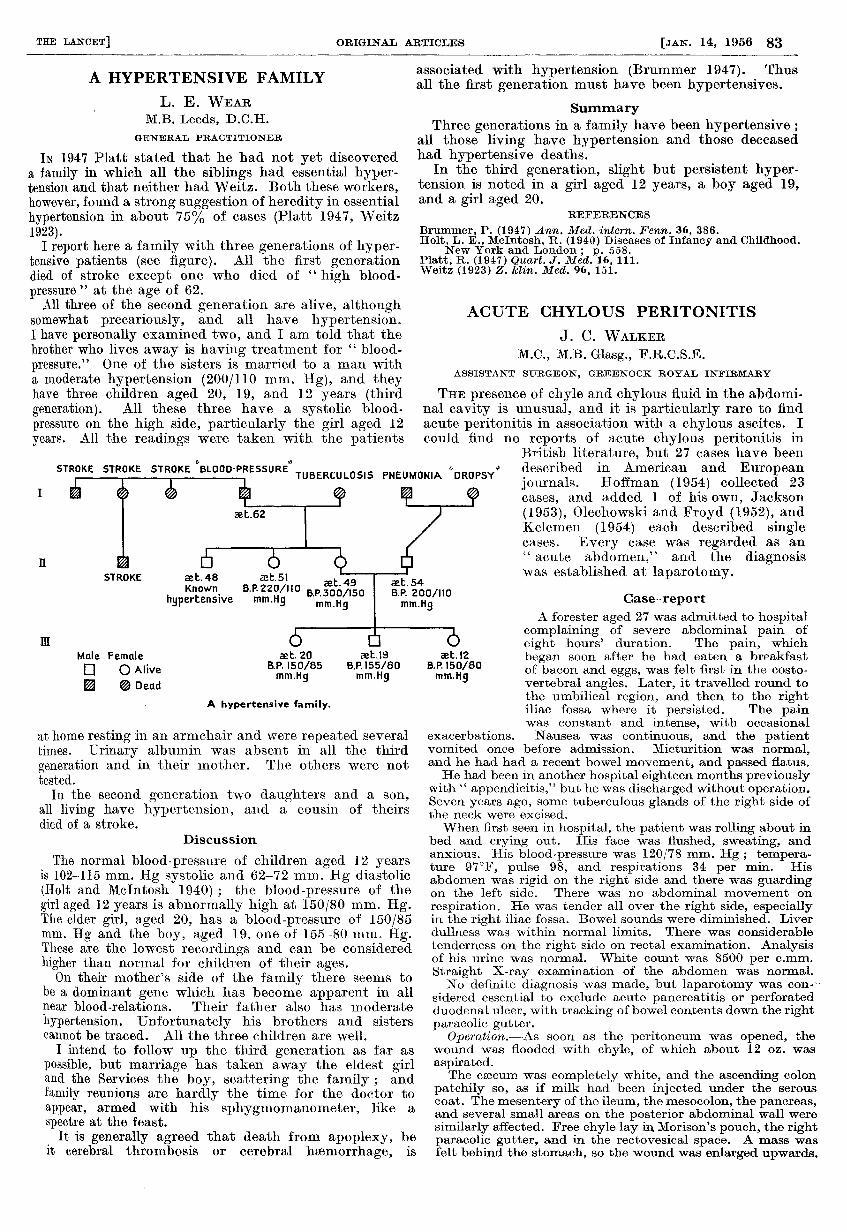
a hypertensive family
TRANSCRIPT
83
A HYPERTENSIVE FAMILY
L. E. WEARM.B. Leeds, D.C.H.
GENERAL PRACTITIONER
IN 1947 Platt stated that he had not yet discovereda family in which all the siblings had essential hyper-tension and that neither had Weitz. Both these workers,however, found a strong suggestion of heredity in essentialhypertension in about 75% of cases (Platt 1947, Weitz1923).
I report here a family with three generations of hyper-tensive patients (see figure). All the first generationdied of stroke except one who died of " high blood-pressure " at the age of 62.
All three of the second generation are alive, althoughsomewhat precariously, and all have hypertension.I have personally examined two, and I am told that thebrother who lives away is having treatment for " blood-pressure." One of the sisters is married to a man witha moderate hypertension (200/110 mm. Hg), and theyhave three children aged 20, 19, and 12 years (thirdgeneration). All these three have a systolic blood-
pressure on the high side, particularly the girl aged 12years. All the readings were taken with the patients
at home resting in an armchair and were repeated severaltimes. Urinary albumin was absent in all the third
generation and in their mother. The others were nottested.
In the second generation two daughters and a son,all living have hypertension, and a cousin of theirsdied of a stroke.
Discussion
The normal blood-pressure of children aged 12 yearsis 102-115 mm. Hg systolic and 62-72 mm. Hg diastolic(Holt and McIntosh 1940) ; the blood-pressure of thegirl aged 12 years is abnormally high at 150/80 mm. Hg.The elder girl, aged 20, has a blood-pressure of 150/85mm. Hg and the boy, aged 19, one of 155-80 mm. Hg.These are the lowest recordings and can be consideredhigher than normal for children of their ages.On their mother’s side of the family there seems to
be a dominant gene which has become apparent in allnear blood-relations. Their father also has moderatehypertension. Unfortunately his brothers and sisterscannot be traced. All the three children are well.
I intend to follow up the third generation as far aspossible, but marriage has taken away the eldest girland the Services the boy, scattering the family ; andfamily reunions are hardly the time for the doctor toappear, armed with his sphygmomanometer, like a
spectre at the feast.It is generally agreed that death from apoplexy, be
it cerebral thrombosis or cerebral haemorrhage, is
associated with hypertension (Brummer 1947). Thusall the first generation must have been hypertensives.
SummaryThree generations in a family have been hypertensive ;
all those living have hypertension and those deceasedhad hypertensive deaths.
In the third generation, slight but persistent hyper-tension is noted in a girl aged 12 years, a boy aged 19,and a girl aged 20.
REFERENCES
Brummer, P. (1947) Ann. Med. intern. Fenn. 36, 386.Holt, L. E., McIntosh, R. (1940) Diseases of Infancy and Childhood.
New York and London ; p. 558.Platt, R. (1947) Quart. J. Med. 16, 111.Weitz (1923) Z. klin. Med. 96, 151.
ACUTE CHYLOUS PERITONITIS
J. C. WALKERM.C., M.B. Glasg., F.R.C.S.E.
ASSISTANT SURGEON, GREENOCK ROYAL INFIRMARY
THE presence of chyle and chylous fluid in the abdomi-nal cavity is unusual, and it is particularly rare to findacute peritonitis in association with a chylous ascites. Icould find no reports of acute chylous peritonitis in
British literature, but 27 cases have beendescribed in American and Europeanjournals. Hoffman (1954) collected 23
cases, and added 1 of his own, Jackson
(1953), Olechowski and Froyd (1952), andKelemen (1954) each described singlecases. Every case was regarded as an" acute abdomen," and the diagnosiswas established at laparotomy.
Case-reportA forester aged 27 was admitted to hospital
complaining of severe abdominal pain of
eight hours’ duration. The pain, which
began soon after he had eaten a breakfastof bacon and eggs, was felt first in the costo-vertebral angles. Later, it travelled round tothe umbilical region, and then to the rightiliac fossa where it persisted. The painwas constant and intense, with occasional
exacerbations. Nausea was continuous, and the patientvomited once before admission. Micturition was normal,and he had had a recent bowel movement, and passed flatus.He had been in another hospital eighteen months previously
with " appendicitis," but he was discharged without operation.Seven years ago, some tuberculous glands of the right side ofthe neck were excised.When first seen in hospital, the patient was rolling about in
bed and crying out. His face was flushed, sweating, andanxious. His blood-pressure was 120/78 mm. Hg ; tempera-ture 97°F, pulse 98, and respirations 34 per min. Hisabdomen was rigid on the right side and there was guardingon the left side. There was no abdominal movement onrespiration. He was tender all over the right side, especiallyin the right iliac fossa. Bowel sounds were diminished. Liverdullness was within normal limits. There was considerabletenderness on the right side on rectal examination. Analysisof his urine was normal. White count was 8500 per c.mm.
Straight X-ray examination of the abdomen was normal.No definite diagnosis was made, but laparotomy was con--
sidered essential to exclude acute pancreatitis or perforatedduodenal ulcer, with tracking of bowel contents down the rightparacolic gutter.
Ope,ration.-As soon as the peritoneum was opened, thewound was flooded with chyle, of which about 12 oz. wasaspirated.The caecum was completely white, and the ascending colon
patchily so, as if milk had been injected under the serouscoat. The mesentery of the ileum, the mesocolon, the pancreas,and several small areas on the posterior abdominal wall weresimilarly affected. Free chyle lay in Morison’s pouch, the rightparacolic gutter, and in the rectovesical space. A mass wasfelt behind the stomach, so the wound was enlarged upwards.