copd
DESCRIPTION
power point copdTRANSCRIPT
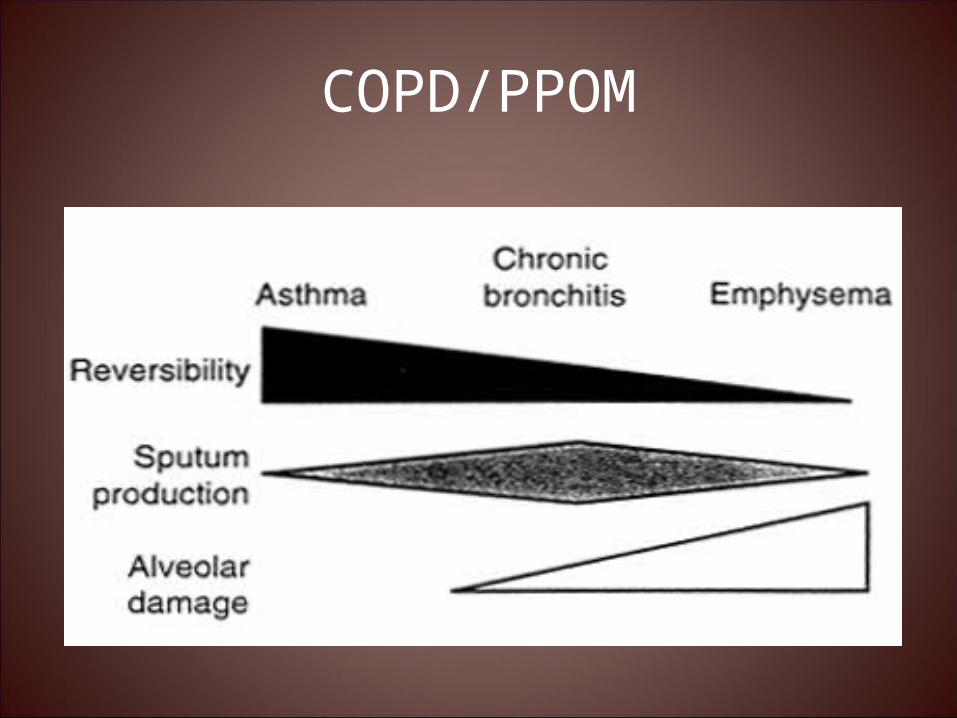
COPDPPOM
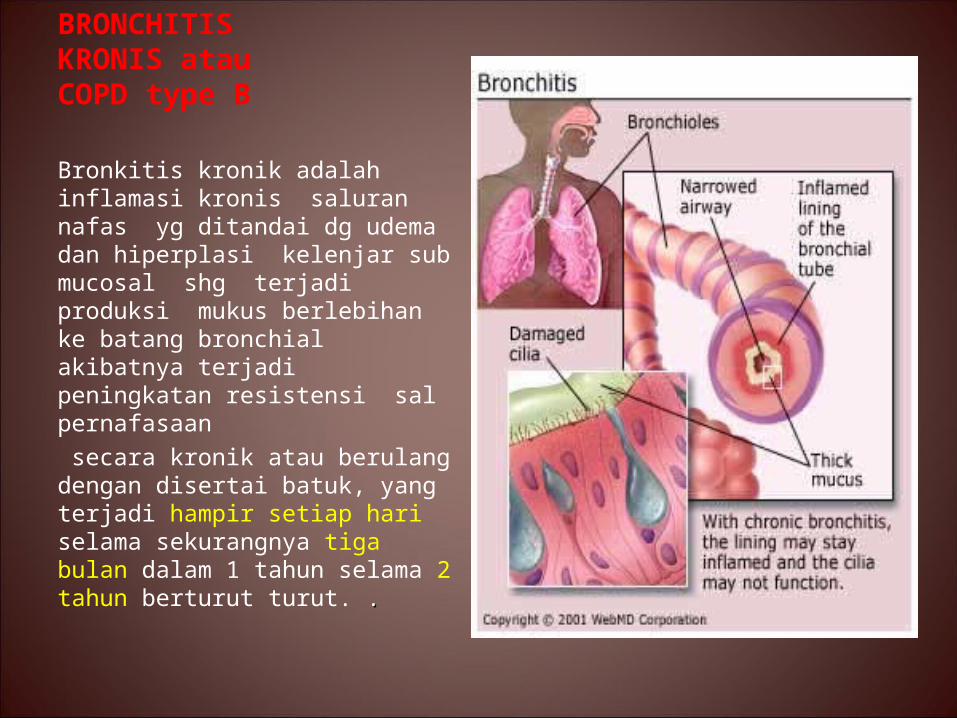
BRONCHITIS KRONIS atau COPD type B
Bronkitis kronik adalah inflamasi kronis saluran nafas yg ditandai dg udema dan hiperplasi kelenjar sub mucosal shg terjadi produksi mukus berlebihan ke batang bronchial akibatnya terjadi peningkatan resistensi sal pernafasaan secara kronik atau berulang dengan disertai batuk yang terjadi hampir setiap hari selama sekurangnya tiga bulan dalam 1 tahun selama 2 tahun berturut turut
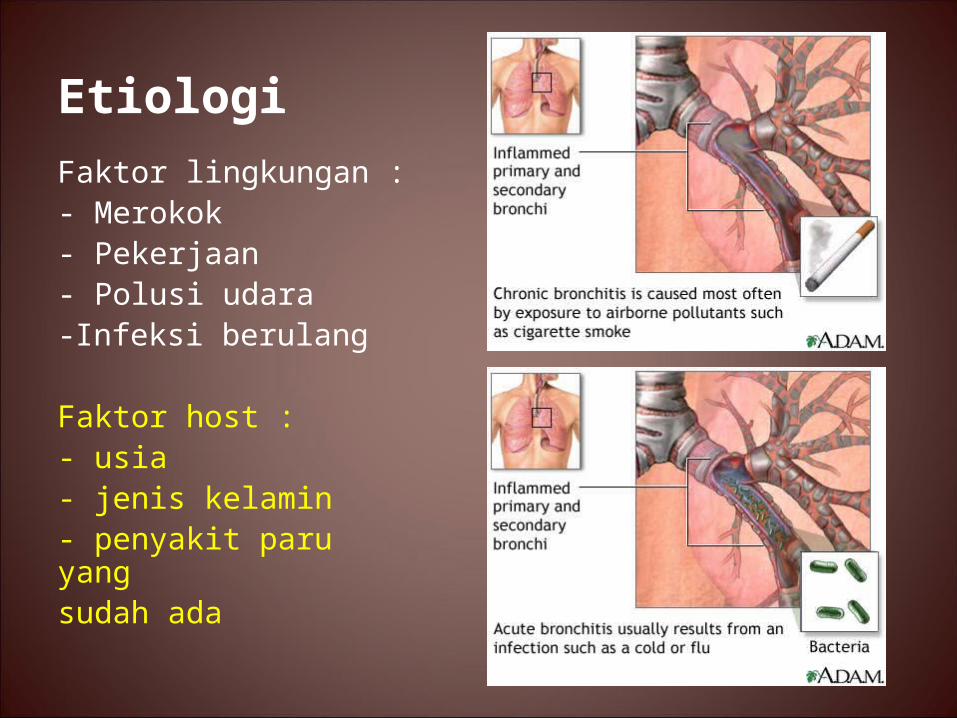
Etiologi Faktor lingkungan - Merokok- Pekerjaan- Polusi udara-Infeksi berulang
Faktor host - usia- jenis kelamin- penyakit paru yangsudah ada
4
5
CHRONIC BRONCHITIS
bull Chronic bronchitis is defined as persistent cough with sputum production for at least 3 months in at least two consecutive
years
bull The most important cause of chronic bronchitis is recurrent irritation of the bronchial mucosa by inhaled substances as
occurs in cigarette smokers
bull The pathological hallmarks of chronic bronchitis are congestion of the bronchial mucosa and a prominent increase in the
number and size of the bronchial mucus glands Copious mucus may be seen within airway lumens The terminal airways are
most susceptible to obstruction by mucus
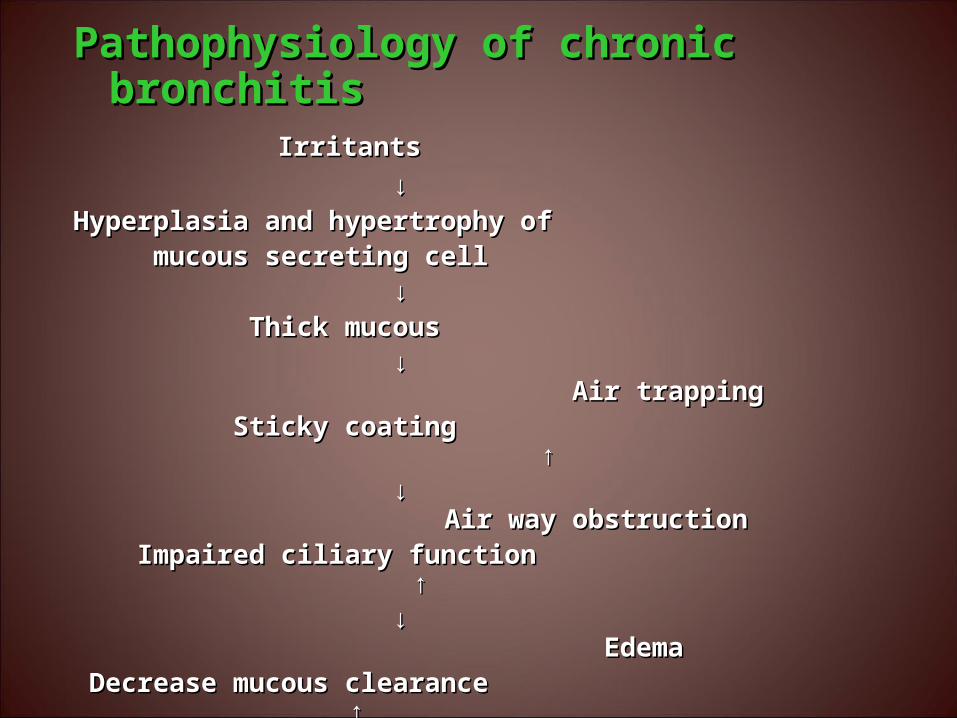
Pathophysiology of chronic bronchitisPathophysiology of chronic bronchitis IrritantsIrritants darr darrHyperplasia and hypertrophy of Hyperplasia and hypertrophy of mucous secreting cellmucous secreting cell darr darr Thick mucousThick mucous darr darr Air trappingAir trapping Sticky coating uarrSticky coating uarr darr darr Air way obstructionAir way obstruction Impaired ciliary function uarrImpaired ciliary function uarr darr darr EdemaEdema Decrease mucous clearance uarrDecrease mucous clearance uarr darr darr Bronchial wall thickness and Bronchial wall thickness and Lung defense system compromise inflammationLung defense system compromise inflammation darr uarr darr uarrVulnerable for infection rarr More infection more mucusVulnerable for infection rarr More infection more mucus
VENTILATION COST
bull In COPD work of breathing is greater for any given level of ventilation than normal
VENTILATIONVENTILATION
WORK OF WORK OF BREATHINGBREATHING
NORMAL COPDNORMAL COPD
SEVERE COPDSEVERE COPD
MODERATE COPDMODERATE COPDThe cost of work at a The cost of work at a given ventilation for given ventilation for lsquonormalrsquo and COPD lsquonormalrsquo and COPD patients (ACSM patients (ACSM 1998)1998)
bull Damage to the epithelium impairs the mucociliary response that clears bacteria and mucus Inflammation and secretions provide the
obstructive component of chronic bronchitis
bull In contrast to emphysema chronic bronchitis is associated with a relatively undamaged
pulmonary capillary bed
Emphysema or type A COPD
DefinitionDefinition Abnormal permanent Abnormal permanent
enlargement of air spaces enlargement of air spaces distal to the terminal distal to the terminal bronchioles accompanied bronchioles accompanied by the destruction of the by the destruction of the walls and without obvious walls and without obvious fibrosisfibrosis
Emphysema is characterized Emphysema is characterized by loss of elasticity of the by loss of elasticity of the lung and abnormal lung and abnormal permanent enlargement of permanent enlargement of air spaces with destruction air spaces with destruction of the alveolar walls and of the alveolar walls and capillary beds capillary beds
EtiologiEmphysemaSmoking the primary risk factorLong-term smoking is responsible for 80-90 of casesProlonged exposures to harmful particles and gases from
passive smoke Industrial smoke Chemical gases vapors mists amp fumesDusts from grains minerals amp other materials
Alpha 1-antitrypsin deficiency gtgtemphysemaGeneticsBronchitisAsthma
Pathophysiology
Exposure to inhaled noxious particles amp gases inflammation imbalance of proteinases and anti-proteinases
Dilatation amp destruction +mucus secretion
FIG 1 Inflammatory mechanisms in COPD Cigarette smoke (and other irritants) activate macrophages in the respiratory tract that release neutrophil chemotactic factors including IL-8 and LTB4 These cells then release proteases that break down connective tissue in the lung parenchyma resulting in emphysema and also stimulate mucus hypersecretion These enzymes are normally counteracted by protease inhibitors including 1-antitrypsin SLPI and TIMP Cytotoxic T cells (CD8) may also be recruited and may be involved in alveolar wall destruction Fibroblasts may be activated by growthfactors releases from macrophages and epithelial cells CTG connective tissue growth factor COB chronic obstructive bronchiolitis
Pathophysiology
bull Affects alveolar membranendash Destruction of alveolar wallndash Loss of elastic recoilndash Over distended alveoli
bull Over distended alveolindash Damage to adjacent
pulmonary capillariesndash dead spacendash Impaired passive expiration
Impaired gas exchange
bull Impaired gas exchangendash impaired expiration
bull CO2 bull Hypercapniabull Respiratory acidosis
bull Damaged pulmonary capillary bedndash pulmonary pressure ndash work load for right ventricle
ndash Right side heart failure (due
to respiratory pressure) ndash Cor Pulmonale
16
SYMPTOMScough
sputumdyspnea
EXPOSURE TO RISKFACTORS
tobaccooccupation
indooroutdoor pollution
SPIROMETRY
Diagnosis of COPD
GAS DARAH ARTERILABORATORY TESTCHEST X-RAY
Spirometry Normal and COPDSpirometry Normal and COPD
0
5
1
4
2
3
Lite
r
1 65432
FVC
FVC
FEV1
FEV1
Normal
COPD
39005200
23504150 80
60 NormalCOPD
FVCFEV1 FVCFEV1
Seconds
Normally the left side of the heart produces a higher level of blood pressure in order to pump blood to the body the right side pumps blood through the lungs under much lower pressure Any condition that leads to prolonged high blood pressure in the arteries or veins of the lungs (called pulmonary hypertension) will be poorly tolerated by the right ventricle of the heart When this right ventricle fails or is unable toproperly pump against these abnormally high pressures this is called cor pulmonale
Prognosis
bull Indikator umur dan keparahanbull Jika ada hipoksia dan cor pulmonale
prognosis jelekbull Dyspnea obstruksi berat saluran nafas FEV1 lt 075 L (20) 1048774 angka kematian meningkat
50 pasien berisiko meninggal dalam waktu 5 tahun
Tujuan Terapi
bull Memperbaiki keadaan obstruksi saluran nafasbull Mencegah dan mengatasi eksaserbasi akutbull Menurunkan progresivitas penyakitbull Meningkatkan keadaan fisik dan psikisbull Menurunkan jumlah hari tidak masuk kerjabull Menurunkan lama tinggal di RSbull Menurunkan angka kematian
NON FARMAKOLOGI
bull Menghentikan kebiasaan merokokbull Rehabilitasi paru-paru secara komprehensif
dengan OR dan latihan pernafasanbull Perbaikan nutrisibull Tidak ada obat yang dapat menunda
memburuknya fungsi paru jika pasien tetap merokok
bull Kortikosteroid 1048774 benefit is very limited laporan tentang efektivitasnya masih bervariasi kecuali jika pasien juga memiliki riwayat asma
bull 1048774 Oksigen 1048774 untuk pasien hipoksemia cor pulmonale Digunakan jika baseline PaO2 turun sampai lt 55 mmHg
bull 1048774 Antibiotik 1048774 digunakan bila ada tanda infeksi bukan untuk maintenance therapy
bull 1048774 Vaksinasi 1048774 direkomendasikan untuk high-risk patients vaksin pneumococcus (tiap 5-10 th) dan vaksin influenza (tiap tahun)
bull 1048774 α1-proteinase inhibitor 1048774 utk pasien yang defisiensi α1- antitripsin 1048774 digunakan per minggu masih mahal 1048774 contoh Prolastin
Tahap terapi pada PPOK yang stabil
bull Tahap 1 Ipratropium bromida (MDI) atau nebulizer 2-6 puff 4 x sehari tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (mulut kering amp rasa pahit) jika hasil trial perbaikan FEV1 lt 20 1048774 step 2
bull Tahap 2 Tambahkan β-agonis MDI atau nebulizer tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (takikardi tremor) 1048774 jika tidak ada perkembangan hentikan β-agonis jika ada perbaikan tapi kecil 1048774 step 3
Terapi antibiotika
bull 1048774 Berdasarkan evidence terbaru yang tersedia antibiotika harus diberikan pada pasien-pasien PPOK yang
bull 1048774 Pasien dengan eksaserbasi akut dengan 3 tanda utama yaitu increased dyspnea increased sputum volume increased sputum purulence (Evidence B) atau
bull 1048774 Pasien dengan eksaserbasi akut dengan 2 tanda utama jika peningkatan purulensi sputum merupakan salah satunya (Evidence C)
bull 1048774 Pasien dengan eksaserbasi parah yang membutuhkan ventilasi mekanik baik invasif maupun non-infvasif (Evidence B)
bull Tahap 3 Tambah teofilinmulai dari 400 mghari dlm bentuk sustained released sesuaikan dosis setiap interval 3 hari untuk menjaga serum level antara 10-15 μgml pantau ESO takikardi tremor nervous efek GI jika tidak ada perbaikan 1048774 hentikan teofilin dan 1048774go to step 4
bull Tahap 4 Coba dengan kortikosteroid prednison 30-40 mghari selama 2-4 minggu cek dengan spirometer (perbaikan ge 20) titrasi dosis ke dosis efektif terkecil (lt 10 μg sehari) pertimbangkan penggunaan kortikosteroid inhalasi 1048774 jika pasien tidak berespon baik 1048774 kembali ke steroid oral
Key points
bull 1048774PPOK adalah penyakit yang sebenarnya secara potensial dapat dicegah 1048774 stop smoking
bull 1048774Sekali PPOK terjadi 1048774 penderita akan memerlukan terapi yang kompleks 1048774 yang efikasinya masih diperdebatkan para ahli
bull 1048774Penyakit ini bersifat progresif dan ireversibel1048774 berbiaya besar baik baik personal maupun masyarakat
Difference between bronchitis and Difference between bronchitis and emphysemaemphysema
Productive cough
bronchitis
Classic sign
emphysema
Late in common with infection
Dyspnea Late in course CommonWheezing Intermittent MildHO smoking Common CommonBarrel chest Occasionally classicProlonged expiration Always present Always presentCyanosis Common UncommonChronic hypoventilation
Common Late in course
Ploycythemia Common Late in course
- COPDPPOM
- BRONCHITIS KRONIS atau COPD type B
- Etiologi
- Slide 4
- Slide 5
- CHRONIC BRONCHITIS
- Slide 7
- Slide 8
- VENTILATION COST
- Slide 10
- Emphysema or type A COPD
- Etiologi Emphysema
- Pathophysiology
- Slide 14
- Pathophysiology
- Slide 16
- Slide 17
- Slide 18
- Prognosis
- Tujuan Terapi
- NON FARMAKOLOGI
- Slide 22
- Slide 23
- Tahap terapi pada PPOK yang stabil
- Terapi antibiotika
- Slide 26
- Key points
- Difference between bronchitis and emphysema
-
BRONCHITIS KRONIS atau COPD type B
Bronkitis kronik adalah inflamasi kronis saluran nafas yg ditandai dg udema dan hiperplasi kelenjar sub mucosal shg terjadi produksi mukus berlebihan ke batang bronchial akibatnya terjadi peningkatan resistensi sal pernafasaan secara kronik atau berulang dengan disertai batuk yang terjadi hampir setiap hari selama sekurangnya tiga bulan dalam 1 tahun selama 2 tahun berturut turut
Etiologi Faktor lingkungan - Merokok- Pekerjaan- Polusi udara-Infeksi berulang
Faktor host - usia- jenis kelamin- penyakit paru yangsudah ada
4
5
CHRONIC BRONCHITIS
bull Chronic bronchitis is defined as persistent cough with sputum production for at least 3 months in at least two consecutive
years
bull The most important cause of chronic bronchitis is recurrent irritation of the bronchial mucosa by inhaled substances as
occurs in cigarette smokers
bull The pathological hallmarks of chronic bronchitis are congestion of the bronchial mucosa and a prominent increase in the
number and size of the bronchial mucus glands Copious mucus may be seen within airway lumens The terminal airways are
most susceptible to obstruction by mucus
Pathophysiology of chronic bronchitisPathophysiology of chronic bronchitis IrritantsIrritants darr darrHyperplasia and hypertrophy of Hyperplasia and hypertrophy of mucous secreting cellmucous secreting cell darr darr Thick mucousThick mucous darr darr Air trappingAir trapping Sticky coating uarrSticky coating uarr darr darr Air way obstructionAir way obstruction Impaired ciliary function uarrImpaired ciliary function uarr darr darr EdemaEdema Decrease mucous clearance uarrDecrease mucous clearance uarr darr darr Bronchial wall thickness and Bronchial wall thickness and Lung defense system compromise inflammationLung defense system compromise inflammation darr uarr darr uarrVulnerable for infection rarr More infection more mucusVulnerable for infection rarr More infection more mucus
VENTILATION COST
bull In COPD work of breathing is greater for any given level of ventilation than normal
VENTILATIONVENTILATION
WORK OF WORK OF BREATHINGBREATHING
NORMAL COPDNORMAL COPD
SEVERE COPDSEVERE COPD
MODERATE COPDMODERATE COPDThe cost of work at a The cost of work at a given ventilation for given ventilation for lsquonormalrsquo and COPD lsquonormalrsquo and COPD patients (ACSM patients (ACSM 1998)1998)
bull Damage to the epithelium impairs the mucociliary response that clears bacteria and mucus Inflammation and secretions provide the
obstructive component of chronic bronchitis
bull In contrast to emphysema chronic bronchitis is associated with a relatively undamaged
pulmonary capillary bed
Emphysema or type A COPD
DefinitionDefinition Abnormal permanent Abnormal permanent
enlargement of air spaces enlargement of air spaces distal to the terminal distal to the terminal bronchioles accompanied bronchioles accompanied by the destruction of the by the destruction of the walls and without obvious walls and without obvious fibrosisfibrosis
Emphysema is characterized Emphysema is characterized by loss of elasticity of the by loss of elasticity of the lung and abnormal lung and abnormal permanent enlargement of permanent enlargement of air spaces with destruction air spaces with destruction of the alveolar walls and of the alveolar walls and capillary beds capillary beds
EtiologiEmphysemaSmoking the primary risk factorLong-term smoking is responsible for 80-90 of casesProlonged exposures to harmful particles and gases from
passive smoke Industrial smoke Chemical gases vapors mists amp fumesDusts from grains minerals amp other materials
Alpha 1-antitrypsin deficiency gtgtemphysemaGeneticsBronchitisAsthma
Pathophysiology
Exposure to inhaled noxious particles amp gases inflammation imbalance of proteinases and anti-proteinases
Dilatation amp destruction +mucus secretion
FIG 1 Inflammatory mechanisms in COPD Cigarette smoke (and other irritants) activate macrophages in the respiratory tract that release neutrophil chemotactic factors including IL-8 and LTB4 These cells then release proteases that break down connective tissue in the lung parenchyma resulting in emphysema and also stimulate mucus hypersecretion These enzymes are normally counteracted by protease inhibitors including 1-antitrypsin SLPI and TIMP Cytotoxic T cells (CD8) may also be recruited and may be involved in alveolar wall destruction Fibroblasts may be activated by growthfactors releases from macrophages and epithelial cells CTG connective tissue growth factor COB chronic obstructive bronchiolitis
Pathophysiology
bull Affects alveolar membranendash Destruction of alveolar wallndash Loss of elastic recoilndash Over distended alveoli
bull Over distended alveolindash Damage to adjacent
pulmonary capillariesndash dead spacendash Impaired passive expiration
Impaired gas exchange
bull Impaired gas exchangendash impaired expiration
bull CO2 bull Hypercapniabull Respiratory acidosis
bull Damaged pulmonary capillary bedndash pulmonary pressure ndash work load for right ventricle
ndash Right side heart failure (due
to respiratory pressure) ndash Cor Pulmonale
16
SYMPTOMScough
sputumdyspnea
EXPOSURE TO RISKFACTORS
tobaccooccupation
indooroutdoor pollution
SPIROMETRY
Diagnosis of COPD
GAS DARAH ARTERILABORATORY TESTCHEST X-RAY
Spirometry Normal and COPDSpirometry Normal and COPD
0
5
1
4
2
3
Lite
r
1 65432
FVC
FVC
FEV1
FEV1
Normal
COPD
39005200
23504150 80
60 NormalCOPD
FVCFEV1 FVCFEV1
Seconds
Normally the left side of the heart produces a higher level of blood pressure in order to pump blood to the body the right side pumps blood through the lungs under much lower pressure Any condition that leads to prolonged high blood pressure in the arteries or veins of the lungs (called pulmonary hypertension) will be poorly tolerated by the right ventricle of the heart When this right ventricle fails or is unable toproperly pump against these abnormally high pressures this is called cor pulmonale
Prognosis
bull Indikator umur dan keparahanbull Jika ada hipoksia dan cor pulmonale
prognosis jelekbull Dyspnea obstruksi berat saluran nafas FEV1 lt 075 L (20) 1048774 angka kematian meningkat
50 pasien berisiko meninggal dalam waktu 5 tahun
Tujuan Terapi
bull Memperbaiki keadaan obstruksi saluran nafasbull Mencegah dan mengatasi eksaserbasi akutbull Menurunkan progresivitas penyakitbull Meningkatkan keadaan fisik dan psikisbull Menurunkan jumlah hari tidak masuk kerjabull Menurunkan lama tinggal di RSbull Menurunkan angka kematian
NON FARMAKOLOGI
bull Menghentikan kebiasaan merokokbull Rehabilitasi paru-paru secara komprehensif
dengan OR dan latihan pernafasanbull Perbaikan nutrisibull Tidak ada obat yang dapat menunda
memburuknya fungsi paru jika pasien tetap merokok
bull Kortikosteroid 1048774 benefit is very limited laporan tentang efektivitasnya masih bervariasi kecuali jika pasien juga memiliki riwayat asma
bull 1048774 Oksigen 1048774 untuk pasien hipoksemia cor pulmonale Digunakan jika baseline PaO2 turun sampai lt 55 mmHg
bull 1048774 Antibiotik 1048774 digunakan bila ada tanda infeksi bukan untuk maintenance therapy
bull 1048774 Vaksinasi 1048774 direkomendasikan untuk high-risk patients vaksin pneumococcus (tiap 5-10 th) dan vaksin influenza (tiap tahun)
bull 1048774 α1-proteinase inhibitor 1048774 utk pasien yang defisiensi α1- antitripsin 1048774 digunakan per minggu masih mahal 1048774 contoh Prolastin
Tahap terapi pada PPOK yang stabil
bull Tahap 1 Ipratropium bromida (MDI) atau nebulizer 2-6 puff 4 x sehari tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (mulut kering amp rasa pahit) jika hasil trial perbaikan FEV1 lt 20 1048774 step 2
bull Tahap 2 Tambahkan β-agonis MDI atau nebulizer tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (takikardi tremor) 1048774 jika tidak ada perkembangan hentikan β-agonis jika ada perbaikan tapi kecil 1048774 step 3
Terapi antibiotika
bull 1048774 Berdasarkan evidence terbaru yang tersedia antibiotika harus diberikan pada pasien-pasien PPOK yang
bull 1048774 Pasien dengan eksaserbasi akut dengan 3 tanda utama yaitu increased dyspnea increased sputum volume increased sputum purulence (Evidence B) atau
bull 1048774 Pasien dengan eksaserbasi akut dengan 2 tanda utama jika peningkatan purulensi sputum merupakan salah satunya (Evidence C)
bull 1048774 Pasien dengan eksaserbasi parah yang membutuhkan ventilasi mekanik baik invasif maupun non-infvasif (Evidence B)
bull Tahap 3 Tambah teofilinmulai dari 400 mghari dlm bentuk sustained released sesuaikan dosis setiap interval 3 hari untuk menjaga serum level antara 10-15 μgml pantau ESO takikardi tremor nervous efek GI jika tidak ada perbaikan 1048774 hentikan teofilin dan 1048774go to step 4
bull Tahap 4 Coba dengan kortikosteroid prednison 30-40 mghari selama 2-4 minggu cek dengan spirometer (perbaikan ge 20) titrasi dosis ke dosis efektif terkecil (lt 10 μg sehari) pertimbangkan penggunaan kortikosteroid inhalasi 1048774 jika pasien tidak berespon baik 1048774 kembali ke steroid oral
Key points
bull 1048774PPOK adalah penyakit yang sebenarnya secara potensial dapat dicegah 1048774 stop smoking
bull 1048774Sekali PPOK terjadi 1048774 penderita akan memerlukan terapi yang kompleks 1048774 yang efikasinya masih diperdebatkan para ahli
bull 1048774Penyakit ini bersifat progresif dan ireversibel1048774 berbiaya besar baik baik personal maupun masyarakat
Difference between bronchitis and Difference between bronchitis and emphysemaemphysema
Productive cough
bronchitis
Classic sign
emphysema
Late in common with infection
Dyspnea Late in course CommonWheezing Intermittent MildHO smoking Common CommonBarrel chest Occasionally classicProlonged expiration Always present Always presentCyanosis Common UncommonChronic hypoventilation
Common Late in course
Ploycythemia Common Late in course
- COPDPPOM
- BRONCHITIS KRONIS atau COPD type B
- Etiologi
- Slide 4
- Slide 5
- CHRONIC BRONCHITIS
- Slide 7
- Slide 8
- VENTILATION COST
- Slide 10
- Emphysema or type A COPD
- Etiologi Emphysema
- Pathophysiology
- Slide 14
- Pathophysiology
- Slide 16
- Slide 17
- Slide 18
- Prognosis
- Tujuan Terapi
- NON FARMAKOLOGI
- Slide 22
- Slide 23
- Tahap terapi pada PPOK yang stabil
- Terapi antibiotika
- Slide 26
- Key points
- Difference between bronchitis and emphysema
-
Etiologi Faktor lingkungan - Merokok- Pekerjaan- Polusi udara-Infeksi berulang
Faktor host - usia- jenis kelamin- penyakit paru yangsudah ada
4
5
CHRONIC BRONCHITIS
bull Chronic bronchitis is defined as persistent cough with sputum production for at least 3 months in at least two consecutive
years
bull The most important cause of chronic bronchitis is recurrent irritation of the bronchial mucosa by inhaled substances as
occurs in cigarette smokers
bull The pathological hallmarks of chronic bronchitis are congestion of the bronchial mucosa and a prominent increase in the
number and size of the bronchial mucus glands Copious mucus may be seen within airway lumens The terminal airways are
most susceptible to obstruction by mucus
Pathophysiology of chronic bronchitisPathophysiology of chronic bronchitis IrritantsIrritants darr darrHyperplasia and hypertrophy of Hyperplasia and hypertrophy of mucous secreting cellmucous secreting cell darr darr Thick mucousThick mucous darr darr Air trappingAir trapping Sticky coating uarrSticky coating uarr darr darr Air way obstructionAir way obstruction Impaired ciliary function uarrImpaired ciliary function uarr darr darr EdemaEdema Decrease mucous clearance uarrDecrease mucous clearance uarr darr darr Bronchial wall thickness and Bronchial wall thickness and Lung defense system compromise inflammationLung defense system compromise inflammation darr uarr darr uarrVulnerable for infection rarr More infection more mucusVulnerable for infection rarr More infection more mucus
VENTILATION COST
bull In COPD work of breathing is greater for any given level of ventilation than normal
VENTILATIONVENTILATION
WORK OF WORK OF BREATHINGBREATHING
NORMAL COPDNORMAL COPD
SEVERE COPDSEVERE COPD
MODERATE COPDMODERATE COPDThe cost of work at a The cost of work at a given ventilation for given ventilation for lsquonormalrsquo and COPD lsquonormalrsquo and COPD patients (ACSM patients (ACSM 1998)1998)
bull Damage to the epithelium impairs the mucociliary response that clears bacteria and mucus Inflammation and secretions provide the
obstructive component of chronic bronchitis
bull In contrast to emphysema chronic bronchitis is associated with a relatively undamaged
pulmonary capillary bed
Emphysema or type A COPD
DefinitionDefinition Abnormal permanent Abnormal permanent
enlargement of air spaces enlargement of air spaces distal to the terminal distal to the terminal bronchioles accompanied bronchioles accompanied by the destruction of the by the destruction of the walls and without obvious walls and without obvious fibrosisfibrosis
Emphysema is characterized Emphysema is characterized by loss of elasticity of the by loss of elasticity of the lung and abnormal lung and abnormal permanent enlargement of permanent enlargement of air spaces with destruction air spaces with destruction of the alveolar walls and of the alveolar walls and capillary beds capillary beds
EtiologiEmphysemaSmoking the primary risk factorLong-term smoking is responsible for 80-90 of casesProlonged exposures to harmful particles and gases from
passive smoke Industrial smoke Chemical gases vapors mists amp fumesDusts from grains minerals amp other materials
Alpha 1-antitrypsin deficiency gtgtemphysemaGeneticsBronchitisAsthma
Pathophysiology
Exposure to inhaled noxious particles amp gases inflammation imbalance of proteinases and anti-proteinases
Dilatation amp destruction +mucus secretion
FIG 1 Inflammatory mechanisms in COPD Cigarette smoke (and other irritants) activate macrophages in the respiratory tract that release neutrophil chemotactic factors including IL-8 and LTB4 These cells then release proteases that break down connective tissue in the lung parenchyma resulting in emphysema and also stimulate mucus hypersecretion These enzymes are normally counteracted by protease inhibitors including 1-antitrypsin SLPI and TIMP Cytotoxic T cells (CD8) may also be recruited and may be involved in alveolar wall destruction Fibroblasts may be activated by growthfactors releases from macrophages and epithelial cells CTG connective tissue growth factor COB chronic obstructive bronchiolitis
Pathophysiology
bull Affects alveolar membranendash Destruction of alveolar wallndash Loss of elastic recoilndash Over distended alveoli
bull Over distended alveolindash Damage to adjacent
pulmonary capillariesndash dead spacendash Impaired passive expiration
Impaired gas exchange
bull Impaired gas exchangendash impaired expiration
bull CO2 bull Hypercapniabull Respiratory acidosis
bull Damaged pulmonary capillary bedndash pulmonary pressure ndash work load for right ventricle
ndash Right side heart failure (due
to respiratory pressure) ndash Cor Pulmonale
16
SYMPTOMScough
sputumdyspnea
EXPOSURE TO RISKFACTORS
tobaccooccupation
indooroutdoor pollution
SPIROMETRY
Diagnosis of COPD
GAS DARAH ARTERILABORATORY TESTCHEST X-RAY
Spirometry Normal and COPDSpirometry Normal and COPD
0
5
1
4
2
3
Lite
r
1 65432
FVC
FVC
FEV1
FEV1
Normal
COPD
39005200
23504150 80
60 NormalCOPD
FVCFEV1 FVCFEV1
Seconds
Normally the left side of the heart produces a higher level of blood pressure in order to pump blood to the body the right side pumps blood through the lungs under much lower pressure Any condition that leads to prolonged high blood pressure in the arteries or veins of the lungs (called pulmonary hypertension) will be poorly tolerated by the right ventricle of the heart When this right ventricle fails or is unable toproperly pump against these abnormally high pressures this is called cor pulmonale
Prognosis
bull Indikator umur dan keparahanbull Jika ada hipoksia dan cor pulmonale
prognosis jelekbull Dyspnea obstruksi berat saluran nafas FEV1 lt 075 L (20) 1048774 angka kematian meningkat
50 pasien berisiko meninggal dalam waktu 5 tahun
Tujuan Terapi
bull Memperbaiki keadaan obstruksi saluran nafasbull Mencegah dan mengatasi eksaserbasi akutbull Menurunkan progresivitas penyakitbull Meningkatkan keadaan fisik dan psikisbull Menurunkan jumlah hari tidak masuk kerjabull Menurunkan lama tinggal di RSbull Menurunkan angka kematian
NON FARMAKOLOGI
bull Menghentikan kebiasaan merokokbull Rehabilitasi paru-paru secara komprehensif
dengan OR dan latihan pernafasanbull Perbaikan nutrisibull Tidak ada obat yang dapat menunda
memburuknya fungsi paru jika pasien tetap merokok
bull Kortikosteroid 1048774 benefit is very limited laporan tentang efektivitasnya masih bervariasi kecuali jika pasien juga memiliki riwayat asma
bull 1048774 Oksigen 1048774 untuk pasien hipoksemia cor pulmonale Digunakan jika baseline PaO2 turun sampai lt 55 mmHg
bull 1048774 Antibiotik 1048774 digunakan bila ada tanda infeksi bukan untuk maintenance therapy
bull 1048774 Vaksinasi 1048774 direkomendasikan untuk high-risk patients vaksin pneumococcus (tiap 5-10 th) dan vaksin influenza (tiap tahun)
bull 1048774 α1-proteinase inhibitor 1048774 utk pasien yang defisiensi α1- antitripsin 1048774 digunakan per minggu masih mahal 1048774 contoh Prolastin
Tahap terapi pada PPOK yang stabil
bull Tahap 1 Ipratropium bromida (MDI) atau nebulizer 2-6 puff 4 x sehari tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (mulut kering amp rasa pahit) jika hasil trial perbaikan FEV1 lt 20 1048774 step 2
bull Tahap 2 Tambahkan β-agonis MDI atau nebulizer tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (takikardi tremor) 1048774 jika tidak ada perkembangan hentikan β-agonis jika ada perbaikan tapi kecil 1048774 step 3
Terapi antibiotika
bull 1048774 Berdasarkan evidence terbaru yang tersedia antibiotika harus diberikan pada pasien-pasien PPOK yang
bull 1048774 Pasien dengan eksaserbasi akut dengan 3 tanda utama yaitu increased dyspnea increased sputum volume increased sputum purulence (Evidence B) atau
bull 1048774 Pasien dengan eksaserbasi akut dengan 2 tanda utama jika peningkatan purulensi sputum merupakan salah satunya (Evidence C)
bull 1048774 Pasien dengan eksaserbasi parah yang membutuhkan ventilasi mekanik baik invasif maupun non-infvasif (Evidence B)
bull Tahap 3 Tambah teofilinmulai dari 400 mghari dlm bentuk sustained released sesuaikan dosis setiap interval 3 hari untuk menjaga serum level antara 10-15 μgml pantau ESO takikardi tremor nervous efek GI jika tidak ada perbaikan 1048774 hentikan teofilin dan 1048774go to step 4
bull Tahap 4 Coba dengan kortikosteroid prednison 30-40 mghari selama 2-4 minggu cek dengan spirometer (perbaikan ge 20) titrasi dosis ke dosis efektif terkecil (lt 10 μg sehari) pertimbangkan penggunaan kortikosteroid inhalasi 1048774 jika pasien tidak berespon baik 1048774 kembali ke steroid oral
Key points
bull 1048774PPOK adalah penyakit yang sebenarnya secara potensial dapat dicegah 1048774 stop smoking
bull 1048774Sekali PPOK terjadi 1048774 penderita akan memerlukan terapi yang kompleks 1048774 yang efikasinya masih diperdebatkan para ahli
bull 1048774Penyakit ini bersifat progresif dan ireversibel1048774 berbiaya besar baik baik personal maupun masyarakat
Difference between bronchitis and Difference between bronchitis and emphysemaemphysema
Productive cough
bronchitis
Classic sign
emphysema
Late in common with infection
Dyspnea Late in course CommonWheezing Intermittent MildHO smoking Common CommonBarrel chest Occasionally classicProlonged expiration Always present Always presentCyanosis Common UncommonChronic hypoventilation
Common Late in course
Ploycythemia Common Late in course
- COPDPPOM
- BRONCHITIS KRONIS atau COPD type B
- Etiologi
- Slide 4
- Slide 5
- CHRONIC BRONCHITIS
- Slide 7
- Slide 8
- VENTILATION COST
- Slide 10
- Emphysema or type A COPD
- Etiologi Emphysema
- Pathophysiology
- Slide 14
- Pathophysiology
- Slide 16
- Slide 17
- Slide 18
- Prognosis
- Tujuan Terapi
- NON FARMAKOLOGI
- Slide 22
- Slide 23
- Tahap terapi pada PPOK yang stabil
- Terapi antibiotika
- Slide 26
- Key points
- Difference between bronchitis and emphysema
-
4
5
CHRONIC BRONCHITIS
bull Chronic bronchitis is defined as persistent cough with sputum production for at least 3 months in at least two consecutive
years
bull The most important cause of chronic bronchitis is recurrent irritation of the bronchial mucosa by inhaled substances as
occurs in cigarette smokers
bull The pathological hallmarks of chronic bronchitis are congestion of the bronchial mucosa and a prominent increase in the
number and size of the bronchial mucus glands Copious mucus may be seen within airway lumens The terminal airways are
most susceptible to obstruction by mucus
Pathophysiology of chronic bronchitisPathophysiology of chronic bronchitis IrritantsIrritants darr darrHyperplasia and hypertrophy of Hyperplasia and hypertrophy of mucous secreting cellmucous secreting cell darr darr Thick mucousThick mucous darr darr Air trappingAir trapping Sticky coating uarrSticky coating uarr darr darr Air way obstructionAir way obstruction Impaired ciliary function uarrImpaired ciliary function uarr darr darr EdemaEdema Decrease mucous clearance uarrDecrease mucous clearance uarr darr darr Bronchial wall thickness and Bronchial wall thickness and Lung defense system compromise inflammationLung defense system compromise inflammation darr uarr darr uarrVulnerable for infection rarr More infection more mucusVulnerable for infection rarr More infection more mucus
VENTILATION COST
bull In COPD work of breathing is greater for any given level of ventilation than normal
VENTILATIONVENTILATION
WORK OF WORK OF BREATHINGBREATHING
NORMAL COPDNORMAL COPD
SEVERE COPDSEVERE COPD
MODERATE COPDMODERATE COPDThe cost of work at a The cost of work at a given ventilation for given ventilation for lsquonormalrsquo and COPD lsquonormalrsquo and COPD patients (ACSM patients (ACSM 1998)1998)
bull Damage to the epithelium impairs the mucociliary response that clears bacteria and mucus Inflammation and secretions provide the
obstructive component of chronic bronchitis
bull In contrast to emphysema chronic bronchitis is associated with a relatively undamaged
pulmonary capillary bed
Emphysema or type A COPD
DefinitionDefinition Abnormal permanent Abnormal permanent
enlargement of air spaces enlargement of air spaces distal to the terminal distal to the terminal bronchioles accompanied bronchioles accompanied by the destruction of the by the destruction of the walls and without obvious walls and without obvious fibrosisfibrosis
Emphysema is characterized Emphysema is characterized by loss of elasticity of the by loss of elasticity of the lung and abnormal lung and abnormal permanent enlargement of permanent enlargement of air spaces with destruction air spaces with destruction of the alveolar walls and of the alveolar walls and capillary beds capillary beds
EtiologiEmphysemaSmoking the primary risk factorLong-term smoking is responsible for 80-90 of casesProlonged exposures to harmful particles and gases from
passive smoke Industrial smoke Chemical gases vapors mists amp fumesDusts from grains minerals amp other materials
Alpha 1-antitrypsin deficiency gtgtemphysemaGeneticsBronchitisAsthma
Pathophysiology
Exposure to inhaled noxious particles amp gases inflammation imbalance of proteinases and anti-proteinases
Dilatation amp destruction +mucus secretion
FIG 1 Inflammatory mechanisms in COPD Cigarette smoke (and other irritants) activate macrophages in the respiratory tract that release neutrophil chemotactic factors including IL-8 and LTB4 These cells then release proteases that break down connective tissue in the lung parenchyma resulting in emphysema and also stimulate mucus hypersecretion These enzymes are normally counteracted by protease inhibitors including 1-antitrypsin SLPI and TIMP Cytotoxic T cells (CD8) may also be recruited and may be involved in alveolar wall destruction Fibroblasts may be activated by growthfactors releases from macrophages and epithelial cells CTG connective tissue growth factor COB chronic obstructive bronchiolitis
Pathophysiology
bull Affects alveolar membranendash Destruction of alveolar wallndash Loss of elastic recoilndash Over distended alveoli
bull Over distended alveolindash Damage to adjacent
pulmonary capillariesndash dead spacendash Impaired passive expiration
Impaired gas exchange
bull Impaired gas exchangendash impaired expiration
bull CO2 bull Hypercapniabull Respiratory acidosis
bull Damaged pulmonary capillary bedndash pulmonary pressure ndash work load for right ventricle
ndash Right side heart failure (due
to respiratory pressure) ndash Cor Pulmonale
16
SYMPTOMScough
sputumdyspnea
EXPOSURE TO RISKFACTORS
tobaccooccupation
indooroutdoor pollution
SPIROMETRY
Diagnosis of COPD
GAS DARAH ARTERILABORATORY TESTCHEST X-RAY
Spirometry Normal and COPDSpirometry Normal and COPD
0
5
1
4
2
3
Lite
r
1 65432
FVC
FVC
FEV1
FEV1
Normal
COPD
39005200
23504150 80
60 NormalCOPD
FVCFEV1 FVCFEV1
Seconds
Normally the left side of the heart produces a higher level of blood pressure in order to pump blood to the body the right side pumps blood through the lungs under much lower pressure Any condition that leads to prolonged high blood pressure in the arteries or veins of the lungs (called pulmonary hypertension) will be poorly tolerated by the right ventricle of the heart When this right ventricle fails or is unable toproperly pump against these abnormally high pressures this is called cor pulmonale
Prognosis
bull Indikator umur dan keparahanbull Jika ada hipoksia dan cor pulmonale
prognosis jelekbull Dyspnea obstruksi berat saluran nafas FEV1 lt 075 L (20) 1048774 angka kematian meningkat
50 pasien berisiko meninggal dalam waktu 5 tahun
Tujuan Terapi
bull Memperbaiki keadaan obstruksi saluran nafasbull Mencegah dan mengatasi eksaserbasi akutbull Menurunkan progresivitas penyakitbull Meningkatkan keadaan fisik dan psikisbull Menurunkan jumlah hari tidak masuk kerjabull Menurunkan lama tinggal di RSbull Menurunkan angka kematian
NON FARMAKOLOGI
bull Menghentikan kebiasaan merokokbull Rehabilitasi paru-paru secara komprehensif
dengan OR dan latihan pernafasanbull Perbaikan nutrisibull Tidak ada obat yang dapat menunda
memburuknya fungsi paru jika pasien tetap merokok
bull Kortikosteroid 1048774 benefit is very limited laporan tentang efektivitasnya masih bervariasi kecuali jika pasien juga memiliki riwayat asma
bull 1048774 Oksigen 1048774 untuk pasien hipoksemia cor pulmonale Digunakan jika baseline PaO2 turun sampai lt 55 mmHg
bull 1048774 Antibiotik 1048774 digunakan bila ada tanda infeksi bukan untuk maintenance therapy
bull 1048774 Vaksinasi 1048774 direkomendasikan untuk high-risk patients vaksin pneumococcus (tiap 5-10 th) dan vaksin influenza (tiap tahun)
bull 1048774 α1-proteinase inhibitor 1048774 utk pasien yang defisiensi α1- antitripsin 1048774 digunakan per minggu masih mahal 1048774 contoh Prolastin
Tahap terapi pada PPOK yang stabil
bull Tahap 1 Ipratropium bromida (MDI) atau nebulizer 2-6 puff 4 x sehari tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (mulut kering amp rasa pahit) jika hasil trial perbaikan FEV1 lt 20 1048774 step 2
bull Tahap 2 Tambahkan β-agonis MDI atau nebulizer tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (takikardi tremor) 1048774 jika tidak ada perkembangan hentikan β-agonis jika ada perbaikan tapi kecil 1048774 step 3
Terapi antibiotika
bull 1048774 Berdasarkan evidence terbaru yang tersedia antibiotika harus diberikan pada pasien-pasien PPOK yang
bull 1048774 Pasien dengan eksaserbasi akut dengan 3 tanda utama yaitu increased dyspnea increased sputum volume increased sputum purulence (Evidence B) atau
bull 1048774 Pasien dengan eksaserbasi akut dengan 2 tanda utama jika peningkatan purulensi sputum merupakan salah satunya (Evidence C)
bull 1048774 Pasien dengan eksaserbasi parah yang membutuhkan ventilasi mekanik baik invasif maupun non-infvasif (Evidence B)
bull Tahap 3 Tambah teofilinmulai dari 400 mghari dlm bentuk sustained released sesuaikan dosis setiap interval 3 hari untuk menjaga serum level antara 10-15 μgml pantau ESO takikardi tremor nervous efek GI jika tidak ada perbaikan 1048774 hentikan teofilin dan 1048774go to step 4
bull Tahap 4 Coba dengan kortikosteroid prednison 30-40 mghari selama 2-4 minggu cek dengan spirometer (perbaikan ge 20) titrasi dosis ke dosis efektif terkecil (lt 10 μg sehari) pertimbangkan penggunaan kortikosteroid inhalasi 1048774 jika pasien tidak berespon baik 1048774 kembali ke steroid oral
Key points
bull 1048774PPOK adalah penyakit yang sebenarnya secara potensial dapat dicegah 1048774 stop smoking
bull 1048774Sekali PPOK terjadi 1048774 penderita akan memerlukan terapi yang kompleks 1048774 yang efikasinya masih diperdebatkan para ahli
bull 1048774Penyakit ini bersifat progresif dan ireversibel1048774 berbiaya besar baik baik personal maupun masyarakat
Difference between bronchitis and Difference between bronchitis and emphysemaemphysema
Productive cough
bronchitis
Classic sign
emphysema
Late in common with infection
Dyspnea Late in course CommonWheezing Intermittent MildHO smoking Common CommonBarrel chest Occasionally classicProlonged expiration Always present Always presentCyanosis Common UncommonChronic hypoventilation
Common Late in course
Ploycythemia Common Late in course
- COPDPPOM
- BRONCHITIS KRONIS atau COPD type B
- Etiologi
- Slide 4
- Slide 5
- CHRONIC BRONCHITIS
- Slide 7
- Slide 8
- VENTILATION COST
- Slide 10
- Emphysema or type A COPD
- Etiologi Emphysema
- Pathophysiology
- Slide 14
- Pathophysiology
- Slide 16
- Slide 17
- Slide 18
- Prognosis
- Tujuan Terapi
- NON FARMAKOLOGI
- Slide 22
- Slide 23
- Tahap terapi pada PPOK yang stabil
- Terapi antibiotika
- Slide 26
- Key points
- Difference between bronchitis and emphysema
-
5
CHRONIC BRONCHITIS
bull Chronic bronchitis is defined as persistent cough with sputum production for at least 3 months in at least two consecutive
years
bull The most important cause of chronic bronchitis is recurrent irritation of the bronchial mucosa by inhaled substances as
occurs in cigarette smokers
bull The pathological hallmarks of chronic bronchitis are congestion of the bronchial mucosa and a prominent increase in the
number and size of the bronchial mucus glands Copious mucus may be seen within airway lumens The terminal airways are
most susceptible to obstruction by mucus
Pathophysiology of chronic bronchitisPathophysiology of chronic bronchitis IrritantsIrritants darr darrHyperplasia and hypertrophy of Hyperplasia and hypertrophy of mucous secreting cellmucous secreting cell darr darr Thick mucousThick mucous darr darr Air trappingAir trapping Sticky coating uarrSticky coating uarr darr darr Air way obstructionAir way obstruction Impaired ciliary function uarrImpaired ciliary function uarr darr darr EdemaEdema Decrease mucous clearance uarrDecrease mucous clearance uarr darr darr Bronchial wall thickness and Bronchial wall thickness and Lung defense system compromise inflammationLung defense system compromise inflammation darr uarr darr uarrVulnerable for infection rarr More infection more mucusVulnerable for infection rarr More infection more mucus
VENTILATION COST
bull In COPD work of breathing is greater for any given level of ventilation than normal
VENTILATIONVENTILATION
WORK OF WORK OF BREATHINGBREATHING
NORMAL COPDNORMAL COPD
SEVERE COPDSEVERE COPD
MODERATE COPDMODERATE COPDThe cost of work at a The cost of work at a given ventilation for given ventilation for lsquonormalrsquo and COPD lsquonormalrsquo and COPD patients (ACSM patients (ACSM 1998)1998)
bull Damage to the epithelium impairs the mucociliary response that clears bacteria and mucus Inflammation and secretions provide the
obstructive component of chronic bronchitis
bull In contrast to emphysema chronic bronchitis is associated with a relatively undamaged
pulmonary capillary bed
Emphysema or type A COPD
DefinitionDefinition Abnormal permanent Abnormal permanent
enlargement of air spaces enlargement of air spaces distal to the terminal distal to the terminal bronchioles accompanied bronchioles accompanied by the destruction of the by the destruction of the walls and without obvious walls and without obvious fibrosisfibrosis
Emphysema is characterized Emphysema is characterized by loss of elasticity of the by loss of elasticity of the lung and abnormal lung and abnormal permanent enlargement of permanent enlargement of air spaces with destruction air spaces with destruction of the alveolar walls and of the alveolar walls and capillary beds capillary beds
EtiologiEmphysemaSmoking the primary risk factorLong-term smoking is responsible for 80-90 of casesProlonged exposures to harmful particles and gases from
passive smoke Industrial smoke Chemical gases vapors mists amp fumesDusts from grains minerals amp other materials
Alpha 1-antitrypsin deficiency gtgtemphysemaGeneticsBronchitisAsthma
Pathophysiology
Exposure to inhaled noxious particles amp gases inflammation imbalance of proteinases and anti-proteinases
Dilatation amp destruction +mucus secretion
FIG 1 Inflammatory mechanisms in COPD Cigarette smoke (and other irritants) activate macrophages in the respiratory tract that release neutrophil chemotactic factors including IL-8 and LTB4 These cells then release proteases that break down connective tissue in the lung parenchyma resulting in emphysema and also stimulate mucus hypersecretion These enzymes are normally counteracted by protease inhibitors including 1-antitrypsin SLPI and TIMP Cytotoxic T cells (CD8) may also be recruited and may be involved in alveolar wall destruction Fibroblasts may be activated by growthfactors releases from macrophages and epithelial cells CTG connective tissue growth factor COB chronic obstructive bronchiolitis
Pathophysiology
bull Affects alveolar membranendash Destruction of alveolar wallndash Loss of elastic recoilndash Over distended alveoli
bull Over distended alveolindash Damage to adjacent
pulmonary capillariesndash dead spacendash Impaired passive expiration
Impaired gas exchange
bull Impaired gas exchangendash impaired expiration
bull CO2 bull Hypercapniabull Respiratory acidosis
bull Damaged pulmonary capillary bedndash pulmonary pressure ndash work load for right ventricle
ndash Right side heart failure (due
to respiratory pressure) ndash Cor Pulmonale
16
SYMPTOMScough
sputumdyspnea
EXPOSURE TO RISKFACTORS
tobaccooccupation
indooroutdoor pollution
SPIROMETRY
Diagnosis of COPD
GAS DARAH ARTERILABORATORY TESTCHEST X-RAY
Spirometry Normal and COPDSpirometry Normal and COPD
0
5
1
4
2
3
Lite
r
1 65432
FVC
FVC
FEV1
FEV1
Normal
COPD
39005200
23504150 80
60 NormalCOPD
FVCFEV1 FVCFEV1
Seconds
Normally the left side of the heart produces a higher level of blood pressure in order to pump blood to the body the right side pumps blood through the lungs under much lower pressure Any condition that leads to prolonged high blood pressure in the arteries or veins of the lungs (called pulmonary hypertension) will be poorly tolerated by the right ventricle of the heart When this right ventricle fails or is unable toproperly pump against these abnormally high pressures this is called cor pulmonale
Prognosis
bull Indikator umur dan keparahanbull Jika ada hipoksia dan cor pulmonale
prognosis jelekbull Dyspnea obstruksi berat saluran nafas FEV1 lt 075 L (20) 1048774 angka kematian meningkat
50 pasien berisiko meninggal dalam waktu 5 tahun
Tujuan Terapi
bull Memperbaiki keadaan obstruksi saluran nafasbull Mencegah dan mengatasi eksaserbasi akutbull Menurunkan progresivitas penyakitbull Meningkatkan keadaan fisik dan psikisbull Menurunkan jumlah hari tidak masuk kerjabull Menurunkan lama tinggal di RSbull Menurunkan angka kematian
NON FARMAKOLOGI
bull Menghentikan kebiasaan merokokbull Rehabilitasi paru-paru secara komprehensif
dengan OR dan latihan pernafasanbull Perbaikan nutrisibull Tidak ada obat yang dapat menunda
memburuknya fungsi paru jika pasien tetap merokok
bull Kortikosteroid 1048774 benefit is very limited laporan tentang efektivitasnya masih bervariasi kecuali jika pasien juga memiliki riwayat asma
bull 1048774 Oksigen 1048774 untuk pasien hipoksemia cor pulmonale Digunakan jika baseline PaO2 turun sampai lt 55 mmHg
bull 1048774 Antibiotik 1048774 digunakan bila ada tanda infeksi bukan untuk maintenance therapy
bull 1048774 Vaksinasi 1048774 direkomendasikan untuk high-risk patients vaksin pneumococcus (tiap 5-10 th) dan vaksin influenza (tiap tahun)
bull 1048774 α1-proteinase inhibitor 1048774 utk pasien yang defisiensi α1- antitripsin 1048774 digunakan per minggu masih mahal 1048774 contoh Prolastin
Tahap terapi pada PPOK yang stabil
bull Tahap 1 Ipratropium bromida (MDI) atau nebulizer 2-6 puff 4 x sehari tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (mulut kering amp rasa pahit) jika hasil trial perbaikan FEV1 lt 20 1048774 step 2
bull Tahap 2 Tambahkan β-agonis MDI atau nebulizer tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (takikardi tremor) 1048774 jika tidak ada perkembangan hentikan β-agonis jika ada perbaikan tapi kecil 1048774 step 3
Terapi antibiotika
bull 1048774 Berdasarkan evidence terbaru yang tersedia antibiotika harus diberikan pada pasien-pasien PPOK yang
bull 1048774 Pasien dengan eksaserbasi akut dengan 3 tanda utama yaitu increased dyspnea increased sputum volume increased sputum purulence (Evidence B) atau
bull 1048774 Pasien dengan eksaserbasi akut dengan 2 tanda utama jika peningkatan purulensi sputum merupakan salah satunya (Evidence C)
bull 1048774 Pasien dengan eksaserbasi parah yang membutuhkan ventilasi mekanik baik invasif maupun non-infvasif (Evidence B)
bull Tahap 3 Tambah teofilinmulai dari 400 mghari dlm bentuk sustained released sesuaikan dosis setiap interval 3 hari untuk menjaga serum level antara 10-15 μgml pantau ESO takikardi tremor nervous efek GI jika tidak ada perbaikan 1048774 hentikan teofilin dan 1048774go to step 4
bull Tahap 4 Coba dengan kortikosteroid prednison 30-40 mghari selama 2-4 minggu cek dengan spirometer (perbaikan ge 20) titrasi dosis ke dosis efektif terkecil (lt 10 μg sehari) pertimbangkan penggunaan kortikosteroid inhalasi 1048774 jika pasien tidak berespon baik 1048774 kembali ke steroid oral
Key points
bull 1048774PPOK adalah penyakit yang sebenarnya secara potensial dapat dicegah 1048774 stop smoking
bull 1048774Sekali PPOK terjadi 1048774 penderita akan memerlukan terapi yang kompleks 1048774 yang efikasinya masih diperdebatkan para ahli
bull 1048774Penyakit ini bersifat progresif dan ireversibel1048774 berbiaya besar baik baik personal maupun masyarakat
Difference between bronchitis and Difference between bronchitis and emphysemaemphysema
Productive cough
bronchitis
Classic sign
emphysema
Late in common with infection
Dyspnea Late in course CommonWheezing Intermittent MildHO smoking Common CommonBarrel chest Occasionally classicProlonged expiration Always present Always presentCyanosis Common UncommonChronic hypoventilation
Common Late in course
Ploycythemia Common Late in course
- COPDPPOM
- BRONCHITIS KRONIS atau COPD type B
- Etiologi
- Slide 4
- Slide 5
- CHRONIC BRONCHITIS
- Slide 7
- Slide 8
- VENTILATION COST
- Slide 10
- Emphysema or type A COPD
- Etiologi Emphysema
- Pathophysiology
- Slide 14
- Pathophysiology
- Slide 16
- Slide 17
- Slide 18
- Prognosis
- Tujuan Terapi
- NON FARMAKOLOGI
- Slide 22
- Slide 23
- Tahap terapi pada PPOK yang stabil
- Terapi antibiotika
- Slide 26
- Key points
- Difference between bronchitis and emphysema
-
CHRONIC BRONCHITIS
bull Chronic bronchitis is defined as persistent cough with sputum production for at least 3 months in at least two consecutive
years
bull The most important cause of chronic bronchitis is recurrent irritation of the bronchial mucosa by inhaled substances as
occurs in cigarette smokers
bull The pathological hallmarks of chronic bronchitis are congestion of the bronchial mucosa and a prominent increase in the
number and size of the bronchial mucus glands Copious mucus may be seen within airway lumens The terminal airways are
most susceptible to obstruction by mucus
Pathophysiology of chronic bronchitisPathophysiology of chronic bronchitis IrritantsIrritants darr darrHyperplasia and hypertrophy of Hyperplasia and hypertrophy of mucous secreting cellmucous secreting cell darr darr Thick mucousThick mucous darr darr Air trappingAir trapping Sticky coating uarrSticky coating uarr darr darr Air way obstructionAir way obstruction Impaired ciliary function uarrImpaired ciliary function uarr darr darr EdemaEdema Decrease mucous clearance uarrDecrease mucous clearance uarr darr darr Bronchial wall thickness and Bronchial wall thickness and Lung defense system compromise inflammationLung defense system compromise inflammation darr uarr darr uarrVulnerable for infection rarr More infection more mucusVulnerable for infection rarr More infection more mucus
VENTILATION COST
bull In COPD work of breathing is greater for any given level of ventilation than normal
VENTILATIONVENTILATION
WORK OF WORK OF BREATHINGBREATHING
NORMAL COPDNORMAL COPD
SEVERE COPDSEVERE COPD
MODERATE COPDMODERATE COPDThe cost of work at a The cost of work at a given ventilation for given ventilation for lsquonormalrsquo and COPD lsquonormalrsquo and COPD patients (ACSM patients (ACSM 1998)1998)
bull Damage to the epithelium impairs the mucociliary response that clears bacteria and mucus Inflammation and secretions provide the
obstructive component of chronic bronchitis
bull In contrast to emphysema chronic bronchitis is associated with a relatively undamaged
pulmonary capillary bed
Emphysema or type A COPD
DefinitionDefinition Abnormal permanent Abnormal permanent
enlargement of air spaces enlargement of air spaces distal to the terminal distal to the terminal bronchioles accompanied bronchioles accompanied by the destruction of the by the destruction of the walls and without obvious walls and without obvious fibrosisfibrosis
Emphysema is characterized Emphysema is characterized by loss of elasticity of the by loss of elasticity of the lung and abnormal lung and abnormal permanent enlargement of permanent enlargement of air spaces with destruction air spaces with destruction of the alveolar walls and of the alveolar walls and capillary beds capillary beds
EtiologiEmphysemaSmoking the primary risk factorLong-term smoking is responsible for 80-90 of casesProlonged exposures to harmful particles and gases from
passive smoke Industrial smoke Chemical gases vapors mists amp fumesDusts from grains minerals amp other materials
Alpha 1-antitrypsin deficiency gtgtemphysemaGeneticsBronchitisAsthma
Pathophysiology
Exposure to inhaled noxious particles amp gases inflammation imbalance of proteinases and anti-proteinases
Dilatation amp destruction +mucus secretion
FIG 1 Inflammatory mechanisms in COPD Cigarette smoke (and other irritants) activate macrophages in the respiratory tract that release neutrophil chemotactic factors including IL-8 and LTB4 These cells then release proteases that break down connective tissue in the lung parenchyma resulting in emphysema and also stimulate mucus hypersecretion These enzymes are normally counteracted by protease inhibitors including 1-antitrypsin SLPI and TIMP Cytotoxic T cells (CD8) may also be recruited and may be involved in alveolar wall destruction Fibroblasts may be activated by growthfactors releases from macrophages and epithelial cells CTG connective tissue growth factor COB chronic obstructive bronchiolitis
Pathophysiology
bull Affects alveolar membranendash Destruction of alveolar wallndash Loss of elastic recoilndash Over distended alveoli
bull Over distended alveolindash Damage to adjacent
pulmonary capillariesndash dead spacendash Impaired passive expiration
Impaired gas exchange
bull Impaired gas exchangendash impaired expiration
bull CO2 bull Hypercapniabull Respiratory acidosis
bull Damaged pulmonary capillary bedndash pulmonary pressure ndash work load for right ventricle
ndash Right side heart failure (due
to respiratory pressure) ndash Cor Pulmonale
16
SYMPTOMScough
sputumdyspnea
EXPOSURE TO RISKFACTORS
tobaccooccupation
indooroutdoor pollution
SPIROMETRY
Diagnosis of COPD
GAS DARAH ARTERILABORATORY TESTCHEST X-RAY
Spirometry Normal and COPDSpirometry Normal and COPD
0
5
1
4
2
3
Lite
r
1 65432
FVC
FVC
FEV1
FEV1
Normal
COPD
39005200
23504150 80
60 NormalCOPD
FVCFEV1 FVCFEV1
Seconds
Normally the left side of the heart produces a higher level of blood pressure in order to pump blood to the body the right side pumps blood through the lungs under much lower pressure Any condition that leads to prolonged high blood pressure in the arteries or veins of the lungs (called pulmonary hypertension) will be poorly tolerated by the right ventricle of the heart When this right ventricle fails or is unable toproperly pump against these abnormally high pressures this is called cor pulmonale
Prognosis
bull Indikator umur dan keparahanbull Jika ada hipoksia dan cor pulmonale
prognosis jelekbull Dyspnea obstruksi berat saluran nafas FEV1 lt 075 L (20) 1048774 angka kematian meningkat
50 pasien berisiko meninggal dalam waktu 5 tahun
Tujuan Terapi
bull Memperbaiki keadaan obstruksi saluran nafasbull Mencegah dan mengatasi eksaserbasi akutbull Menurunkan progresivitas penyakitbull Meningkatkan keadaan fisik dan psikisbull Menurunkan jumlah hari tidak masuk kerjabull Menurunkan lama tinggal di RSbull Menurunkan angka kematian
NON FARMAKOLOGI
bull Menghentikan kebiasaan merokokbull Rehabilitasi paru-paru secara komprehensif
dengan OR dan latihan pernafasanbull Perbaikan nutrisibull Tidak ada obat yang dapat menunda
memburuknya fungsi paru jika pasien tetap merokok
bull Kortikosteroid 1048774 benefit is very limited laporan tentang efektivitasnya masih bervariasi kecuali jika pasien juga memiliki riwayat asma
bull 1048774 Oksigen 1048774 untuk pasien hipoksemia cor pulmonale Digunakan jika baseline PaO2 turun sampai lt 55 mmHg
bull 1048774 Antibiotik 1048774 digunakan bila ada tanda infeksi bukan untuk maintenance therapy
bull 1048774 Vaksinasi 1048774 direkomendasikan untuk high-risk patients vaksin pneumococcus (tiap 5-10 th) dan vaksin influenza (tiap tahun)
bull 1048774 α1-proteinase inhibitor 1048774 utk pasien yang defisiensi α1- antitripsin 1048774 digunakan per minggu masih mahal 1048774 contoh Prolastin
Tahap terapi pada PPOK yang stabil
bull Tahap 1 Ipratropium bromida (MDI) atau nebulizer 2-6 puff 4 x sehari tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (mulut kering amp rasa pahit) jika hasil trial perbaikan FEV1 lt 20 1048774 step 2
bull Tahap 2 Tambahkan β-agonis MDI atau nebulizer tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (takikardi tremor) 1048774 jika tidak ada perkembangan hentikan β-agonis jika ada perbaikan tapi kecil 1048774 step 3
Terapi antibiotika
bull 1048774 Berdasarkan evidence terbaru yang tersedia antibiotika harus diberikan pada pasien-pasien PPOK yang
bull 1048774 Pasien dengan eksaserbasi akut dengan 3 tanda utama yaitu increased dyspnea increased sputum volume increased sputum purulence (Evidence B) atau
bull 1048774 Pasien dengan eksaserbasi akut dengan 2 tanda utama jika peningkatan purulensi sputum merupakan salah satunya (Evidence C)
bull 1048774 Pasien dengan eksaserbasi parah yang membutuhkan ventilasi mekanik baik invasif maupun non-infvasif (Evidence B)
bull Tahap 3 Tambah teofilinmulai dari 400 mghari dlm bentuk sustained released sesuaikan dosis setiap interval 3 hari untuk menjaga serum level antara 10-15 μgml pantau ESO takikardi tremor nervous efek GI jika tidak ada perbaikan 1048774 hentikan teofilin dan 1048774go to step 4
bull Tahap 4 Coba dengan kortikosteroid prednison 30-40 mghari selama 2-4 minggu cek dengan spirometer (perbaikan ge 20) titrasi dosis ke dosis efektif terkecil (lt 10 μg sehari) pertimbangkan penggunaan kortikosteroid inhalasi 1048774 jika pasien tidak berespon baik 1048774 kembali ke steroid oral
Key points
bull 1048774PPOK adalah penyakit yang sebenarnya secara potensial dapat dicegah 1048774 stop smoking
bull 1048774Sekali PPOK terjadi 1048774 penderita akan memerlukan terapi yang kompleks 1048774 yang efikasinya masih diperdebatkan para ahli
bull 1048774Penyakit ini bersifat progresif dan ireversibel1048774 berbiaya besar baik baik personal maupun masyarakat
Difference between bronchitis and Difference between bronchitis and emphysemaemphysema
Productive cough
bronchitis
Classic sign
emphysema
Late in common with infection
Dyspnea Late in course CommonWheezing Intermittent MildHO smoking Common CommonBarrel chest Occasionally classicProlonged expiration Always present Always presentCyanosis Common UncommonChronic hypoventilation
Common Late in course
Ploycythemia Common Late in course
- COPDPPOM
- BRONCHITIS KRONIS atau COPD type B
- Etiologi
- Slide 4
- Slide 5
- CHRONIC BRONCHITIS
- Slide 7
- Slide 8
- VENTILATION COST
- Slide 10
- Emphysema or type A COPD
- Etiologi Emphysema
- Pathophysiology
- Slide 14
- Pathophysiology
- Slide 16
- Slide 17
- Slide 18
- Prognosis
- Tujuan Terapi
- NON FARMAKOLOGI
- Slide 22
- Slide 23
- Tahap terapi pada PPOK yang stabil
- Terapi antibiotika
- Slide 26
- Key points
- Difference between bronchitis and emphysema
-
Pathophysiology of chronic bronchitisPathophysiology of chronic bronchitis IrritantsIrritants darr darrHyperplasia and hypertrophy of Hyperplasia and hypertrophy of mucous secreting cellmucous secreting cell darr darr Thick mucousThick mucous darr darr Air trappingAir trapping Sticky coating uarrSticky coating uarr darr darr Air way obstructionAir way obstruction Impaired ciliary function uarrImpaired ciliary function uarr darr darr EdemaEdema Decrease mucous clearance uarrDecrease mucous clearance uarr darr darr Bronchial wall thickness and Bronchial wall thickness and Lung defense system compromise inflammationLung defense system compromise inflammation darr uarr darr uarrVulnerable for infection rarr More infection more mucusVulnerable for infection rarr More infection more mucus
VENTILATION COST
bull In COPD work of breathing is greater for any given level of ventilation than normal
VENTILATIONVENTILATION
WORK OF WORK OF BREATHINGBREATHING
NORMAL COPDNORMAL COPD
SEVERE COPDSEVERE COPD
MODERATE COPDMODERATE COPDThe cost of work at a The cost of work at a given ventilation for given ventilation for lsquonormalrsquo and COPD lsquonormalrsquo and COPD patients (ACSM patients (ACSM 1998)1998)
bull Damage to the epithelium impairs the mucociliary response that clears bacteria and mucus Inflammation and secretions provide the
obstructive component of chronic bronchitis
bull In contrast to emphysema chronic bronchitis is associated with a relatively undamaged
pulmonary capillary bed
Emphysema or type A COPD
DefinitionDefinition Abnormal permanent Abnormal permanent
enlargement of air spaces enlargement of air spaces distal to the terminal distal to the terminal bronchioles accompanied bronchioles accompanied by the destruction of the by the destruction of the walls and without obvious walls and without obvious fibrosisfibrosis
Emphysema is characterized Emphysema is characterized by loss of elasticity of the by loss of elasticity of the lung and abnormal lung and abnormal permanent enlargement of permanent enlargement of air spaces with destruction air spaces with destruction of the alveolar walls and of the alveolar walls and capillary beds capillary beds
EtiologiEmphysemaSmoking the primary risk factorLong-term smoking is responsible for 80-90 of casesProlonged exposures to harmful particles and gases from
passive smoke Industrial smoke Chemical gases vapors mists amp fumesDusts from grains minerals amp other materials
Alpha 1-antitrypsin deficiency gtgtemphysemaGeneticsBronchitisAsthma
Pathophysiology
Exposure to inhaled noxious particles amp gases inflammation imbalance of proteinases and anti-proteinases
Dilatation amp destruction +mucus secretion
FIG 1 Inflammatory mechanisms in COPD Cigarette smoke (and other irritants) activate macrophages in the respiratory tract that release neutrophil chemotactic factors including IL-8 and LTB4 These cells then release proteases that break down connective tissue in the lung parenchyma resulting in emphysema and also stimulate mucus hypersecretion These enzymes are normally counteracted by protease inhibitors including 1-antitrypsin SLPI and TIMP Cytotoxic T cells (CD8) may also be recruited and may be involved in alveolar wall destruction Fibroblasts may be activated by growthfactors releases from macrophages and epithelial cells CTG connective tissue growth factor COB chronic obstructive bronchiolitis
Pathophysiology
bull Affects alveolar membranendash Destruction of alveolar wallndash Loss of elastic recoilndash Over distended alveoli
bull Over distended alveolindash Damage to adjacent
pulmonary capillariesndash dead spacendash Impaired passive expiration
Impaired gas exchange
bull Impaired gas exchangendash impaired expiration
bull CO2 bull Hypercapniabull Respiratory acidosis
bull Damaged pulmonary capillary bedndash pulmonary pressure ndash work load for right ventricle
ndash Right side heart failure (due
to respiratory pressure) ndash Cor Pulmonale
16
SYMPTOMScough
sputumdyspnea
EXPOSURE TO RISKFACTORS
tobaccooccupation
indooroutdoor pollution
SPIROMETRY
Diagnosis of COPD
GAS DARAH ARTERILABORATORY TESTCHEST X-RAY
Spirometry Normal and COPDSpirometry Normal and COPD
0
5
1
4
2
3
Lite
r
1 65432
FVC
FVC
FEV1
FEV1
Normal
COPD
39005200
23504150 80
60 NormalCOPD
FVCFEV1 FVCFEV1
Seconds
Normally the left side of the heart produces a higher level of blood pressure in order to pump blood to the body the right side pumps blood through the lungs under much lower pressure Any condition that leads to prolonged high blood pressure in the arteries or veins of the lungs (called pulmonary hypertension) will be poorly tolerated by the right ventricle of the heart When this right ventricle fails or is unable toproperly pump against these abnormally high pressures this is called cor pulmonale
Prognosis
bull Indikator umur dan keparahanbull Jika ada hipoksia dan cor pulmonale
prognosis jelekbull Dyspnea obstruksi berat saluran nafas FEV1 lt 075 L (20) 1048774 angka kematian meningkat
50 pasien berisiko meninggal dalam waktu 5 tahun
Tujuan Terapi
bull Memperbaiki keadaan obstruksi saluran nafasbull Mencegah dan mengatasi eksaserbasi akutbull Menurunkan progresivitas penyakitbull Meningkatkan keadaan fisik dan psikisbull Menurunkan jumlah hari tidak masuk kerjabull Menurunkan lama tinggal di RSbull Menurunkan angka kematian
NON FARMAKOLOGI
bull Menghentikan kebiasaan merokokbull Rehabilitasi paru-paru secara komprehensif
dengan OR dan latihan pernafasanbull Perbaikan nutrisibull Tidak ada obat yang dapat menunda
memburuknya fungsi paru jika pasien tetap merokok
bull Kortikosteroid 1048774 benefit is very limited laporan tentang efektivitasnya masih bervariasi kecuali jika pasien juga memiliki riwayat asma
bull 1048774 Oksigen 1048774 untuk pasien hipoksemia cor pulmonale Digunakan jika baseline PaO2 turun sampai lt 55 mmHg
bull 1048774 Antibiotik 1048774 digunakan bila ada tanda infeksi bukan untuk maintenance therapy
bull 1048774 Vaksinasi 1048774 direkomendasikan untuk high-risk patients vaksin pneumococcus (tiap 5-10 th) dan vaksin influenza (tiap tahun)
bull 1048774 α1-proteinase inhibitor 1048774 utk pasien yang defisiensi α1- antitripsin 1048774 digunakan per minggu masih mahal 1048774 contoh Prolastin
Tahap terapi pada PPOK yang stabil
bull Tahap 1 Ipratropium bromida (MDI) atau nebulizer 2-6 puff 4 x sehari tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (mulut kering amp rasa pahit) jika hasil trial perbaikan FEV1 lt 20 1048774 step 2
bull Tahap 2 Tambahkan β-agonis MDI atau nebulizer tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (takikardi tremor) 1048774 jika tidak ada perkembangan hentikan β-agonis jika ada perbaikan tapi kecil 1048774 step 3
Terapi antibiotika
bull 1048774 Berdasarkan evidence terbaru yang tersedia antibiotika harus diberikan pada pasien-pasien PPOK yang
bull 1048774 Pasien dengan eksaserbasi akut dengan 3 tanda utama yaitu increased dyspnea increased sputum volume increased sputum purulence (Evidence B) atau
bull 1048774 Pasien dengan eksaserbasi akut dengan 2 tanda utama jika peningkatan purulensi sputum merupakan salah satunya (Evidence C)
bull 1048774 Pasien dengan eksaserbasi parah yang membutuhkan ventilasi mekanik baik invasif maupun non-infvasif (Evidence B)
bull Tahap 3 Tambah teofilinmulai dari 400 mghari dlm bentuk sustained released sesuaikan dosis setiap interval 3 hari untuk menjaga serum level antara 10-15 μgml pantau ESO takikardi tremor nervous efek GI jika tidak ada perbaikan 1048774 hentikan teofilin dan 1048774go to step 4
bull Tahap 4 Coba dengan kortikosteroid prednison 30-40 mghari selama 2-4 minggu cek dengan spirometer (perbaikan ge 20) titrasi dosis ke dosis efektif terkecil (lt 10 μg sehari) pertimbangkan penggunaan kortikosteroid inhalasi 1048774 jika pasien tidak berespon baik 1048774 kembali ke steroid oral
Key points
bull 1048774PPOK adalah penyakit yang sebenarnya secara potensial dapat dicegah 1048774 stop smoking
bull 1048774Sekali PPOK terjadi 1048774 penderita akan memerlukan terapi yang kompleks 1048774 yang efikasinya masih diperdebatkan para ahli
bull 1048774Penyakit ini bersifat progresif dan ireversibel1048774 berbiaya besar baik baik personal maupun masyarakat
Difference between bronchitis and Difference between bronchitis and emphysemaemphysema
Productive cough
bronchitis
Classic sign
emphysema
Late in common with infection
Dyspnea Late in course CommonWheezing Intermittent MildHO smoking Common CommonBarrel chest Occasionally classicProlonged expiration Always present Always presentCyanosis Common UncommonChronic hypoventilation
Common Late in course
Ploycythemia Common Late in course
- COPDPPOM
- BRONCHITIS KRONIS atau COPD type B
- Etiologi
- Slide 4
- Slide 5
- CHRONIC BRONCHITIS
- Slide 7
- Slide 8
- VENTILATION COST
- Slide 10
- Emphysema or type A COPD
- Etiologi Emphysema
- Pathophysiology
- Slide 14
- Pathophysiology
- Slide 16
- Slide 17
- Slide 18
- Prognosis
- Tujuan Terapi
- NON FARMAKOLOGI
- Slide 22
- Slide 23
- Tahap terapi pada PPOK yang stabil
- Terapi antibiotika
- Slide 26
- Key points
- Difference between bronchitis and emphysema
-
VENTILATION COST
bull In COPD work of breathing is greater for any given level of ventilation than normal
VENTILATIONVENTILATION
WORK OF WORK OF BREATHINGBREATHING
NORMAL COPDNORMAL COPD
SEVERE COPDSEVERE COPD
MODERATE COPDMODERATE COPDThe cost of work at a The cost of work at a given ventilation for given ventilation for lsquonormalrsquo and COPD lsquonormalrsquo and COPD patients (ACSM patients (ACSM 1998)1998)
bull Damage to the epithelium impairs the mucociliary response that clears bacteria and mucus Inflammation and secretions provide the
obstructive component of chronic bronchitis
bull In contrast to emphysema chronic bronchitis is associated with a relatively undamaged
pulmonary capillary bed
Emphysema or type A COPD
DefinitionDefinition Abnormal permanent Abnormal permanent
enlargement of air spaces enlargement of air spaces distal to the terminal distal to the terminal bronchioles accompanied bronchioles accompanied by the destruction of the by the destruction of the walls and without obvious walls and without obvious fibrosisfibrosis
Emphysema is characterized Emphysema is characterized by loss of elasticity of the by loss of elasticity of the lung and abnormal lung and abnormal permanent enlargement of permanent enlargement of air spaces with destruction air spaces with destruction of the alveolar walls and of the alveolar walls and capillary beds capillary beds
EtiologiEmphysemaSmoking the primary risk factorLong-term smoking is responsible for 80-90 of casesProlonged exposures to harmful particles and gases from
passive smoke Industrial smoke Chemical gases vapors mists amp fumesDusts from grains minerals amp other materials
Alpha 1-antitrypsin deficiency gtgtemphysemaGeneticsBronchitisAsthma
Pathophysiology
Exposure to inhaled noxious particles amp gases inflammation imbalance of proteinases and anti-proteinases
Dilatation amp destruction +mucus secretion
FIG 1 Inflammatory mechanisms in COPD Cigarette smoke (and other irritants) activate macrophages in the respiratory tract that release neutrophil chemotactic factors including IL-8 and LTB4 These cells then release proteases that break down connective tissue in the lung parenchyma resulting in emphysema and also stimulate mucus hypersecretion These enzymes are normally counteracted by protease inhibitors including 1-antitrypsin SLPI and TIMP Cytotoxic T cells (CD8) may also be recruited and may be involved in alveolar wall destruction Fibroblasts may be activated by growthfactors releases from macrophages and epithelial cells CTG connective tissue growth factor COB chronic obstructive bronchiolitis
Pathophysiology
bull Affects alveolar membranendash Destruction of alveolar wallndash Loss of elastic recoilndash Over distended alveoli
bull Over distended alveolindash Damage to adjacent
pulmonary capillariesndash dead spacendash Impaired passive expiration
Impaired gas exchange
bull Impaired gas exchangendash impaired expiration
bull CO2 bull Hypercapniabull Respiratory acidosis
bull Damaged pulmonary capillary bedndash pulmonary pressure ndash work load for right ventricle
ndash Right side heart failure (due
to respiratory pressure) ndash Cor Pulmonale
16
SYMPTOMScough
sputumdyspnea
EXPOSURE TO RISKFACTORS
tobaccooccupation
indooroutdoor pollution
SPIROMETRY
Diagnosis of COPD
GAS DARAH ARTERILABORATORY TESTCHEST X-RAY
Spirometry Normal and COPDSpirometry Normal and COPD
0
5
1
4
2
3
Lite
r
1 65432
FVC
FVC
FEV1
FEV1
Normal
COPD
39005200
23504150 80
60 NormalCOPD
FVCFEV1 FVCFEV1
Seconds
Normally the left side of the heart produces a higher level of blood pressure in order to pump blood to the body the right side pumps blood through the lungs under much lower pressure Any condition that leads to prolonged high blood pressure in the arteries or veins of the lungs (called pulmonary hypertension) will be poorly tolerated by the right ventricle of the heart When this right ventricle fails or is unable toproperly pump against these abnormally high pressures this is called cor pulmonale
Prognosis
bull Indikator umur dan keparahanbull Jika ada hipoksia dan cor pulmonale
prognosis jelekbull Dyspnea obstruksi berat saluran nafas FEV1 lt 075 L (20) 1048774 angka kematian meningkat
50 pasien berisiko meninggal dalam waktu 5 tahun
Tujuan Terapi
bull Memperbaiki keadaan obstruksi saluran nafasbull Mencegah dan mengatasi eksaserbasi akutbull Menurunkan progresivitas penyakitbull Meningkatkan keadaan fisik dan psikisbull Menurunkan jumlah hari tidak masuk kerjabull Menurunkan lama tinggal di RSbull Menurunkan angka kematian
NON FARMAKOLOGI
bull Menghentikan kebiasaan merokokbull Rehabilitasi paru-paru secara komprehensif
dengan OR dan latihan pernafasanbull Perbaikan nutrisibull Tidak ada obat yang dapat menunda
memburuknya fungsi paru jika pasien tetap merokok
bull Kortikosteroid 1048774 benefit is very limited laporan tentang efektivitasnya masih bervariasi kecuali jika pasien juga memiliki riwayat asma
bull 1048774 Oksigen 1048774 untuk pasien hipoksemia cor pulmonale Digunakan jika baseline PaO2 turun sampai lt 55 mmHg
bull 1048774 Antibiotik 1048774 digunakan bila ada tanda infeksi bukan untuk maintenance therapy
bull 1048774 Vaksinasi 1048774 direkomendasikan untuk high-risk patients vaksin pneumococcus (tiap 5-10 th) dan vaksin influenza (tiap tahun)
bull 1048774 α1-proteinase inhibitor 1048774 utk pasien yang defisiensi α1- antitripsin 1048774 digunakan per minggu masih mahal 1048774 contoh Prolastin
Tahap terapi pada PPOK yang stabil
bull Tahap 1 Ipratropium bromida (MDI) atau nebulizer 2-6 puff 4 x sehari tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (mulut kering amp rasa pahit) jika hasil trial perbaikan FEV1 lt 20 1048774 step 2
bull Tahap 2 Tambahkan β-agonis MDI atau nebulizer tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (takikardi tremor) 1048774 jika tidak ada perkembangan hentikan β-agonis jika ada perbaikan tapi kecil 1048774 step 3
Terapi antibiotika
bull 1048774 Berdasarkan evidence terbaru yang tersedia antibiotika harus diberikan pada pasien-pasien PPOK yang
bull 1048774 Pasien dengan eksaserbasi akut dengan 3 tanda utama yaitu increased dyspnea increased sputum volume increased sputum purulence (Evidence B) atau
bull 1048774 Pasien dengan eksaserbasi akut dengan 2 tanda utama jika peningkatan purulensi sputum merupakan salah satunya (Evidence C)
bull 1048774 Pasien dengan eksaserbasi parah yang membutuhkan ventilasi mekanik baik invasif maupun non-infvasif (Evidence B)
bull Tahap 3 Tambah teofilinmulai dari 400 mghari dlm bentuk sustained released sesuaikan dosis setiap interval 3 hari untuk menjaga serum level antara 10-15 μgml pantau ESO takikardi tremor nervous efek GI jika tidak ada perbaikan 1048774 hentikan teofilin dan 1048774go to step 4
bull Tahap 4 Coba dengan kortikosteroid prednison 30-40 mghari selama 2-4 minggu cek dengan spirometer (perbaikan ge 20) titrasi dosis ke dosis efektif terkecil (lt 10 μg sehari) pertimbangkan penggunaan kortikosteroid inhalasi 1048774 jika pasien tidak berespon baik 1048774 kembali ke steroid oral
Key points
bull 1048774PPOK adalah penyakit yang sebenarnya secara potensial dapat dicegah 1048774 stop smoking
bull 1048774Sekali PPOK terjadi 1048774 penderita akan memerlukan terapi yang kompleks 1048774 yang efikasinya masih diperdebatkan para ahli
bull 1048774Penyakit ini bersifat progresif dan ireversibel1048774 berbiaya besar baik baik personal maupun masyarakat
Difference between bronchitis and Difference between bronchitis and emphysemaemphysema
Productive cough
bronchitis
Classic sign
emphysema
Late in common with infection
Dyspnea Late in course CommonWheezing Intermittent MildHO smoking Common CommonBarrel chest Occasionally classicProlonged expiration Always present Always presentCyanosis Common UncommonChronic hypoventilation
Common Late in course
Ploycythemia Common Late in course
- COPDPPOM
- BRONCHITIS KRONIS atau COPD type B
- Etiologi
- Slide 4
- Slide 5
- CHRONIC BRONCHITIS
- Slide 7
- Slide 8
- VENTILATION COST
- Slide 10
- Emphysema or type A COPD
- Etiologi Emphysema
- Pathophysiology
- Slide 14
- Pathophysiology
- Slide 16
- Slide 17
- Slide 18
- Prognosis
- Tujuan Terapi
- NON FARMAKOLOGI
- Slide 22
- Slide 23
- Tahap terapi pada PPOK yang stabil
- Terapi antibiotika
- Slide 26
- Key points
- Difference between bronchitis and emphysema
-
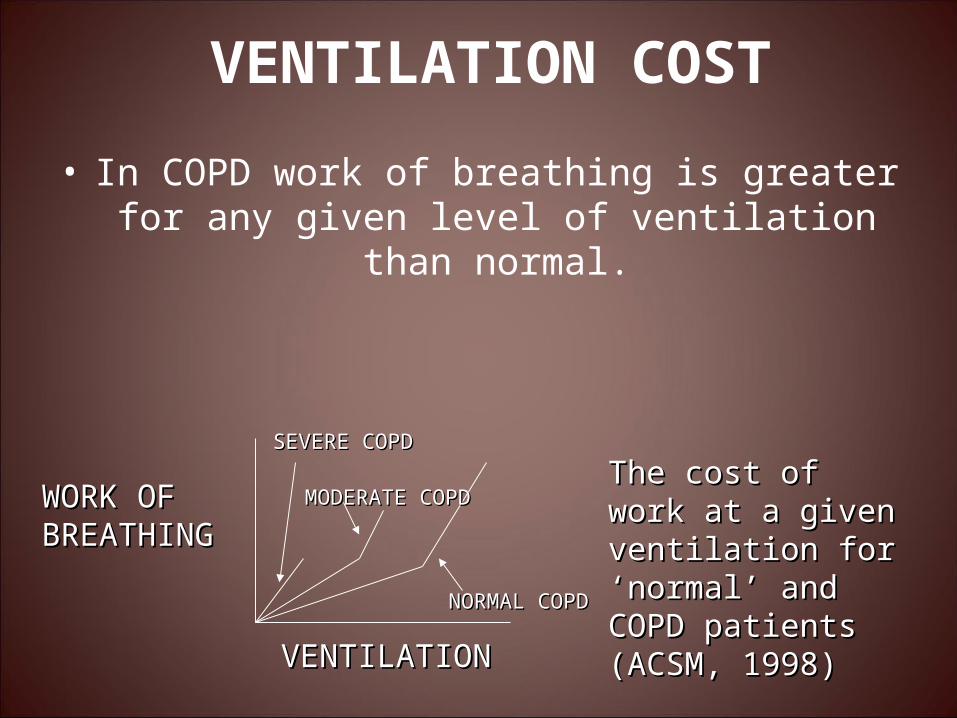
bull Damage to the epithelium impairs the mucociliary response that clears bacteria and mucus Inflammation and secretions provide the
obstructive component of chronic bronchitis
bull In contrast to emphysema chronic bronchitis is associated with a relatively undamaged
pulmonary capillary bed
Emphysema or type A COPD
DefinitionDefinition Abnormal permanent Abnormal permanent
enlargement of air spaces enlargement of air spaces distal to the terminal distal to the terminal bronchioles accompanied bronchioles accompanied by the destruction of the by the destruction of the walls and without obvious walls and without obvious fibrosisfibrosis
Emphysema is characterized Emphysema is characterized by loss of elasticity of the by loss of elasticity of the lung and abnormal lung and abnormal permanent enlargement of permanent enlargement of air spaces with destruction air spaces with destruction of the alveolar walls and of the alveolar walls and capillary beds capillary beds
EtiologiEmphysemaSmoking the primary risk factorLong-term smoking is responsible for 80-90 of casesProlonged exposures to harmful particles and gases from
passive smoke Industrial smoke Chemical gases vapors mists amp fumesDusts from grains minerals amp other materials
Alpha 1-antitrypsin deficiency gtgtemphysemaGeneticsBronchitisAsthma
Pathophysiology
Exposure to inhaled noxious particles amp gases inflammation imbalance of proteinases and anti-proteinases
Dilatation amp destruction +mucus secretion
FIG 1 Inflammatory mechanisms in COPD Cigarette smoke (and other irritants) activate macrophages in the respiratory tract that release neutrophil chemotactic factors including IL-8 and LTB4 These cells then release proteases that break down connective tissue in the lung parenchyma resulting in emphysema and also stimulate mucus hypersecretion These enzymes are normally counteracted by protease inhibitors including 1-antitrypsin SLPI and TIMP Cytotoxic T cells (CD8) may also be recruited and may be involved in alveolar wall destruction Fibroblasts may be activated by growthfactors releases from macrophages and epithelial cells CTG connective tissue growth factor COB chronic obstructive bronchiolitis
Pathophysiology
bull Affects alveolar membranendash Destruction of alveolar wallndash Loss of elastic recoilndash Over distended alveoli
bull Over distended alveolindash Damage to adjacent
pulmonary capillariesndash dead spacendash Impaired passive expiration
Impaired gas exchange
bull Impaired gas exchangendash impaired expiration
bull CO2 bull Hypercapniabull Respiratory acidosis
bull Damaged pulmonary capillary bedndash pulmonary pressure ndash work load for right ventricle
ndash Right side heart failure (due
to respiratory pressure) ndash Cor Pulmonale
16
SYMPTOMScough
sputumdyspnea
EXPOSURE TO RISKFACTORS
tobaccooccupation
indooroutdoor pollution
SPIROMETRY
Diagnosis of COPD
GAS DARAH ARTERILABORATORY TESTCHEST X-RAY
Spirometry Normal and COPDSpirometry Normal and COPD
0
5
1
4
2
3
Lite
r
1 65432
FVC
FVC
FEV1
FEV1
Normal
COPD
39005200
23504150 80
60 NormalCOPD
FVCFEV1 FVCFEV1
Seconds
Normally the left side of the heart produces a higher level of blood pressure in order to pump blood to the body the right side pumps blood through the lungs under much lower pressure Any condition that leads to prolonged high blood pressure in the arteries or veins of the lungs (called pulmonary hypertension) will be poorly tolerated by the right ventricle of the heart When this right ventricle fails or is unable toproperly pump against these abnormally high pressures this is called cor pulmonale
Prognosis
bull Indikator umur dan keparahanbull Jika ada hipoksia dan cor pulmonale
prognosis jelekbull Dyspnea obstruksi berat saluran nafas FEV1 lt 075 L (20) 1048774 angka kematian meningkat
50 pasien berisiko meninggal dalam waktu 5 tahun
Tujuan Terapi
bull Memperbaiki keadaan obstruksi saluran nafasbull Mencegah dan mengatasi eksaserbasi akutbull Menurunkan progresivitas penyakitbull Meningkatkan keadaan fisik dan psikisbull Menurunkan jumlah hari tidak masuk kerjabull Menurunkan lama tinggal di RSbull Menurunkan angka kematian
NON FARMAKOLOGI
bull Menghentikan kebiasaan merokokbull Rehabilitasi paru-paru secara komprehensif
dengan OR dan latihan pernafasanbull Perbaikan nutrisibull Tidak ada obat yang dapat menunda
memburuknya fungsi paru jika pasien tetap merokok
bull Kortikosteroid 1048774 benefit is very limited laporan tentang efektivitasnya masih bervariasi kecuali jika pasien juga memiliki riwayat asma
bull 1048774 Oksigen 1048774 untuk pasien hipoksemia cor pulmonale Digunakan jika baseline PaO2 turun sampai lt 55 mmHg
bull 1048774 Antibiotik 1048774 digunakan bila ada tanda infeksi bukan untuk maintenance therapy
bull 1048774 Vaksinasi 1048774 direkomendasikan untuk high-risk patients vaksin pneumococcus (tiap 5-10 th) dan vaksin influenza (tiap tahun)
bull 1048774 α1-proteinase inhibitor 1048774 utk pasien yang defisiensi α1- antitripsin 1048774 digunakan per minggu masih mahal 1048774 contoh Prolastin
Tahap terapi pada PPOK yang stabil
bull Tahap 1 Ipratropium bromida (MDI) atau nebulizer 2-6 puff 4 x sehari tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (mulut kering amp rasa pahit) jika hasil trial perbaikan FEV1 lt 20 1048774 step 2
bull Tahap 2 Tambahkan β-agonis MDI atau nebulizer tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (takikardi tremor) 1048774 jika tidak ada perkembangan hentikan β-agonis jika ada perbaikan tapi kecil 1048774 step 3
Terapi antibiotika
bull 1048774 Berdasarkan evidence terbaru yang tersedia antibiotika harus diberikan pada pasien-pasien PPOK yang
bull 1048774 Pasien dengan eksaserbasi akut dengan 3 tanda utama yaitu increased dyspnea increased sputum volume increased sputum purulence (Evidence B) atau
bull 1048774 Pasien dengan eksaserbasi akut dengan 2 tanda utama jika peningkatan purulensi sputum merupakan salah satunya (Evidence C)
bull 1048774 Pasien dengan eksaserbasi parah yang membutuhkan ventilasi mekanik baik invasif maupun non-infvasif (Evidence B)
bull Tahap 3 Tambah teofilinmulai dari 400 mghari dlm bentuk sustained released sesuaikan dosis setiap interval 3 hari untuk menjaga serum level antara 10-15 μgml pantau ESO takikardi tremor nervous efek GI jika tidak ada perbaikan 1048774 hentikan teofilin dan 1048774go to step 4
bull Tahap 4 Coba dengan kortikosteroid prednison 30-40 mghari selama 2-4 minggu cek dengan spirometer (perbaikan ge 20) titrasi dosis ke dosis efektif terkecil (lt 10 μg sehari) pertimbangkan penggunaan kortikosteroid inhalasi 1048774 jika pasien tidak berespon baik 1048774 kembali ke steroid oral
Key points
bull 1048774PPOK adalah penyakit yang sebenarnya secara potensial dapat dicegah 1048774 stop smoking
bull 1048774Sekali PPOK terjadi 1048774 penderita akan memerlukan terapi yang kompleks 1048774 yang efikasinya masih diperdebatkan para ahli
bull 1048774Penyakit ini bersifat progresif dan ireversibel1048774 berbiaya besar baik baik personal maupun masyarakat
Difference between bronchitis and Difference between bronchitis and emphysemaemphysema
Productive cough
bronchitis
Classic sign
emphysema
Late in common with infection
Dyspnea Late in course CommonWheezing Intermittent MildHO smoking Common CommonBarrel chest Occasionally classicProlonged expiration Always present Always presentCyanosis Common UncommonChronic hypoventilation
Common Late in course
Ploycythemia Common Late in course
- COPDPPOM
- BRONCHITIS KRONIS atau COPD type B
- Etiologi
- Slide 4
- Slide 5
- CHRONIC BRONCHITIS
- Slide 7
- Slide 8
- VENTILATION COST
- Slide 10
- Emphysema or type A COPD
- Etiologi Emphysema
- Pathophysiology
- Slide 14
- Pathophysiology
- Slide 16
- Slide 17
- Slide 18
- Prognosis
- Tujuan Terapi
- NON FARMAKOLOGI
- Slide 22
- Slide 23
- Tahap terapi pada PPOK yang stabil
- Terapi antibiotika
- Slide 26
- Key points
- Difference between bronchitis and emphysema
-
Emphysema or type A COPD
DefinitionDefinition Abnormal permanent Abnormal permanent
enlargement of air spaces enlargement of air spaces distal to the terminal distal to the terminal bronchioles accompanied bronchioles accompanied by the destruction of the by the destruction of the walls and without obvious walls and without obvious fibrosisfibrosis
Emphysema is characterized Emphysema is characterized by loss of elasticity of the by loss of elasticity of the lung and abnormal lung and abnormal permanent enlargement of permanent enlargement of air spaces with destruction air spaces with destruction of the alveolar walls and of the alveolar walls and capillary beds capillary beds
EtiologiEmphysemaSmoking the primary risk factorLong-term smoking is responsible for 80-90 of casesProlonged exposures to harmful particles and gases from
passive smoke Industrial smoke Chemical gases vapors mists amp fumesDusts from grains minerals amp other materials
Alpha 1-antitrypsin deficiency gtgtemphysemaGeneticsBronchitisAsthma
Pathophysiology
Exposure to inhaled noxious particles amp gases inflammation imbalance of proteinases and anti-proteinases
Dilatation amp destruction +mucus secretion
FIG 1 Inflammatory mechanisms in COPD Cigarette smoke (and other irritants) activate macrophages in the respiratory tract that release neutrophil chemotactic factors including IL-8 and LTB4 These cells then release proteases that break down connective tissue in the lung parenchyma resulting in emphysema and also stimulate mucus hypersecretion These enzymes are normally counteracted by protease inhibitors including 1-antitrypsin SLPI and TIMP Cytotoxic T cells (CD8) may also be recruited and may be involved in alveolar wall destruction Fibroblasts may be activated by growthfactors releases from macrophages and epithelial cells CTG connective tissue growth factor COB chronic obstructive bronchiolitis
Pathophysiology
bull Affects alveolar membranendash Destruction of alveolar wallndash Loss of elastic recoilndash Over distended alveoli
bull Over distended alveolindash Damage to adjacent
pulmonary capillariesndash dead spacendash Impaired passive expiration
Impaired gas exchange
bull Impaired gas exchangendash impaired expiration
bull CO2 bull Hypercapniabull Respiratory acidosis
bull Damaged pulmonary capillary bedndash pulmonary pressure ndash work load for right ventricle
ndash Right side heart failure (due
to respiratory pressure) ndash Cor Pulmonale
16
SYMPTOMScough
sputumdyspnea
EXPOSURE TO RISKFACTORS
tobaccooccupation
indooroutdoor pollution
SPIROMETRY
Diagnosis of COPD
GAS DARAH ARTERILABORATORY TESTCHEST X-RAY
Spirometry Normal and COPDSpirometry Normal and COPD
0
5
1
4
2
3
Lite
r
1 65432
FVC
FVC
FEV1
FEV1
Normal
COPD
39005200
23504150 80
60 NormalCOPD
FVCFEV1 FVCFEV1
Seconds
Normally the left side of the heart produces a higher level of blood pressure in order to pump blood to the body the right side pumps blood through the lungs under much lower pressure Any condition that leads to prolonged high blood pressure in the arteries or veins of the lungs (called pulmonary hypertension) will be poorly tolerated by the right ventricle of the heart When this right ventricle fails or is unable toproperly pump against these abnormally high pressures this is called cor pulmonale
Prognosis
bull Indikator umur dan keparahanbull Jika ada hipoksia dan cor pulmonale
prognosis jelekbull Dyspnea obstruksi berat saluran nafas FEV1 lt 075 L (20) 1048774 angka kematian meningkat
50 pasien berisiko meninggal dalam waktu 5 tahun
Tujuan Terapi
bull Memperbaiki keadaan obstruksi saluran nafasbull Mencegah dan mengatasi eksaserbasi akutbull Menurunkan progresivitas penyakitbull Meningkatkan keadaan fisik dan psikisbull Menurunkan jumlah hari tidak masuk kerjabull Menurunkan lama tinggal di RSbull Menurunkan angka kematian
NON FARMAKOLOGI
bull Menghentikan kebiasaan merokokbull Rehabilitasi paru-paru secara komprehensif
dengan OR dan latihan pernafasanbull Perbaikan nutrisibull Tidak ada obat yang dapat menunda
memburuknya fungsi paru jika pasien tetap merokok
bull Kortikosteroid 1048774 benefit is very limited laporan tentang efektivitasnya masih bervariasi kecuali jika pasien juga memiliki riwayat asma
bull 1048774 Oksigen 1048774 untuk pasien hipoksemia cor pulmonale Digunakan jika baseline PaO2 turun sampai lt 55 mmHg
bull 1048774 Antibiotik 1048774 digunakan bila ada tanda infeksi bukan untuk maintenance therapy
bull 1048774 Vaksinasi 1048774 direkomendasikan untuk high-risk patients vaksin pneumococcus (tiap 5-10 th) dan vaksin influenza (tiap tahun)
bull 1048774 α1-proteinase inhibitor 1048774 utk pasien yang defisiensi α1- antitripsin 1048774 digunakan per minggu masih mahal 1048774 contoh Prolastin
Tahap terapi pada PPOK yang stabil
bull Tahap 1 Ipratropium bromida (MDI) atau nebulizer 2-6 puff 4 x sehari tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (mulut kering amp rasa pahit) jika hasil trial perbaikan FEV1 lt 20 1048774 step 2
bull Tahap 2 Tambahkan β-agonis MDI atau nebulizer tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (takikardi tremor) 1048774 jika tidak ada perkembangan hentikan β-agonis jika ada perbaikan tapi kecil 1048774 step 3
Terapi antibiotika
bull 1048774 Berdasarkan evidence terbaru yang tersedia antibiotika harus diberikan pada pasien-pasien PPOK yang
bull 1048774 Pasien dengan eksaserbasi akut dengan 3 tanda utama yaitu increased dyspnea increased sputum volume increased sputum purulence (Evidence B) atau
bull 1048774 Pasien dengan eksaserbasi akut dengan 2 tanda utama jika peningkatan purulensi sputum merupakan salah satunya (Evidence C)
bull 1048774 Pasien dengan eksaserbasi parah yang membutuhkan ventilasi mekanik baik invasif maupun non-infvasif (Evidence B)
bull Tahap 3 Tambah teofilinmulai dari 400 mghari dlm bentuk sustained released sesuaikan dosis setiap interval 3 hari untuk menjaga serum level antara 10-15 μgml pantau ESO takikardi tremor nervous efek GI jika tidak ada perbaikan 1048774 hentikan teofilin dan 1048774go to step 4
bull Tahap 4 Coba dengan kortikosteroid prednison 30-40 mghari selama 2-4 minggu cek dengan spirometer (perbaikan ge 20) titrasi dosis ke dosis efektif terkecil (lt 10 μg sehari) pertimbangkan penggunaan kortikosteroid inhalasi 1048774 jika pasien tidak berespon baik 1048774 kembali ke steroid oral
Key points
bull 1048774PPOK adalah penyakit yang sebenarnya secara potensial dapat dicegah 1048774 stop smoking
bull 1048774Sekali PPOK terjadi 1048774 penderita akan memerlukan terapi yang kompleks 1048774 yang efikasinya masih diperdebatkan para ahli
bull 1048774Penyakit ini bersifat progresif dan ireversibel1048774 berbiaya besar baik baik personal maupun masyarakat
Difference between bronchitis and Difference between bronchitis and emphysemaemphysema
Productive cough
bronchitis
Classic sign
emphysema
Late in common with infection
Dyspnea Late in course CommonWheezing Intermittent MildHO smoking Common CommonBarrel chest Occasionally classicProlonged expiration Always present Always presentCyanosis Common UncommonChronic hypoventilation
Common Late in course
Ploycythemia Common Late in course
- COPDPPOM
- BRONCHITIS KRONIS atau COPD type B
- Etiologi
- Slide 4
- Slide 5
- CHRONIC BRONCHITIS
- Slide 7
- Slide 8
- VENTILATION COST
- Slide 10
- Emphysema or type A COPD
- Etiologi Emphysema
- Pathophysiology
- Slide 14
- Pathophysiology
- Slide 16
- Slide 17
- Slide 18
- Prognosis
- Tujuan Terapi
- NON FARMAKOLOGI
- Slide 22
- Slide 23
- Tahap terapi pada PPOK yang stabil
- Terapi antibiotika
- Slide 26
- Key points
- Difference between bronchitis and emphysema
-
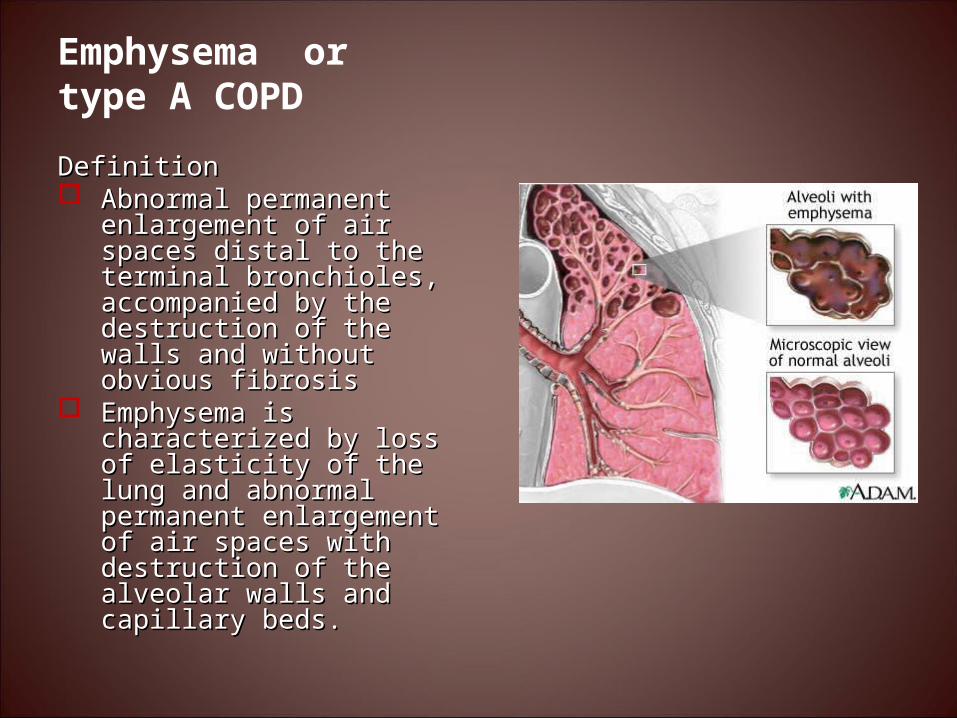
EtiologiEmphysemaSmoking the primary risk factorLong-term smoking is responsible for 80-90 of casesProlonged exposures to harmful particles and gases from
passive smoke Industrial smoke Chemical gases vapors mists amp fumesDusts from grains minerals amp other materials
Alpha 1-antitrypsin deficiency gtgtemphysemaGeneticsBronchitisAsthma
Pathophysiology
Exposure to inhaled noxious particles amp gases inflammation imbalance of proteinases and anti-proteinases
Dilatation amp destruction +mucus secretion
FIG 1 Inflammatory mechanisms in COPD Cigarette smoke (and other irritants) activate macrophages in the respiratory tract that release neutrophil chemotactic factors including IL-8 and LTB4 These cells then release proteases that break down connective tissue in the lung parenchyma resulting in emphysema and also stimulate mucus hypersecretion These enzymes are normally counteracted by protease inhibitors including 1-antitrypsin SLPI and TIMP Cytotoxic T cells (CD8) may also be recruited and may be involved in alveolar wall destruction Fibroblasts may be activated by growthfactors releases from macrophages and epithelial cells CTG connective tissue growth factor COB chronic obstructive bronchiolitis
Pathophysiology
bull Affects alveolar membranendash Destruction of alveolar wallndash Loss of elastic recoilndash Over distended alveoli
bull Over distended alveolindash Damage to adjacent
pulmonary capillariesndash dead spacendash Impaired passive expiration
Impaired gas exchange
bull Impaired gas exchangendash impaired expiration
bull CO2 bull Hypercapniabull Respiratory acidosis
bull Damaged pulmonary capillary bedndash pulmonary pressure ndash work load for right ventricle
ndash Right side heart failure (due
to respiratory pressure) ndash Cor Pulmonale
16
SYMPTOMScough
sputumdyspnea
EXPOSURE TO RISKFACTORS
tobaccooccupation
indooroutdoor pollution
SPIROMETRY
Diagnosis of COPD
GAS DARAH ARTERILABORATORY TESTCHEST X-RAY
Spirometry Normal and COPDSpirometry Normal and COPD
0
5
1
4
2
3
Lite
r
1 65432
FVC
FVC
FEV1
FEV1
Normal
COPD
39005200
23504150 80
60 NormalCOPD
FVCFEV1 FVCFEV1
Seconds
Normally the left side of the heart produces a higher level of blood pressure in order to pump blood to the body the right side pumps blood through the lungs under much lower pressure Any condition that leads to prolonged high blood pressure in the arteries or veins of the lungs (called pulmonary hypertension) will be poorly tolerated by the right ventricle of the heart When this right ventricle fails or is unable toproperly pump against these abnormally high pressures this is called cor pulmonale
Prognosis
bull Indikator umur dan keparahanbull Jika ada hipoksia dan cor pulmonale
prognosis jelekbull Dyspnea obstruksi berat saluran nafas FEV1 lt 075 L (20) 1048774 angka kematian meningkat
50 pasien berisiko meninggal dalam waktu 5 tahun
Tujuan Terapi
bull Memperbaiki keadaan obstruksi saluran nafasbull Mencegah dan mengatasi eksaserbasi akutbull Menurunkan progresivitas penyakitbull Meningkatkan keadaan fisik dan psikisbull Menurunkan jumlah hari tidak masuk kerjabull Menurunkan lama tinggal di RSbull Menurunkan angka kematian
NON FARMAKOLOGI
bull Menghentikan kebiasaan merokokbull Rehabilitasi paru-paru secara komprehensif
dengan OR dan latihan pernafasanbull Perbaikan nutrisibull Tidak ada obat yang dapat menunda
memburuknya fungsi paru jika pasien tetap merokok
bull Kortikosteroid 1048774 benefit is very limited laporan tentang efektivitasnya masih bervariasi kecuali jika pasien juga memiliki riwayat asma
bull 1048774 Oksigen 1048774 untuk pasien hipoksemia cor pulmonale Digunakan jika baseline PaO2 turun sampai lt 55 mmHg
bull 1048774 Antibiotik 1048774 digunakan bila ada tanda infeksi bukan untuk maintenance therapy
bull 1048774 Vaksinasi 1048774 direkomendasikan untuk high-risk patients vaksin pneumococcus (tiap 5-10 th) dan vaksin influenza (tiap tahun)
bull 1048774 α1-proteinase inhibitor 1048774 utk pasien yang defisiensi α1- antitripsin 1048774 digunakan per minggu masih mahal 1048774 contoh Prolastin
Tahap terapi pada PPOK yang stabil
bull Tahap 1 Ipratropium bromida (MDI) atau nebulizer 2-6 puff 4 x sehari tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (mulut kering amp rasa pahit) jika hasil trial perbaikan FEV1 lt 20 1048774 step 2
bull Tahap 2 Tambahkan β-agonis MDI atau nebulizer tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (takikardi tremor) 1048774 jika tidak ada perkembangan hentikan β-agonis jika ada perbaikan tapi kecil 1048774 step 3
Terapi antibiotika
bull 1048774 Berdasarkan evidence terbaru yang tersedia antibiotika harus diberikan pada pasien-pasien PPOK yang
bull 1048774 Pasien dengan eksaserbasi akut dengan 3 tanda utama yaitu increased dyspnea increased sputum volume increased sputum purulence (Evidence B) atau
bull 1048774 Pasien dengan eksaserbasi akut dengan 2 tanda utama jika peningkatan purulensi sputum merupakan salah satunya (Evidence C)
bull 1048774 Pasien dengan eksaserbasi parah yang membutuhkan ventilasi mekanik baik invasif maupun non-infvasif (Evidence B)
bull Tahap 3 Tambah teofilinmulai dari 400 mghari dlm bentuk sustained released sesuaikan dosis setiap interval 3 hari untuk menjaga serum level antara 10-15 μgml pantau ESO takikardi tremor nervous efek GI jika tidak ada perbaikan 1048774 hentikan teofilin dan 1048774go to step 4
bull Tahap 4 Coba dengan kortikosteroid prednison 30-40 mghari selama 2-4 minggu cek dengan spirometer (perbaikan ge 20) titrasi dosis ke dosis efektif terkecil (lt 10 μg sehari) pertimbangkan penggunaan kortikosteroid inhalasi 1048774 jika pasien tidak berespon baik 1048774 kembali ke steroid oral
Key points
bull 1048774PPOK adalah penyakit yang sebenarnya secara potensial dapat dicegah 1048774 stop smoking
bull 1048774Sekali PPOK terjadi 1048774 penderita akan memerlukan terapi yang kompleks 1048774 yang efikasinya masih diperdebatkan para ahli
bull 1048774Penyakit ini bersifat progresif dan ireversibel1048774 berbiaya besar baik baik personal maupun masyarakat
Difference between bronchitis and Difference between bronchitis and emphysemaemphysema
Productive cough
bronchitis
Classic sign
emphysema
Late in common with infection
Dyspnea Late in course CommonWheezing Intermittent MildHO smoking Common CommonBarrel chest Occasionally classicProlonged expiration Always present Always presentCyanosis Common UncommonChronic hypoventilation
Common Late in course
Ploycythemia Common Late in course
- COPDPPOM
- BRONCHITIS KRONIS atau COPD type B
- Etiologi
- Slide 4
- Slide 5
- CHRONIC BRONCHITIS
- Slide 7
- Slide 8
- VENTILATION COST
- Slide 10
- Emphysema or type A COPD
- Etiologi Emphysema
- Pathophysiology
- Slide 14
- Pathophysiology
- Slide 16
- Slide 17
- Slide 18
- Prognosis
- Tujuan Terapi
- NON FARMAKOLOGI
- Slide 22
- Slide 23
- Tahap terapi pada PPOK yang stabil
- Terapi antibiotika
- Slide 26
- Key points
- Difference between bronchitis and emphysema
-
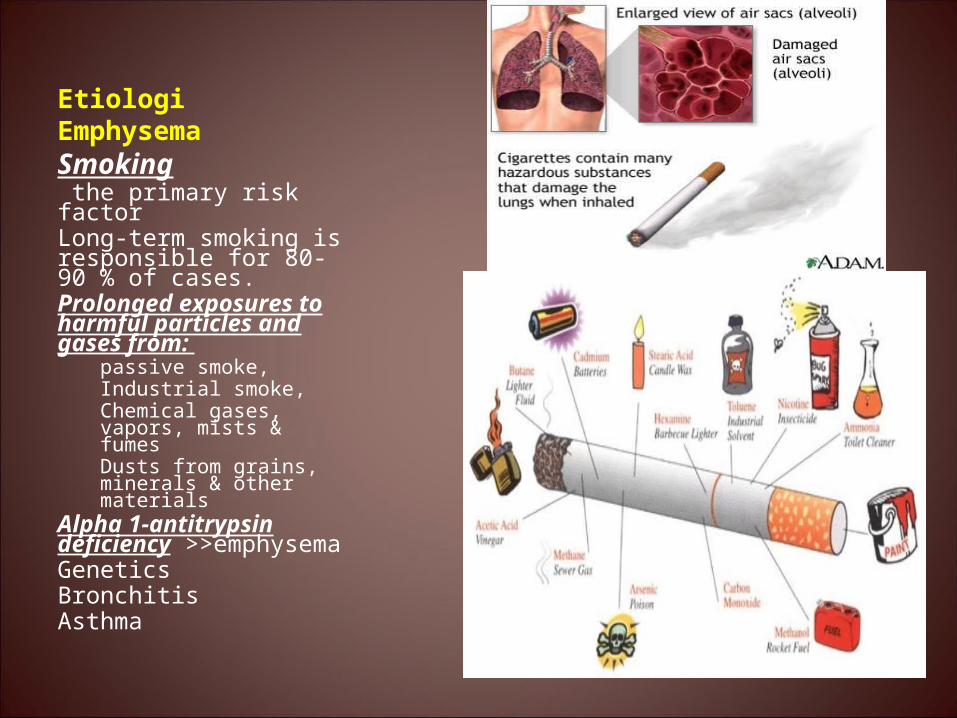
Pathophysiology
Exposure to inhaled noxious particles amp gases inflammation imbalance of proteinases and anti-proteinases
Dilatation amp destruction +mucus secretion
FIG 1 Inflammatory mechanisms in COPD Cigarette smoke (and other irritants) activate macrophages in the respiratory tract that release neutrophil chemotactic factors including IL-8 and LTB4 These cells then release proteases that break down connective tissue in the lung parenchyma resulting in emphysema and also stimulate mucus hypersecretion These enzymes are normally counteracted by protease inhibitors including 1-antitrypsin SLPI and TIMP Cytotoxic T cells (CD8) may also be recruited and may be involved in alveolar wall destruction Fibroblasts may be activated by growthfactors releases from macrophages and epithelial cells CTG connective tissue growth factor COB chronic obstructive bronchiolitis
Pathophysiology
bull Affects alveolar membranendash Destruction of alveolar wallndash Loss of elastic recoilndash Over distended alveoli
bull Over distended alveolindash Damage to adjacent
pulmonary capillariesndash dead spacendash Impaired passive expiration
Impaired gas exchange
bull Impaired gas exchangendash impaired expiration
bull CO2 bull Hypercapniabull Respiratory acidosis
bull Damaged pulmonary capillary bedndash pulmonary pressure ndash work load for right ventricle
ndash Right side heart failure (due
to respiratory pressure) ndash Cor Pulmonale
16
SYMPTOMScough
sputumdyspnea
EXPOSURE TO RISKFACTORS
tobaccooccupation
indooroutdoor pollution
SPIROMETRY
Diagnosis of COPD
GAS DARAH ARTERILABORATORY TESTCHEST X-RAY
Spirometry Normal and COPDSpirometry Normal and COPD
0
5
1
4
2
3
Lite
r
1 65432
FVC
FVC
FEV1
FEV1
Normal
COPD
39005200
23504150 80
60 NormalCOPD
FVCFEV1 FVCFEV1
Seconds
Normally the left side of the heart produces a higher level of blood pressure in order to pump blood to the body the right side pumps blood through the lungs under much lower pressure Any condition that leads to prolonged high blood pressure in the arteries or veins of the lungs (called pulmonary hypertension) will be poorly tolerated by the right ventricle of the heart When this right ventricle fails or is unable toproperly pump against these abnormally high pressures this is called cor pulmonale
Prognosis
bull Indikator umur dan keparahanbull Jika ada hipoksia dan cor pulmonale
prognosis jelekbull Dyspnea obstruksi berat saluran nafas FEV1 lt 075 L (20) 1048774 angka kematian meningkat
50 pasien berisiko meninggal dalam waktu 5 tahun
Tujuan Terapi
bull Memperbaiki keadaan obstruksi saluran nafasbull Mencegah dan mengatasi eksaserbasi akutbull Menurunkan progresivitas penyakitbull Meningkatkan keadaan fisik dan psikisbull Menurunkan jumlah hari tidak masuk kerjabull Menurunkan lama tinggal di RSbull Menurunkan angka kematian
NON FARMAKOLOGI
bull Menghentikan kebiasaan merokokbull Rehabilitasi paru-paru secara komprehensif
dengan OR dan latihan pernafasanbull Perbaikan nutrisibull Tidak ada obat yang dapat menunda
memburuknya fungsi paru jika pasien tetap merokok
bull Kortikosteroid 1048774 benefit is very limited laporan tentang efektivitasnya masih bervariasi kecuali jika pasien juga memiliki riwayat asma
bull 1048774 Oksigen 1048774 untuk pasien hipoksemia cor pulmonale Digunakan jika baseline PaO2 turun sampai lt 55 mmHg
bull 1048774 Antibiotik 1048774 digunakan bila ada tanda infeksi bukan untuk maintenance therapy
bull 1048774 Vaksinasi 1048774 direkomendasikan untuk high-risk patients vaksin pneumococcus (tiap 5-10 th) dan vaksin influenza (tiap tahun)
bull 1048774 α1-proteinase inhibitor 1048774 utk pasien yang defisiensi α1- antitripsin 1048774 digunakan per minggu masih mahal 1048774 contoh Prolastin
Tahap terapi pada PPOK yang stabil
bull Tahap 1 Ipratropium bromida (MDI) atau nebulizer 2-6 puff 4 x sehari tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (mulut kering amp rasa pahit) jika hasil trial perbaikan FEV1 lt 20 1048774 step 2
bull Tahap 2 Tambahkan β-agonis MDI atau nebulizer tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (takikardi tremor) 1048774 jika tidak ada perkembangan hentikan β-agonis jika ada perbaikan tapi kecil 1048774 step 3
Terapi antibiotika
bull 1048774 Berdasarkan evidence terbaru yang tersedia antibiotika harus diberikan pada pasien-pasien PPOK yang
bull 1048774 Pasien dengan eksaserbasi akut dengan 3 tanda utama yaitu increased dyspnea increased sputum volume increased sputum purulence (Evidence B) atau
bull 1048774 Pasien dengan eksaserbasi akut dengan 2 tanda utama jika peningkatan purulensi sputum merupakan salah satunya (Evidence C)
bull 1048774 Pasien dengan eksaserbasi parah yang membutuhkan ventilasi mekanik baik invasif maupun non-infvasif (Evidence B)
bull Tahap 3 Tambah teofilinmulai dari 400 mghari dlm bentuk sustained released sesuaikan dosis setiap interval 3 hari untuk menjaga serum level antara 10-15 μgml pantau ESO takikardi tremor nervous efek GI jika tidak ada perbaikan 1048774 hentikan teofilin dan 1048774go to step 4
bull Tahap 4 Coba dengan kortikosteroid prednison 30-40 mghari selama 2-4 minggu cek dengan spirometer (perbaikan ge 20) titrasi dosis ke dosis efektif terkecil (lt 10 μg sehari) pertimbangkan penggunaan kortikosteroid inhalasi 1048774 jika pasien tidak berespon baik 1048774 kembali ke steroid oral
Key points
bull 1048774PPOK adalah penyakit yang sebenarnya secara potensial dapat dicegah 1048774 stop smoking
bull 1048774Sekali PPOK terjadi 1048774 penderita akan memerlukan terapi yang kompleks 1048774 yang efikasinya masih diperdebatkan para ahli
bull 1048774Penyakit ini bersifat progresif dan ireversibel1048774 berbiaya besar baik baik personal maupun masyarakat
Difference between bronchitis and Difference between bronchitis and emphysemaemphysema
Productive cough
bronchitis
Classic sign
emphysema
Late in common with infection
Dyspnea Late in course CommonWheezing Intermittent MildHO smoking Common CommonBarrel chest Occasionally classicProlonged expiration Always present Always presentCyanosis Common UncommonChronic hypoventilation
Common Late in course
Ploycythemia Common Late in course
- COPDPPOM
- BRONCHITIS KRONIS atau COPD type B
- Etiologi
- Slide 4
- Slide 5
- CHRONIC BRONCHITIS
- Slide 7
- Slide 8
- VENTILATION COST
- Slide 10
- Emphysema or type A COPD
- Etiologi Emphysema
- Pathophysiology
- Slide 14
- Pathophysiology
- Slide 16
- Slide 17
- Slide 18
- Prognosis
- Tujuan Terapi
- NON FARMAKOLOGI
- Slide 22
- Slide 23
- Tahap terapi pada PPOK yang stabil
- Terapi antibiotika
- Slide 26
- Key points
- Difference between bronchitis and emphysema
-
FIG 1 Inflammatory mechanisms in COPD Cigarette smoke (and other irritants) activate macrophages in the respiratory tract that release neutrophil chemotactic factors including IL-8 and LTB4 These cells then release proteases that break down connective tissue in the lung parenchyma resulting in emphysema and also stimulate mucus hypersecretion These enzymes are normally counteracted by protease inhibitors including 1-antitrypsin SLPI and TIMP Cytotoxic T cells (CD8) may also be recruited and may be involved in alveolar wall destruction Fibroblasts may be activated by growthfactors releases from macrophages and epithelial cells CTG connective tissue growth factor COB chronic obstructive bronchiolitis
Pathophysiology
bull Affects alveolar membranendash Destruction of alveolar wallndash Loss of elastic recoilndash Over distended alveoli
bull Over distended alveolindash Damage to adjacent
pulmonary capillariesndash dead spacendash Impaired passive expiration
Impaired gas exchange
bull Impaired gas exchangendash impaired expiration
bull CO2 bull Hypercapniabull Respiratory acidosis
bull Damaged pulmonary capillary bedndash pulmonary pressure ndash work load for right ventricle
ndash Right side heart failure (due
to respiratory pressure) ndash Cor Pulmonale
16
SYMPTOMScough
sputumdyspnea
EXPOSURE TO RISKFACTORS
tobaccooccupation
indooroutdoor pollution
SPIROMETRY
Diagnosis of COPD
GAS DARAH ARTERILABORATORY TESTCHEST X-RAY
Spirometry Normal and COPDSpirometry Normal and COPD
0
5
1
4
2
3
Lite
r
1 65432
FVC
FVC
FEV1
FEV1
Normal
COPD
39005200
23504150 80
60 NormalCOPD
FVCFEV1 FVCFEV1
Seconds
Normally the left side of the heart produces a higher level of blood pressure in order to pump blood to the body the right side pumps blood through the lungs under much lower pressure Any condition that leads to prolonged high blood pressure in the arteries or veins of the lungs (called pulmonary hypertension) will be poorly tolerated by the right ventricle of the heart When this right ventricle fails or is unable toproperly pump against these abnormally high pressures this is called cor pulmonale
Prognosis
bull Indikator umur dan keparahanbull Jika ada hipoksia dan cor pulmonale
prognosis jelekbull Dyspnea obstruksi berat saluran nafas FEV1 lt 075 L (20) 1048774 angka kematian meningkat
50 pasien berisiko meninggal dalam waktu 5 tahun
Tujuan Terapi
bull Memperbaiki keadaan obstruksi saluran nafasbull Mencegah dan mengatasi eksaserbasi akutbull Menurunkan progresivitas penyakitbull Meningkatkan keadaan fisik dan psikisbull Menurunkan jumlah hari tidak masuk kerjabull Menurunkan lama tinggal di RSbull Menurunkan angka kematian
NON FARMAKOLOGI
bull Menghentikan kebiasaan merokokbull Rehabilitasi paru-paru secara komprehensif
dengan OR dan latihan pernafasanbull Perbaikan nutrisibull Tidak ada obat yang dapat menunda
memburuknya fungsi paru jika pasien tetap merokok
bull Kortikosteroid 1048774 benefit is very limited laporan tentang efektivitasnya masih bervariasi kecuali jika pasien juga memiliki riwayat asma
bull 1048774 Oksigen 1048774 untuk pasien hipoksemia cor pulmonale Digunakan jika baseline PaO2 turun sampai lt 55 mmHg
bull 1048774 Antibiotik 1048774 digunakan bila ada tanda infeksi bukan untuk maintenance therapy
bull 1048774 Vaksinasi 1048774 direkomendasikan untuk high-risk patients vaksin pneumococcus (tiap 5-10 th) dan vaksin influenza (tiap tahun)
bull 1048774 α1-proteinase inhibitor 1048774 utk pasien yang defisiensi α1- antitripsin 1048774 digunakan per minggu masih mahal 1048774 contoh Prolastin
Tahap terapi pada PPOK yang stabil
bull Tahap 1 Ipratropium bromida (MDI) atau nebulizer 2-6 puff 4 x sehari tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (mulut kering amp rasa pahit) jika hasil trial perbaikan FEV1 lt 20 1048774 step 2
bull Tahap 2 Tambahkan β-agonis MDI atau nebulizer tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (takikardi tremor) 1048774 jika tidak ada perkembangan hentikan β-agonis jika ada perbaikan tapi kecil 1048774 step 3
Terapi antibiotika
bull 1048774 Berdasarkan evidence terbaru yang tersedia antibiotika harus diberikan pada pasien-pasien PPOK yang
bull 1048774 Pasien dengan eksaserbasi akut dengan 3 tanda utama yaitu increased dyspnea increased sputum volume increased sputum purulence (Evidence B) atau
bull 1048774 Pasien dengan eksaserbasi akut dengan 2 tanda utama jika peningkatan purulensi sputum merupakan salah satunya (Evidence C)
bull 1048774 Pasien dengan eksaserbasi parah yang membutuhkan ventilasi mekanik baik invasif maupun non-infvasif (Evidence B)
bull Tahap 3 Tambah teofilinmulai dari 400 mghari dlm bentuk sustained released sesuaikan dosis setiap interval 3 hari untuk menjaga serum level antara 10-15 μgml pantau ESO takikardi tremor nervous efek GI jika tidak ada perbaikan 1048774 hentikan teofilin dan 1048774go to step 4
bull Tahap 4 Coba dengan kortikosteroid prednison 30-40 mghari selama 2-4 minggu cek dengan spirometer (perbaikan ge 20) titrasi dosis ke dosis efektif terkecil (lt 10 μg sehari) pertimbangkan penggunaan kortikosteroid inhalasi 1048774 jika pasien tidak berespon baik 1048774 kembali ke steroid oral
Key points
bull 1048774PPOK adalah penyakit yang sebenarnya secara potensial dapat dicegah 1048774 stop smoking
bull 1048774Sekali PPOK terjadi 1048774 penderita akan memerlukan terapi yang kompleks 1048774 yang efikasinya masih diperdebatkan para ahli
bull 1048774Penyakit ini bersifat progresif dan ireversibel1048774 berbiaya besar baik baik personal maupun masyarakat
Difference between bronchitis and Difference between bronchitis and emphysemaemphysema
Productive cough
bronchitis
Classic sign
emphysema
Late in common with infection
Dyspnea Late in course CommonWheezing Intermittent MildHO smoking Common CommonBarrel chest Occasionally classicProlonged expiration Always present Always presentCyanosis Common UncommonChronic hypoventilation
Common Late in course
Ploycythemia Common Late in course
- COPDPPOM
- BRONCHITIS KRONIS atau COPD type B
- Etiologi
- Slide 4
- Slide 5
- CHRONIC BRONCHITIS
- Slide 7
- Slide 8
- VENTILATION COST
- Slide 10
- Emphysema or type A COPD
- Etiologi Emphysema
- Pathophysiology
- Slide 14
- Pathophysiology
- Slide 16
- Slide 17
- Slide 18
- Prognosis
- Tujuan Terapi
- NON FARMAKOLOGI
- Slide 22
- Slide 23
- Tahap terapi pada PPOK yang stabil
- Terapi antibiotika
- Slide 26
- Key points
- Difference between bronchitis and emphysema
-
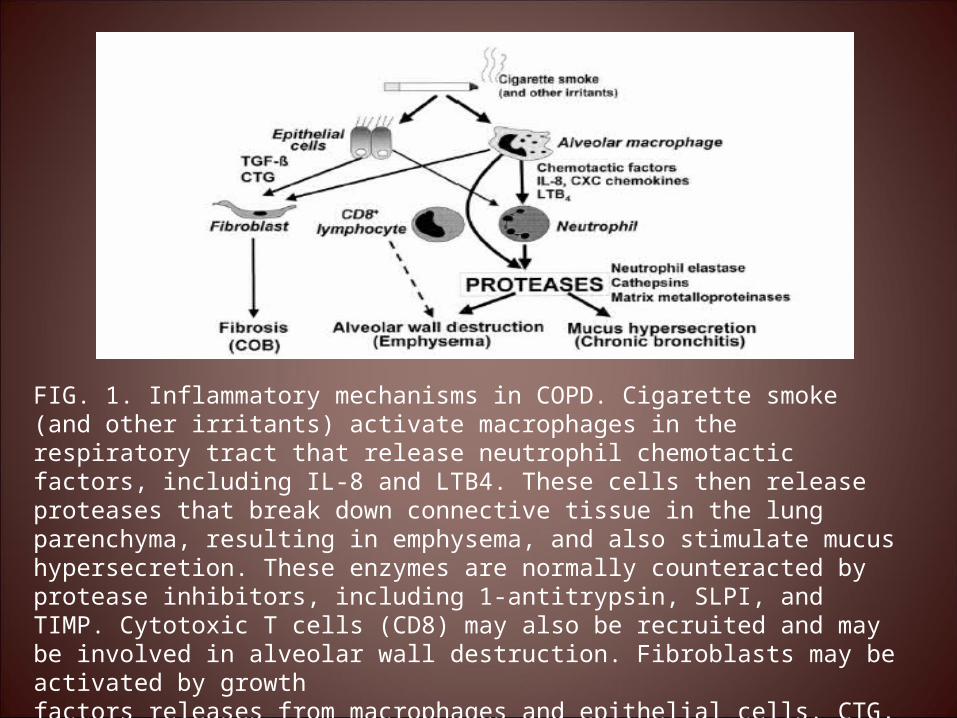
Pathophysiology
bull Affects alveolar membranendash Destruction of alveolar wallndash Loss of elastic recoilndash Over distended alveoli
bull Over distended alveolindash Damage to adjacent
pulmonary capillariesndash dead spacendash Impaired passive expiration
Impaired gas exchange
bull Impaired gas exchangendash impaired expiration
bull CO2 bull Hypercapniabull Respiratory acidosis
bull Damaged pulmonary capillary bedndash pulmonary pressure ndash work load for right ventricle
ndash Right side heart failure (due
to respiratory pressure) ndash Cor Pulmonale
16
SYMPTOMScough
sputumdyspnea
EXPOSURE TO RISKFACTORS
tobaccooccupation
indooroutdoor pollution
SPIROMETRY
Diagnosis of COPD
GAS DARAH ARTERILABORATORY TESTCHEST X-RAY
Spirometry Normal and COPDSpirometry Normal and COPD
0
5
1
4
2
3
Lite
r
1 65432
FVC
FVC
FEV1
FEV1
Normal
COPD
39005200
23504150 80
60 NormalCOPD
FVCFEV1 FVCFEV1
Seconds
Normally the left side of the heart produces a higher level of blood pressure in order to pump blood to the body the right side pumps blood through the lungs under much lower pressure Any condition that leads to prolonged high blood pressure in the arteries or veins of the lungs (called pulmonary hypertension) will be poorly tolerated by the right ventricle of the heart When this right ventricle fails or is unable toproperly pump against these abnormally high pressures this is called cor pulmonale
Prognosis
bull Indikator umur dan keparahanbull Jika ada hipoksia dan cor pulmonale
prognosis jelekbull Dyspnea obstruksi berat saluran nafas FEV1 lt 075 L (20) 1048774 angka kematian meningkat
50 pasien berisiko meninggal dalam waktu 5 tahun
Tujuan Terapi
bull Memperbaiki keadaan obstruksi saluran nafasbull Mencegah dan mengatasi eksaserbasi akutbull Menurunkan progresivitas penyakitbull Meningkatkan keadaan fisik dan psikisbull Menurunkan jumlah hari tidak masuk kerjabull Menurunkan lama tinggal di RSbull Menurunkan angka kematian
NON FARMAKOLOGI
bull Menghentikan kebiasaan merokokbull Rehabilitasi paru-paru secara komprehensif
dengan OR dan latihan pernafasanbull Perbaikan nutrisibull Tidak ada obat yang dapat menunda
memburuknya fungsi paru jika pasien tetap merokok
bull Kortikosteroid 1048774 benefit is very limited laporan tentang efektivitasnya masih bervariasi kecuali jika pasien juga memiliki riwayat asma
bull 1048774 Oksigen 1048774 untuk pasien hipoksemia cor pulmonale Digunakan jika baseline PaO2 turun sampai lt 55 mmHg
bull 1048774 Antibiotik 1048774 digunakan bila ada tanda infeksi bukan untuk maintenance therapy
bull 1048774 Vaksinasi 1048774 direkomendasikan untuk high-risk patients vaksin pneumococcus (tiap 5-10 th) dan vaksin influenza (tiap tahun)
bull 1048774 α1-proteinase inhibitor 1048774 utk pasien yang defisiensi α1- antitripsin 1048774 digunakan per minggu masih mahal 1048774 contoh Prolastin
Tahap terapi pada PPOK yang stabil
bull Tahap 1 Ipratropium bromida (MDI) atau nebulizer 2-6 puff 4 x sehari tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (mulut kering amp rasa pahit) jika hasil trial perbaikan FEV1 lt 20 1048774 step 2
bull Tahap 2 Tambahkan β-agonis MDI atau nebulizer tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (takikardi tremor) 1048774 jika tidak ada perkembangan hentikan β-agonis jika ada perbaikan tapi kecil 1048774 step 3
Terapi antibiotika
bull 1048774 Berdasarkan evidence terbaru yang tersedia antibiotika harus diberikan pada pasien-pasien PPOK yang
bull 1048774 Pasien dengan eksaserbasi akut dengan 3 tanda utama yaitu increased dyspnea increased sputum volume increased sputum purulence (Evidence B) atau
bull 1048774 Pasien dengan eksaserbasi akut dengan 2 tanda utama jika peningkatan purulensi sputum merupakan salah satunya (Evidence C)
bull 1048774 Pasien dengan eksaserbasi parah yang membutuhkan ventilasi mekanik baik invasif maupun non-infvasif (Evidence B)
bull Tahap 3 Tambah teofilinmulai dari 400 mghari dlm bentuk sustained released sesuaikan dosis setiap interval 3 hari untuk menjaga serum level antara 10-15 μgml pantau ESO takikardi tremor nervous efek GI jika tidak ada perbaikan 1048774 hentikan teofilin dan 1048774go to step 4
bull Tahap 4 Coba dengan kortikosteroid prednison 30-40 mghari selama 2-4 minggu cek dengan spirometer (perbaikan ge 20) titrasi dosis ke dosis efektif terkecil (lt 10 μg sehari) pertimbangkan penggunaan kortikosteroid inhalasi 1048774 jika pasien tidak berespon baik 1048774 kembali ke steroid oral
Key points
bull 1048774PPOK adalah penyakit yang sebenarnya secara potensial dapat dicegah 1048774 stop smoking
bull 1048774Sekali PPOK terjadi 1048774 penderita akan memerlukan terapi yang kompleks 1048774 yang efikasinya masih diperdebatkan para ahli
bull 1048774Penyakit ini bersifat progresif dan ireversibel1048774 berbiaya besar baik baik personal maupun masyarakat
Difference between bronchitis and Difference between bronchitis and emphysemaemphysema
Productive cough
bronchitis
Classic sign
emphysema
Late in common with infection
Dyspnea Late in course CommonWheezing Intermittent MildHO smoking Common CommonBarrel chest Occasionally classicProlonged expiration Always present Always presentCyanosis Common UncommonChronic hypoventilation
Common Late in course
Ploycythemia Common Late in course
- COPDPPOM
- BRONCHITIS KRONIS atau COPD type B
- Etiologi
- Slide 4
- Slide 5
- CHRONIC BRONCHITIS
- Slide 7
- Slide 8
- VENTILATION COST
- Slide 10
- Emphysema or type A COPD
- Etiologi Emphysema
- Pathophysiology
- Slide 14
- Pathophysiology
- Slide 16
- Slide 17
- Slide 18
- Prognosis
- Tujuan Terapi
- NON FARMAKOLOGI
- Slide 22
- Slide 23
- Tahap terapi pada PPOK yang stabil
- Terapi antibiotika
- Slide 26
- Key points
- Difference between bronchitis and emphysema
-
16
SYMPTOMScough
sputumdyspnea
EXPOSURE TO RISKFACTORS
tobaccooccupation
indooroutdoor pollution
SPIROMETRY
Diagnosis of COPD
GAS DARAH ARTERILABORATORY TESTCHEST X-RAY
Spirometry Normal and COPDSpirometry Normal and COPD
0
5
1
4
2
3
Lite
r
1 65432
FVC
FVC
FEV1
FEV1
Normal
COPD
39005200
23504150 80
60 NormalCOPD
FVCFEV1 FVCFEV1
Seconds
Normally the left side of the heart produces a higher level of blood pressure in order to pump blood to the body the right side pumps blood through the lungs under much lower pressure Any condition that leads to prolonged high blood pressure in the arteries or veins of the lungs (called pulmonary hypertension) will be poorly tolerated by the right ventricle of the heart When this right ventricle fails or is unable toproperly pump against these abnormally high pressures this is called cor pulmonale
Prognosis
bull Indikator umur dan keparahanbull Jika ada hipoksia dan cor pulmonale
prognosis jelekbull Dyspnea obstruksi berat saluran nafas FEV1 lt 075 L (20) 1048774 angka kematian meningkat
50 pasien berisiko meninggal dalam waktu 5 tahun
Tujuan Terapi
bull Memperbaiki keadaan obstruksi saluran nafasbull Mencegah dan mengatasi eksaserbasi akutbull Menurunkan progresivitas penyakitbull Meningkatkan keadaan fisik dan psikisbull Menurunkan jumlah hari tidak masuk kerjabull Menurunkan lama tinggal di RSbull Menurunkan angka kematian
NON FARMAKOLOGI
bull Menghentikan kebiasaan merokokbull Rehabilitasi paru-paru secara komprehensif
dengan OR dan latihan pernafasanbull Perbaikan nutrisibull Tidak ada obat yang dapat menunda
memburuknya fungsi paru jika pasien tetap merokok
bull Kortikosteroid 1048774 benefit is very limited laporan tentang efektivitasnya masih bervariasi kecuali jika pasien juga memiliki riwayat asma
bull 1048774 Oksigen 1048774 untuk pasien hipoksemia cor pulmonale Digunakan jika baseline PaO2 turun sampai lt 55 mmHg
bull 1048774 Antibiotik 1048774 digunakan bila ada tanda infeksi bukan untuk maintenance therapy
bull 1048774 Vaksinasi 1048774 direkomendasikan untuk high-risk patients vaksin pneumococcus (tiap 5-10 th) dan vaksin influenza (tiap tahun)
bull 1048774 α1-proteinase inhibitor 1048774 utk pasien yang defisiensi α1- antitripsin 1048774 digunakan per minggu masih mahal 1048774 contoh Prolastin
Tahap terapi pada PPOK yang stabil
bull Tahap 1 Ipratropium bromida (MDI) atau nebulizer 2-6 puff 4 x sehari tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (mulut kering amp rasa pahit) jika hasil trial perbaikan FEV1 lt 20 1048774 step 2
bull Tahap 2 Tambahkan β-agonis MDI atau nebulizer tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (takikardi tremor) 1048774 jika tidak ada perkembangan hentikan β-agonis jika ada perbaikan tapi kecil 1048774 step 3
Terapi antibiotika
bull 1048774 Berdasarkan evidence terbaru yang tersedia antibiotika harus diberikan pada pasien-pasien PPOK yang
bull 1048774 Pasien dengan eksaserbasi akut dengan 3 tanda utama yaitu increased dyspnea increased sputum volume increased sputum purulence (Evidence B) atau
bull 1048774 Pasien dengan eksaserbasi akut dengan 2 tanda utama jika peningkatan purulensi sputum merupakan salah satunya (Evidence C)
bull 1048774 Pasien dengan eksaserbasi parah yang membutuhkan ventilasi mekanik baik invasif maupun non-infvasif (Evidence B)
bull Tahap 3 Tambah teofilinmulai dari 400 mghari dlm bentuk sustained released sesuaikan dosis setiap interval 3 hari untuk menjaga serum level antara 10-15 μgml pantau ESO takikardi tremor nervous efek GI jika tidak ada perbaikan 1048774 hentikan teofilin dan 1048774go to step 4
bull Tahap 4 Coba dengan kortikosteroid prednison 30-40 mghari selama 2-4 minggu cek dengan spirometer (perbaikan ge 20) titrasi dosis ke dosis efektif terkecil (lt 10 μg sehari) pertimbangkan penggunaan kortikosteroid inhalasi 1048774 jika pasien tidak berespon baik 1048774 kembali ke steroid oral
Key points
bull 1048774PPOK adalah penyakit yang sebenarnya secara potensial dapat dicegah 1048774 stop smoking
bull 1048774Sekali PPOK terjadi 1048774 penderita akan memerlukan terapi yang kompleks 1048774 yang efikasinya masih diperdebatkan para ahli
bull 1048774Penyakit ini bersifat progresif dan ireversibel1048774 berbiaya besar baik baik personal maupun masyarakat
Difference between bronchitis and Difference between bronchitis and emphysemaemphysema
Productive cough
bronchitis
Classic sign
emphysema
Late in common with infection
Dyspnea Late in course CommonWheezing Intermittent MildHO smoking Common CommonBarrel chest Occasionally classicProlonged expiration Always present Always presentCyanosis Common UncommonChronic hypoventilation
Common Late in course
Ploycythemia Common Late in course
- COPDPPOM
- BRONCHITIS KRONIS atau COPD type B
- Etiologi
- Slide 4
- Slide 5
- CHRONIC BRONCHITIS
- Slide 7
- Slide 8
- VENTILATION COST
- Slide 10
- Emphysema or type A COPD
- Etiologi Emphysema
- Pathophysiology
- Slide 14
- Pathophysiology
- Slide 16
- Slide 17
- Slide 18
- Prognosis
- Tujuan Terapi
- NON FARMAKOLOGI
- Slide 22
- Slide 23
- Tahap terapi pada PPOK yang stabil
- Terapi antibiotika
- Slide 26
- Key points
- Difference between bronchitis and emphysema
-
Spirometry Normal and COPDSpirometry Normal and COPD
0
5
1
4
2
3
Lite
r
1 65432
FVC
FVC
FEV1
FEV1
Normal
COPD
39005200
23504150 80
60 NormalCOPD
FVCFEV1 FVCFEV1
Seconds
Normally the left side of the heart produces a higher level of blood pressure in order to pump blood to the body the right side pumps blood through the lungs under much lower pressure Any condition that leads to prolonged high blood pressure in the arteries or veins of the lungs (called pulmonary hypertension) will be poorly tolerated by the right ventricle of the heart When this right ventricle fails or is unable toproperly pump against these abnormally high pressures this is called cor pulmonale
Prognosis
bull Indikator umur dan keparahanbull Jika ada hipoksia dan cor pulmonale
prognosis jelekbull Dyspnea obstruksi berat saluran nafas FEV1 lt 075 L (20) 1048774 angka kematian meningkat
50 pasien berisiko meninggal dalam waktu 5 tahun
Tujuan Terapi
bull Memperbaiki keadaan obstruksi saluran nafasbull Mencegah dan mengatasi eksaserbasi akutbull Menurunkan progresivitas penyakitbull Meningkatkan keadaan fisik dan psikisbull Menurunkan jumlah hari tidak masuk kerjabull Menurunkan lama tinggal di RSbull Menurunkan angka kematian
NON FARMAKOLOGI
bull Menghentikan kebiasaan merokokbull Rehabilitasi paru-paru secara komprehensif
dengan OR dan latihan pernafasanbull Perbaikan nutrisibull Tidak ada obat yang dapat menunda
memburuknya fungsi paru jika pasien tetap merokok
bull Kortikosteroid 1048774 benefit is very limited laporan tentang efektivitasnya masih bervariasi kecuali jika pasien juga memiliki riwayat asma
bull 1048774 Oksigen 1048774 untuk pasien hipoksemia cor pulmonale Digunakan jika baseline PaO2 turun sampai lt 55 mmHg
bull 1048774 Antibiotik 1048774 digunakan bila ada tanda infeksi bukan untuk maintenance therapy
bull 1048774 Vaksinasi 1048774 direkomendasikan untuk high-risk patients vaksin pneumococcus (tiap 5-10 th) dan vaksin influenza (tiap tahun)
bull 1048774 α1-proteinase inhibitor 1048774 utk pasien yang defisiensi α1- antitripsin 1048774 digunakan per minggu masih mahal 1048774 contoh Prolastin
Tahap terapi pada PPOK yang stabil
bull Tahap 1 Ipratropium bromida (MDI) atau nebulizer 2-6 puff 4 x sehari tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (mulut kering amp rasa pahit) jika hasil trial perbaikan FEV1 lt 20 1048774 step 2
bull Tahap 2 Tambahkan β-agonis MDI atau nebulizer tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (takikardi tremor) 1048774 jika tidak ada perkembangan hentikan β-agonis jika ada perbaikan tapi kecil 1048774 step 3
Terapi antibiotika
bull 1048774 Berdasarkan evidence terbaru yang tersedia antibiotika harus diberikan pada pasien-pasien PPOK yang
bull 1048774 Pasien dengan eksaserbasi akut dengan 3 tanda utama yaitu increased dyspnea increased sputum volume increased sputum purulence (Evidence B) atau
bull 1048774 Pasien dengan eksaserbasi akut dengan 2 tanda utama jika peningkatan purulensi sputum merupakan salah satunya (Evidence C)
bull 1048774 Pasien dengan eksaserbasi parah yang membutuhkan ventilasi mekanik baik invasif maupun non-infvasif (Evidence B)
bull Tahap 3 Tambah teofilinmulai dari 400 mghari dlm bentuk sustained released sesuaikan dosis setiap interval 3 hari untuk menjaga serum level antara 10-15 μgml pantau ESO takikardi tremor nervous efek GI jika tidak ada perbaikan 1048774 hentikan teofilin dan 1048774go to step 4
bull Tahap 4 Coba dengan kortikosteroid prednison 30-40 mghari selama 2-4 minggu cek dengan spirometer (perbaikan ge 20) titrasi dosis ke dosis efektif terkecil (lt 10 μg sehari) pertimbangkan penggunaan kortikosteroid inhalasi 1048774 jika pasien tidak berespon baik 1048774 kembali ke steroid oral
Key points
bull 1048774PPOK adalah penyakit yang sebenarnya secara potensial dapat dicegah 1048774 stop smoking
bull 1048774Sekali PPOK terjadi 1048774 penderita akan memerlukan terapi yang kompleks 1048774 yang efikasinya masih diperdebatkan para ahli
bull 1048774Penyakit ini bersifat progresif dan ireversibel1048774 berbiaya besar baik baik personal maupun masyarakat
Difference between bronchitis and Difference between bronchitis and emphysemaemphysema
Productive cough
bronchitis
Classic sign
emphysema
Late in common with infection
Dyspnea Late in course CommonWheezing Intermittent MildHO smoking Common CommonBarrel chest Occasionally classicProlonged expiration Always present Always presentCyanosis Common UncommonChronic hypoventilation
Common Late in course
Ploycythemia Common Late in course
- COPDPPOM
- BRONCHITIS KRONIS atau COPD type B
- Etiologi
- Slide 4
- Slide 5
- CHRONIC BRONCHITIS
- Slide 7
- Slide 8
- VENTILATION COST
- Slide 10
- Emphysema or type A COPD
- Etiologi Emphysema
- Pathophysiology
- Slide 14
- Pathophysiology
- Slide 16
- Slide 17
- Slide 18
- Prognosis
- Tujuan Terapi
- NON FARMAKOLOGI
- Slide 22
- Slide 23
- Tahap terapi pada PPOK yang stabil
- Terapi antibiotika
- Slide 26
- Key points
- Difference between bronchitis and emphysema
-
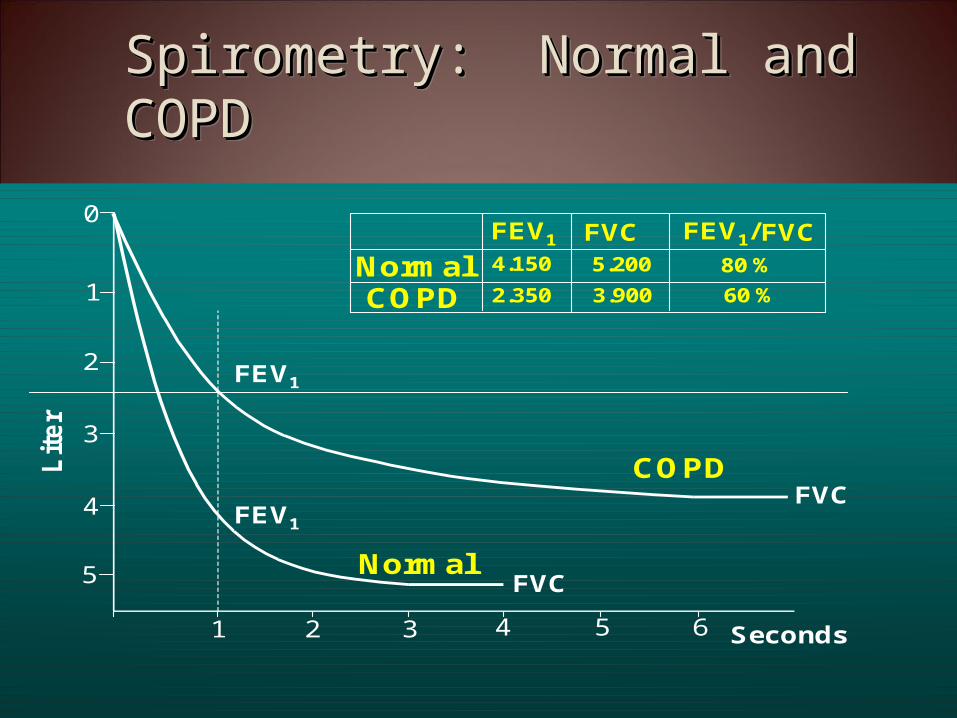
Normally the left side of the heart produces a higher level of blood pressure in order to pump blood to the body the right side pumps blood through the lungs under much lower pressure Any condition that leads to prolonged high blood pressure in the arteries or veins of the lungs (called pulmonary hypertension) will be poorly tolerated by the right ventricle of the heart When this right ventricle fails or is unable toproperly pump against these abnormally high pressures this is called cor pulmonale
Prognosis
bull Indikator umur dan keparahanbull Jika ada hipoksia dan cor pulmonale
prognosis jelekbull Dyspnea obstruksi berat saluran nafas FEV1 lt 075 L (20) 1048774 angka kematian meningkat
50 pasien berisiko meninggal dalam waktu 5 tahun
Tujuan Terapi
bull Memperbaiki keadaan obstruksi saluran nafasbull Mencegah dan mengatasi eksaserbasi akutbull Menurunkan progresivitas penyakitbull Meningkatkan keadaan fisik dan psikisbull Menurunkan jumlah hari tidak masuk kerjabull Menurunkan lama tinggal di RSbull Menurunkan angka kematian
NON FARMAKOLOGI
bull Menghentikan kebiasaan merokokbull Rehabilitasi paru-paru secara komprehensif
dengan OR dan latihan pernafasanbull Perbaikan nutrisibull Tidak ada obat yang dapat menunda
memburuknya fungsi paru jika pasien tetap merokok
bull Kortikosteroid 1048774 benefit is very limited laporan tentang efektivitasnya masih bervariasi kecuali jika pasien juga memiliki riwayat asma
bull 1048774 Oksigen 1048774 untuk pasien hipoksemia cor pulmonale Digunakan jika baseline PaO2 turun sampai lt 55 mmHg
bull 1048774 Antibiotik 1048774 digunakan bila ada tanda infeksi bukan untuk maintenance therapy
bull 1048774 Vaksinasi 1048774 direkomendasikan untuk high-risk patients vaksin pneumococcus (tiap 5-10 th) dan vaksin influenza (tiap tahun)
bull 1048774 α1-proteinase inhibitor 1048774 utk pasien yang defisiensi α1- antitripsin 1048774 digunakan per minggu masih mahal 1048774 contoh Prolastin
Tahap terapi pada PPOK yang stabil
bull Tahap 1 Ipratropium bromida (MDI) atau nebulizer 2-6 puff 4 x sehari tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (mulut kering amp rasa pahit) jika hasil trial perbaikan FEV1 lt 20 1048774 step 2
bull Tahap 2 Tambahkan β-agonis MDI atau nebulizer tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (takikardi tremor) 1048774 jika tidak ada perkembangan hentikan β-agonis jika ada perbaikan tapi kecil 1048774 step 3
Terapi antibiotika
bull 1048774 Berdasarkan evidence terbaru yang tersedia antibiotika harus diberikan pada pasien-pasien PPOK yang
bull 1048774 Pasien dengan eksaserbasi akut dengan 3 tanda utama yaitu increased dyspnea increased sputum volume increased sputum purulence (Evidence B) atau
bull 1048774 Pasien dengan eksaserbasi akut dengan 2 tanda utama jika peningkatan purulensi sputum merupakan salah satunya (Evidence C)
bull 1048774 Pasien dengan eksaserbasi parah yang membutuhkan ventilasi mekanik baik invasif maupun non-infvasif (Evidence B)
bull Tahap 3 Tambah teofilinmulai dari 400 mghari dlm bentuk sustained released sesuaikan dosis setiap interval 3 hari untuk menjaga serum level antara 10-15 μgml pantau ESO takikardi tremor nervous efek GI jika tidak ada perbaikan 1048774 hentikan teofilin dan 1048774go to step 4
bull Tahap 4 Coba dengan kortikosteroid prednison 30-40 mghari selama 2-4 minggu cek dengan spirometer (perbaikan ge 20) titrasi dosis ke dosis efektif terkecil (lt 10 μg sehari) pertimbangkan penggunaan kortikosteroid inhalasi 1048774 jika pasien tidak berespon baik 1048774 kembali ke steroid oral
Key points
bull 1048774PPOK adalah penyakit yang sebenarnya secara potensial dapat dicegah 1048774 stop smoking
bull 1048774Sekali PPOK terjadi 1048774 penderita akan memerlukan terapi yang kompleks 1048774 yang efikasinya masih diperdebatkan para ahli
bull 1048774Penyakit ini bersifat progresif dan ireversibel1048774 berbiaya besar baik baik personal maupun masyarakat
Difference between bronchitis and Difference between bronchitis and emphysemaemphysema
Productive cough
bronchitis
Classic sign
emphysema
Late in common with infection
Dyspnea Late in course CommonWheezing Intermittent MildHO smoking Common CommonBarrel chest Occasionally classicProlonged expiration Always present Always presentCyanosis Common UncommonChronic hypoventilation
Common Late in course
Ploycythemia Common Late in course
- COPDPPOM
- BRONCHITIS KRONIS atau COPD type B
- Etiologi
- Slide 4
- Slide 5
- CHRONIC BRONCHITIS
- Slide 7
- Slide 8
- VENTILATION COST
- Slide 10
- Emphysema or type A COPD
- Etiologi Emphysema
- Pathophysiology
- Slide 14
- Pathophysiology
- Slide 16
- Slide 17
- Slide 18
- Prognosis
- Tujuan Terapi
- NON FARMAKOLOGI
- Slide 22
- Slide 23
- Tahap terapi pada PPOK yang stabil
- Terapi antibiotika
- Slide 26
- Key points
- Difference between bronchitis and emphysema
-
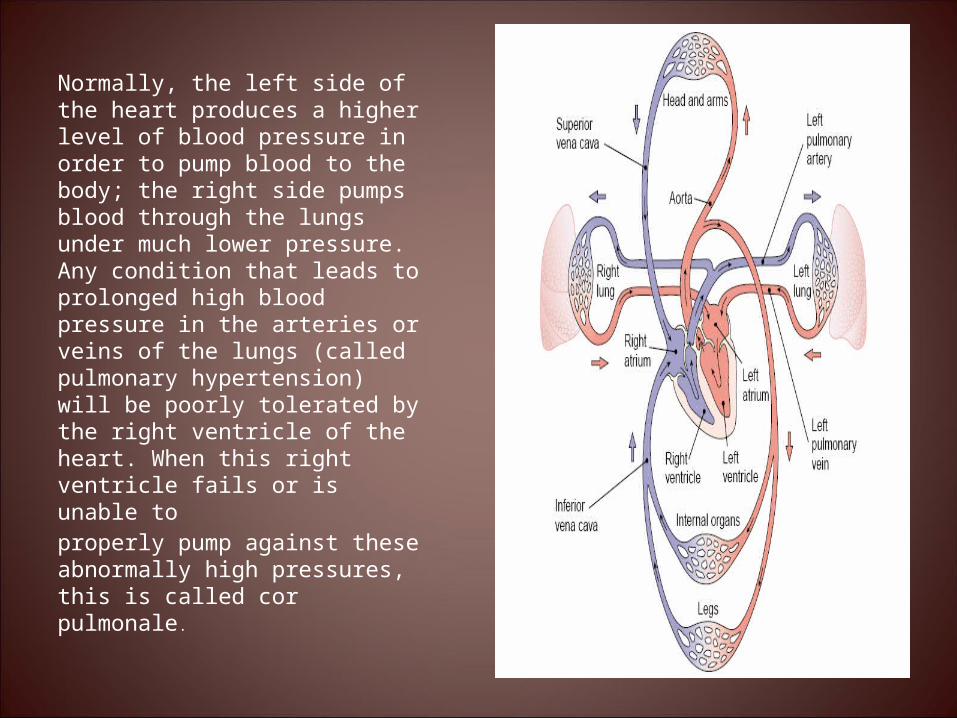
Prognosis
bull Indikator umur dan keparahanbull Jika ada hipoksia dan cor pulmonale
prognosis jelekbull Dyspnea obstruksi berat saluran nafas FEV1 lt 075 L (20) 1048774 angka kematian meningkat
50 pasien berisiko meninggal dalam waktu 5 tahun
Tujuan Terapi
bull Memperbaiki keadaan obstruksi saluran nafasbull Mencegah dan mengatasi eksaserbasi akutbull Menurunkan progresivitas penyakitbull Meningkatkan keadaan fisik dan psikisbull Menurunkan jumlah hari tidak masuk kerjabull Menurunkan lama tinggal di RSbull Menurunkan angka kematian
NON FARMAKOLOGI
bull Menghentikan kebiasaan merokokbull Rehabilitasi paru-paru secara komprehensif
dengan OR dan latihan pernafasanbull Perbaikan nutrisibull Tidak ada obat yang dapat menunda
memburuknya fungsi paru jika pasien tetap merokok
bull Kortikosteroid 1048774 benefit is very limited laporan tentang efektivitasnya masih bervariasi kecuali jika pasien juga memiliki riwayat asma
bull 1048774 Oksigen 1048774 untuk pasien hipoksemia cor pulmonale Digunakan jika baseline PaO2 turun sampai lt 55 mmHg
bull 1048774 Antibiotik 1048774 digunakan bila ada tanda infeksi bukan untuk maintenance therapy
bull 1048774 Vaksinasi 1048774 direkomendasikan untuk high-risk patients vaksin pneumococcus (tiap 5-10 th) dan vaksin influenza (tiap tahun)
bull 1048774 α1-proteinase inhibitor 1048774 utk pasien yang defisiensi α1- antitripsin 1048774 digunakan per minggu masih mahal 1048774 contoh Prolastin
Tahap terapi pada PPOK yang stabil
bull Tahap 1 Ipratropium bromida (MDI) atau nebulizer 2-6 puff 4 x sehari tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (mulut kering amp rasa pahit) jika hasil trial perbaikan FEV1 lt 20 1048774 step 2
bull Tahap 2 Tambahkan β-agonis MDI atau nebulizer tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (takikardi tremor) 1048774 jika tidak ada perkembangan hentikan β-agonis jika ada perbaikan tapi kecil 1048774 step 3
Terapi antibiotika
bull 1048774 Berdasarkan evidence terbaru yang tersedia antibiotika harus diberikan pada pasien-pasien PPOK yang
bull 1048774 Pasien dengan eksaserbasi akut dengan 3 tanda utama yaitu increased dyspnea increased sputum volume increased sputum purulence (Evidence B) atau
bull 1048774 Pasien dengan eksaserbasi akut dengan 2 tanda utama jika peningkatan purulensi sputum merupakan salah satunya (Evidence C)
bull 1048774 Pasien dengan eksaserbasi parah yang membutuhkan ventilasi mekanik baik invasif maupun non-infvasif (Evidence B)
bull Tahap 3 Tambah teofilinmulai dari 400 mghari dlm bentuk sustained released sesuaikan dosis setiap interval 3 hari untuk menjaga serum level antara 10-15 μgml pantau ESO takikardi tremor nervous efek GI jika tidak ada perbaikan 1048774 hentikan teofilin dan 1048774go to step 4
bull Tahap 4 Coba dengan kortikosteroid prednison 30-40 mghari selama 2-4 minggu cek dengan spirometer (perbaikan ge 20) titrasi dosis ke dosis efektif terkecil (lt 10 μg sehari) pertimbangkan penggunaan kortikosteroid inhalasi 1048774 jika pasien tidak berespon baik 1048774 kembali ke steroid oral
Key points
bull 1048774PPOK adalah penyakit yang sebenarnya secara potensial dapat dicegah 1048774 stop smoking
bull 1048774Sekali PPOK terjadi 1048774 penderita akan memerlukan terapi yang kompleks 1048774 yang efikasinya masih diperdebatkan para ahli
bull 1048774Penyakit ini bersifat progresif dan ireversibel1048774 berbiaya besar baik baik personal maupun masyarakat
Difference between bronchitis and Difference between bronchitis and emphysemaemphysema
Productive cough
bronchitis
Classic sign
emphysema
Late in common with infection
Dyspnea Late in course CommonWheezing Intermittent MildHO smoking Common CommonBarrel chest Occasionally classicProlonged expiration Always present Always presentCyanosis Common UncommonChronic hypoventilation
Common Late in course
Ploycythemia Common Late in course
- COPDPPOM
- BRONCHITIS KRONIS atau COPD type B
- Etiologi
- Slide 4
- Slide 5
- CHRONIC BRONCHITIS
- Slide 7
- Slide 8
- VENTILATION COST
- Slide 10
- Emphysema or type A COPD
- Etiologi Emphysema
- Pathophysiology
- Slide 14
- Pathophysiology
- Slide 16
- Slide 17
- Slide 18
- Prognosis
- Tujuan Terapi
- NON FARMAKOLOGI
- Slide 22
- Slide 23
- Tahap terapi pada PPOK yang stabil
- Terapi antibiotika
- Slide 26
- Key points
- Difference between bronchitis and emphysema
-
Tujuan Terapi
bull Memperbaiki keadaan obstruksi saluran nafasbull Mencegah dan mengatasi eksaserbasi akutbull Menurunkan progresivitas penyakitbull Meningkatkan keadaan fisik dan psikisbull Menurunkan jumlah hari tidak masuk kerjabull Menurunkan lama tinggal di RSbull Menurunkan angka kematian
NON FARMAKOLOGI
bull Menghentikan kebiasaan merokokbull Rehabilitasi paru-paru secara komprehensif
dengan OR dan latihan pernafasanbull Perbaikan nutrisibull Tidak ada obat yang dapat menunda
memburuknya fungsi paru jika pasien tetap merokok
bull Kortikosteroid 1048774 benefit is very limited laporan tentang efektivitasnya masih bervariasi kecuali jika pasien juga memiliki riwayat asma
bull 1048774 Oksigen 1048774 untuk pasien hipoksemia cor pulmonale Digunakan jika baseline PaO2 turun sampai lt 55 mmHg
bull 1048774 Antibiotik 1048774 digunakan bila ada tanda infeksi bukan untuk maintenance therapy
bull 1048774 Vaksinasi 1048774 direkomendasikan untuk high-risk patients vaksin pneumococcus (tiap 5-10 th) dan vaksin influenza (tiap tahun)
bull 1048774 α1-proteinase inhibitor 1048774 utk pasien yang defisiensi α1- antitripsin 1048774 digunakan per minggu masih mahal 1048774 contoh Prolastin
Tahap terapi pada PPOK yang stabil
bull Tahap 1 Ipratropium bromida (MDI) atau nebulizer 2-6 puff 4 x sehari tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (mulut kering amp rasa pahit) jika hasil trial perbaikan FEV1 lt 20 1048774 step 2
bull Tahap 2 Tambahkan β-agonis MDI atau nebulizer tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (takikardi tremor) 1048774 jika tidak ada perkembangan hentikan β-agonis jika ada perbaikan tapi kecil 1048774 step 3
Terapi antibiotika
bull 1048774 Berdasarkan evidence terbaru yang tersedia antibiotika harus diberikan pada pasien-pasien PPOK yang
bull 1048774 Pasien dengan eksaserbasi akut dengan 3 tanda utama yaitu increased dyspnea increased sputum volume increased sputum purulence (Evidence B) atau
bull 1048774 Pasien dengan eksaserbasi akut dengan 2 tanda utama jika peningkatan purulensi sputum merupakan salah satunya (Evidence C)
bull 1048774 Pasien dengan eksaserbasi parah yang membutuhkan ventilasi mekanik baik invasif maupun non-infvasif (Evidence B)
bull Tahap 3 Tambah teofilinmulai dari 400 mghari dlm bentuk sustained released sesuaikan dosis setiap interval 3 hari untuk menjaga serum level antara 10-15 μgml pantau ESO takikardi tremor nervous efek GI jika tidak ada perbaikan 1048774 hentikan teofilin dan 1048774go to step 4
bull Tahap 4 Coba dengan kortikosteroid prednison 30-40 mghari selama 2-4 minggu cek dengan spirometer (perbaikan ge 20) titrasi dosis ke dosis efektif terkecil (lt 10 μg sehari) pertimbangkan penggunaan kortikosteroid inhalasi 1048774 jika pasien tidak berespon baik 1048774 kembali ke steroid oral
Key points
bull 1048774PPOK adalah penyakit yang sebenarnya secara potensial dapat dicegah 1048774 stop smoking
bull 1048774Sekali PPOK terjadi 1048774 penderita akan memerlukan terapi yang kompleks 1048774 yang efikasinya masih diperdebatkan para ahli
bull 1048774Penyakit ini bersifat progresif dan ireversibel1048774 berbiaya besar baik baik personal maupun masyarakat
Difference between bronchitis and Difference between bronchitis and emphysemaemphysema
Productive cough
bronchitis
Classic sign
emphysema
Late in common with infection
Dyspnea Late in course CommonWheezing Intermittent MildHO smoking Common CommonBarrel chest Occasionally classicProlonged expiration Always present Always presentCyanosis Common UncommonChronic hypoventilation
Common Late in course
Ploycythemia Common Late in course
- COPDPPOM
- BRONCHITIS KRONIS atau COPD type B
- Etiologi
- Slide 4
- Slide 5
- CHRONIC BRONCHITIS
- Slide 7
- Slide 8
- VENTILATION COST
- Slide 10
- Emphysema or type A COPD
- Etiologi Emphysema
- Pathophysiology
- Slide 14
- Pathophysiology
- Slide 16
- Slide 17
- Slide 18
- Prognosis
- Tujuan Terapi
- NON FARMAKOLOGI
- Slide 22
- Slide 23
- Tahap terapi pada PPOK yang stabil
- Terapi antibiotika
- Slide 26
- Key points
- Difference between bronchitis and emphysema
-
NON FARMAKOLOGI
bull Menghentikan kebiasaan merokokbull Rehabilitasi paru-paru secara komprehensif
dengan OR dan latihan pernafasanbull Perbaikan nutrisibull Tidak ada obat yang dapat menunda
memburuknya fungsi paru jika pasien tetap merokok
bull Kortikosteroid 1048774 benefit is very limited laporan tentang efektivitasnya masih bervariasi kecuali jika pasien juga memiliki riwayat asma
bull 1048774 Oksigen 1048774 untuk pasien hipoksemia cor pulmonale Digunakan jika baseline PaO2 turun sampai lt 55 mmHg
bull 1048774 Antibiotik 1048774 digunakan bila ada tanda infeksi bukan untuk maintenance therapy
bull 1048774 Vaksinasi 1048774 direkomendasikan untuk high-risk patients vaksin pneumococcus (tiap 5-10 th) dan vaksin influenza (tiap tahun)
bull 1048774 α1-proteinase inhibitor 1048774 utk pasien yang defisiensi α1- antitripsin 1048774 digunakan per minggu masih mahal 1048774 contoh Prolastin
Tahap terapi pada PPOK yang stabil
bull Tahap 1 Ipratropium bromida (MDI) atau nebulizer 2-6 puff 4 x sehari tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (mulut kering amp rasa pahit) jika hasil trial perbaikan FEV1 lt 20 1048774 step 2
bull Tahap 2 Tambahkan β-agonis MDI atau nebulizer tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (takikardi tremor) 1048774 jika tidak ada perkembangan hentikan β-agonis jika ada perbaikan tapi kecil 1048774 step 3
Terapi antibiotika
bull 1048774 Berdasarkan evidence terbaru yang tersedia antibiotika harus diberikan pada pasien-pasien PPOK yang
bull 1048774 Pasien dengan eksaserbasi akut dengan 3 tanda utama yaitu increased dyspnea increased sputum volume increased sputum purulence (Evidence B) atau
bull 1048774 Pasien dengan eksaserbasi akut dengan 2 tanda utama jika peningkatan purulensi sputum merupakan salah satunya (Evidence C)
bull 1048774 Pasien dengan eksaserbasi parah yang membutuhkan ventilasi mekanik baik invasif maupun non-infvasif (Evidence B)
bull Tahap 3 Tambah teofilinmulai dari 400 mghari dlm bentuk sustained released sesuaikan dosis setiap interval 3 hari untuk menjaga serum level antara 10-15 μgml pantau ESO takikardi tremor nervous efek GI jika tidak ada perbaikan 1048774 hentikan teofilin dan 1048774go to step 4
bull Tahap 4 Coba dengan kortikosteroid prednison 30-40 mghari selama 2-4 minggu cek dengan spirometer (perbaikan ge 20) titrasi dosis ke dosis efektif terkecil (lt 10 μg sehari) pertimbangkan penggunaan kortikosteroid inhalasi 1048774 jika pasien tidak berespon baik 1048774 kembali ke steroid oral
Key points
bull 1048774PPOK adalah penyakit yang sebenarnya secara potensial dapat dicegah 1048774 stop smoking
bull 1048774Sekali PPOK terjadi 1048774 penderita akan memerlukan terapi yang kompleks 1048774 yang efikasinya masih diperdebatkan para ahli
bull 1048774Penyakit ini bersifat progresif dan ireversibel1048774 berbiaya besar baik baik personal maupun masyarakat
Difference between bronchitis and Difference between bronchitis and emphysemaemphysema
Productive cough
bronchitis
Classic sign
emphysema
Late in common with infection
Dyspnea Late in course CommonWheezing Intermittent MildHO smoking Common CommonBarrel chest Occasionally classicProlonged expiration Always present Always presentCyanosis Common UncommonChronic hypoventilation
Common Late in course
Ploycythemia Common Late in course
- COPDPPOM
- BRONCHITIS KRONIS atau COPD type B
- Etiologi
- Slide 4
- Slide 5
- CHRONIC BRONCHITIS
- Slide 7
- Slide 8
- VENTILATION COST
- Slide 10
- Emphysema or type A COPD
- Etiologi Emphysema
- Pathophysiology
- Slide 14
- Pathophysiology
- Slide 16
- Slide 17
- Slide 18
- Prognosis
- Tujuan Terapi
- NON FARMAKOLOGI
- Slide 22
- Slide 23
- Tahap terapi pada PPOK yang stabil
- Terapi antibiotika
- Slide 26
- Key points
- Difference between bronchitis and emphysema
-
bull Kortikosteroid 1048774 benefit is very limited laporan tentang efektivitasnya masih bervariasi kecuali jika pasien juga memiliki riwayat asma
bull 1048774 Oksigen 1048774 untuk pasien hipoksemia cor pulmonale Digunakan jika baseline PaO2 turun sampai lt 55 mmHg
bull 1048774 Antibiotik 1048774 digunakan bila ada tanda infeksi bukan untuk maintenance therapy
bull 1048774 Vaksinasi 1048774 direkomendasikan untuk high-risk patients vaksin pneumococcus (tiap 5-10 th) dan vaksin influenza (tiap tahun)
bull 1048774 α1-proteinase inhibitor 1048774 utk pasien yang defisiensi α1- antitripsin 1048774 digunakan per minggu masih mahal 1048774 contoh Prolastin
Tahap terapi pada PPOK yang stabil
bull Tahap 1 Ipratropium bromida (MDI) atau nebulizer 2-6 puff 4 x sehari tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (mulut kering amp rasa pahit) jika hasil trial perbaikan FEV1 lt 20 1048774 step 2
bull Tahap 2 Tambahkan β-agonis MDI atau nebulizer tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (takikardi tremor) 1048774 jika tidak ada perkembangan hentikan β-agonis jika ada perbaikan tapi kecil 1048774 step 3
Terapi antibiotika
bull 1048774 Berdasarkan evidence terbaru yang tersedia antibiotika harus diberikan pada pasien-pasien PPOK yang
bull 1048774 Pasien dengan eksaserbasi akut dengan 3 tanda utama yaitu increased dyspnea increased sputum volume increased sputum purulence (Evidence B) atau
bull 1048774 Pasien dengan eksaserbasi akut dengan 2 tanda utama jika peningkatan purulensi sputum merupakan salah satunya (Evidence C)
bull 1048774 Pasien dengan eksaserbasi parah yang membutuhkan ventilasi mekanik baik invasif maupun non-infvasif (Evidence B)
bull Tahap 3 Tambah teofilinmulai dari 400 mghari dlm bentuk sustained released sesuaikan dosis setiap interval 3 hari untuk menjaga serum level antara 10-15 μgml pantau ESO takikardi tremor nervous efek GI jika tidak ada perbaikan 1048774 hentikan teofilin dan 1048774go to step 4
bull Tahap 4 Coba dengan kortikosteroid prednison 30-40 mghari selama 2-4 minggu cek dengan spirometer (perbaikan ge 20) titrasi dosis ke dosis efektif terkecil (lt 10 μg sehari) pertimbangkan penggunaan kortikosteroid inhalasi 1048774 jika pasien tidak berespon baik 1048774 kembali ke steroid oral
Key points
bull 1048774PPOK adalah penyakit yang sebenarnya secara potensial dapat dicegah 1048774 stop smoking
bull 1048774Sekali PPOK terjadi 1048774 penderita akan memerlukan terapi yang kompleks 1048774 yang efikasinya masih diperdebatkan para ahli
bull 1048774Penyakit ini bersifat progresif dan ireversibel1048774 berbiaya besar baik baik personal maupun masyarakat
Difference between bronchitis and Difference between bronchitis and emphysemaemphysema
Productive cough
bronchitis
Classic sign
emphysema
Late in common with infection
Dyspnea Late in course CommonWheezing Intermittent MildHO smoking Common CommonBarrel chest Occasionally classicProlonged expiration Always present Always presentCyanosis Common UncommonChronic hypoventilation
Common Late in course
Ploycythemia Common Late in course
- COPDPPOM
- BRONCHITIS KRONIS atau COPD type B
- Etiologi
- Slide 4
- Slide 5
- CHRONIC BRONCHITIS
- Slide 7
- Slide 8
- VENTILATION COST
- Slide 10
- Emphysema or type A COPD
- Etiologi Emphysema
- Pathophysiology
- Slide 14
- Pathophysiology
- Slide 16
- Slide 17
- Slide 18
- Prognosis
- Tujuan Terapi
- NON FARMAKOLOGI
- Slide 22
- Slide 23
- Tahap terapi pada PPOK yang stabil
- Terapi antibiotika
- Slide 26
- Key points
- Difference between bronchitis and emphysema
-
Tahap terapi pada PPOK yang stabil
bull Tahap 1 Ipratropium bromida (MDI) atau nebulizer 2-6 puff 4 x sehari tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (mulut kering amp rasa pahit) jika hasil trial perbaikan FEV1 lt 20 1048774 step 2
bull Tahap 2 Tambahkan β-agonis MDI atau nebulizer tunjukkan cara penggunaan yang tepat advis pasien ttg pentingnya penggunaan teratur dan efek samping yg mungkin timbul (takikardi tremor) 1048774 jika tidak ada perkembangan hentikan β-agonis jika ada perbaikan tapi kecil 1048774 step 3
Terapi antibiotika
bull 1048774 Berdasarkan evidence terbaru yang tersedia antibiotika harus diberikan pada pasien-pasien PPOK yang
bull 1048774 Pasien dengan eksaserbasi akut dengan 3 tanda utama yaitu increased dyspnea increased sputum volume increased sputum purulence (Evidence B) atau
bull 1048774 Pasien dengan eksaserbasi akut dengan 2 tanda utama jika peningkatan purulensi sputum merupakan salah satunya (Evidence C)
bull 1048774 Pasien dengan eksaserbasi parah yang membutuhkan ventilasi mekanik baik invasif maupun non-infvasif (Evidence B)
bull Tahap 3 Tambah teofilinmulai dari 400 mghari dlm bentuk sustained released sesuaikan dosis setiap interval 3 hari untuk menjaga serum level antara 10-15 μgml pantau ESO takikardi tremor nervous efek GI jika tidak ada perbaikan 1048774 hentikan teofilin dan 1048774go to step 4
bull Tahap 4 Coba dengan kortikosteroid prednison 30-40 mghari selama 2-4 minggu cek dengan spirometer (perbaikan ge 20) titrasi dosis ke dosis efektif terkecil (lt 10 μg sehari) pertimbangkan penggunaan kortikosteroid inhalasi 1048774 jika pasien tidak berespon baik 1048774 kembali ke steroid oral
Key points
bull 1048774PPOK adalah penyakit yang sebenarnya secara potensial dapat dicegah 1048774 stop smoking
bull 1048774Sekali PPOK terjadi 1048774 penderita akan memerlukan terapi yang kompleks 1048774 yang efikasinya masih diperdebatkan para ahli
bull 1048774Penyakit ini bersifat progresif dan ireversibel1048774 berbiaya besar baik baik personal maupun masyarakat
Difference between bronchitis and Difference between bronchitis and emphysemaemphysema
Productive cough
bronchitis
Classic sign
emphysema
Late in common with infection
Dyspnea Late in course CommonWheezing Intermittent MildHO smoking Common CommonBarrel chest Occasionally classicProlonged expiration Always present Always presentCyanosis Common UncommonChronic hypoventilation
Common Late in course
Ploycythemia Common Late in course
- COPDPPOM
- BRONCHITIS KRONIS atau COPD type B
- Etiologi
- Slide 4
- Slide 5
- CHRONIC BRONCHITIS
- Slide 7
- Slide 8
- VENTILATION COST
- Slide 10
- Emphysema or type A COPD
- Etiologi Emphysema
- Pathophysiology
- Slide 14
- Pathophysiology
- Slide 16
- Slide 17
- Slide 18
- Prognosis
- Tujuan Terapi
- NON FARMAKOLOGI
- Slide 22
- Slide 23
- Tahap terapi pada PPOK yang stabil
- Terapi antibiotika
- Slide 26
- Key points
- Difference between bronchitis and emphysema
-
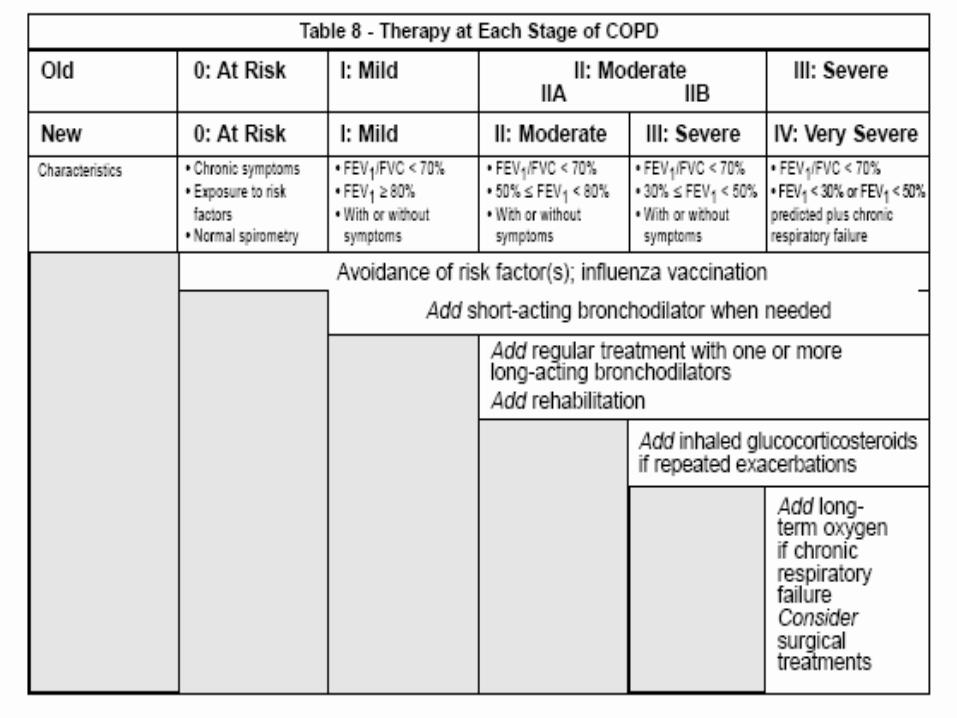
Terapi antibiotika
bull 1048774 Berdasarkan evidence terbaru yang tersedia antibiotika harus diberikan pada pasien-pasien PPOK yang
bull 1048774 Pasien dengan eksaserbasi akut dengan 3 tanda utama yaitu increased dyspnea increased sputum volume increased sputum purulence (Evidence B) atau
bull 1048774 Pasien dengan eksaserbasi akut dengan 2 tanda utama jika peningkatan purulensi sputum merupakan salah satunya (Evidence C)
bull 1048774 Pasien dengan eksaserbasi parah yang membutuhkan ventilasi mekanik baik invasif maupun non-infvasif (Evidence B)
bull Tahap 3 Tambah teofilinmulai dari 400 mghari dlm bentuk sustained released sesuaikan dosis setiap interval 3 hari untuk menjaga serum level antara 10-15 μgml pantau ESO takikardi tremor nervous efek GI jika tidak ada perbaikan 1048774 hentikan teofilin dan 1048774go to step 4
bull Tahap 4 Coba dengan kortikosteroid prednison 30-40 mghari selama 2-4 minggu cek dengan spirometer (perbaikan ge 20) titrasi dosis ke dosis efektif terkecil (lt 10 μg sehari) pertimbangkan penggunaan kortikosteroid inhalasi 1048774 jika pasien tidak berespon baik 1048774 kembali ke steroid oral
Key points
bull 1048774PPOK adalah penyakit yang sebenarnya secara potensial dapat dicegah 1048774 stop smoking
bull 1048774Sekali PPOK terjadi 1048774 penderita akan memerlukan terapi yang kompleks 1048774 yang efikasinya masih diperdebatkan para ahli
bull 1048774Penyakit ini bersifat progresif dan ireversibel1048774 berbiaya besar baik baik personal maupun masyarakat
Difference between bronchitis and Difference between bronchitis and emphysemaemphysema
Productive cough
bronchitis
Classic sign
emphysema
Late in common with infection
Dyspnea Late in course CommonWheezing Intermittent MildHO smoking Common CommonBarrel chest Occasionally classicProlonged expiration Always present Always presentCyanosis Common UncommonChronic hypoventilation
Common Late in course
Ploycythemia Common Late in course
- COPDPPOM
- BRONCHITIS KRONIS atau COPD type B
- Etiologi
- Slide 4
- Slide 5
- CHRONIC BRONCHITIS
- Slide 7
- Slide 8
- VENTILATION COST
- Slide 10
- Emphysema or type A COPD
- Etiologi Emphysema
- Pathophysiology
- Slide 14
- Pathophysiology
- Slide 16
- Slide 17
- Slide 18
- Prognosis
- Tujuan Terapi
- NON FARMAKOLOGI
- Slide 22
- Slide 23
- Tahap terapi pada PPOK yang stabil
- Terapi antibiotika
- Slide 26
- Key points
- Difference between bronchitis and emphysema
-
bull Tahap 3 Tambah teofilinmulai dari 400 mghari dlm bentuk sustained released sesuaikan dosis setiap interval 3 hari untuk menjaga serum level antara 10-15 μgml pantau ESO takikardi tremor nervous efek GI jika tidak ada perbaikan 1048774 hentikan teofilin dan 1048774go to step 4
bull Tahap 4 Coba dengan kortikosteroid prednison 30-40 mghari selama 2-4 minggu cek dengan spirometer (perbaikan ge 20) titrasi dosis ke dosis efektif terkecil (lt 10 μg sehari) pertimbangkan penggunaan kortikosteroid inhalasi 1048774 jika pasien tidak berespon baik 1048774 kembali ke steroid oral
Key points
bull 1048774PPOK adalah penyakit yang sebenarnya secara potensial dapat dicegah 1048774 stop smoking
bull 1048774Sekali PPOK terjadi 1048774 penderita akan memerlukan terapi yang kompleks 1048774 yang efikasinya masih diperdebatkan para ahli
bull 1048774Penyakit ini bersifat progresif dan ireversibel1048774 berbiaya besar baik baik personal maupun masyarakat
Difference between bronchitis and Difference between bronchitis and emphysemaemphysema
Productive cough
bronchitis
Classic sign
emphysema
Late in common with infection
Dyspnea Late in course CommonWheezing Intermittent MildHO smoking Common CommonBarrel chest Occasionally classicProlonged expiration Always present Always presentCyanosis Common UncommonChronic hypoventilation
Common Late in course
Ploycythemia Common Late in course
- COPDPPOM
- BRONCHITIS KRONIS atau COPD type B
- Etiologi
- Slide 4
- Slide 5
- CHRONIC BRONCHITIS
- Slide 7
- Slide 8
- VENTILATION COST
- Slide 10
- Emphysema or type A COPD
- Etiologi Emphysema
- Pathophysiology
- Slide 14
- Pathophysiology
- Slide 16
- Slide 17
- Slide 18
- Prognosis
- Tujuan Terapi
- NON FARMAKOLOGI
- Slide 22
- Slide 23
- Tahap terapi pada PPOK yang stabil
- Terapi antibiotika
- Slide 26
- Key points
- Difference between bronchitis and emphysema
-
Key points
bull 1048774PPOK adalah penyakit yang sebenarnya secara potensial dapat dicegah 1048774 stop smoking
bull 1048774Sekali PPOK terjadi 1048774 penderita akan memerlukan terapi yang kompleks 1048774 yang efikasinya masih diperdebatkan para ahli
bull 1048774Penyakit ini bersifat progresif dan ireversibel1048774 berbiaya besar baik baik personal maupun masyarakat
Difference between bronchitis and Difference between bronchitis and emphysemaemphysema
Productive cough
bronchitis
Classic sign
emphysema
Late in common with infection
Dyspnea Late in course CommonWheezing Intermittent MildHO smoking Common CommonBarrel chest Occasionally classicProlonged expiration Always present Always presentCyanosis Common UncommonChronic hypoventilation
Common Late in course
Ploycythemia Common Late in course
- COPDPPOM
- BRONCHITIS KRONIS atau COPD type B
- Etiologi
- Slide 4
- Slide 5
- CHRONIC BRONCHITIS
- Slide 7
- Slide 8
- VENTILATION COST
- Slide 10
- Emphysema or type A COPD
- Etiologi Emphysema
- Pathophysiology
- Slide 14
- Pathophysiology
- Slide 16
- Slide 17
- Slide 18
- Prognosis
- Tujuan Terapi
- NON FARMAKOLOGI
- Slide 22
- Slide 23
- Tahap terapi pada PPOK yang stabil
- Terapi antibiotika
- Slide 26
- Key points
- Difference between bronchitis and emphysema
-
Difference between bronchitis and Difference between bronchitis and emphysemaemphysema
Productive cough
bronchitis
Classic sign
emphysema
Late in common with infection
Dyspnea Late in course CommonWheezing Intermittent MildHO smoking Common CommonBarrel chest Occasionally classicProlonged expiration Always present Always presentCyanosis Common UncommonChronic hypoventilation
Common Late in course
Ploycythemia Common Late in course
- COPDPPOM
- BRONCHITIS KRONIS atau COPD type B
- Etiologi
- Slide 4
- Slide 5
- CHRONIC BRONCHITIS
- Slide 7
- Slide 8
- VENTILATION COST
- Slide 10
- Emphysema or type A COPD
- Etiologi Emphysema
- Pathophysiology
- Slide 14
- Pathophysiology
- Slide 16
- Slide 17
- Slide 18
- Prognosis
- Tujuan Terapi
- NON FARMAKOLOGI
- Slide 22
- Slide 23
- Tahap terapi pada PPOK yang stabil
- Terapi antibiotika
- Slide 26
- Key points
- Difference between bronchitis and emphysema
-