cardiovascular, kuliah atma
TRANSCRIPT
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 1/75
Cardiovascular
Dr. Yanto Budiman, Sp.Rad, M.Kes
Bagian Radiologi
RS/FK Atma Jaya Jakarta

7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 2/75
ANATOMY AND PATHOLOGY
1. Chest X Ray
Standard projections and technical consideration :
high Kv 120-145, low KV 60-80Position : postero-anterior, lateral, oblique
Deep inspiration, suspended breathDistance : 72 inches/ 180-200 cm
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 3/75
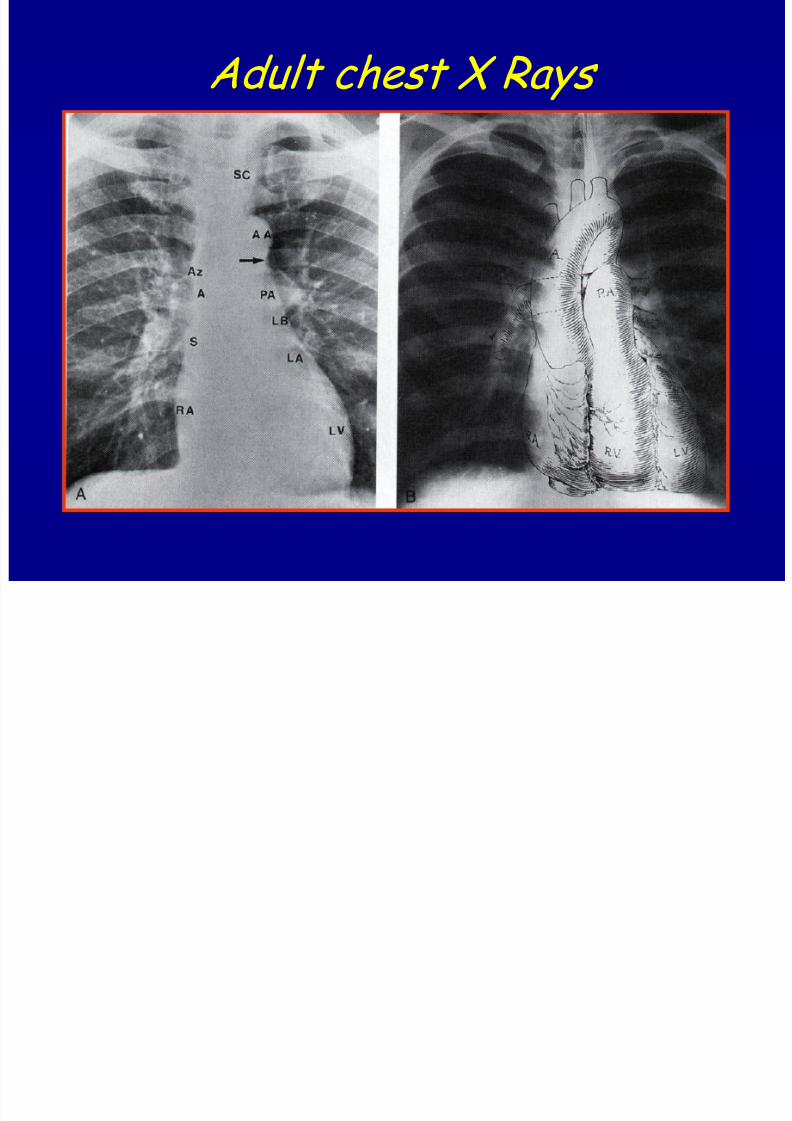
2. Mediastinum The heart and great vessels occupy the mid thorax,
within the mediastinum
The anatomic borders of the mediastinum :
1. Anteriorly : the sternum and its adjacent ribs
2. Posteriorly : the vertebral column and its ribs
3. Laterally : the medial aspects of the parietal
pleuras4. Superiorly : the plane of the 1st rib
5. Inferiorly : the diaphragm
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 4/75
3. Heart image on chest X-ray - Opaque silhoutte
- Mostly located in left hemithorax
- Aortic arch
- Diaphragm
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 5/75
4. Influence factor of the heart
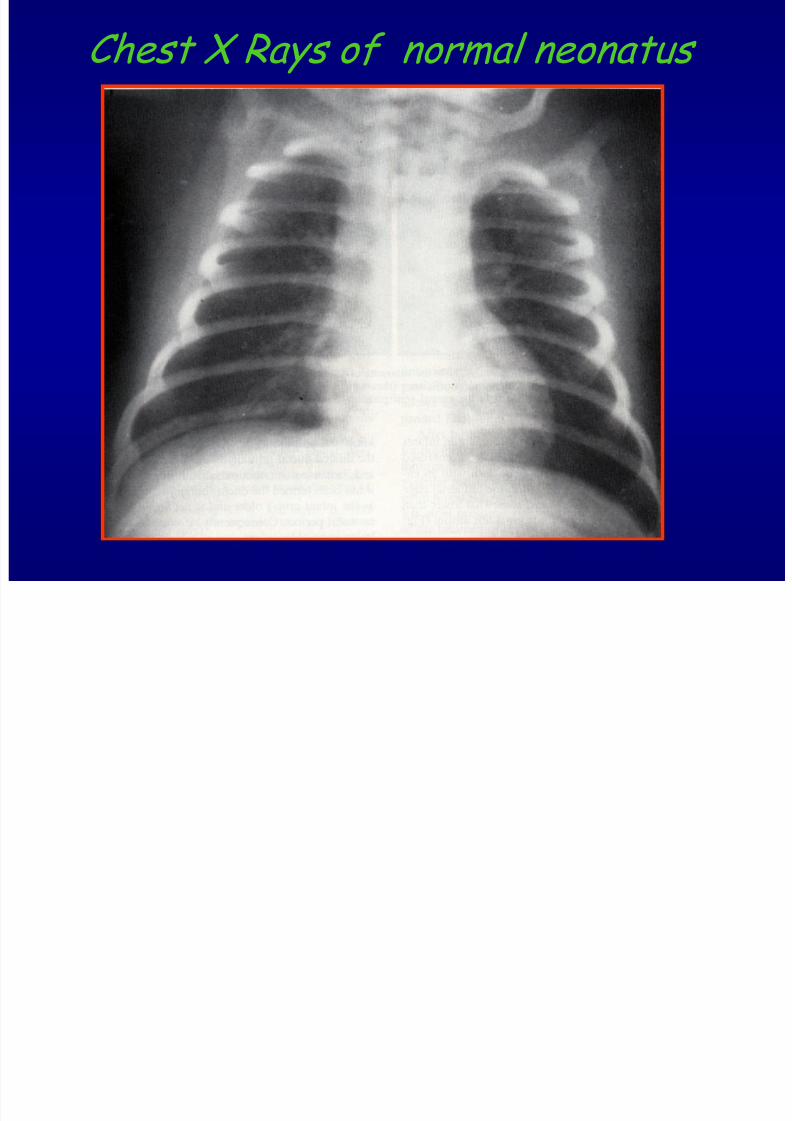
contour 1. The age : infant / newborn : more rounded
and transversal
Childhood
Adult
2. Respiration
Deep inspiration
Expiration
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 6/75
Chest X Rays of normal neonatus
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 7/75
1. Focus - film distance
2. Habitus - pycknicus and asthenicus
3. Abnormalities of the spine, sternum,the lungs --rotation of the heart
4. Position of the patient, erect, supine
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 8/75
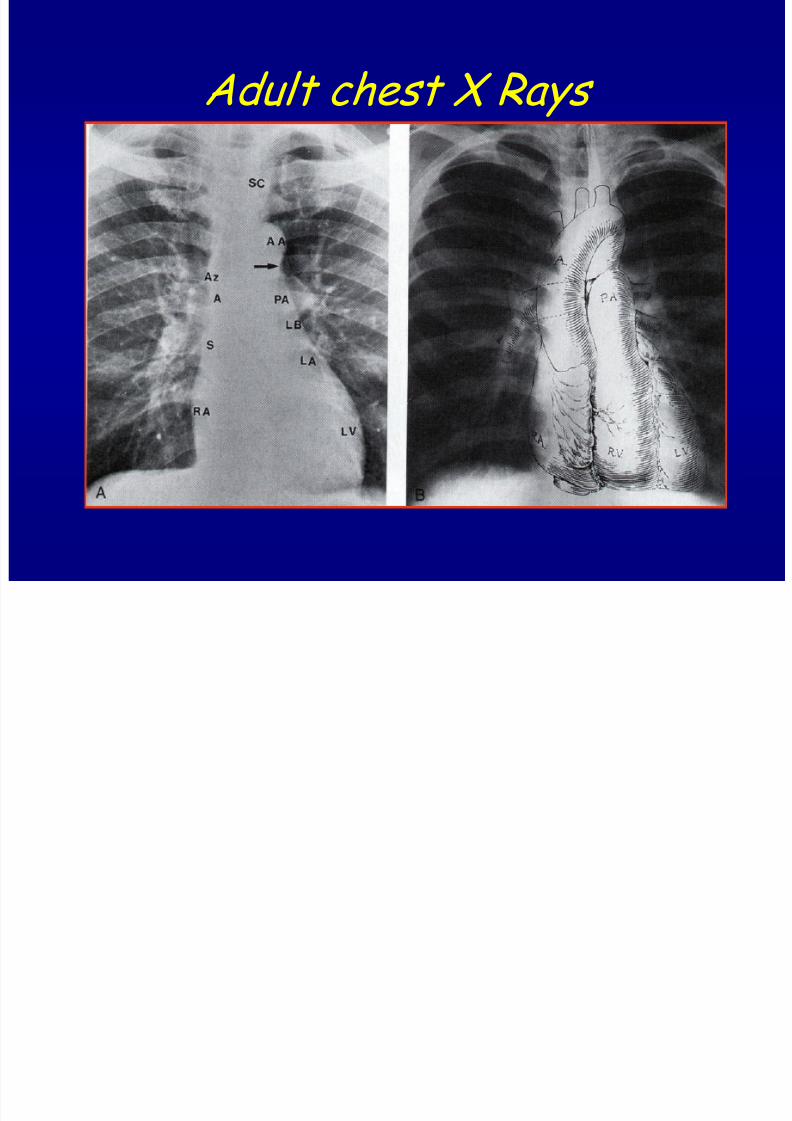
Adult chest X Rays
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 9/75
5. Evaluation of the chest X-ray
Technical aspect : KV, mAs, Artifact,
blurring, distance
Object aspect : deep inspiration,
symmetrical, supine, erect
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 10/75
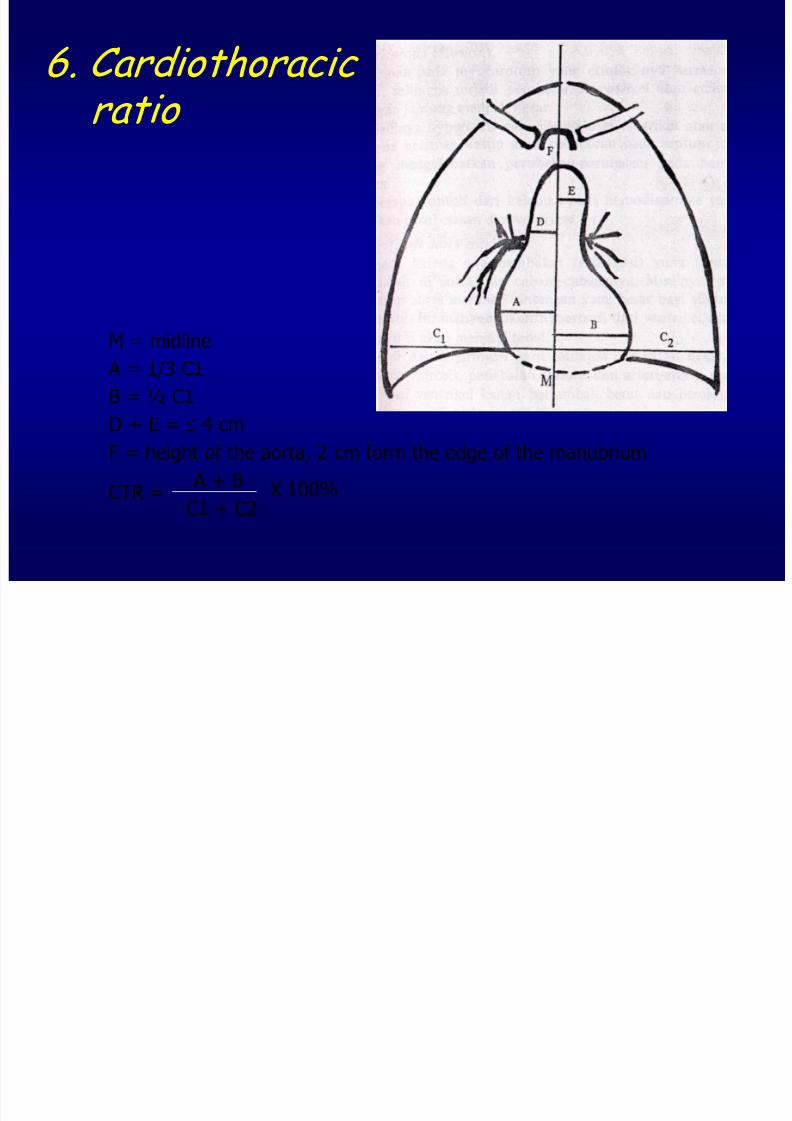
6. Cardiothoracic ratio
M = midline
A = 1/3 C1
B = ½ C1
D + E = 4 cm
F = height of the aorta, 2 cm form the edge of the manubrium
A + B
C1 + C2X 100%CTR =
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 11/75
7. Visualisation of the heart structures
Postero-anterior projection : RA, RV, LV
Lateral projection : RV, LV, LA , AA
Right anterior oblique projection : LA,RA,
RV,AA
Left anterior oblique projection : RV , LV-LA, PA
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 12/75
8. Imaging of the lungs vascular
Close relation between the lungs vascular
and abnormalities of the heart, vice
versa
Pulmonary arteries
Pulmonary veins
Aorta
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 13/75
Pulmonary artery/veins
Normally : Blood (RV) --> thru PA --> Rightand Left Lungs
PA tributaries (small arteries) with bronchi tothe alveoli capillaries
PVs (capillary plexus) in alveoli septa --> tomedial part of the lungs --> wider --> LA
PVs of the lungs basis --> to the lower part
of LA
PVs of the other part of the lungs --> to theupper part of LA
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 14/75
Pulmonary artery
• Hilum : consist of the pulmonary
artery, pulmonary veins, bronchus and
nodes
• Right hilum : in the middle of right
lungs, apex and right diaphragm
• Left hilum : higher than the right hilum
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 15/75
Adult chest X Rays
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 16/75
Pulmonary artery
Hilum : consist of the pulmonary
artery, pulmonary veins, bronchus and
nodes
Right hilum : in the middle of right
lungs, apex and right diaphragm Left hilum : higher than the right hilum
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 17/75
PATHOLOGY
ABNORMALITIES OF LUNG VASCULATURES
Abnormalities of pulmonary vessels
Vascular widening
Vascular narrowing
Pathways irregularity
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 18/75
Vascular widening
Hilum enlargement > 16 mm, conformwith trachea
node enlargement - prominent-
mediastinal enlargement pulmonal artery widening(MPA)
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 19/75
Vascular narrowing
Vascular narrowing : pulmonary stenosis :
decrease of blood volume in lungs, ---
small hilum, small and smooth periphery
vessels, more radio lucent
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 20/75
Abnormality of the aorta
Pitfalls : rotation of the heart, asymmetrical of chest X ray
Widening of the aorta : – Increase blood volume : leakage septal, R to L
–Obstruction of its tributaries at the periphery level :Coarctatio aorta, stenosis Aorta--Takayashudisease --- abdominal aorta
– Abnormality of the aorta itself --widening in chronichypertension
Narrowing of the aorta
– Decrease of blood volume to the aorta --- septalleakage L to R, mitral stenosis
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 21/75
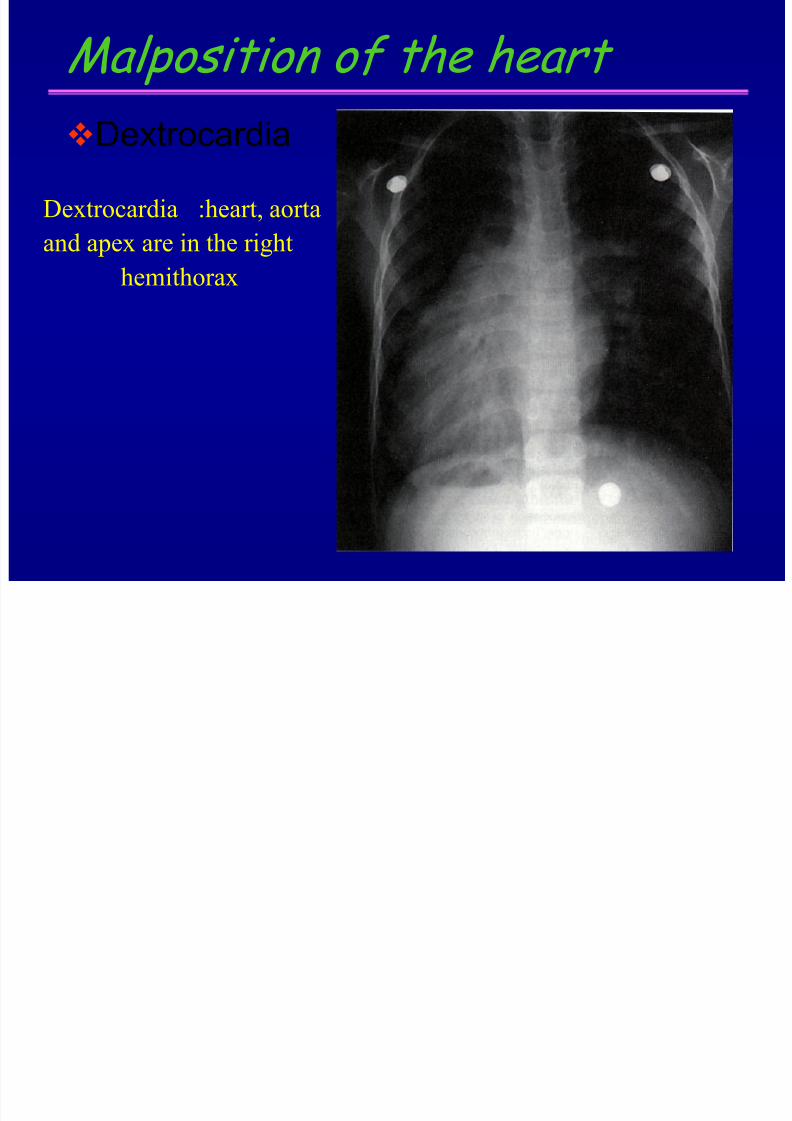
Malposition of the heart
Dextrocardia
Dextrocardia :heart, aorta
and apex are in the right
hemithorax
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 22/75
Enlargement of the heart
1. Enlargement of the heart image
– pericardial disease : pericardial effusion
–
myocardial disease : enlargement of thecardiac chambers, cardiomyopathy
– valvular disease : stenosis, insufficiency
2. Enlargement of the heart chambers :hypertrophy, dilatation
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 23/75
Right atrial enlargement
PA : extension to right of right atrial border,
with increased convexity
RAO : slight posteroinferior convexity
LAO : increases supero-inferior convexity
(prominence of right atrial auricle)
LAT : right atrium protrudes behind esophagus

7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 24/75
Right atrial enlargement
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 25/75
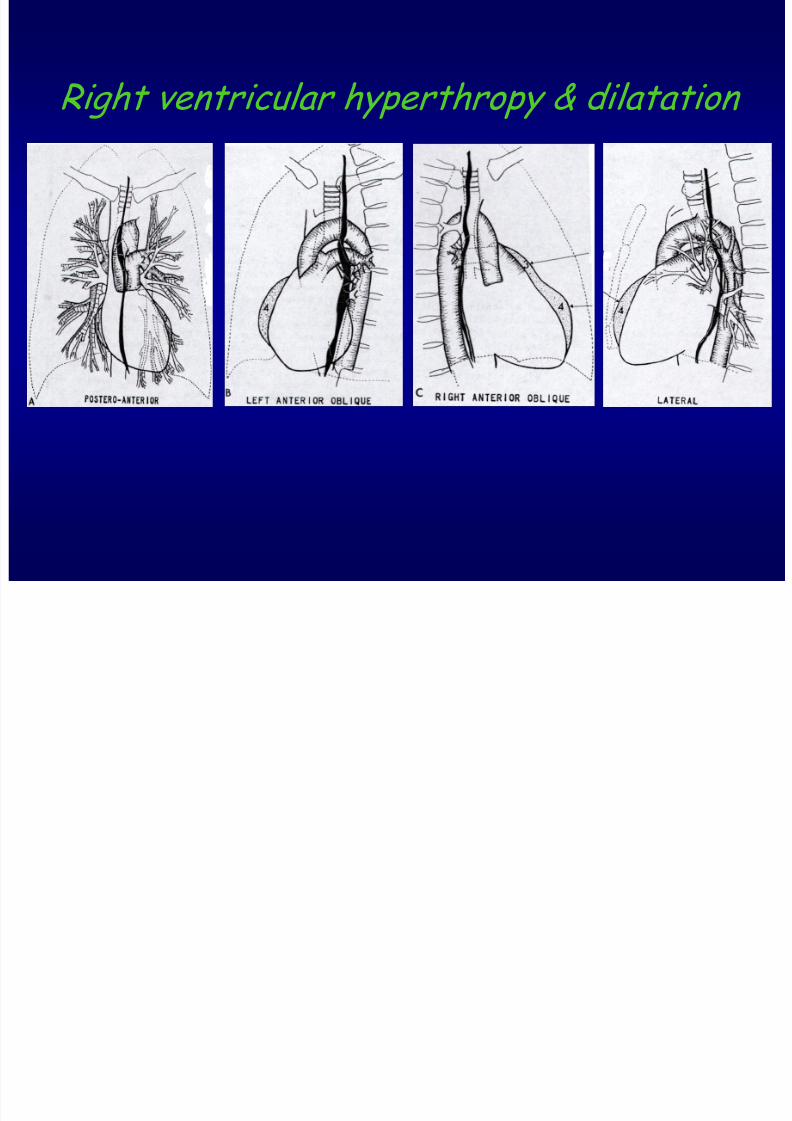
Right ventricle enlargement (hypertrophy & dilatation)
PA : enlargement heart to left side
enlargement dilatation of pulmonary arteries
increased convexing of heart waist, pushing
pulmonary arteries to upper side
RAO : increased prominence of pulmonary sector
(bulguing of MPA)
LAO : bulging on anterior aspect of RV
LAT : right ventricle “clumbs” upward, close to the
sternum
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 26/75
Right ventricular hyperthropy & dilatation
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 27/75
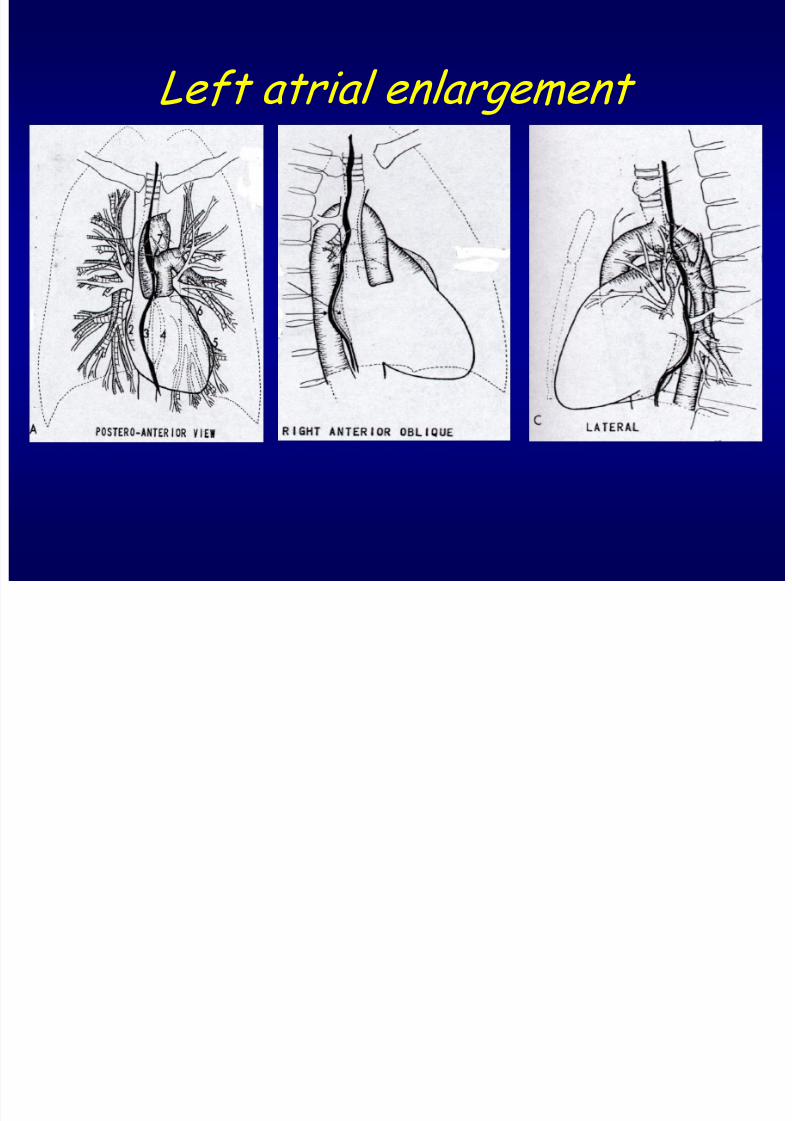
Left atrial enlargement PA : enlargement heart to left & right side
- prominence of left auricle
- double contour at right side
- left main bronchus displaced upward
RAO/LAT :
- enlargement heart to postero-interal (displaced
esophagus to right)- bulging of left atrial auricle/(appendage) displaces
esophagus posteriorly
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 28/75
Left atrial enlargement
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 29/75
Left ventricle enlargement
PA : left extends laterally, left diaphragm is depressed
RAO : - heart intersects left leaf of diaphragm
- anterior apical position of heart extends further
anteriorly
- heart is displaced posteriorly, close to spinal
LAO : LV extends beyond retrocardiac space, and cannot
clear the spine
LAT : LV displaced posteriorly, close to spine
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 30/75
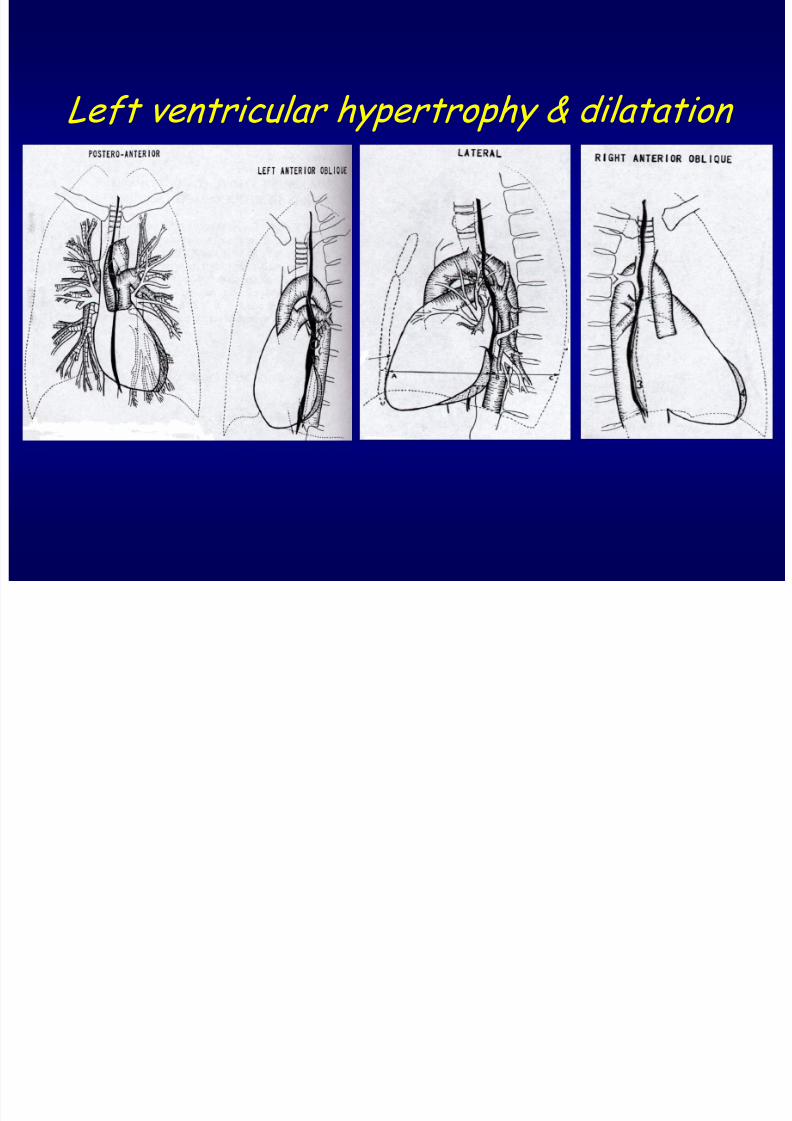
Left ventricular hypertrophy & dilatation
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 31/75
CONGENITAL ANOMALY
Abnormality of the septum
Abnormality of the great arteries ---
shape and position
Abnormality of chamber of the heart
Abnormality of position
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 32/75
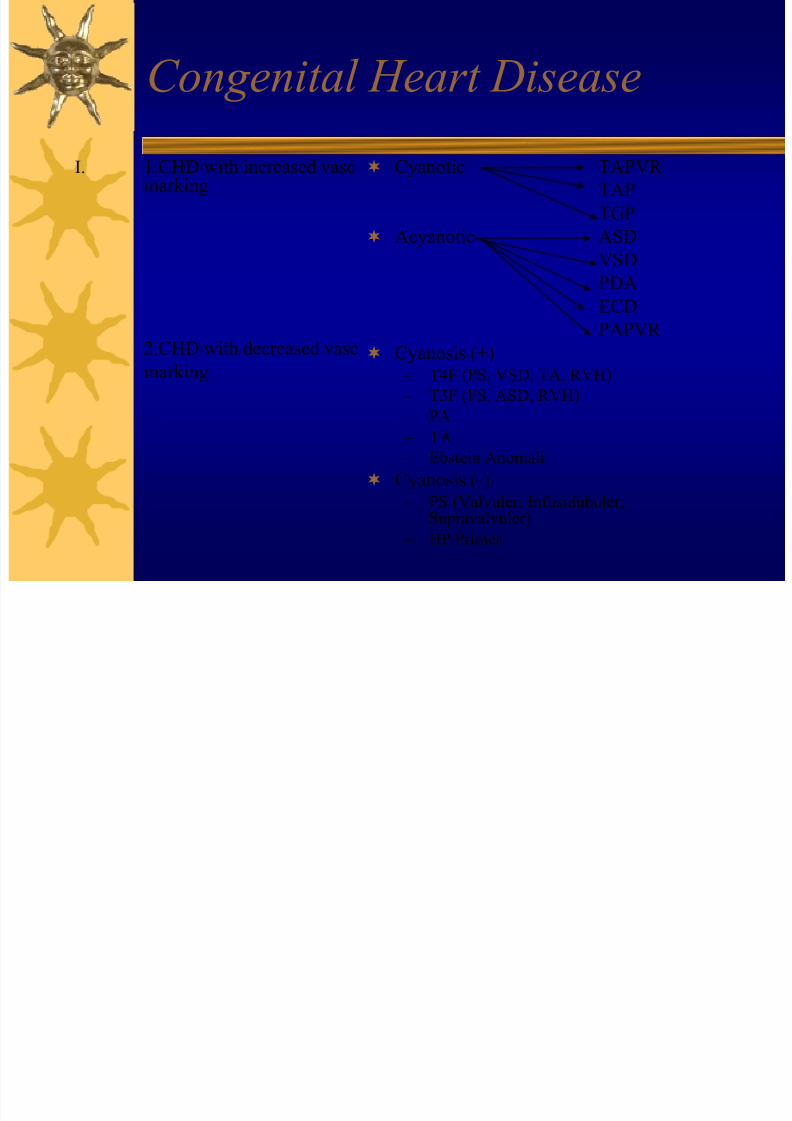
Congenital Heart Disease
I. 1.CHD with increased vascmarking
2.CHD with decreased vasc
marking
Cyanotic TAPVR
TAP
TGP
Acyanotic ASD
VSD
PDAECD
PAPVR
Cyanosis (+) – T4F (PS, VSD, TA, RVH)
– T3F (FS, ASD, RVH)
– PA
– TA
– Ebstein Anomali
Cyanosis (-) – PS (Valvuler, Infusidubuler,
Supravalvuler)
– HP Primer
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 33/75
1. Congenital anomaly with increased pulmonary vascular markings
A. Without cyanosis
1. Atrial septal defect (ASD)
Septum primum
Ostium primum closed
Septum secundum
Foramen ovale closed
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 34/75
Chest X ray Depends on :
• The severity of the defect
• Complication
L to R shunt
R to L shunt
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 35/75
Chest X ray
Without pulmonary hypertensionPA position
- Heart enlargement to left side
- Apex is rounded & upward
- Widening of the hila
- Widening of pulmonary artery and its tributaries
- Widening of pulmonary veins at supra and perihilar
- Periphery pulmonary vascular are clear
- Prominence of MPA
- Aortic arch is small
Increased pulmonary vascular marking
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 36/75
Chest X ray
Lat Position
No enlargement of LA & LV
Enlargement of RV
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 37/75
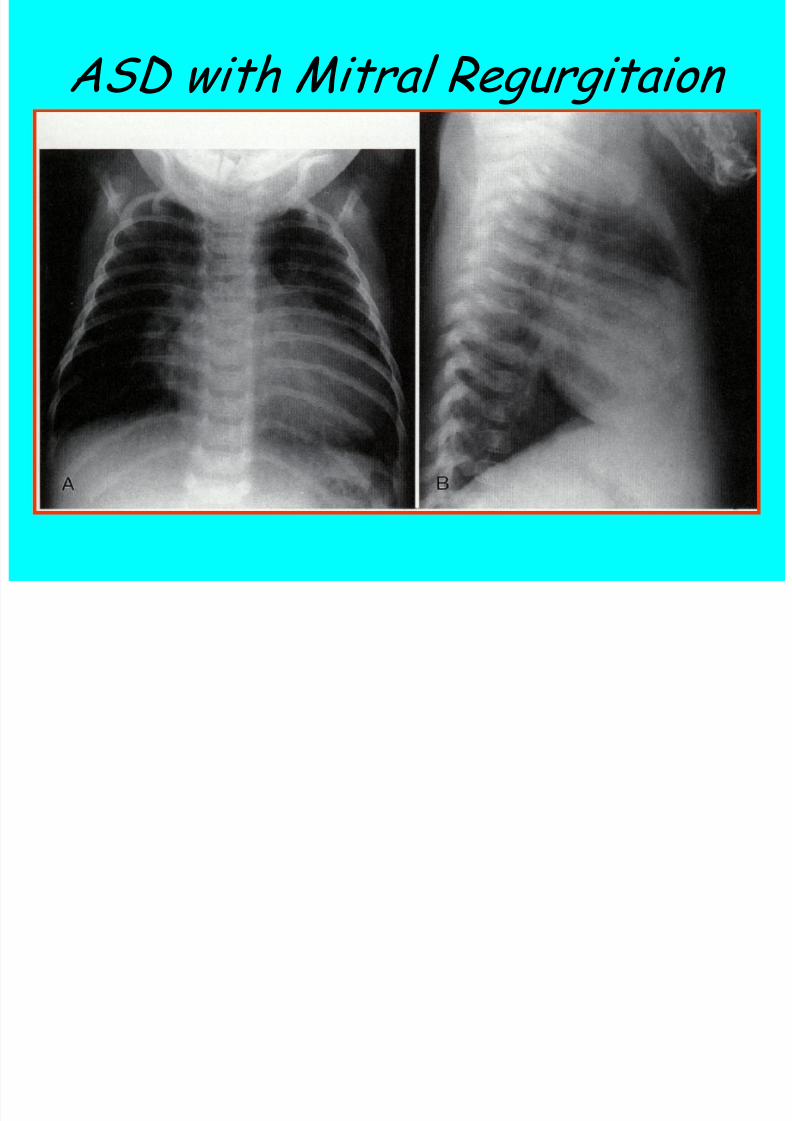
ASD with Mitral Regurgitaion
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 38/75
With pulmonary hypertension PA position
Enlargement of the heart on bothsides
Extremely wide of central hila andbecame smaller to periphery
MPA is very prominent
Small aorta
Pulmonary veins are faint
Periphery area is more radio lucent
Barrel chest
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 39/75
Lateral position
• LV Enlargement
• LA is normal/enlarged
• RV Enlargement close to uppersternum
• Hilar enlargement
• Infero-posterior part of the heart
overlapping with vertebral column
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 40/75
3. Ventricular septal defect (VSD)
Incidence :
The most common form of CHD (20-25%) of all CHD
Clinical manifestation
- Small VSD : N growth, development, symptoms
- Moderate to large VSD : Increase exercise tolerance
- Delayed growth and development
- CHF is relative common in infancy
- Cyanosis with long standing pulmonary hypertension
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 41/75
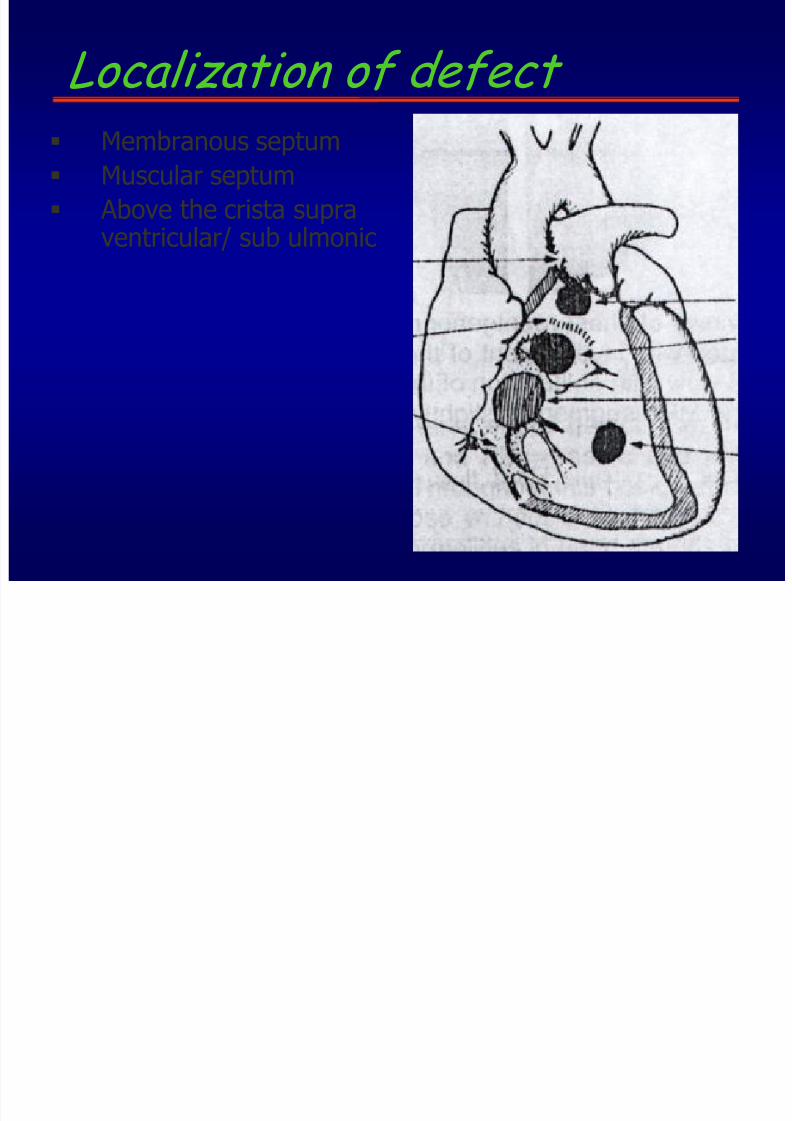
Localization of defect
Membranous septum Muscular septum
Above the crista supraventricular/ sub ulmonic
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 42/75
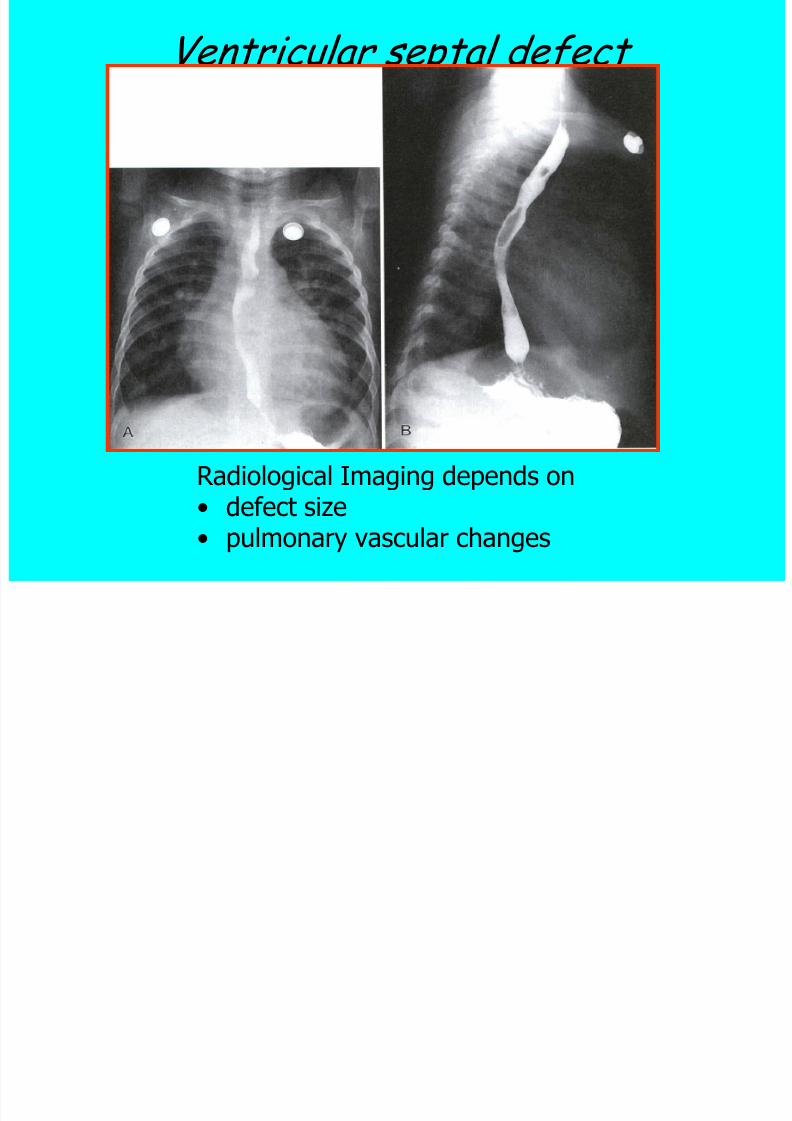
Ventricular septal defect
Radiological Imaging depends on• defect size•
pulmonary vascular changes
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 43/75
Chest X ray Tiny defect (maladies de Roger )
No heart enlargement
Normal of pulmonary vascular
markings
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 44/75
Small defect
• Heart enlargement to left side (LVH)
• Dilatation of LA
• Dilatation of RV
• Increased pulmonary vascular markings
• Apex towards diaphragm
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 45/75
VSD Moderate to large
RV dilatation and hypertrophy
LV hyperthropy
RA is normal
LA dilatation
Aorta is small
Widening of pulmonary arteries
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 46/75
VSD with pulmonary hypertension
• RV is more dilated
• LA is Normal
• Aorta is normal• MPA is prominent
• Pulmonary artery and its central
tributaries are wider• Chest is more emphysematous
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 47/75
Patent Ductus Arteriousus (PDA)
Incidence : 10 % of all CHD, excludingpremature infants
Female : male = 3 : 1
A common problem in premature infants
It is a patency of a normal fetal structure
between the left PA and the descending
aorta (ductus arteriosus Botalli) L to R shunt
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 48/75
Chest X ray :
LA dilatation LV hypertrophy
PA
PVLA are enlarged
LV
AO
RV dilatation (large defect)
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 49/75
Small PDA : Heart
Pulmonary vascularitiesModerate PDA : Ascending aorta
aorta arch PA : prominent next to AO
Pulmonary vascular markings : increased
Hila : wide R
LA : enlarged
LV
RV
N
N/slightly enlarged
are enlarged
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 50/75
PDA with pulmonary hypertension
RV dilatation (hypertrophy and dilatation)
LA : normal
Asc aorta : wide Aortic arch : prominent
MPA : prominent
Hila : wide Periphery pulmonary vascularities : faint
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 51/75
Partial anomalous pulmonary venous return (PAPVR)
Incidence “ Less than 1 % of all CHD
One or more (but not all) pulmonary veinsdrain into the RA or its tributaries, such asthe SVC, IVC, left innominate vein
Important consideration
• The number of anomalous pulmonary vein
• The prescence and the size of ASD
• The pulmonary vascular resistance
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 52/75
Chest X ray Important RA
RV are enlarged
PA
Similar to ASD
Heart enlargement (RA, RV)
Widening of MPA
Widening of hila
Occasionally : a dilated PVC, a crescent,shaped, vertical shadow in the right lowerlung
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 53/75
B. Increased pulmonary vascular
markings with cyanosis Total anomalous pulmonary venous
return (TAPVR)Incidence : 1 % of all CHD
No direct communication between the
pulmonary veins and LA
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 54/75
Depending on the site of the
drainage of the pulmonary veins
Supracardiac SVC
Cardiac coronary smos
Infra cardiac PV, HV, IVC
Mixed type
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 55/75
2. Persistent truncus arteriosus
Incidence : less than 1 % of all CHD
VSD : is always present
Only a single trunk leaves the heartand gives rise to pulmonary,
systemic and coronary circulations
Blood from RV & LV drain into thetrunk cyanotic
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 56/75
Chest X rays Heart enlargement, oval shaped (RV,
LV, LA)
Increased pulmonary vascularity
A right aortic arch (50%)
T iti f th t l
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 57/75
Transposition of the great vessel
• Incidence “ 5% of all CH defect
• More common in males M : F = 3 : 1• The aorta arises anteriorly from RV
• The pulmonary artery arises posteriorly fromLV
• ASD, VSD, PDA are necessary for survival
• More common bidirectional shunt
• More common R to L shunt
• Chest X-ray• Heart enlargement, oval/egg shaped, with a
narrow superior mediastinum
• Increases pulmonary vascularity
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 58/75
Congenital heart anomalies with decrease pulmonary vascularity
A. Without cyanosis
1. Pulmonary stenosis
– Incidence 5% - 8% of all congenital heartdefects
– Valvular stenosis
– Subvalvular stenosis (infundibulum) – Supravalvular stenosis (mainstem of PA)
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 59/75
Chest X rays
Heart size is normal RV enlargement : hyperthrophy dilatation
MPA is prominent
Pulmonary vascularity is normal decreased Heart enlargement (CHF)
Lung : more lucency (small lung vessels)
Different vascularization between right andleft lung on valvular stenosis
Post stenotic dilatation
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 60/75
B. With cyanosis
1. Tetralogy of Fallot
• Incidence 10% of all congenital heart diseases
• The most common cyanotic cardiac defect beyondinfancy
•Four abnormalities – VSD (R to L)
– Pulmonary stenosis infundibular/valvular
– Over riding aorta
– Right ventricular hypertrophy• The severity of RVH and defect of VSD depend on
stenotic of pulmonary artery
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 61/75
Chest X ray
• RV : enlargement, extends heart to left
• Apex : upturned
•Concavity of heart waist/MPA
• Booth shaped/coeur en sabot
• Lungs vessels are smaller increasedradiolucency
• Widening of the aortic arch
• Right sided aorta/aortic arch (25%)
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 62/75
2. Trilogy of Fallot
Similar to Tetralogy of Fallot excluded VSD/overridingaorta
Abnormalities are :
• Pulmonary stenosis
• RVH
• Leakage of atrial septum thru ASD/persistenforamen ovale
Chest X ray
Similar to PS imaging
• RVH
• Apex : uptoward
• Decreased pulmonary vascularity
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 63/75
3. Pulmonary atresia
• Is a part of RV hypoplasie
• RV : small
• PA : absent
• VSD : absent
• Combination between ASD & PDA
Chest X ray
• Heart enlargement, oval shaped
• LA enlargement
• RA enlargement
• LV enlargement
• Concavity of heart waist
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 64/75
4. Tricuspid valve atresia
• Connection of LA & RA thru ASD
• Connecting of LV & RV thru VSD
5. Ebstein anomaly• Chest X ray
• Extreme cardiomegaly
• Decreased pulmonary vascular markings
A qui d h t dis s
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 65/75
Acquired heart disease
1. Mitral stenosis
Incidence : - Rare in children
- The most common valvular involvementin adult rheumatic patients
Etiology : - Rheumatic fever
- Viral- Streptococcus bacteria
Involved area :
- Valves
- Ring of valves- Papillary muscles
- Myocardium
- Pericardium
7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 66/75
Involved valves valves weakness 2 chorda
tendinae weakness valves are insuficient narrowing of the valve
Valve narrowing LA dilatation (because of
blood accumulation) increased LA pressure
congestion of the pulmonary veins
pulmonary hypertension increased
resistancy in capillaries obstruction of blood
from RV increased in RV pressure RVH

7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 67/75
Chest X ray
Changing of : - heart shaped &
- pulmonary vascularity

7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 68/75
PA LA dilatation
Double contour in right side Prominence of LAA, MPA
Elevation of main stein left bronchus
Small aorta
Heart enlargement to left with upright apex
Displaced esophagus to right side
Lateral
Without contrast Holtzknecht space is clear
With contrast
Displaced esophagus posteriorly

7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 69/75
2. Mitral insuficiency
Incidence : - the most common valvular involvement
in children with RHD
- Males are more commonly affected
than females
Etiology : Rheumatic fever- Paralyzed of mitral valve, chorda hendriae
- Paralyzed of papillary muscls
- Prolaps of one valve leaflet
- Dilatation of ring valve
Blood few back into LA

7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 70/75
Chest X rays
PA : - Enlargement of LA & LV- Pulmonary vascularity is usually within normal
limits
- Double contour
- Auricle of LA prominent
- Elevation of the left mainstem bronchus
- Displacement esophagus to right
Lat : - Displacement esophagus posteriorly
- LV protruded posteriorly

7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 71/75
3. Aorta insuficiency
Incidence : - More common in males than females
- Rheumatic endocarditis
- Aneurysma
- Aortasclerotic
Regurgitation of blood into LV dilatation LVH + dilatation
Chest X ray :
PA : - apex turned down
- aortic arch : prominent wide
- concavity of pulmonal, auricle area
- aortic configuration
Lat : retrocardiac space is occupied (LV dilatation)

7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 72/75
4. Aortic stenosis
Incidence : - 5% of all congenital heart defect
- more common in males than females (4:1)
Chest X ray :
PA : - heart enlargement to left side
- apex turned down
- occasionally widening of ascending aorta
Lat : anterior part of ascending
Aorta : prominent (post stenotic dilatation)
RV, LV N
5 T i id i fi i

7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 73/75
5. Tricuspid insuficiency
Incidence : - 2% of all congenital disease in infancy
Etiology : - congenital- rheumatic
Chest X ray :
PA : - RA dilatation
- pulmonary vascularity : decreased
LAO : auricle RA : more prominent
RAO : enlargement RA, protruded posteriorly,
beneath LA
6. Pulmonary stenosis
Etiology : most commonly congenital
l / b l

7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 74/75
Aortic anomalies/abnormalities
Etiology : - inflammation process
- degenerative process
- traumatic factor
- congenital
Aortitis
Aortasclerotic
Aortaelongation
Aortic aneurysm Coarctatio aortae
Vascular ring

7/30/2019 Cardiovascular, Kuliah Atma
http://slidepdf.com/reader/full/cardiovascular-kuliah-atma 75/75