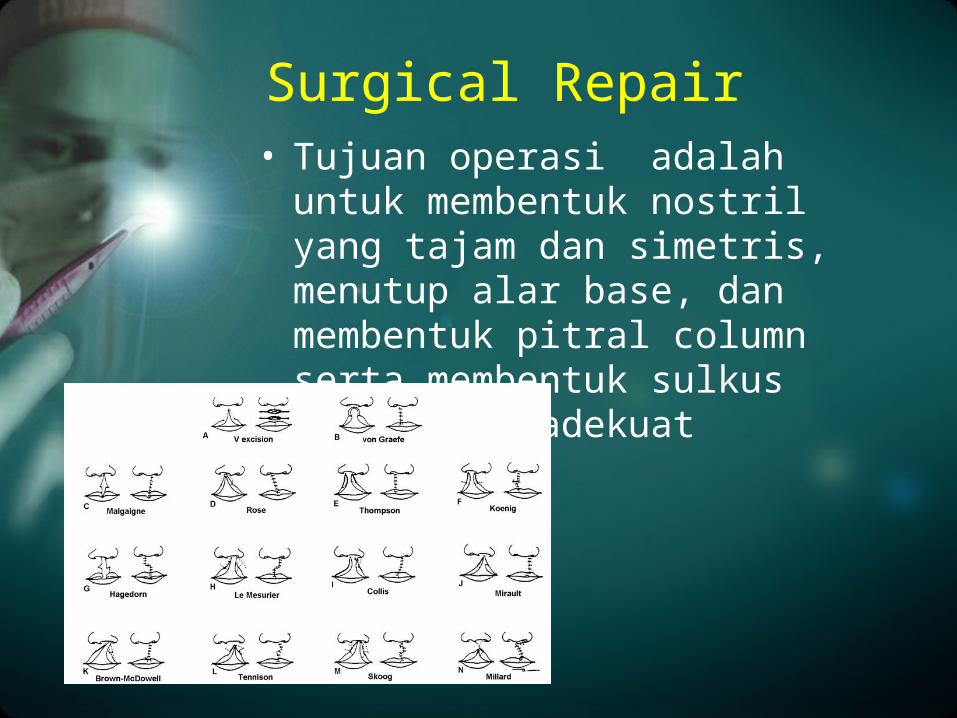
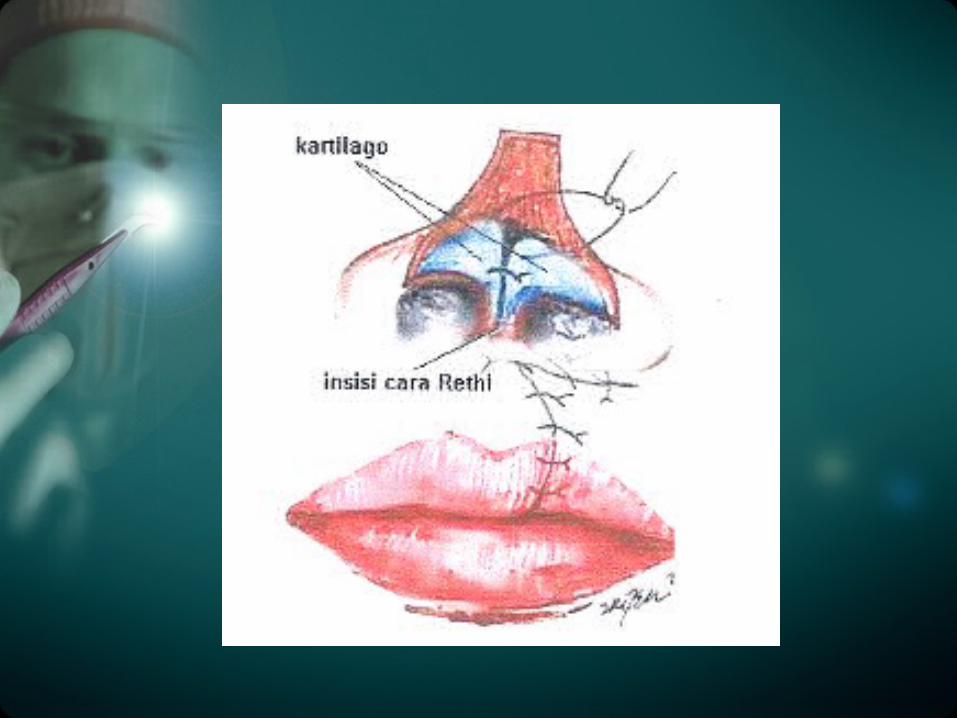
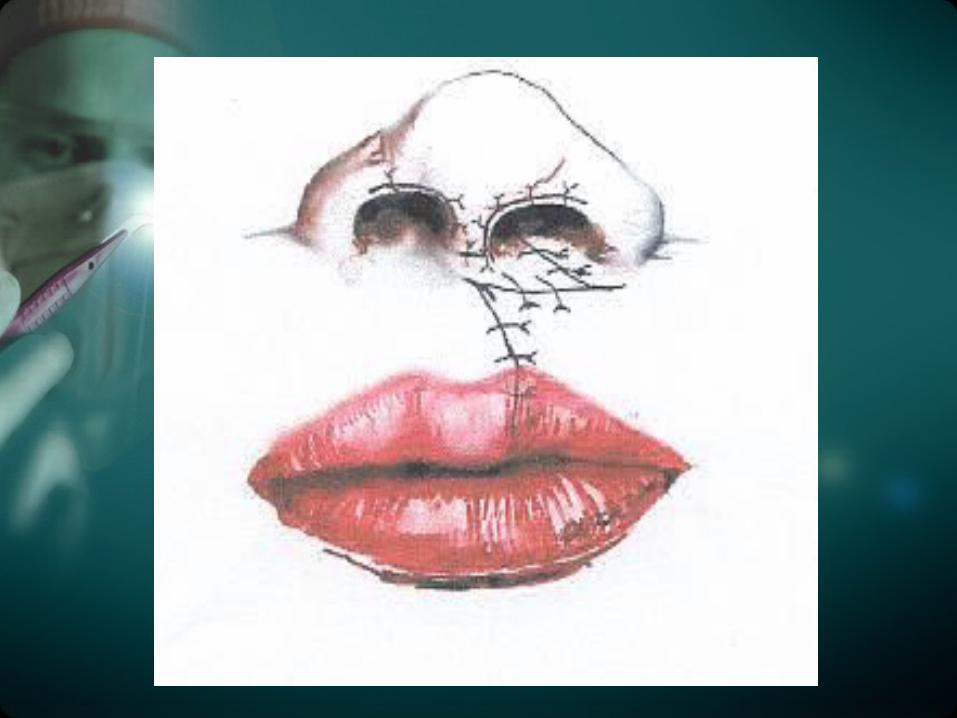
Surgical Repair • Tujuan operasi adalah untuk
membentuk nostril yang tajam dan simetris, menutup alar base, dan membentuk pitral column serta membentuk sulkus labia yang adekuat
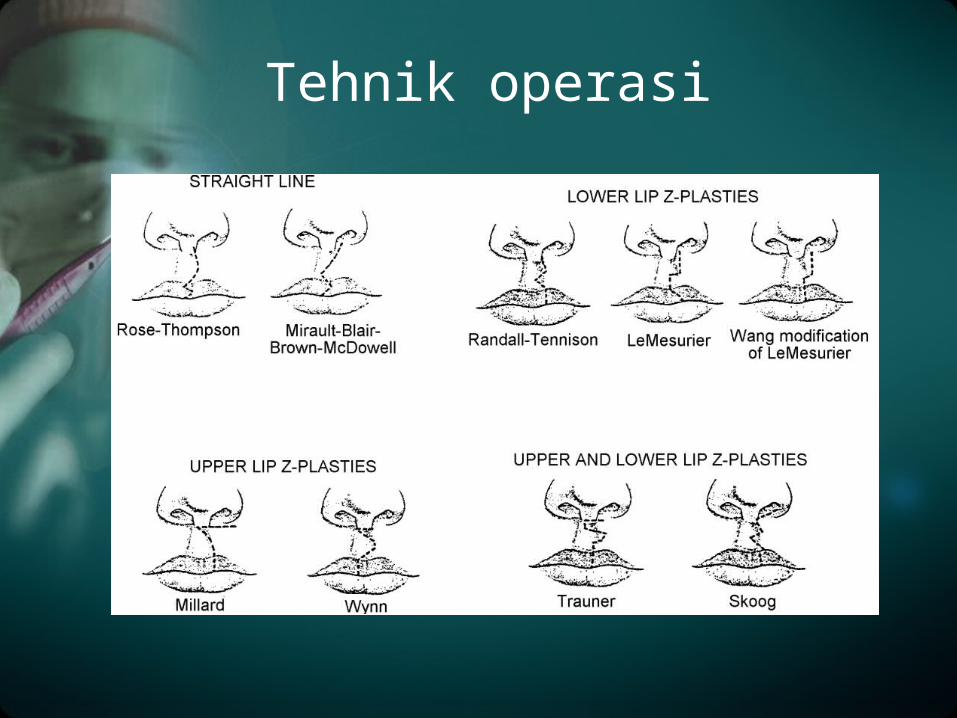
Tehnik operasi
• LeMesurier quadrilateral flap repair, • Randall-Tennison Triangular flap repair, • Millard rotation-advancement repair, • Skoorg and Kernahan-Bauer upper and
lower lip-Z plasty repair, • Rose Thompson repair .• Clifford dan Pool telah menunjukkan
hasil anatomi yang baik pada pasien Unilateral Cleft Lip yang menggunakan teknik pembedahan Z-Plasty
Tehnik operasi
Prinsip-prinsip Operasi Celah Bibir
Mengikuti kriteria• Perhitungan akurat pada kulit, otot, & mukosa• Luka parut samar• Panjang bibir simetris• Cupid bow simetris• Membentuk phyltrum & dimple• Bibir bawah tidak manyun setelah operasi• Lubang hidung simetris• Kolumela tegak• Membuat sulcus labialis• Teknik operasi yang mudah diterapkan
Cheiloraphy Unilateral
• Timing: mengikuti kaidah rule of ten
• Persiapan
• Posisi penderita
• Disain
• Tindakan
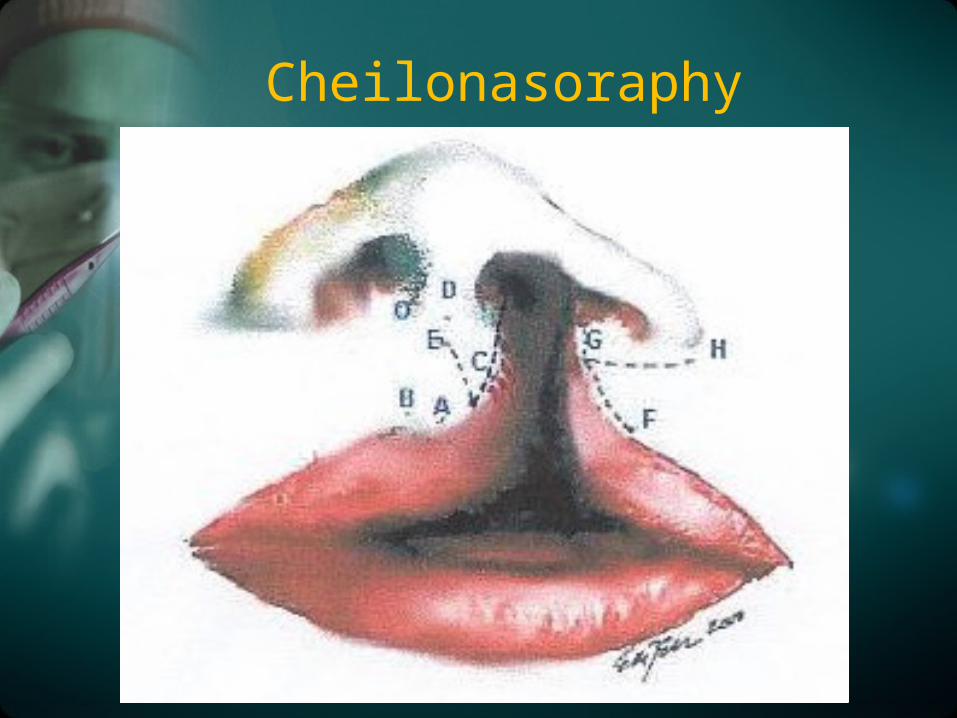
Cheilonasoraphy

HAL-HAL PENTING YANG HARUS DIPERHATIKAN PADA SAAT OPERASI
• Menghargai jaringan
• Trauma seminimal mungkin
• Benang sehalus mungkin
• Mengatasi regangan dg jahitan penunjang
• Tidak membuang jaringan
PERAWATAN PASCA BEDAH
• Salep antibiotik dosis rendah
• Rawat jalan
• Pemberian antibiotik
• Pembersihan luka
• Pengangkatan jahitan
• Kontrol
• Minum dengan sendok (untuk anak-anak)
KOMPLIKASI OPERASI
• Perdarahan
• Jahitan lepas
• Edema
• Ischemia
• Infeksi
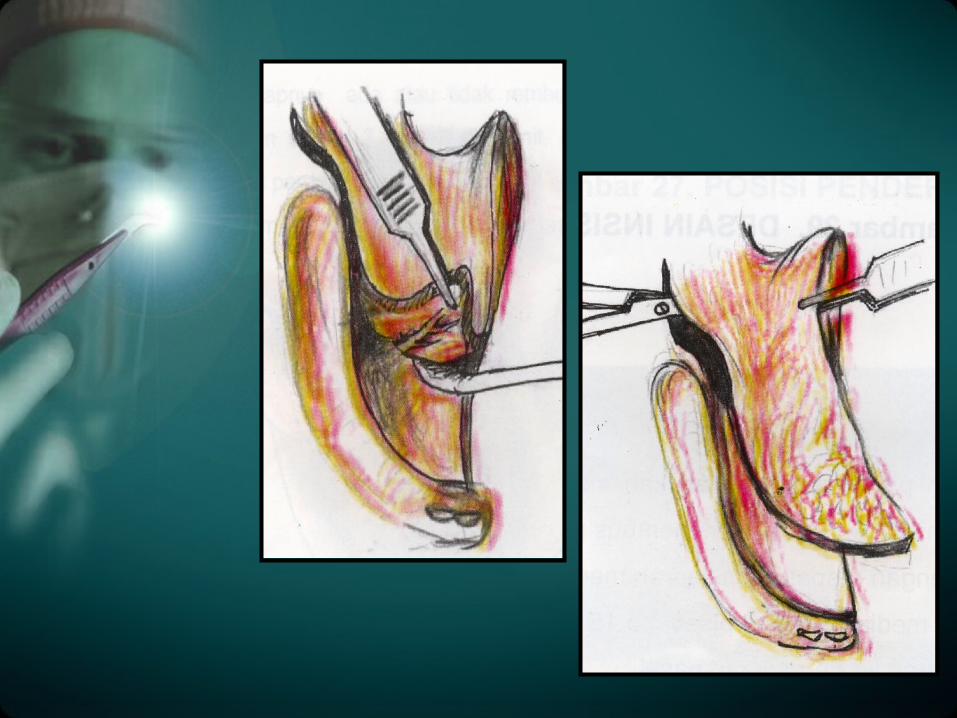
Palatoraphy
• Tujuan pembedahan palatoraphy : untuk meningkatkan perkembangan fungsi bicara dan meminimalkan efek samping dari celah palatum.
Penanganan Palatoraphy. Ditangani oleh tim untuk
mendeteksi kelainan lain yang berhubungan
• Konsep kerja :– Sistematis– Menyeluruh– Bekerja sama
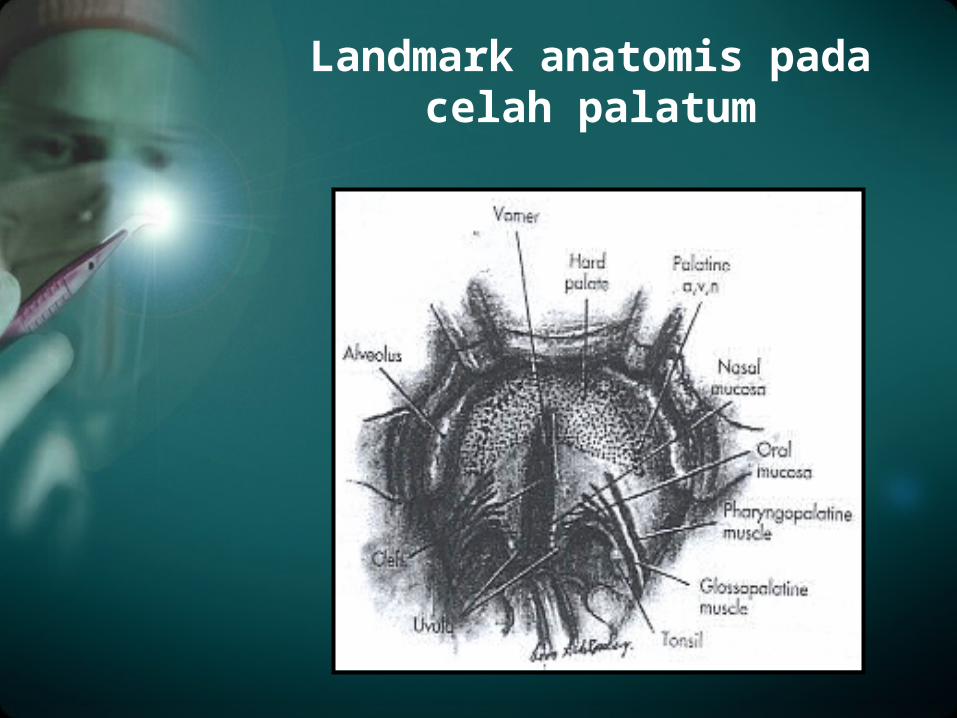
Landmark anatomis pada celah palatum

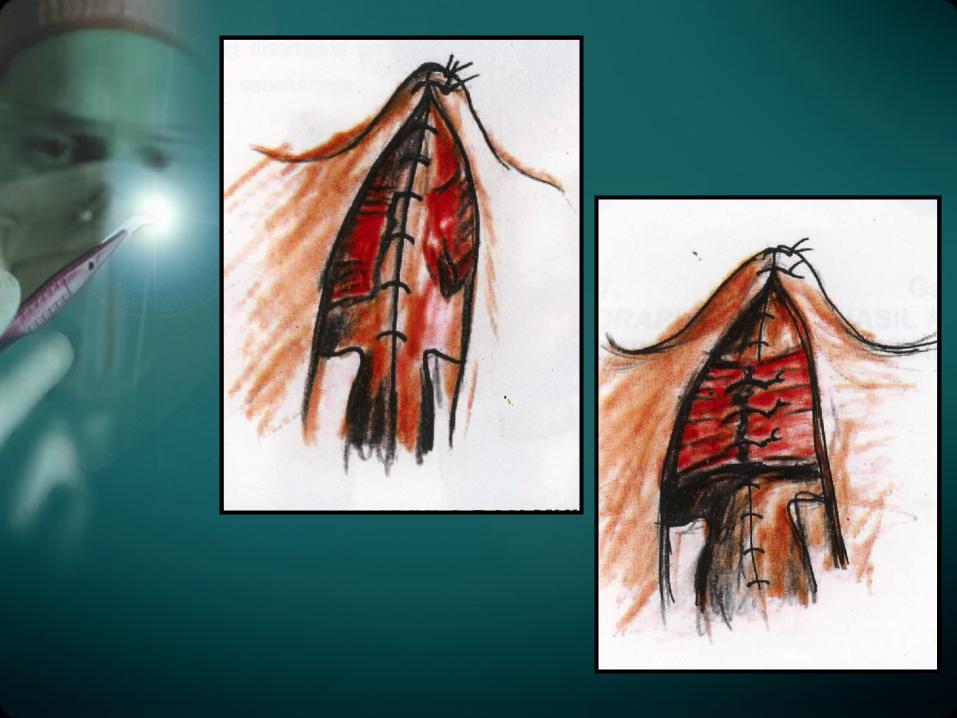
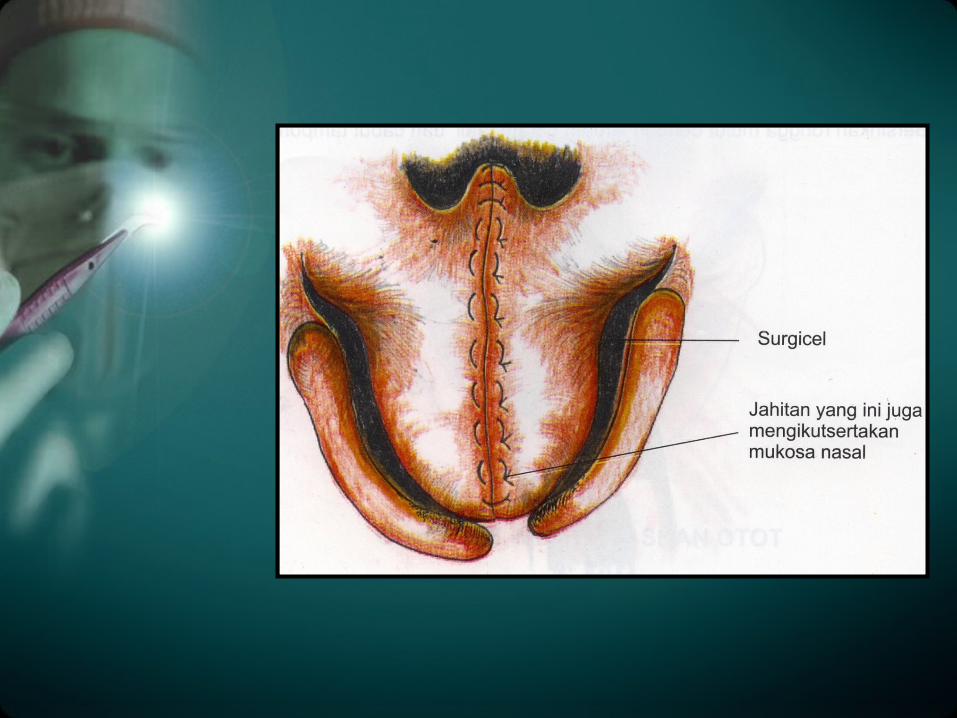
Teknik Operasi
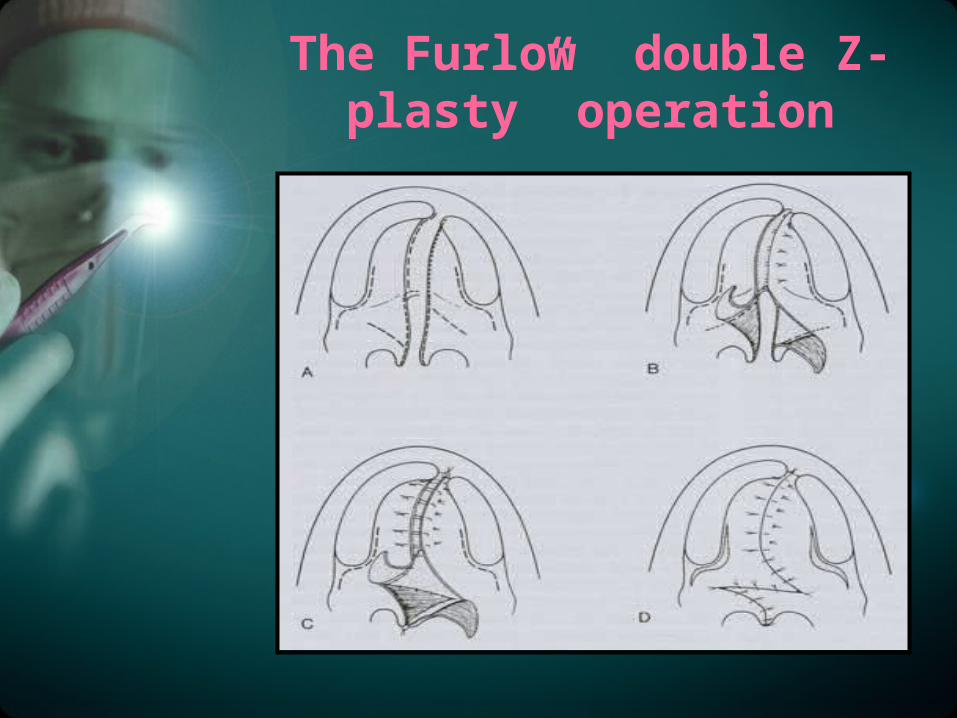
The Furlow ”double Z-plasty” operation
Waktu Intervensi
• Palatoraphy : 10-12 bulan - luka operasi diharapkan
sembuh,sebelum anak mulai aktif bicara
- 3 bln post operasi mulai speech theraphy
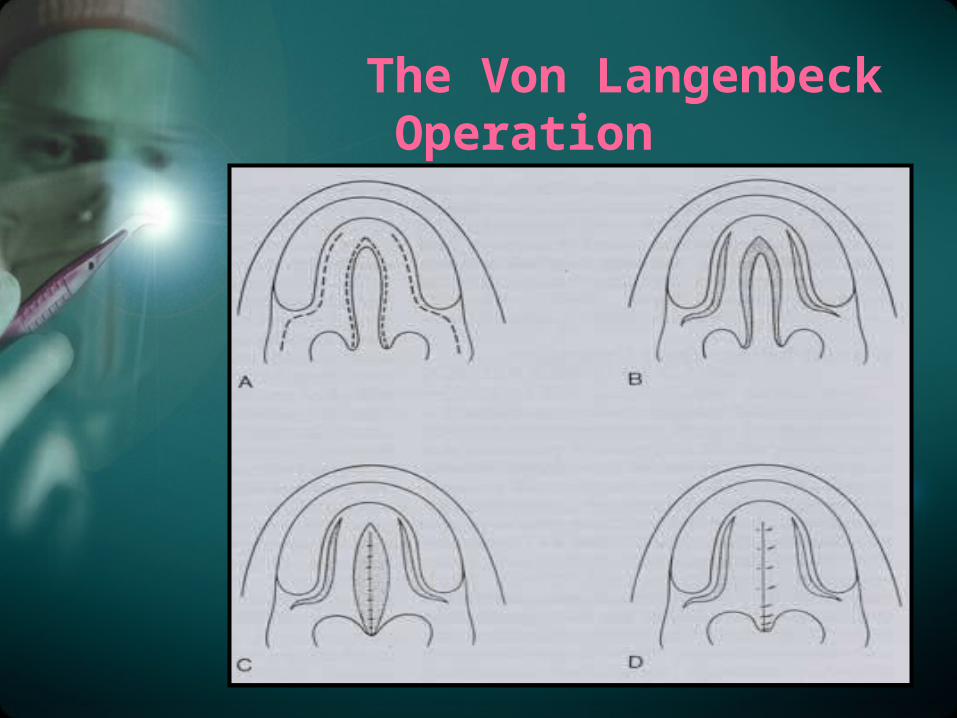
The Von Langenbeck Operation
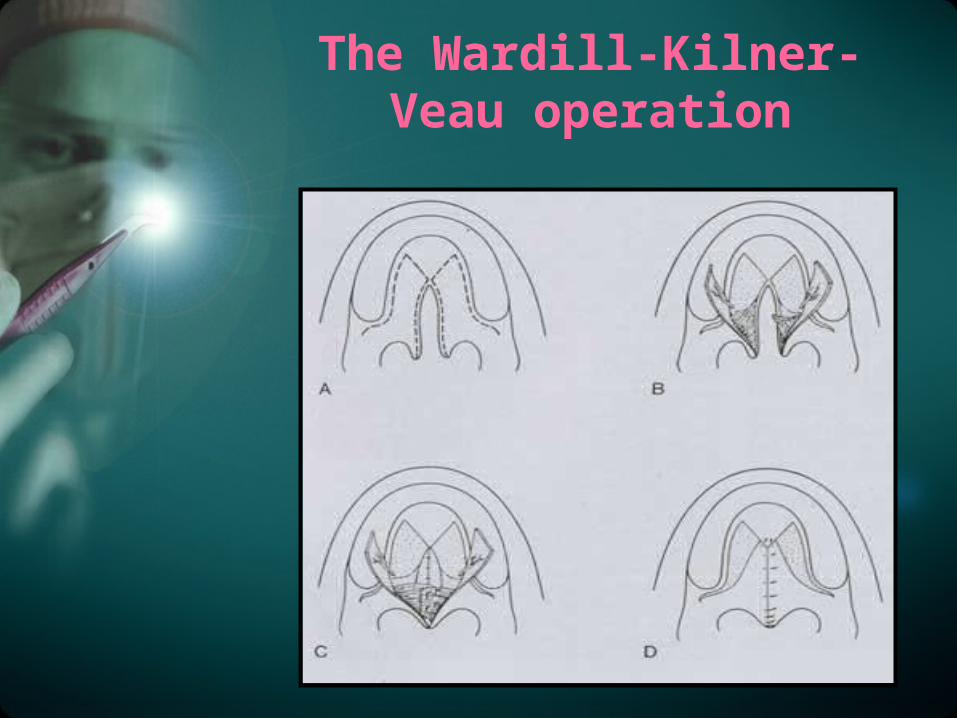
The Wardill-Kilner-Veau operation
Pharyngeal Flap
• Diperkirakan 70-80% CP mengalami perbaikan kemampuan velopharyngeal setelah palatoraphy
• Sekitar 20-30% perlu terapi bicara atau tambahan prosedur bedah pharyngeal flap
• Indikasi flap bila repaired palate terlalu pendek/otot tak berfungsi persistent hypernasal speech
Perawatan
• Post operasi,penderita melakukan diet cair TKTP selama 3 minggu, dan menjaga higiene oral
Komplikasi
• Perdarahan
• Wound dehiscense
• Infeksi
• Oronasal Fistula
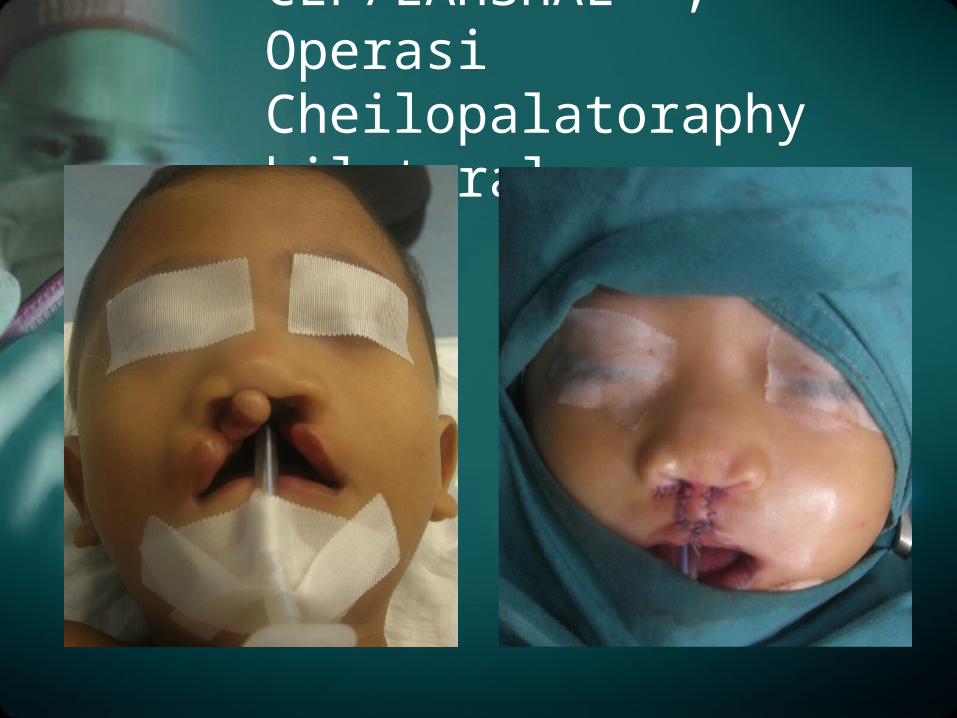
CLP/LAHSHAL ; Operasi Cheilopalatoraphy bilateral
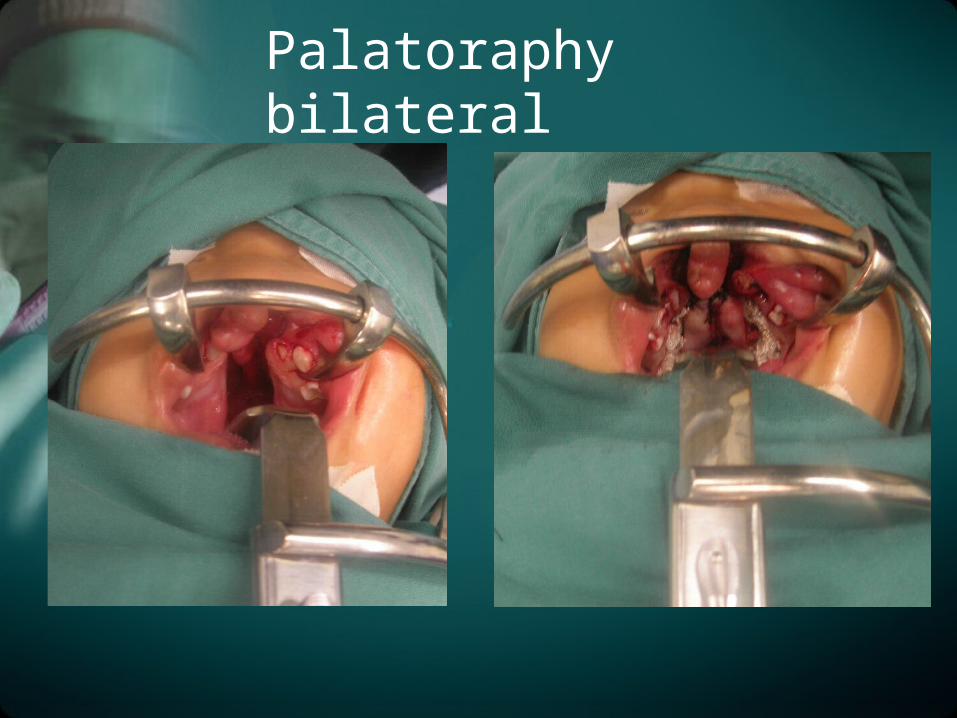
Palatoraphy bilateral
Terima Kasih
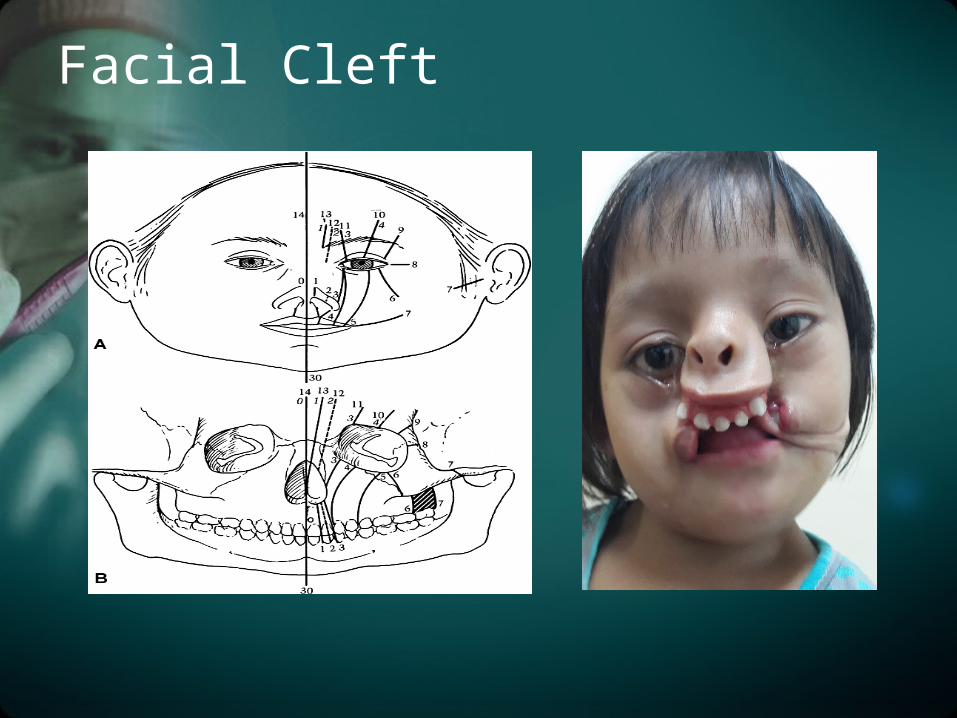
Facial Cleft
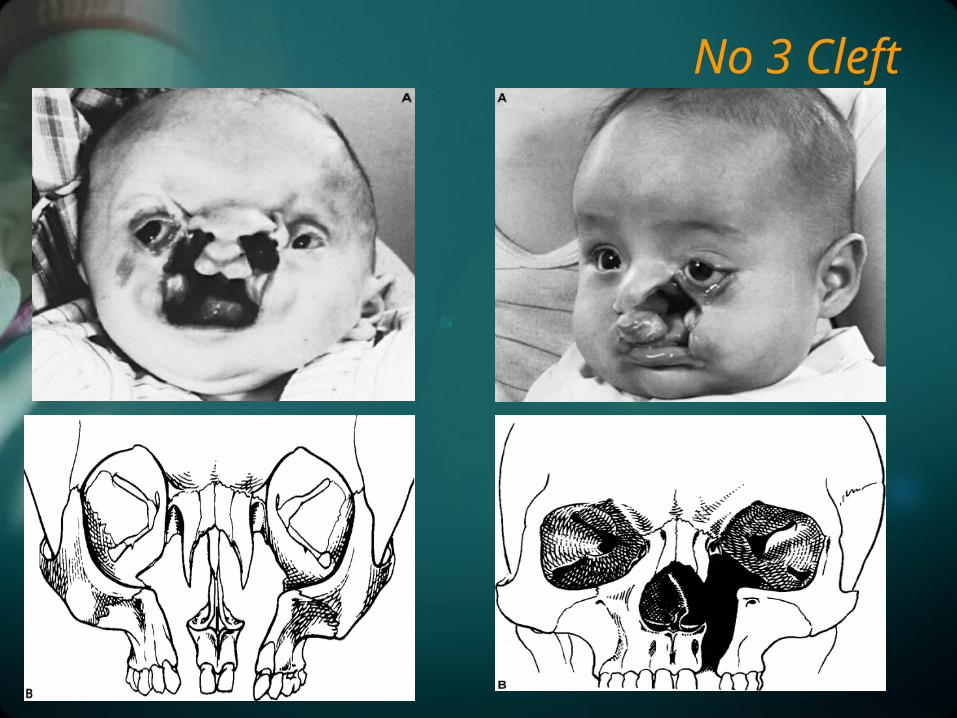
No 3 Cleft
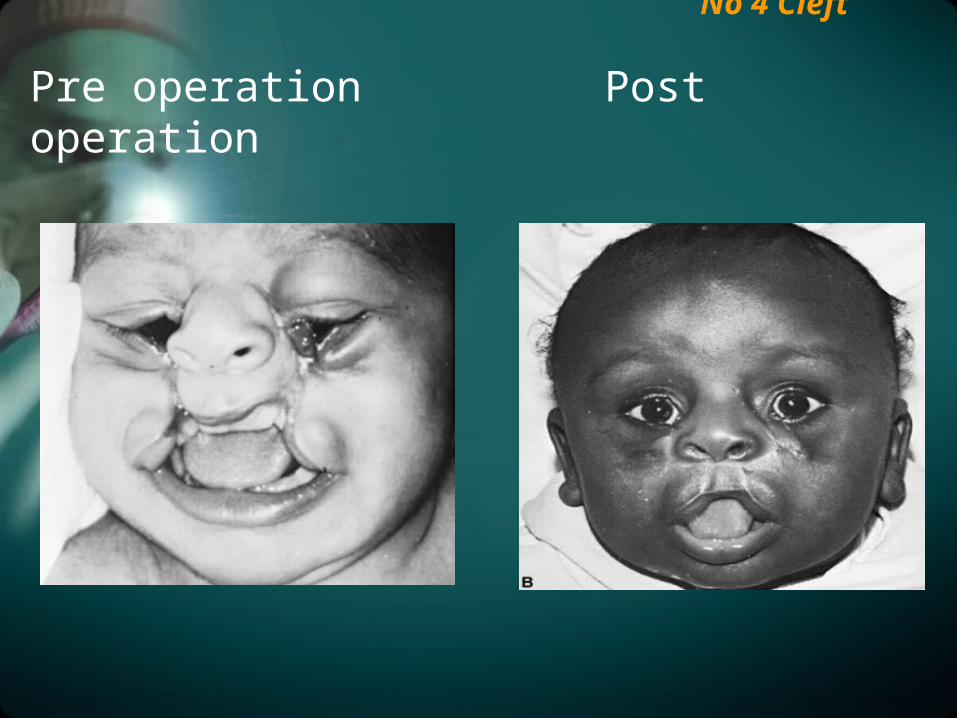
No 4 Cleft
Pre operation Post operation

No 5 Cleft
Treatment :
• Local transposition flaps
• Bone Graft
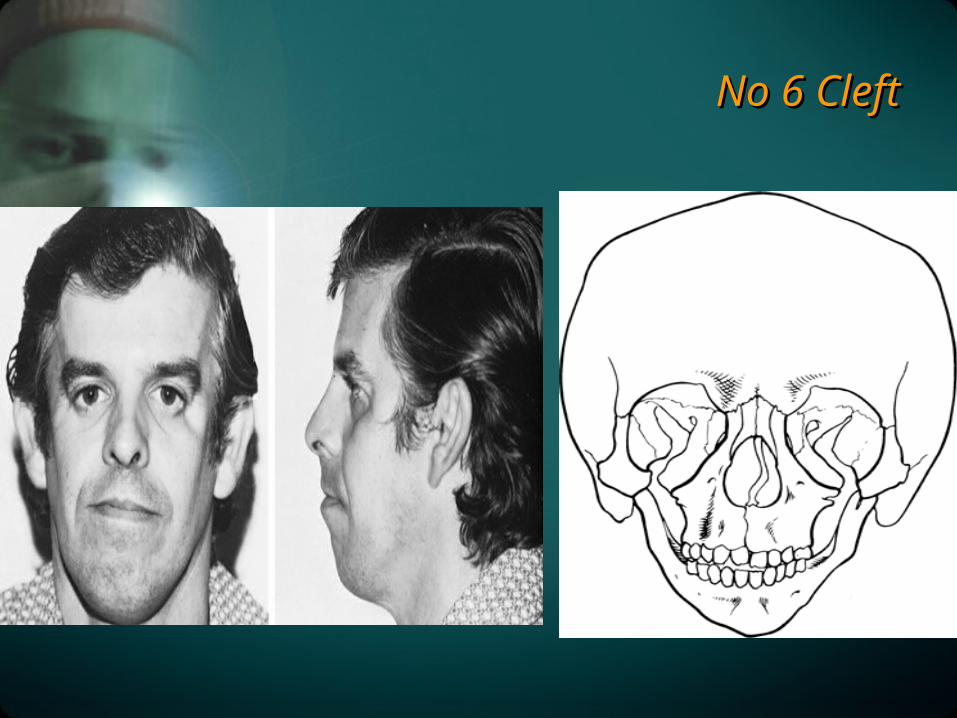
No 6 CleftNo 6 Cleft

No 7 CleftNo 7 Cleft
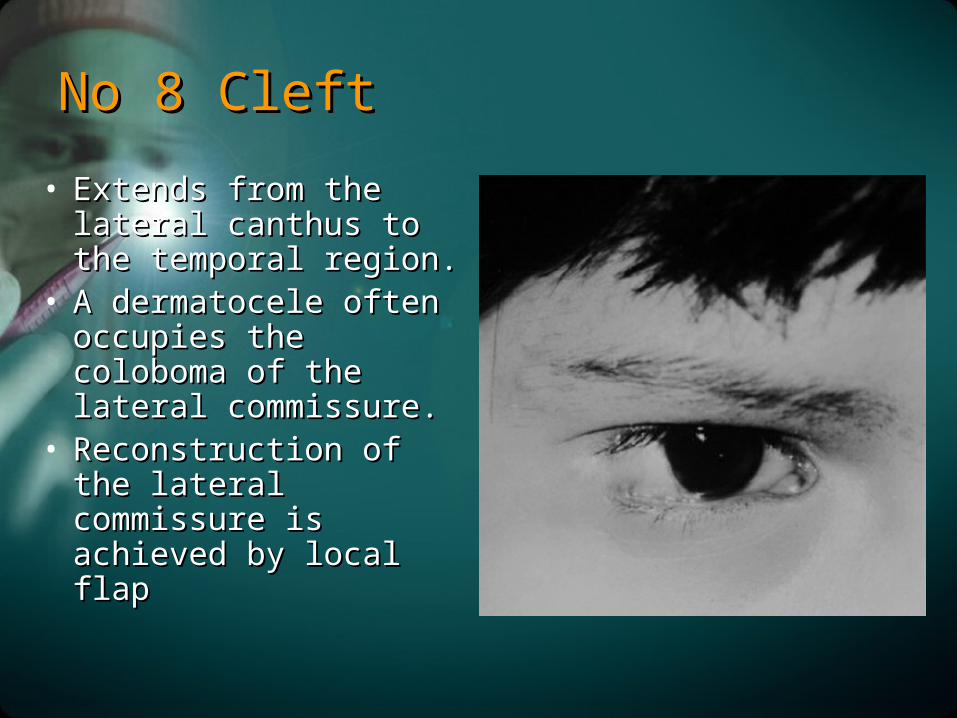
No 8 CleftNo 8 Cleft
• Extends from the lateral Extends from the lateral canthus to the temporal canthus to the temporal region.region.
• A dermatocele often A dermatocele often occupies the coloboma of occupies the coloboma of the lateral commissure.the lateral commissure.
• Reconstruction of the Reconstruction of the lateral commissure is lateral commissure is achieved by local flapachieved by local flap
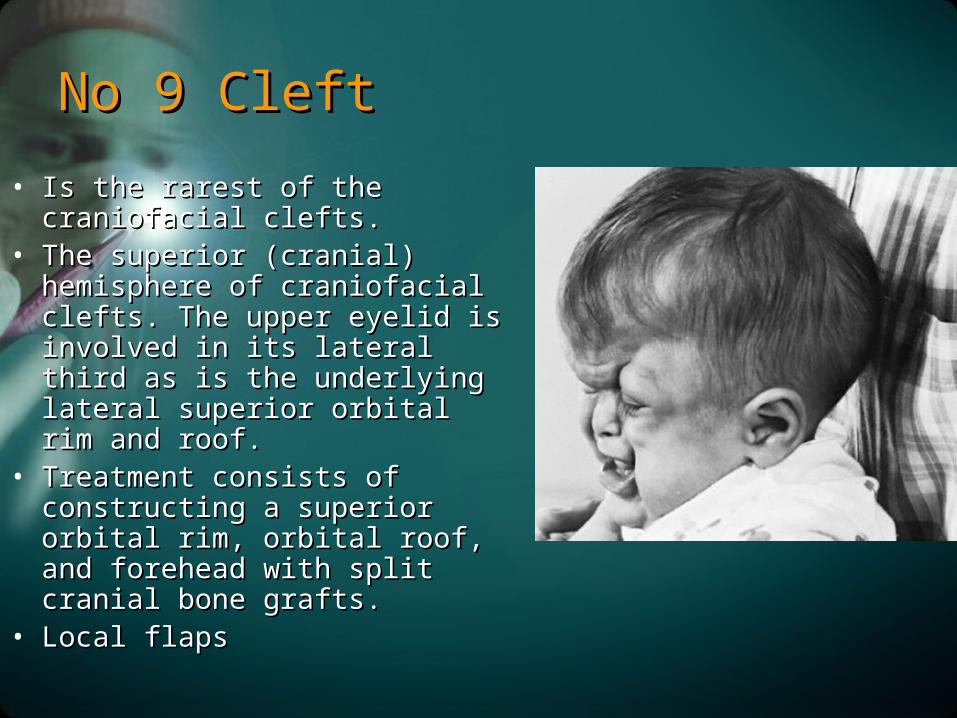
No 9 CleftNo 9 Cleft
• Is the rarest of the craniofacial Is the rarest of the craniofacial clefts.clefts.
• The superior (cranial) hemisphere of The superior (cranial) hemisphere of craniofacial clefts. The upper eyelid craniofacial clefts. The upper eyelid is involved in its lateral third as is is involved in its lateral third as is the underlying lateral superior the underlying lateral superior orbital rim and roof.orbital rim and roof.
• Treatment consists of constructing a Treatment consists of constructing a superior orbital rim, orbital roof, superior orbital rim, orbital roof, and forehead with split cranial bone and forehead with split cranial bone grafts.grafts.
• Local flapsLocal flaps
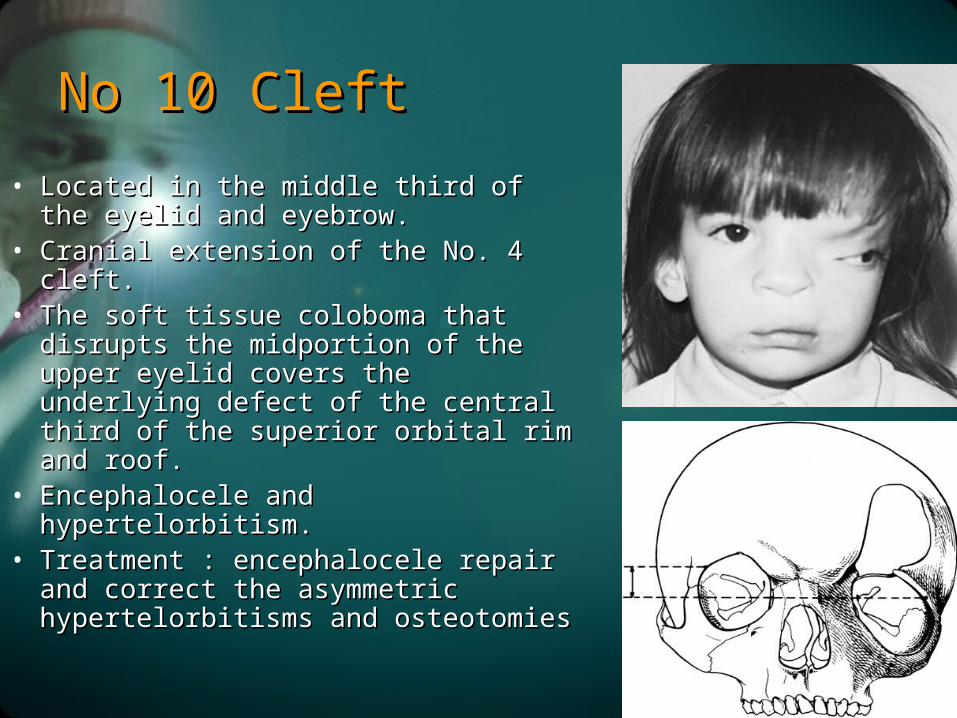
No 10 CleftNo 10 Cleft
• Located in the middle third of the eyelid Located in the middle third of the eyelid and eyebrow.and eyebrow.
• Cranial extension of the No. 4 cleft. Cranial extension of the No. 4 cleft. • The soft tissue coloboma that disrupts the The soft tissue coloboma that disrupts the
midportion of the upper eyelid covers the midportion of the upper eyelid covers the underlying defect of the central third of underlying defect of the central third of the superior orbital rim and roof.the superior orbital rim and roof.
• Encephalocele and hypertelorbitism.Encephalocele and hypertelorbitism.• Treatment : encephalocele repair and Treatment : encephalocele repair and
correct the asymmetric hypertelorbitisms correct the asymmetric hypertelorbitisms and osteotomiesand osteotomies
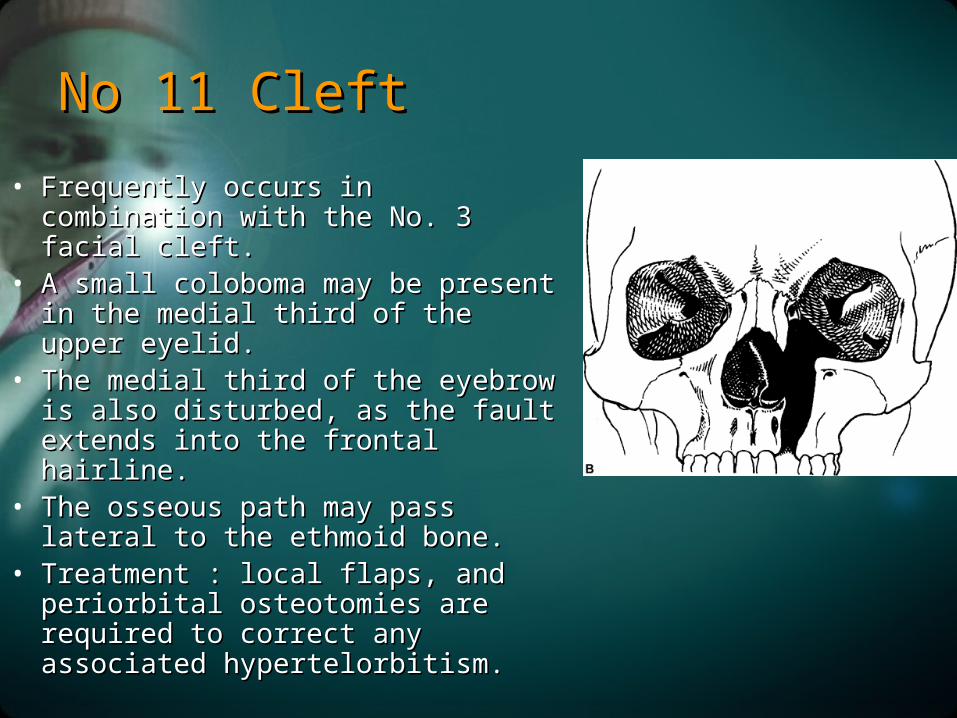
No 11 CleftNo 11 Cleft
• Frequently occurs in combination with Frequently occurs in combination with the No. 3 facial cleft.the No. 3 facial cleft.
• A small coloboma may be present in the A small coloboma may be present in the medial third of the upper eyelid.medial third of the upper eyelid.
• The medial third of the eyebrow is also The medial third of the eyebrow is also disturbed, as the fault extends into the disturbed, as the fault extends into the frontal hairline. frontal hairline.
• The osseous path may pass lateral to the The osseous path may pass lateral to the ethmoid bone.ethmoid bone.
• Treatment : local flaps, and periorbital Treatment : local flaps, and periorbital osteotomies are required to correct any osteotomies are required to correct any associated hypertelorbitism. associated hypertelorbitism.
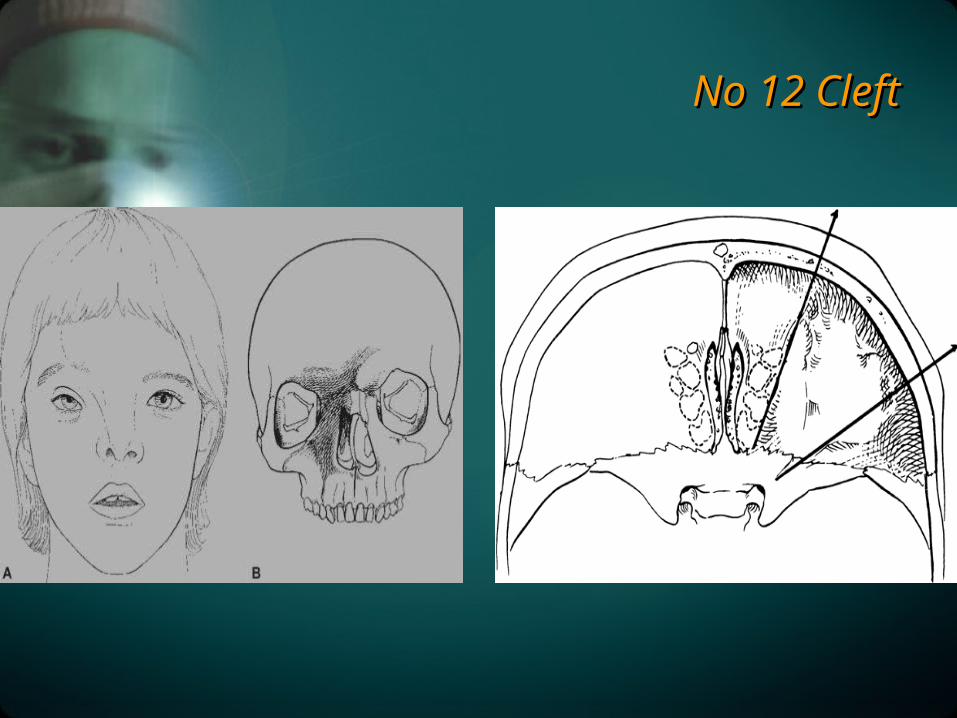
No 12 CleftNo 12 Cleft
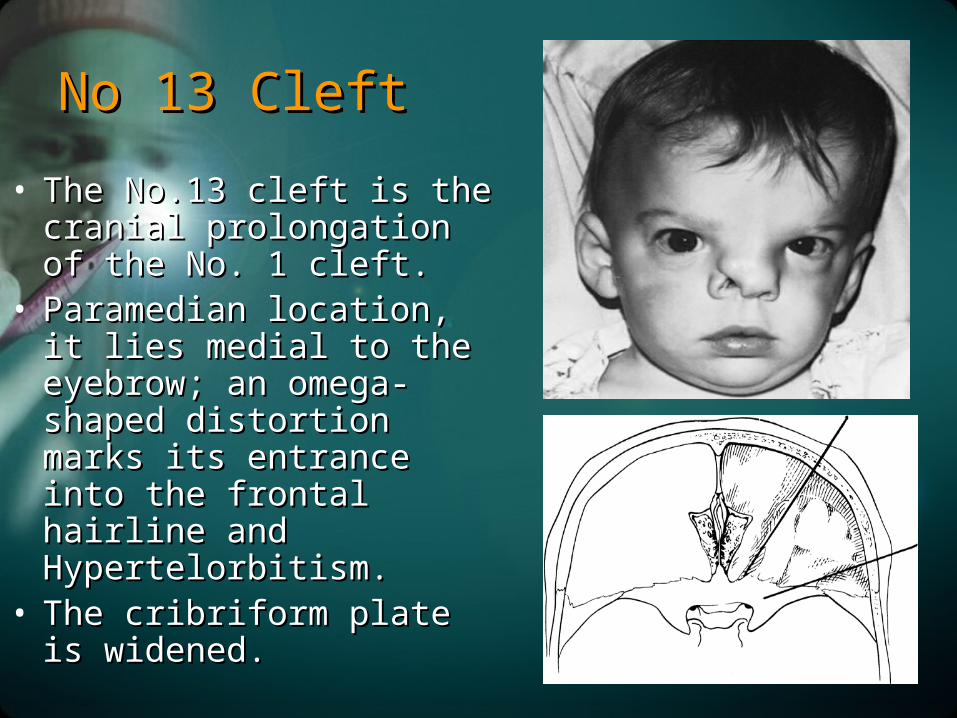
No 13 CleftNo 13 Cleft
• The No.13 cleft is the cranial The No.13 cleft is the cranial prolongation of the No. 1 prolongation of the No. 1 cleft.cleft.
• Paramedian location, it lies Paramedian location, it lies medial to the eyebrow; an medial to the eyebrow; an omega-shaped distortion omega-shaped distortion marks its entrance into the marks its entrance into the frontal hairline and frontal hairline and Hypertelorbitism. Hypertelorbitism.
• The cribriform plate is The cribriform plate is widened. widened.
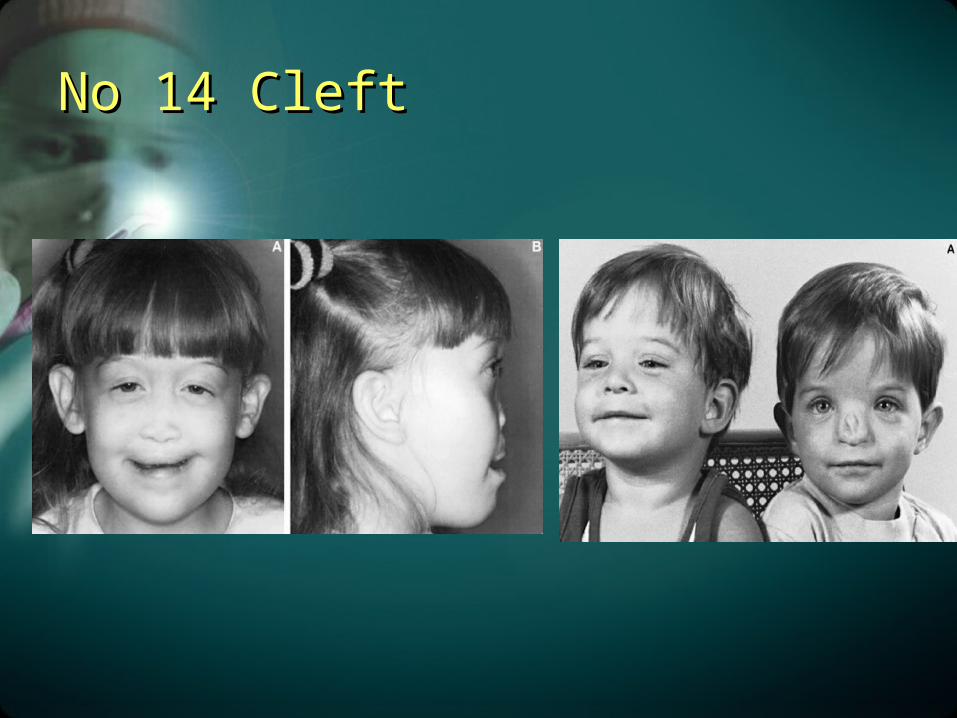
No 14 CleftNo 14 Cleft

Terima Kasih