aspir
TRANSCRIPT
Aspirin
Dari Wikipedia bahasa Indonesia, ensiklopedia bebas
Struktur kimia aspirin
Aspirin atau asam asetilsalisilat (asetosal) adalah suatu jenis obat dari keluarga salisilat yang sering digunakan sebagai analgesik (terhadap rasa sakit atau nyeri minor), antipiretik (terhadap demam), dan anti-inflamasi. Aspirin juga memiliki efek antikoagulan dan digunakan dalam dosis rendah dalam tempo lama untuk mencegah serangan jantung.
Asal dari obat yang dikenal dengan "Aspirin" - ternyata dari zaman Yunani kuno, dan diperkenalkan oleh Bapak Para Dokter se-dunia - yaitu Hippocrates. Tentu saja Hippocrates tidak menyebut Aspirin, melainkan menyebut tumbuhan bernama willow yang bila batangnya dikeringkan dan dijadikan bubuk, dapat menghilangkan rasa sakit.
Ribuan tahun berlalu, hingga di tahun 1829, para ilmuwan berhasil mengisolasi bahan dalam tumbuhan willow yang berfungsi meredakan rasa sakit. Bahan tersebut bernama salicin. Bahan ini dapat menghilangkan sakit, tapi memiliki efek samping terhadap perut - manfaat dan mudaratnya sama besar. Tentu saja harus ada jalan keluar. Di tahun 1853, seorang ahli kimia Perancis bernama Charles Frederic Gerhardt berhasil menetralkan salicin alami menjadi asam salisilat (salicylic acid) lewat penyanggaan (buffering) dengan natrium dan asam asetat. Asam salisilat ini lebih "ramah" terhadap perut.
Di tahun 1899, seorang ahli kimia Jerman, bernama Felix Hoffmann, yang bekerja bagi Bayer, menemukan kembali formula Gerhardt. Hoffmann membujuk Bayer untuk memasarkan obat itu, yang selanjutnya muncul di pasar dengan nama pasaran "Aspirin".
Aspirin adalah obat pertama yang dipasarkan dalam bentuk tablet. Sebelumnya, obat diperdagangkan dalam bentuk bubuk (puyer). Dalam menyambut Piala Dunia FIFA 2006 di Jerman, replika tablet aspirin raksasa dipajang di Berlin sebagai bagian dari pameran terbuka Deutschland, Land der Ideen ("Jerman, negeri berbagai ide").
Research in The 1990s: The Search for New Drugs
In 1763, the Reverend Edmund Stone took the first step toward the discovery of one of the most commonly used medicines when he noted that the bark of the English willow was an effective treatment for patients suffering from a fever. Stone explained the effect of willow bark by noting that ". . . many natural maladies carry their cures along with them, or their remedies lie not far from their causes." Thus, he argued, the English willow grows in the same moist regions where one was likely to catch the fever treated with its bark.
It took 50 years before the active ingredient in willow bark was isolated and named salicin, from the Latin name for the willow (Salix alba). Another 50 years elapsed before a large-scale synthesis for this compound was available. By that time, the compound was known as salicylic acid because saturated solutions in water are highly acidic (pH = 2.4).
By the end of the 19th century, salicylic acid was being used to treat rheumatic fever, gout, and arthritis. Many patients treated with this drug complained of chronic stomach irritation because of its acidity and the large doses (6-8 g/d) required. Because his father was one of these patients, Felix Hoffman searched the chemical literature for a less acidic derivative of salicylic acid. In 1898, Hoffman reported that the acetyl ester of salicylic acid was simultaneously more effective and easier to tolerate than the parent compound. He named this compound aspirin, taking the prefix a- from the name of the acetyl group and spirin from the German name of the parent compound spirsaure.
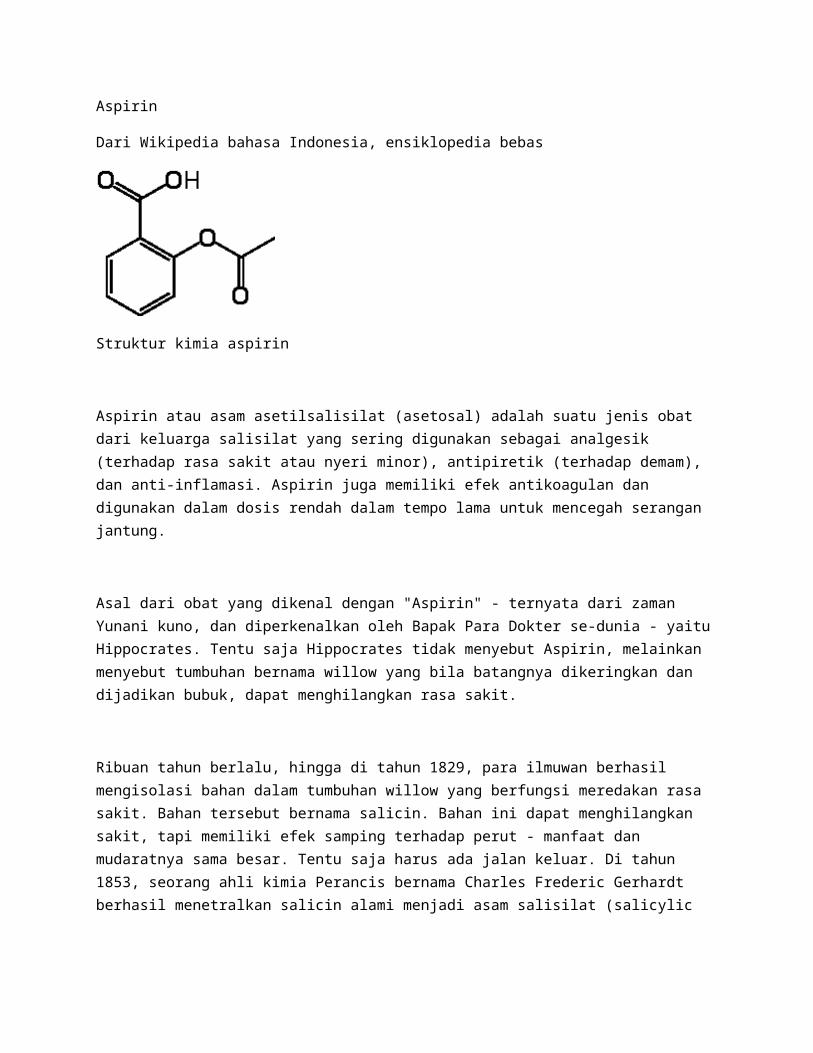
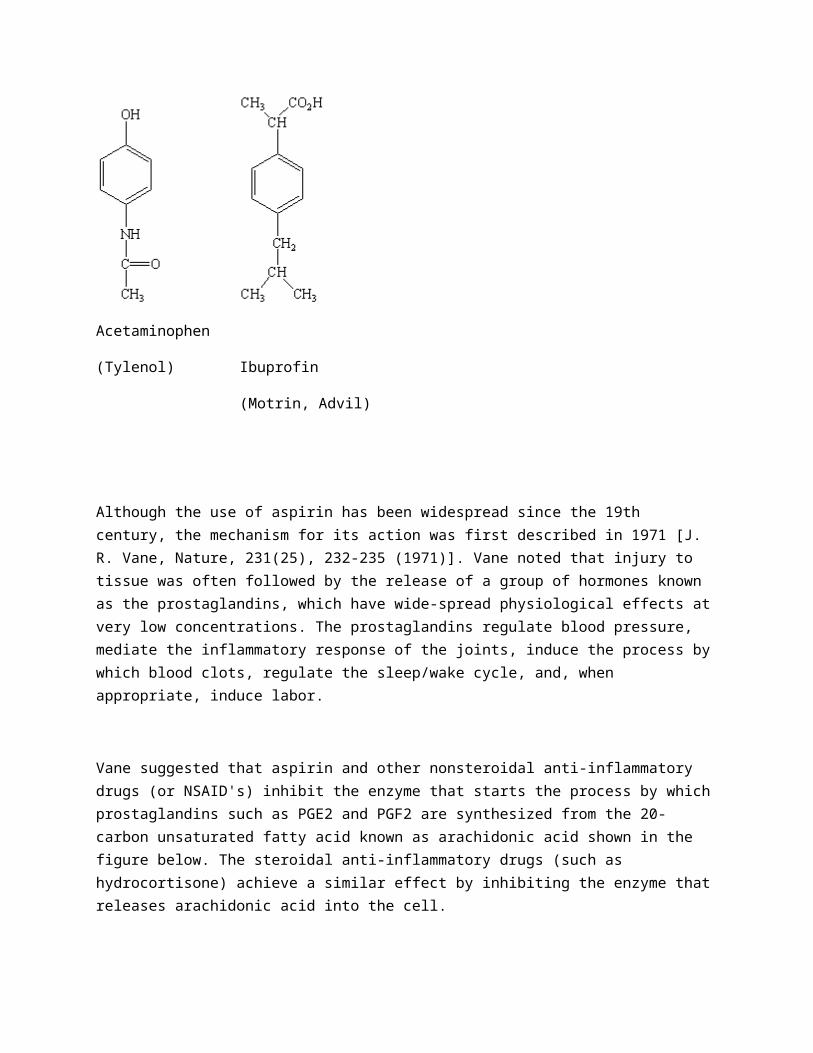
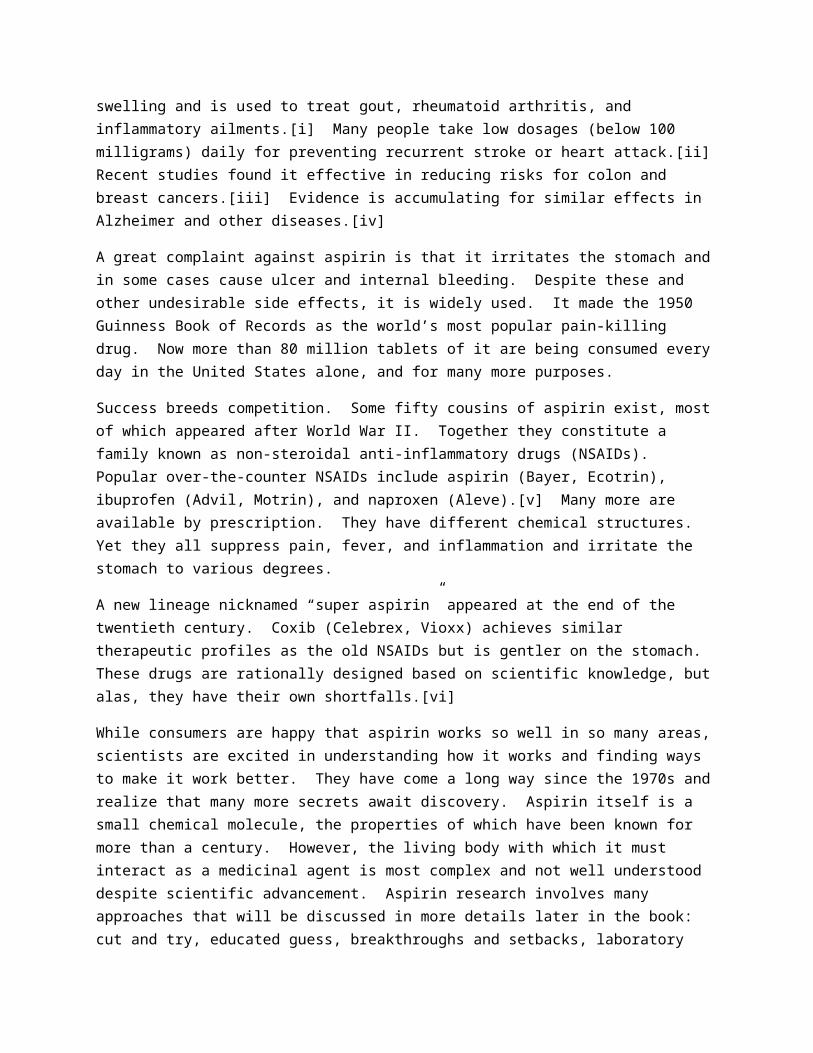
The existence of a drug that reduced both pain and fever initiated a search for other compounds that could achieve the same result. Although it was based on trial and error, this search inevitably produced a variety of substances, such as those in the figure below, that are analgesics, antipyretics, and/or anti-inflammatory agents. Analgesics relieve pain without decreasing sensibility or consciousness. Antipyretics reduce the body temperature when it is elevated. Anti-inflammatory agents counteract swelling or inflammation of the joints, skin, and eyes.
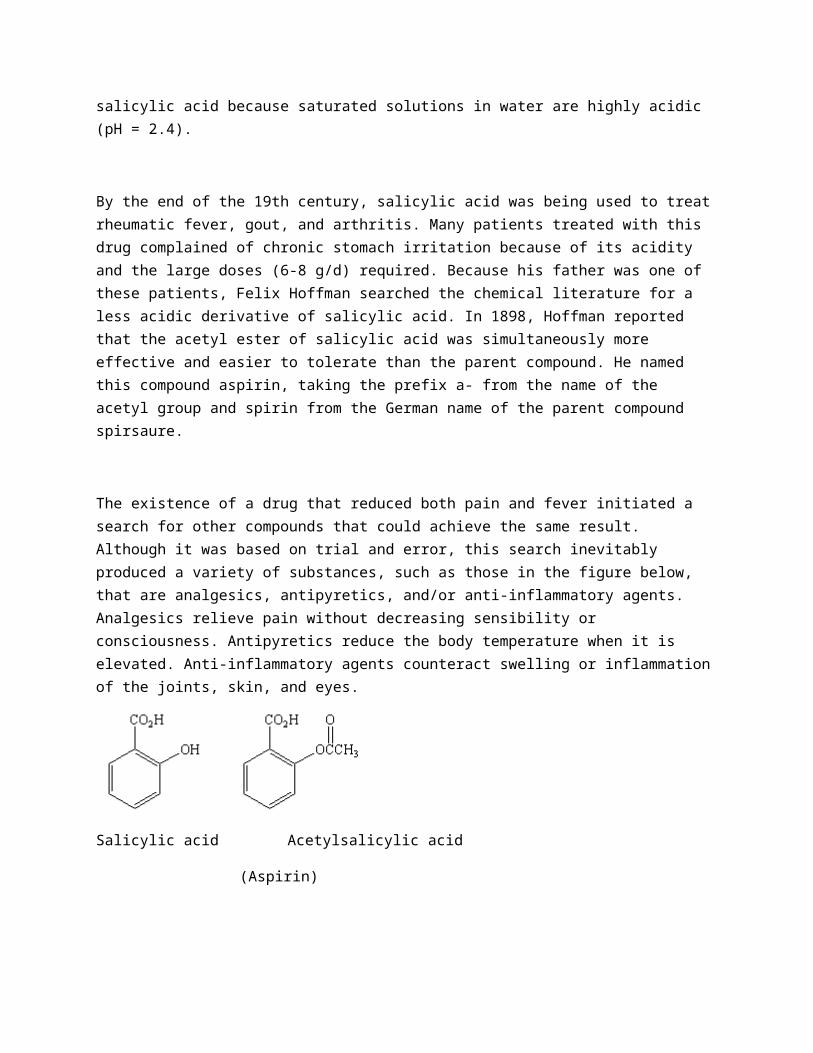
Salicylic acid Acetylsalicylic acid
(Aspirin)
Acetaminophen
(Tylenol) Ibuprofin
(Motrin, Advil)
Although the use of aspirin has been widespread since the 19th century, the mechanism for its action was first described in 1971 [J. R. Vane, Nature, 231(25), 232-235 (1971)]. Vane noted that injury to tissue was often followed by the release of a group of hormones known as the prostaglandins, which have wide-spread physiological effects at very low concentrations. The prostaglandins regulate blood pressure, mediate the inflammatory response of the joints, induce the process by which blood clots, regulate the sleep/wake cycle, and, when appropriate, induce labor.
Vane suggested that aspirin and other nonsteroidal anti-inflammatory drugs (or NSAID's) inhibit the enzyme that starts the process by which prostaglandins such as PGE2 and PGF2 are synthesized from the 20-carbon unsaturated fatty acid known as arachidonic acid shown in the figure below. The steroidal anti-inflammatory drugs (such as hydrocortisone) achieve a similar effect by inhibiting the enzyme that releases arachidonic acid into the cell.
PGE2 PGF2a
Now that they are beginning to understand the mechanism by which drugs operate, medicinal chemists can approach the design of drugs by a rational process. A recent paper described progress toward the design of a drug to treat the debilitating diseases caused by protozoan parasites that afflict millions of people in Latin America, Africa, and Asia [W. N. Hunter, et al., Journal of Molecular Biology, 227, 1992, 322-333]. The potential target for this drug is an enzyme trypanothione reductase (TR) that protects the parasite from oxidative damage from the immune system of its mammalian host. Mammalian cells use a similar enzyme, known as glutathione reductase (GR), to protect against damage from oxidation reactions.
Hunter and coworkers found that the human GR enzyme has a smaller, more positively charged active site than the TR enzyme in the parasite. The structural information in this study can now be used to rationally modify a substrate of these enzymes until it possesses the following characteristics.
The substrate must be too large to bind to the GR enzyme in humans.
The substrate must have a high affinity for binding to the TR enzyme in the parasite.
The substrate must inhibit the activity of the TR enzyme, thereby allowing the immune system of the mammalian host to attack and eventually destroy the parasite.
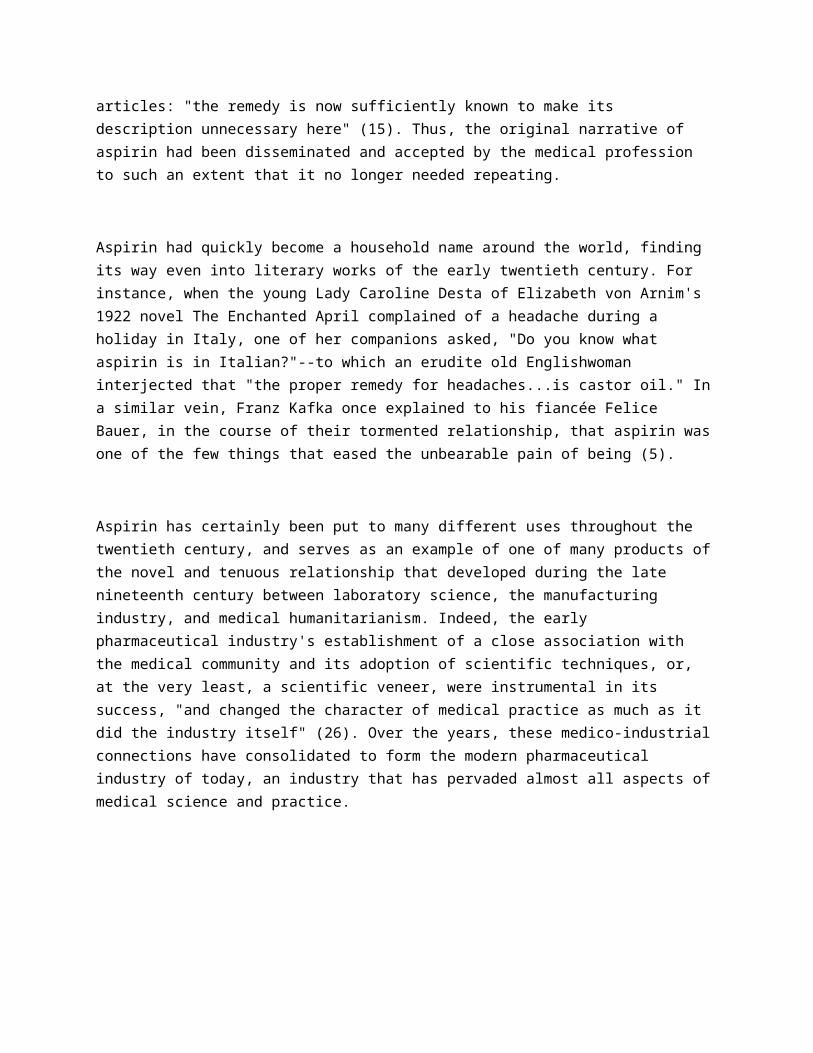
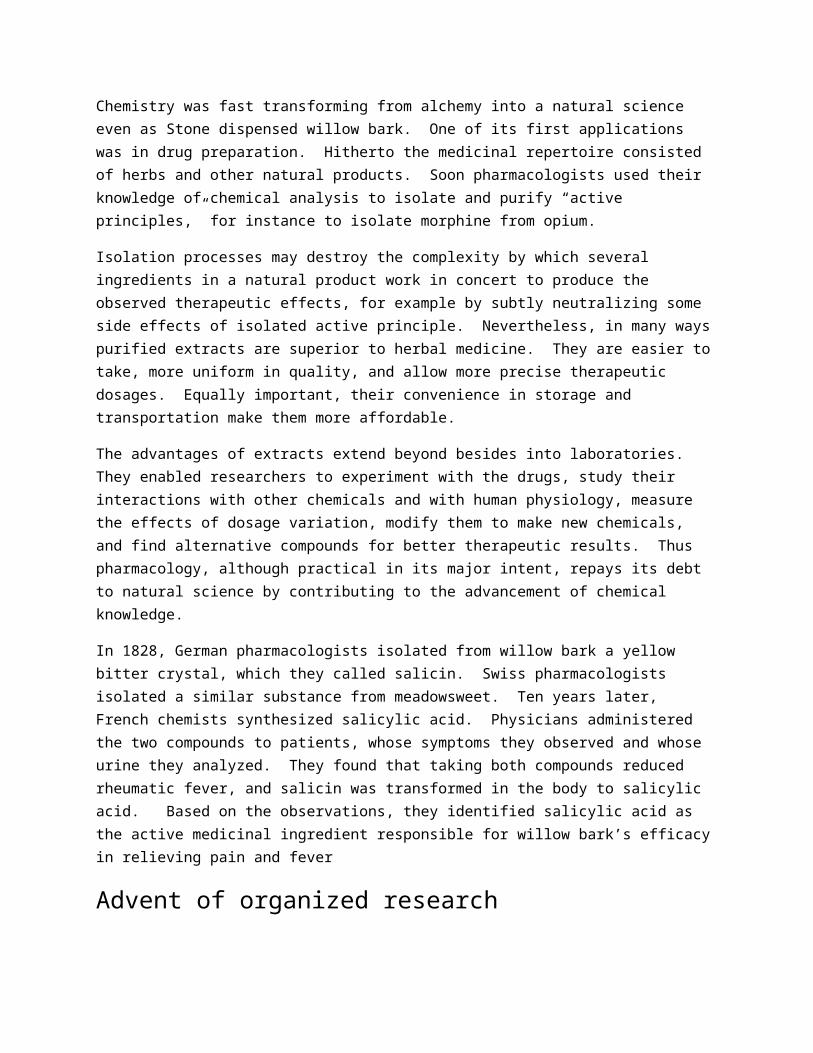
Aspirin crystals
Aspirin was originally extracted from willow bark but is actually produced in all plants as a defence mechanism in response to damage or attack. Much higher levels are therefore found in less than perfect fruit and vegetables. Aspirin is used to treat pain, reduce fever, and prevent heart disease and cancer. Some people think it should be reclassified as a vitamin.
Colour-enhanced scanning electron micrograph by Annie Cavanagh and Dave McCarthy.
B0006253
Politics is down there in the laboratory."
--Bruno Latour (1).
Aspirin is a product of the late-nineteenth-century laboratory, pharmaceutical industry, and medical community. The prevailing scientific techniques, industrial approaches, and medical beliefs were

instrumental in the development, promotion and reception of the drug. As a result, the present account does not extend further back than a few decades prior to the release of aspirin from the laboratories of Farbenfabriken vormals Friedrich Bayer & Co. in 1899. In contrast, much of the current literature on aspirin (2,3,4) attempts to trace the compound back to antiquity through the Ebers papyrus, the Hippocratic writings, and the works of Galen. Such histories tell a simple, linear tale of the numerous "discoveries" proposed to have led to the use of certain salicylate-containing plants, such as willow bark and wintergreen, or salicylate-related compounds, including salicilin and salicylic acid, as cures for a variety of ailments. Indeed, according to Mann and Plummer:
Both [salicilin and salicylic acid] attacked fever and pain, and their partisans advocated the salicylates' use as antiseptics, mouthwashes, and water preservatives for ocean voyages; one important chemist further suggested (erroneously) that sodium salicylate, a chemical relative, would successfully treat scarlet fever, diphtheria, measles, syphilis, cholera, rabies and anthrax (5).
However, it is difficult to establish what effect, if any, these examples of the "historical" uses of
"proto-aspirin" had on the impetus for and modes of developing and using the actual drug called aspirin. As a matter of course, aspirin is usually described as the natural descendant from these salicylate forefathers. However, the history of aspirin is not as straightforward a tale as conventional histories suggest, but rather is a complex narrative of the people and circumstances involved in transforming a simple chemical compound into a popular pharmaceutical product that has remained one of the most widely consumed drugs for almost a century.
Bayer began in 1863 as Friedrich Bayer & Co., a dye-manufacturing plant in Germany. When the dye industry began to wane during the late 1880s, Bayer made the transition into the more active and lucrative sector of pharmaceuticals by developing, producing, and marketing phenacetin (acetophenetidin) from a dye-making by-product. The company's switch from dyes to pharmaceuticals was so rapid that the first lots of the drug were alkylated in make-shift containers--empty beer bottles wrapped in towels--before the company decided to invest in suitable equipment and proper facilities for its production (6). However, despite the change in the products being manufactured, Bayer retained many of the methods used previously in the sale of dyestuffs in highly competitive markets: sales representatives, advertisements in trade journals, and the use of patents and trade names. As McTavish, a noted medical historian, remarks:
By restricting its market to the pharmaceutical and medical professions, the chemical industry avoided the unseemly trappings of the nostrum trade and established itself as a member of the 'ethical' fraternity (7).

From then on, McTavish affirms, "[drug production] took place in an industrial setting. Drugs were commodities similar in most respects to any other commodity: they were manufactured for profit" (7). During the 1890's, Carl Duisberg and other key figures at Bayer were busily involved in reorganizing the company, in setting up pharmaceutical laboratories for the development and standardization of drugs, and, most importantly, in establishing links with the medical world.
The late nineteenth century saw an unprecedented rise in the number of new pharmaceutical products on the market. One physician in 1889 commented: "Every week, almost every day, brings its new drug, each in turn praised as being the greatest discovery of modern therapeutics" (8). McTavish attributes this tremendous influx of new products to "the increasing industrial role of the laboratory, especially in the drug industry" (7). However, the utility of these novel therapeutic products in medical practice was a source of great debate. Certain physicians staunchly opposed what they saw as "the growing tendency among German medical men to convert the 'Republic of Science' into a commercial oligarchy for the benefit of plutocrats at the expense of suffering humanity" (7). Others were more accepting of the new developments, but remained wary of those who hailed new compounds as milestone drugs or panaceas, "lest they bring into discredit both their own calling and that of the pharmaceutical chemist" (9). In an address on the Progress of Medicine in the Nineteenth Century, Dr. F. Roberts confessed:
Out of the enormous number of medicinal agents brought under our notice by puffing advertisements in the press, medical as well as lay, by pamphlets or even large books delivered by post, or by actual 'specimens for trial' which are nowadays so liberally delivered at our residences, comparatively few hold their ground, or stand a fair and candid criticism and investigation of their vaunted merits. Still a certain proportion do and I see every reason to anticipate that, as the result of the systematic researches, scientific and practical, now carried on in so many laboratories, valuable additions will be made from time to time to the medicinal agents at our disposal for the help and comfort of our patients. I only hope that in our love for the new we will not entirely throw out old friends which have done real and effective service in the past and are today as deserving of our regard as ever (10).
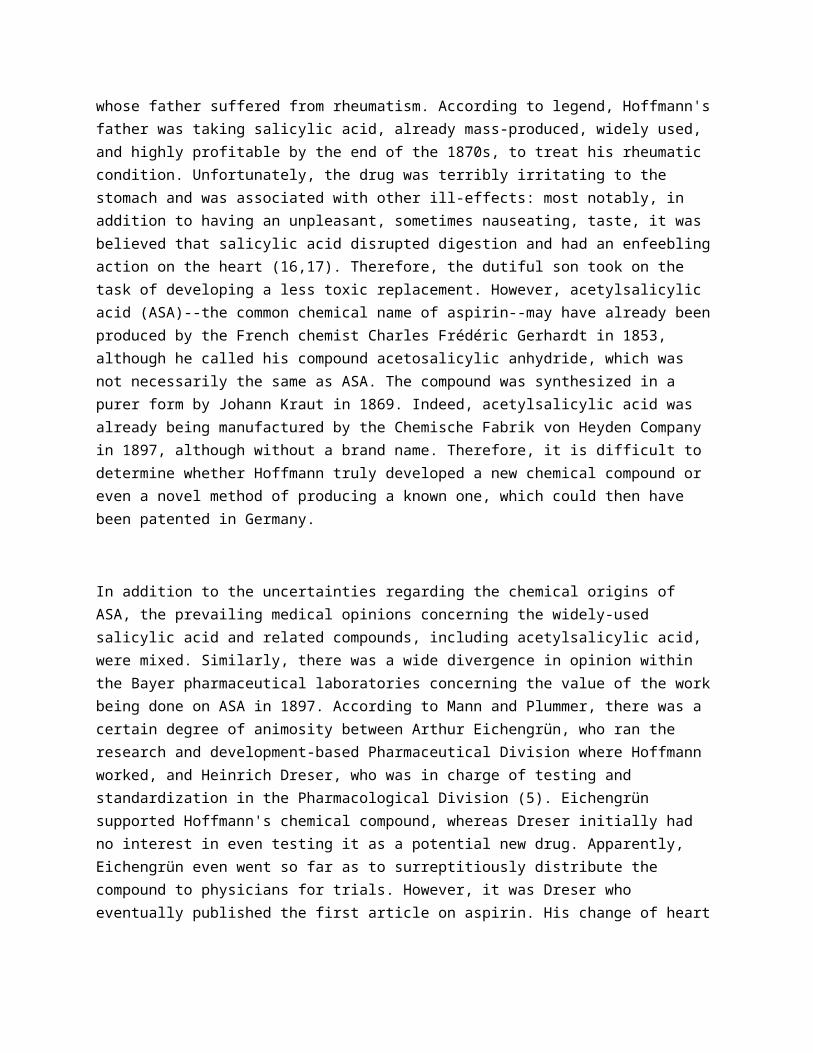
Therefore, for those pharmaceutical companies that had managed to establish a place for themselves within the medical community, drug production became a legitimate science-based industry, whereby manufacturers and medics engaged in a profitable producer-consumer partnership. For instance, as written in the Lancet in August 1899, many new pharmaceuticals were the product of the increased attention paid "to the toleration of drugs and to the avoiding of effects which are undesirable" (11). Furthermore:

Modification of the salicylates and the introduction of new morphine derivatives [which were both activities carried out in the Bayer laboratories] occur as single examples. In these matters it is satisfactory to find that the pharmacist is guided by the medical man and not solely by a knowledge of the chemistry of the principles concerned (11).
Thus, the inspiration and drive to produce aspirin can be explained in terms of a medico-industrial relationship in which the pharmaceutical companies supplied products that interested the doctors, and the doctors, in turn, maintained an active interest in what the pharmaceutical companies had to offer.
During the 1880s and 1890s, when physicians became intensely interested in the possible adverse effects of fever on the human body, the use of antipyretics became one of the hottest topics in therapeutic medicine. According to one pharmacology textbook published at the beginning of the 20th century:
From the highest to the lowest in the profession, the fad was to regard fever as the most deleterious factor in a case, and to treat it as if it were a part of the disease, or the disease itself, instead of a symptom of almost all infections, and one which in itself is not capable of doing harm, unless it is excessive or very prolonged. [It was believed] that not only did fever, when sufficiently high, coagulate the protoplasm of vital parts, but that the patient was having his tissues burnt up, and that this excessive combustion, or conflagration, must be arrested even though the disease spent itself unaltered in its other clinical manifestations and pathological tendencies. The discovery by numerous laboratory investigations that this group of drugs decreased heat production, and increased heat dissipation, seemed to fit them in a peculiar manner to meet the therapeutic needs of the hour, and they were tested on a scale of experimental therapeutics hardly before equaled. At first, cases of untoward effects were frequently recorded, with fortunately very few fatal cases. Often these effects were due to heroic doses; in other cases, when patients in low fevers received the drug, the fall in temperature which succeeded produced collapse; while in maladies like pneumonia, with deficient aeration of the blood, or other pulmonary affectations, cyanosis, excessive sweating, and feebleness of the circulation occurred (12).
Therefore, until the fever fad ended at the turn of the century, most likely as a result of the increasing popularity of the germ theory, most physicians concentrated their efforts on treating pyrexia. The drug companies responded to the medical demands of the day by catering to, and perhaps even fueling the fires of, the antipyretic era. New antipyretics and analgesics--most drugs in this class were believed to possess more or less of both properties--were introduced monthly: "those coal-tar crystalline products which have almost deluged the market as quinine substitutes, [were] being offered from time to time as

analgesics, anodynes, antipyretics, as the case may be" (13). Moreover, most of these new therapeutic compounds were commonly promoted as and subsequently referred to by catchy brand names such as malarin, pyrantin, cosaprin, phesin, eupyrine, and, of course, aspirin (14).
Still, it is not exactly clear how aspirin came to be. Many give the title of "discoverer of aspirin" to Felix Hoffmann, a chemist at Bayer whose father suffered from rheumatism. According to legend, Hoffmann's father was taking salicylic acid, already mass-produced, widely used, and highly profitable by the end of the 1870s, to treat his rheumatic condition. Unfortunately, the drug was terribly irritating to the stomach and was associated with other ill-effects: most notably, in addition to having an unpleasant, sometimes nauseating, taste, it was believed that salicylic acid disrupted digestion and had an enfeebling action on the heart (16,17). Therefore, the dutiful son took on the task of developing a less toxic replacement. However, acetylsalicylic acid (ASA)--the common chemical name of aspirin--may have already been produced by the French chemist Charles Frédéric Gerhardt in 1853, although he called his compound acetosalicylic anhydride, which was not necessarily the same as ASA. The compound was synthesized in a purer form by Johann Kraut in 1869. Indeed, acetylsalicylic acid was already being manufactured by the Chemische Fabrik von Heyden Company in 1897, although without a brand name. Therefore, it is difficult to determine whether Hoffmann truly developed a new chemical compound or even a novel method of producing a known one, which could then have been patented in Germany.
In addition to the uncertainties regarding the chemical origins of ASA, the prevailing medical opinions concerning the widely-used salicylic acid and related compounds, including acetylsalicylic acid, were mixed. Similarly, there was a wide divergence in opinion within the Bayer pharmaceutical laboratories concerning the value of the work being done on ASA in 1897. According to Mann and Plummer, there was a certain degree of animosity between Arthur Eichengrün, who ran the research and development-based Pharmaceutical Division where Hoffmann worked, and Heinrich Dreser, who was in charge of testing and standardization in the Pharmacological Division (5). Eichengrün supported Hoffmann's chemical compound, whereas Dreser initially had no interest in even testing it as a potential new drug. Apparently, Eichengrün even went so far as to surreptitiously distribute the compound to physicians for trials. However, it was Dreser who eventually published the first article on aspirin. His change of heart regarding the value of this compound likely reflects his own financial interests, since, according to Mann and Plummer:
[Hoffmann and Eichengrün] had contracts with Bayer by which they would receive a royalty on any patentable product they invented. Since there was no patent, neither of them received any royalties from the sale of aspirin in Germany. However, Heinrich Dreser had an agreement with Bayer by which he would receive a royalty on any product that he introduced. Thus he received a very substantial royalty for aspirin and was able to retire early a very rich man (5).
As suggested in the July 1899 issue of the Lancet:
No one [in the pharmaceutical industry] would undertake the irksome task of making new products known to the medical profession without being, whether rightly or wrongly, convinced of their superior properties (17).
Therefore, once Dreser finally chose to promote Hoffmann's chemical compound as aspirin, he certainly built up a strong case for its superiority over other available remedies.
In his article published in the Archiv fur die Gesamte Physiologie in 1899, Dreser begins by describing the unsatisfactory nature of the drugs then available, thereby creating the need for new alternatives:
In many diseases related to common cold, the use of sodium salicylate would be definitely much more popular if it would not provoke strong rejection by its disgusting sweet taste which can be corrected only to some extent (18).
Dreser then suggests:
Pharmacological chemistry should develop synthetically a new preparation which would avoid in addition to the disgusting sweet taste other undesirable characteristics such as the overloading of the stomach. After resorption, the active salicylate should be rapidly split off from the new product.
These improvements are precisely what Dreser claims to have achieved through the synthesis of aspirin. First, the taste was refined by masking the free phenolic hydroxyl group of salicylic acid through substitution of the hydrogen atom with a methyl group. To prove that aspirin is reabsorbed and cleaved into salicylic acid, Dreser cites the work of the German scientist Lesnik published in the Archiv fur Experimentelle Pathologie und Pharmakologie to maintain that the increase of nitrogen in the urine "could be due only to the nitrogen-containing metabolic product of salicylic acid . . . also clearly shown by aspirin."

Dreser then carried out comparative studies of aspirin and other salicylates to demonstrate that the former was less noxious and more beneficial than the latter. For instance, he tested the sodium salt of aspirin and sodium salicylate on normal rabbits and on cold-blooded animals, which, to his mind, "showed clearly that aspirin is less poisonous than salicylic acid." Dreser also tested aspirin on the most fine and delicate tissues, such as the gills of fish, to further demonstrate the gentleness of the compound. Finally, to put to rest any fears that aspirin might depress the heart, he conducted experiments to show that sodium salicylate decreased cardiac output, whereas the sodium salt of aspirin increased it. Dreser concludes his article as follows:
Summing up the most important pharmacologic characteristics of aspirin we may suggest the following: The aspirin has a more pleasant harsh acidic taste than sodium salicylate before resorption. It is also more protective to the stomach wall according to the above experiments. It is very advantageous, furthermore, that aspirin is split by the gastric hydrochloric acid only to a small extent (0.2%). Differences are evident between aspirin and sodium salicylate also after resorption... (18).
By publishing these findings in a physiological journal, Dreser was able to provide a "scientific" and "objective" account of this new compound as a potentially powerful pharmaceutical product with few side-effects. At the same time, he was one of the top employees at Bayer, and would therefore benefit personally from the success that his pharmacological analysis had brought upon aspirin.
In concert with Dreser's efforts, physicians were co-opted into supporting the effectiveness and harmlessness of aspirin. Two such doctors cited in Dreser's article were Dr. C. Witthauer, who published a paper on his experiences with aspirin in Die Heilkunde in April 1899, and Dr. Julius Wohlgemuth, who had his results published in Therapeutische Monatshefte in May of the same year. Both Witthauer's and Wohlgemuth's articles (19,20) provide a general introduction to the novel powder, corroborate Dreser's findings, and describe the results of clinical trials with aspirin. Unequivocally, they conclude that the new drug is superior to the other pharmaceutical products then available.
The elegance of the early medical and pharmaceutical reports lies in their ability to ally aspirin with the already widely accepted salicylic compounds, whilst concurrently presenting aspirin as distinct from them. Thus, the new drug possessed a certain familiarity, and more importantly, the manufacturers could then claim the proven medicinal properties of salicylic acid and related compounds by association. However, it was equally important to disassociate aspirin from the negative qualities that had been attributed to these products through the development of scientific truths in the laboratory which attested to such differences. In this way, a white powder that had spent many years collecting dust on a shelf along with hundreds of other chemical compounds stored at Bayer was transformed into a
substantive pharmaceutical product. Since then, each new report by members of the medical community or pharmaceutical world has expanded and altered the ever-growing narrative on aspirin.
On July 22, 1899, aspirin was featured in the "Analytical Records from the Lancet Laboratory" along with several other products that had undergone the rigors of scientific analysis: an old pale cognac found to be suitable for medicinal purposes; Johannis potash water, a diuretic and alkaline treatment; Sandron's iron tonic, which was found to contain a very small quantity of iron; and finally, two specimens of Scotch whisky. The journal's announcement of The Bayer Company's latest drug resembled, in both content and intent, the articles published previously by Dreser, Witthauer, and Wohlgemuth. Within a few years, a barrage of articles singing the praises of aspirin had been published. The clinician Floeckinger even went so far as to take two large doses of aspirin himself: first 75 grains and then another 60 grains (21). After the first dose he found himself "without toxic effects, except violent headache and tinnitus" which lasted for 16 hours, until it subsided following profuse sweats. After the second dose, Floeckinger experienced "increased pulse, reduced temperature, and flashes of light before the eyes." Nonetheless, Floeckinger concludes his article as follows:
[It] presents several advantages over salicylic acid. It does not irritate the stomach. There is no cardiac depression. In ordinary doses there is no tinnitus or headache...and [it] is best prescribed in wafers or sachets for acute and chronic rheumatism, polyarthritis, and pleurisy...but it is ineffective in neuralgias and pleurodynia (21).
Any adverse effects experienced when taking aspirin were attributed not to this new drug, but rather to extrinsic factors, such as the medium of administration or the magnitude of the dose. Although certain physicians claimed that "some observers--Osler, for instance--recognize little or no advantage in salicylates beyond some power in relieving pain" (15), most physicians strongly supported aspirin as a valuable addition to the pharmacopoeia.
Soon after its release onto the market, aspirin began to appear in the new pharmacological texts. Nonetheless, there were still many recent and reputable works that did not mention Bayer's new drug (12,22,23). Indeed, even when aspirin was included in these works, it was not always cited for use in treating ailments with which one now associate the drug. The Index of Diseases and Remedies in an American textbook on materia medica, pharmacology and therapeutics, for example, cites aspirin for the treatment of certain diseases, but does not prescribe it as a general substitute for salicylic acid and the other salicylates. The text lists salicylic acid as a drug useful for burns, eczema, ephelides (freckles), lupus vulgaris, pertussis, and ulceration. Salicilin, salol, salipyrin, and other salicylates are recommended for different disorders such as chorea, diabetes mellitus, endocarditis, fever, pharyngitis, and pleurisy,

whereas aspirin is recommended, in addition to other drugs, in the treatment of influenza, neuralgia, and neuritis (24).
Indeed, within the first five years after its release, aspirin was seen less and less as an antipyretic, and was increasingly prescribed for the relief of pain. By 1903, "numerous observations had been made on the analgesic effect of aspirin in neuralgias and other painful affectations," including carcinoma (25). In this way, aspirin was similar to its predecessor phenacetin, which "found its birth in what may be called the antipyretic era [of the 1880s and 1890s, and] like its relatives has come to be employed chiefly for the relief of pain" (12). The shift in interest from the antipyretic to the analgesic properties of these drugs in the early twentieth century is best summarized by the entry in the Text-book of Pharmacology and Therapeutics of 1901:
As the fad for antipyresis waned by its loss of novelty, physicians began to ask each other whether these drugs which acted so well in reducing fever had any influence in shortening the course of the disease, and it was speedily determined that they did not. Simultaneously, the increasingly thorough investigations into the pathology of fever, and our increased knowledge of the life history of the organisms causing disease, made it clear that fever was a comparatively unimportant factor in a given case, unless excessive; and it begins to be apparent that fever is not only not a peculiarly harmful process, but in some cases may be actually of value... Finally, the recollection of the fact that the use of these drugs necessitates their absorption and elimination, changed or unchanged, and that in these processes they may be guilty of a deleterious influence, has still further decreased their popularity as antipyretics, while the discovery that all of them possess pain-relieving properties has also diverted attention to their use for other purposes than antipyresis (12).
Thus, the uses of aspirin changed with the changing trends in the medical profession, becoming progressively less linked to the drug's initial description and indications first marketed by the pharmaceutical company. The original experiments conducted on aspirin in the Bayer laboratory were superceded by more recent clinical findings conducted by medical men not affiliated with the pharmaceutical company. Gradually, all the stories told by those who had been instrumental in presenting and promoting acetylsalicylic acid as aspirin faded into the background. By 1903, authors no longer felt the need to include comprehensive profiles of aspirin in their articles: "the remedy is now sufficiently known to make its description unnecessary here" (15). Thus, the original narrative of aspirin had been disseminated and accepted by the medical profession to such an extent that it no longer needed repeating.
Aspirin had quickly become a household name around the world, finding its way even into literary works of the early twentieth century. For instance, when the young Lady Caroline Desta of Elizabeth von Arnim's 1922 novel The Enchanted April complained of a headache during a holiday in Italy, one of her companions asked, "Do you know what aspirin is in Italian?"--to which an erudite old Englishwoman interjected that "the proper remedy for headaches...is castor oil." In a similar vein, Franz Kafka once explained to his fiancée Felice Bauer, in the course of their tormented relationship, that aspirin was one of the few things that eased the unbearable pain of being (5).
Aspirin has certainly been put to many different uses throughout the twentieth century, and serves as an example of one of many products of the novel and tenuous relationship that developed during the late nineteenth century between laboratory science, the manufacturing industry, and medical humanitarianism. Indeed, the early pharmaceutical industry's establishment of a close association with the medical community and its adoption of scientific techniques, or, at the very least, a scientific veneer, were instrumental in its success, "and changed the character of medical practice as much as it did the industry itself" (26). Over the years, these medico-industrial connections have consolidated to form the modern pharmaceutical industry of today, an industry that has pervaded almost all aspects of medical science and practice.
The story of aspirin--its origins, popularization, and varied uses--is rather unique:
Few groups of drugs have provided the manufacturers with such fortunes, physicians with such therapeutic resources, and the laity with so many semi-proprietary remedies as have the so-called antipyretic or analgesic derivatives of coal tar. Nor is there any group which illustrates so well the close relationship between chemistry and practical therapeutics, and the relation of chemical constitution to physiological action (12).

Yet, the story of aspirin to a great degree epitomizes the stories of many pharmaceutical products developed both for increased therapeutic efficacy and for profit. The histories of these products generally share certain themes. The usually vague and contentious origins of a drug soon become overshadowed by the multitude of clinical reports produced with the help of medical allies. Extensive clinical trials serve to introduce new drugs to the greater medical community, to specific patient groups, and eventually, to the population at large. As the years pass, however, many drugs are used to treat diseases different from those for which the drugs were originally intended. For example, with the advent of the "anti-coagulant era," aspirin has acquired new indications as a platelet anti-aggregant, and is already widely used in the prophylaxis and treatment of strokes and myocardial infarcts. Therefore, drugs currently being produced and prescribed remain a reflection of the ever-changing state of medical knowledge and of the pharmaceutical industry's eagerness to meet the needs of the day.
As the quest for more potent and less toxic drugs continues in the age of rational therapeutics, advanced technology, and designer drugs, the treatment of disease continues to be shaped by the symbiotic relationship between physicians and pharmaceutical companies forged a century ago
ACKNOWLEDGMENTS
History of aspirinA wonder drug and its family
To find a story that provides a thumbnail illustration for the nature and progress of worldly science, one needs to look no further than the medicine cabinet of any home. Chances are it contains aspirin. If not, then look for one of aspirin’s many cousins, pain killers that, despite their long and widespread usages, never cease to make headline news.
After eons of prehistory as folk remedy, aspirin emerged in 1899 in one of the world’s first industrial research laboratories. Aspirin has many therapeutic effects. At over-the-counter dosage (one or two grams), it relieves fever and minor aches and pains. At dosages three or four times higher, available by prescription only, it reduces swelling and is used to treat gout, rheumatoid arthritis, and inflammatory ailments.[i] Many people take low dosages (below 100 milligrams) daily for preventing recurrent stroke or heart attack.[ii] Recent studies found it effective in reducing risks for colon and breast cancers.[iii] Evidence is accumulating for similar effects in Alzheimer and other diseases.[iv]
A great complaint against aspirin is that it irritates the stomach and in some cases cause ulcer and internal bleeding. Despite these and other undesirable side effects, it is widely used. It made the 1950 Guinness Book of Records as the world’s most popular pain-killing drug. Now more than 80 million tablets of it are being consumed every day in the United States alone, and for many more purposes.
Success breeds competition. Some fifty cousins of aspirin exist, most of which appeared after World War II. Together they constitute a family known as non-steroidal anti-inflammatory drugs (NSAIDs). Popular over-the-counter NSAIDs include aspirin (Bayer, Ecotrin), ibuprofen (Advil, Motrin), and naproxen (Aleve).[v] Many more are available by prescription. They have different chemical structures. Yet they all suppress pain, fever, and inflammation and irritate the stomach to various degrees.
A new lineage nicknamed “super aspirin” appeared at the end of the twentieth century. Coxib (Celebrex, Vioxx) achieves similar therapeutic profiles as the old NSAIDs but is gentler on the stomach. These drugs are rationally designed based on scientific knowledge, but alas, they have their own shortfalls.[vi]
While consumers are happy that aspirin works so well in so many areas, scientists are excited in understanding how it works and finding ways to make it work better. They have come a long way since the 1970s and realize that many more secrets await discovery. Aspirin itself is a small chemical molecule, the properties of which have been known for more than a century. However, the living body with which it must interact as a medicinal agent is most complex and not well understood despite scientific advancement. Aspirin research involves many approaches that will be discussed in more details later in the book: cut and try, educated guess, breakthroughs and setbacks, laboratory experiments, theories and controversies, synthesis of knowledge from many disciplines, clinical trials with definitive or inconclusive results, and judgments based on incomplete knowledge.
Contrary to the stereotype of applied science as perfunctory deployment of complete knowledge swayed only by cultural tastes, aspirin tells how judicious applications themselves demand and generate new scientific knowledge. Its story reveals worldly science as a trustworthy friend in the tough journey of life. As you make your way through the knotty problems of the world, you develop a deeper understanding of your friend, the world, and perhaps yourself, so that you are better prepared for the new problems to come.
From folk remedy to pure chemical
Aspirin is the generic medical name for the chemical acetylsalicylic acid, a derivative of salicylic acid. Compounds of salicylic acid are found in some plants, notably white willow and meadowsweet (Spirea ulmaria). Acetyl- and spirea inspired the name aspirin.[vii]
The medicinal effects of the plants were discovered by people through life experiences. An Egyptian papyrus prescribed willow leaves for fever and swelling. The Greek Hippocrates, who was honored as the father of medicine, recommended willow bark for pain and fever. Medieval medical scripts contained many references to the plant.
Willow bark made its way into scientific literature in 1763 through the work of English vicar Edmund Stone. It had been among folk remedies of rural workers. Stone decided to pick it out for study because he believed that remedies came in the vicinity of ailments and observed that both willows and fevers occurred commonly in swampy areas. He dispensed a fixed amount of willow bark powder every four

hours to many feverish patients, recorded the results, and wrote a letter complete with a speculative explanation of its efficacy to the Royal Society of London. The specific explanation he gave turned out to be wrong and his clinical method was crude. Nevertheless, his systematic approach and attempt at a principled explanation were close to that of science.
Chemistry was fast transforming from alchemy into a natural science even as Stone dispensed willow bark. One of its first applications was in drug preparation. Hitherto the medicinal repertoire consisted of herbs and other natural products. Soon pharmacologists used their knowledge of chemical analysis to isolate and purify “active principles,” for instance to isolate morphine from opium.
Isolation processes may destroy the complexity by which several ingredients in a natural product work in concert to produce the observed therapeutic effects, for example by subtly neutralizing some side effects of isolated active principle. Nevertheless, in many ways purified extracts are superior to herbal medicine. They are easier to take, more uniform in quality, and allow more precise therapeutic dosages. Equally important, their convenience in storage and transportation make them more affordable.
The advantages of extracts extend beyond besides into laboratories. They enabled researchers to experiment with the drugs, study their interactions with other chemicals and with human physiology, measure the effects of dosage variation, modify them to make new chemicals, and find alternative compounds for better therapeutic results. Thus pharmacology, although practical in its major intent, repays its debt to natural science by contributing to the advancement of chemical knowledge.
In 1828, German pharmacologists isolated from willow bark a yellow bitter crystal, which they called salicin. Swiss pharmacologists isolated a similar substance from meadowsweet. Ten years later, French chemists synthesized salicylic acid. Physicians administered the two compounds to patients, whose symptoms they observed and whose urine they analyzed. They found that taking both compounds reduced rheumatic fever, and salicin was transformed in the body to salicylic acid. Based on the observations, they identified salicylic acid as the active medicinal ingredient responsible for willow bark’s efficacy in relieving pain and fever
Advent of organized research
Scientists extract or synthesize spoonfuls of a chemical and are happy that it suffices for laboratory experiments. As a useful drug for the mass of people, however, large quantity of the stuff at reasonable prices is required. To develop cost effective processes for mass production, science and technology again come into play.
Soon after chemical extracts and synthetics appeared, they were in demand. Supply of drugs came from two kinds of companies, pharmacies and chemical manufacturers. Some pharmacies, which traditionally prepared the portions prescribed by physicians, set up laboratories and factories and morphed into pharmaceutical firms. Among them was Merck, an early seller of salicin. As foundation of the modern science-based pharmaceutical industry, however, pharmacies were perhaps less important than
manufacturers of fine chemicals – to this day the U.S. national accounting classifies pharmaceuticals under “chemicals and allied products.”[viii]
The first fine chemicals to have wide social impacts were dyes, which brightened life by turning drab garments into a rainbow of colors. The dyes industry grew up alongside organic chemistry in the second half of the nineteenth century. Their mutual stimulations exemplified the coupled dynamics of science and business. Dyes are complex organic chemicals. Much technical knowledge is required to find dyes for desirable colors, make them adhere to popular fabrics, and ensure their color-fastness. To meet these challenges the German firms that manufactured dyes from coal tar initiated organizational innovations of lasting impact. They invented industrial research laboratories and forged close ties with research universities, which emerged around the same time. These institutions contribute crucially to the enabling environment in which worldly sciences thrive.[ix]
Anyone who has tried to wash stained hands knows the affinity of dyes to living tissues. Scientists went one step further and put the knowledge to use. Since 1849, they had been using dyes to stain otherwise colorless biological specimen and make them visible under the microscope. Noting the different susceptibilities of various cells and bacteria to various dyes, they developed differential staining criteria to identify and classify types of cell, for example, a particular staining differentiates two kinds of bacteria with different cell walls. Toward the end of the century Paul Ehrlich and other chemists suggested that staining was a chemical reaction between a dye and a bacterium or a cell. Because cells were susceptible to specific staining, perhaps dyes may be harnessed for chemotheurapeutic purposes.[x] Such ideas were not lost on the dyes firms. As the market for dyes matured, those looking to diversify turned their scientific and organization prowess to drug development.
Bayer was one of three leading research-intensive dyes firms. Its research supervisor Carl Duisberg, a chemist who later became the firm’s chief executive, contributed much to instituting the organization of modern industrial research. He directed company researchers into the drug area, and after initial sucesses set up in 1896 an independent drug laboratory. It had a pharmaceutical division for drug discovery, directed by Arthur Eichengrün, and a pharmacological division for testing the drugs, directed by Heinrich Dreser.
Among Eichengrün’s first ideas was to find a derivative of salicylic acid that would be as therapeutically effective but with less undesirable side effects. He hired a young chemist Felix Hoffmann who, because of his arthritic father, had a personal passion in the project. Hoffmann came up with acetylsalicylic acid.[xi]
At first acetylsalicylic acid failed even to win everyone at Bayer. Eichengrün tested it on himself and pushed it vigorously. Dreser thought it was just a better-tasting salicylic acid unworthy of production. As the two heads of research quarreled, acetylsalicylic acid languished on the shelf. Finally Duisberg stepped in and had it tested by outside pharmacologists and physicians. They brimmed with enthusiasm. Dreser changed his mind and published a paper that did not mention Eichengrün and Hoffmann. Bayer launched acetylsalicylic acid as a commercial drug in 1899 under the name Aspirin.
Research, development, marketing
Three innovations of the dyes industry became invaluable legacies of the pharmaceutical industry. The first was research and development, of which aspirin was among the first pharmaceutical products. Emphasis on science and research remains a distinctive tradition of the pharmaceutical industry.
The second innovation was in marketing. The dyes industry pioneered the practice of targeting not ordinary consumers but professionals. It hired technical salesmen to explain to other technicians how to use various dyes on various fashionable fabrics. Adapting this approach, Bayer mounted an extensive sales campaign for aspirin targeting physicians. It initiated the drug marketing strategy “to help doctors to help their patients,” which thrives alongside advertisements prompting consumers to “ask your doctor about it.”[xii]
The dyes industry was also in the forefront in asserting intellectual property rights. Favorable patent laws play important roles in the pharmaceutical and life science industries; witness the recent scramble to patent human genes.[xiii] However, they did not benefit aspirin. Bayer settled for registering a trademark for the name Aspirin.[xiv] It did not patent acetylsalicylic acid, not because it would not but because it could not. The chemical was old stuff, synthesized by French chemist Charles Frederic Gerhardt back in 1853.
The significance of Bayer’s work on aspirin lies not in the discovery of a chemical compound but in the development of a compound into a useful drug. Turning a chemical into a drug calls for extensive research to identify its potential applications and markets, evaluate its clinical effects, optimize its properties, and design efficient manufacturing processes. The research generates application related knowledge that marks the difference between discovering something and discovering it as something useful, or between pure and worldly sciences.
To discover what a thing is good for requires knowledge about relevant situations, which are often subtle and difficult. Lack of such knowledge partly explains why many chemicals sat on the shelf for decades before their therapeutic values were realized. This happened to aspirin’s rival Tylenol. Its active ingredient was synthesized in 1878, but had to wait until 1955 before being developed into a popular drug.[xv] Ever more revealing are the stories of antibacterial drugs. Sulfanilamide was synthesized in 1908, but it was the discovery of its therapeutic effectiveness in 1932 that won a Nobel Prize. Penicillin was discovered in 1928 and its therapeutic properties in 1939, and both discoveries were cited in the Nobel Prize. In Nobel Prizes such as these, the scientific community acknowledges the equal scientific importance of discovering and developing a drug. Unfortunately, this point is often overlooked in science studies, so that Hoffmann is often accorded with the credit for aspirin, to the neglect of Eichengrün and others in Bayer.[xvi]
The importance of analytic techniques
Aspirin works. Willow bark works; it is available as herbal medicine and clinical trials find it effective against osteoarthritic pain.[xvii] The old NSAIDs work. Chemical analysis brought more knowledge

about what are working – chemical molecules whose structures are known precisely. However, for seven decades physiological and pharmacological knowledge of the old NSAIDs did not advance much beyond that of willow bark. Both remained on the empirical and phenomenological level. People knew from experience that aspirin worked, but lacked scientific knowledge about how it worked and why it worked like its cousins. New York Times Magazine aptly called it in 1966: “The wonder drug nobody understands.”[xviii]
Discovering mechanisms underlying disparate phenomena is the font of basic science. Science, especially biochemistry and molecular biology, advanced tremendously since aspirin made its debut. The castle of NSAIDs’ working principles was still intact, but siege engines were ready. The first to breach the wall in 1971, and would receive a Nobel Prize for it, was pharmacologist John Vane.[xix]
No scientific discovery is solely the work of a single person, as acknowledged in Isaac Newton’s famous aphorism: “If I have seen further, it is by standing on ye shoulders of giants.” So it was with Vane. He was brought to aspirin in 1968 by Henry Collier, a pharmacologist who had worked on it for a decade. Collier had discovered that although both morphine and aspirin kill pain, they act by different principles. Morphine acts on the brain. Aspirin acts locally at the sites of injury. What local biochemical mechanisms underlie aspirin’s actions? Collier’s research was stymied, partly because his tools and techniques were rather blunt.
Collier experimented with whole animals such as guinea pigs and rabbits. He injected an animal with a pathology-inducing chemical and then a drug, observed the animal’s responses and analyzed its blood and tissues. By varying the pathogen and the drug, he hoped to tease out what acted on what and how. After numerous experiments, no pattern emerged. An animal’s body harbors millions of chemicals and hundreds of biochemical pathways. It is so complex a medium that therapeutic mechanisms are easily obscured. Furthermore, biopsy and blood analysis, which take time to perform, may not be able to capture fleeting biochemical reactions. Frustrated, Collier turned to Vane, an expert in bioassay. The relative successes of the two scientists illustrate the importance of experimental techniques and instruments in research.
Vane’s method depends on the central tenet of biochemistry and molecular biology: What occur inside a living body are not mysterious “vital forces.” Rather, they are chemical and physical processes that obey the laws of chemistry and physics and can also occur outside the body, in tissue culture, cell culture, or even cell-free medium. Cells in a dish or molecules in a test tube are much simpler and easier to manipulate than living organisms, hence much more susceptible to analysis and understanding. This partly explains the increasing importance of biochemistry and molecular biology in biology.
Over the years, researchers have assembled a large library of how a kind of tissue reacts physically and chemically to various kinds of irritants. For instance, a tissue secrets a specific substance when it is exposed to a chemical known to cause inflammation in people, and that substance in turn causes another tissue to twitch. A bioassay test exposes a piece of partially known tissue to a novel environment and records the tissue’s reaction to figure out unknown characteristics of it or the environment. Vane had developed a powerful bioassay technique in which a sequence of tissues
probed a chain of chemical reactions. When Collier approached him, he agreed to investigate what happened when he exposed tissues to pain-inducing chemicals, and what happened if he added aspirin to the chemicals.
With bioassay experiments, Vane soon found that aspirin inhibits the production of a mysterious substance. Without aspirin, that substance would be produced by guinea pig lungs in shock and caused rabbit aorta to contract. What is it that aspirin preempted? Vane took eighteen months to identify it as a prostaglandin. Many experiments by him and his group confirmed his conjecture: aspirin inhibits the production of prostaglandins.[xx]
How aspirin works
What are prostaglandins, the production of which aspirin inhibits? They constitute a class of unsaturated fatty acids produced by cells in many parts of the body. Discovered in the 1920s, they excited much scientific excitement in the late 1960s.
Many kinds of prostaglandin exist in the body to serve a plethora of physiological functions, some of which are irritable, others beneficial. Prostaglandins are among the chemicals secreted by the body’s immune system when it fights off bacteria and other invaders in injuries. Located around wounds , these chemicals cause pain and inflammation. Following bacterial infection, prostaglandins are also produced the hypothalamus, the brain’s center for controlling body temperature, resulting in a rise in temperature. In their capacities to cause pain, inflammation, and fever, prostaglandins are nuisances. Inhibiting their production, consequently reducing pain, inflammation, and fever, is the main therapeutic value of aspirin.
On the other hand, prostaglandins secreted by the stomach regulate acid production and maintain the mucus lining that protects the stomach from digesting itself. Prostaglandins in the blood’s platelets cause the platelets to stick together to initiate blood clotting in wounds. In these capacities, prostaglandins are crucial to a healthy body. Inhibiting their production leads to aspirin’s undesirable side effects, including upset stomach and excessive bleeding.
How does aspirin curb prostaglandin production? The many kinds of prostaglandin are synthesized by a host of complicated biochemical pathways. However, all pathways share a common stage facilitated by an enzyme called COX, whose action aspirin suppresses.
Enzymes are protein catalysts that speed up chemical reactions without being themselves used up in the reactions. An enzyme is a huge molecule with an active area that works somehow like a mold that accepts certain raw pieces and casts them into a final form. Imagine a mold that stamps a rod and a bowl into a spoon. Spoon production would be disrupted if someone throws a monkey range into the mold. Such a monkey range – an enzyme inhibitor – would make a desirable drug if it stops an enzyme from producing disease-inducing chemicals. Aspirin is an enzyme inhibitor. It suppresses the action of the enzyme COX, stops the production of prostaglandin, thus disrupting the pathways to pain, inflammation, elevated temperature, and stomach protection.
Vane’s success attracted many researchers to the area. Their investigations spread from aspirin to similar drugs that suppress pain and inflammation. By 1974, it was fairly well established that all NSAIDs act with similar mechanisms. They are all COX inhibitors.
Aspirin, ibuprofen, naproxen, and many other non-steroidal anti-inflammatory drugs (NSAIDs) work as COX inhibitors. They suppress the catalytic functions of the enzymes COX1 and COX2. COX2, which appears up injuries and other inflammatory stimuli, is deemed “bad”. It catalyzes the synthesis of prostaglandins that, located near sites of injuries, cause pain and inflammation. Inhibition of COX2 is responsible for the therapeutic effects of reducing pain, inflammation, and fever. COX1, which is present in many parts of the body, is deemed “good.” It catalyzes the synthesis of prostaglandins that perform many physiological functions, e.g., maintaining the mucus lining of the stomach or causing platelets in the blood to stick and form clots over wounds. Inhibition of COX1 is responsible for the drugs’ side effect of stomach irritation. In reducing the risk of blood clots, it is also responsible for aspirin’s efficacy in heart attack prevention. A new class of NSAID, COX2 inhibitor, is designed to target bad COX2 selectively and leave good COX1 alone, thus reducing pain and inflammation without upsetting the stomach.
From empiricism to concept-directed research
Connecting the dots has become a familiar phrase in the aftermath of September 11, 2001, when the intelligence community was blamed for failing to connect the dots and read from available information the message that terrorists were preparing to attack America. Dots can be connected arbitrarily to suit any agenda, but that is not what people want. They demand connections that reveal significant objective patterns.
Empirical observations yield dots of data. To connect them objectively depends on appropriate concepts and theories. The concept of COX-inhibition connects aspirin’s medicinal effects to prostaglandin and COX action. Due to the conceptual connection, these hitherto disparate pieces of

knowledge become nexus in a network of relations. Furthermore, the network reveals other nexus and patterns that no one had dreamed of before. Therein lies the power of scientific theories to predict new phenomena, raise new questions, and indicate new areas for inquiry. That is why scientists highly value concepts and theories that correctly extract a set of relevant data and reveal their connections.
With the concept of COX-inhibition, knowledge about aspirin changes from mere empiricism to theory guided research. Whereas an empirical fact is specific to a particular phenomenon, a concept is general and potentially applicable to other phenomena. COX enzyme is present in many parts of the body, including unexpected places such as colon tumors. The conceptual framework of COX inhibition suggests links between aspirin and phenomena hitherto deemed unrelated, thus enabling scientists to ask significant questions and direct their research efforts. Basic scientists can use NSAIDs as tools to probe the physiological effects of COX, for instance in the formation of cancer.[xxi] Pharmaceutical firms can use COX enzyme in test tubes to screen for promising drugs. A conceptual framework that explains phenomena by their underlying mechanisms is not a last word but a scientific breakthrough. A final word closes the door on exploration, a breakthrough opens up a frontier of research.
Biochemistry meets molecular biology
The COX inhibition concept brought out many interesting questions.[xxii] The NSAIDs are similar but not identical. They exhibit considerable variations in their effects. For instance, ibuprofen is easer on the stomach than aspirin. How can the variations be explained in terms of COX inhibition? This calls on basic science to uncover the detailed mechanisms by which the drugs interact with COX enzyme.
Detailed mechanisms depend on the internal structure of COX, which biochemists did not know. They investigated external properties of COX and discovered that it behaves differently in different situations. Some COX enzymes, for instance those in the stomach, are present all the time. Others, for instance those responsible for pain-inducing prostaglandins, appear only at the heel of physiological injuries. This and other experimental results prompted biochemists to speculate that COX existed in two similar but distinct forms.
Further scientific research proceeded slowly. Even if two forms of COX existed, their catalytic actions were so similar it was difficult to tease them apart by biochemical means. The secret lies in the internal structure of COX, but this is a hard nut to crack. Unlike most drugs, which are rather simple molecules with tens or hundreds of atoms, COX and other enzymes are huge molecules with thousands of atoms and monstrous complexity.
So far, aspirin research mainly marched from the top down, from organisms to tissues to enzymes. Now biochemistry rendezvoused with a branch of science marching from the bottom up, from atoms to
enzymes. When two sciences meet, their concepts mesh and many more dots are connected to yield improved intelligence. Using X-ray crystallography and other technologies, molecular biologists were unraveling the molecular structures of genes and the enzymes encoded by the genes. They discovered in 1991 a novel gene that coded for an enzyme highly similar, but not identical, to the COX that was isolated from smooth muscles and widely studied. Soon molecular biologists established that COX enzyme has two forms, called COX1 and COX2. The two are coded by different genes and serve different physiological functions.[xxiii]
Briefly, molecules of COX1 are widely distributed in the body’s cells, from the stomach to the platelets of the blood. Continuously present in the body, they serve “housekeeping” functions that maintain various normal physiological conditions. For its maintenance of healthy physiology, COX1 is duped “good.” Molecules of COX2 are not present all the time. Their production is induced by inflammatory and other injurious stimuli, and they tend to localize in the sites of injury, for instance the swelled joints of people suffering from rheumatoid arthritis. For its culpability in pain and inflammation, COX2 is duped “bad.”
Old COX inhibitors – NSAIDs such as aspirin and ibuprofen – inhibit the actions of both COX1 and COX2. Suppressing the bad COX2 accounts for the drugs’ therapeutic effects. Suppressing the good COX1 leads to their undesirable side effects. Different drugs have different selectivity for the two COXs, which partly explains their varying medicinal profiles. Unfortunately, they all tend to be harsher on the good COX1. The worse is aspirin itself. It is 150 times more effective in inhibiting COX1 than COX2, and is harsher on the stomach than its cousins.
Success and setback of rational drug design.
The physiology of COX enzymes is complex. However, once the big picture of the COX1/COX2 concept is established, it does not take much for pharmacologists to recognize the appeal to design a drug that selectively inhibits the bad COX2 while sparing the good COX1.
Rational drug design is a very different approach than the trial and error that led to the first use of aspirin. To design drugs that target a specific enzyme or biochemical mechanism is increasingly feasible since the 1980s, when scientific knowledge about relevant mechanisms began to accumulate. Molecular biologists had deciphered the molecular sequences of the COX enzymes and how they fold into complex three-dimensional structures. Armed with this knowledge, pharmacologists set about finding small drug molecules that interfere with only COX2 and not COX1.[xxiv]
First generation COX2 inhibitors, Celebrex and Vioxx, reached consumers in 1999. Nicknamed “super aspirins,” they are comparable to aspirin in reducing pain and inflammation. Large scale clinical trials also found that they cause significantly less gastrointestinal irritation than the old COX inhibitors. Gastrointestinal side effects of COX inhibitors were blamed for roughly 100,000 hospitalizations and 15,000 deaths each year in the United States alone. Rheumatoid arthritic patients who had to take high dosages for long periods suffered most. To them COX2 inhibitors that promise to lessen the toll were godsend.[xxv]

Both Celebrex and Vioxx made the 2001 list of top ten drugs by global sales, beating the famous impotence drug Viagra, introduced in 1998. Clinical superiority is not the only reason for the high dollar sales of COX2 inhibitors. Another reason is that super aspirins are much more expensive than aspirin. Social critics grumble that the new drugs are not worth their high prices, but people whose drug bills are covered by health insurance do not care.[xxvi] They demand the best, whether or not aspirin upsets their stomachs; they pay the same insurance premium anyway. COX2 inhibitors grossed $5.7 billions and accounted for 23 percent of the pain and inflammation drug market in 2001. That was smaller than the 30 percent for the old COX inhibitors, but the trend of replacement was unmistakable. Optimistic analysts projected that by 2010, the market share of COX2 inhibitors would more than double that of COX inhibitors.[xxvii]
Optimism turned sour when the rising star of COX2 inhibitors took a major hit. Drugs on market are already approved by the Food and Drug Administration and not required to undergo further safety tests. Nevertheless, people are free to test them, perhaps in search for possible additional applications. Following indications that COX2 inhibitors may be effective in reducing the risks of colon cancer and Alzheimer’s disease, drug makers and independent research institutes conduct long-term clinical trials on them. In late 2004, a major trial found that almost twice the subjects who took Vioxx for eighteen months had strokes or heart attacks than subjects who took sugar pills. The trial was terminated midway. Vioxx was immediately withdrawn from the market. The entire class of COX2 inhibitors was in trouble. Nor were the old COX inhibitors spared. Other trials cast clouds over Celebrex and naproxen (Aleve, Naprosyn). The FDA came under intense fire for failure to monitoring long-term safety.[xxviii]
The saga of COX inhibitors continues. Already the second generation of COX2 inhibitors is in the development pipeline. As long as people need pain killers without side effects, research continues.
Aspirin and the heart – scientific results are inconclusive
The fall of COX2 inhibitors reveals the complexity of physiology. Their fault for raising risks for heart attacks does not come as a bolt from the blue. Years before they hit the market, Vane predicted that COX2 inhibitors would replace COX inhibitors in most areas except one: prevention of heart attacks.
COX1, which super aspirins spare but aspirin inhibits, is good but not absolutely good – nothing is absolute in a complex world. COX1 is indispensable in many healthy functions. Among them is blood clotting. If blood fails to clot and close a wound, one can bleed to death from a small cut, a danger well know to people suffering from hemophilia. Therefore the action of COX1 in blood clotting is crucial for most ordinary situations. However, in some rare cases, unwanted blood clot in the wrong places can also lead to heart attacks. In those heart-related circumstances, the action of aspirin as COX1 inhibitor would be beneficial.
Aspirin began its affair with the heart even before it got its name. A major reason that Bayer initially hesitated to market it was its perceived “enfeebling action on the heart.” That misperception persisted for decades, so much so that some aspirin advertisements carried the claim: “Does not affect the heart.”

Judging the claim unsubstantiated, the U.S. government banned it in the 1930s. Fifty years later, government regulators faced the opposite claim: Aspirin does affect the heart – in a good way.[xxix]
Heart attack, the biggest killer in America, involves many factors. One is the narrowing of arteries by plaque such as cholesterol. Another is the formation of blood clots in arteries. If a blood clot blocks a narrowed artery, it can stop blood flow to the heart, resulting in damages of heart tissues, commonly called a heart attack. Or it can stop blood flow to the brain, resulting in a stroke. In the 1960s, some physicians hoped to reduce the risk of artery blood clots by blood thinning drugs. The hope collapsed; these drugs did seemed to reduce heart attacks, but they also increased fatal bleeding in the brain – a devil’s trade.[xxx]
Blood clotting is a complex process. The blood contains, besides red and white blood cells, partial cells called platelets. The disc-like platelets are produced in the bone marrow and cannot reproduce themselves because they contain no nucleus. They usually lie dormant in the blood, awakened only by chemicals released by injured tissues or a tear in the artery’s plaque. These stimulants activate the COX1 enzyme in the platelets to produce a prostaglandin, which causes the platelets to stick together, triggering the cascade of reactions that result in clotting of blood. By inhibiting COX1 from synthesizing the prostaglandin, aspirin reduces the stickiness of platelets, hence the chance of forming blood clots. For this antiplatelet purpose aspirin is uniquely effective. All other aspirin-like drugs inhibit COX temporarily, aspirin alone inhibits it permanently. One dose of aspirin has antiplatelet effects that last through the platelet’s lifetime, about ten days.
Aspirin’s antiplatelet effect was observed in 1967. Harvey Weiss and Louis Aledort divided their experimental subjects into two groups, gave aspirin to one but not the other. They then measured how long the subjects bleed from pinpricks and correlated it to the degree of platelet aggregation in blood taken from the subjects. Data revealed that those who had taken aspirin bleed longer and the platelets in their blood aggregated less. Weiss and Aledort suggested that aspirin may prevent artery blood clots.[xxxi] They did not know how aspirin prevented platelet aggregation, but that was explained four years later when Vane discovered aspirin’s COX inhibition effect.
Basic science and knowledge about underlying mechanisms strengthen the case for “an aspirin a day keeps heart attacks away.” However, they are not sufficient to prove it. We saw earlier that tissue bioassay is better than whole animal experiments in isolating a process and uncovering its underlying mechanism, which is buried under myriad processes going on in a life animal. The advantage in discovery can become a disadvantage in applying its results. In isolating a process we ignore its interaction with other processes in the context of application. These interactions can generate side effects or even derail the process itself. In the test tube, aspirin inhibits COX1 in platelets and hence the formation of a prostaglandin that promotes blood clots; fine. In the body, the situation is far more complex. For instance, aspirin also inhibits COX2 in blood vessels and hence the formation of another prostaglandin that prevents blood clots.[xxxii] How would the two processes of opposing effects balance out? Another question, would taking aspirin years on end, even at low dosages, increase the risk of bleeding in the brain? These and many other questions involving the functioning of the body as a
whole cannot be answered by test-tube experiments on individual processes. That is why governments require drugs to pass clinical trials in human subjects to prove their effectiveness and safety.
Encouraged by the experimental results of Weiss and Aledort, epidemiologist Peter Elwood initiated the first clinical trial of aspirin’s efficacy in preventing second heart attacks in 1971. It ended thirty months later with the all-too familiar remark: “The results of this trial were inconclusive.”[xxxiii]
Elwood persisted with further trials, so did other academicians and pharmaceutical companies. A three-year and $17 million experiment funded by the U.S. government returned in 1980 the disheartening result that aspirin had no effect on the heart. However, other trials returned mildly favorable results. Scientific debates ensued. Trial protocols were criticized, new experiments designed and launched, data analyzed and reanalyzed and aggregated with sophisticated mathematics. Finally in 1985, the U.S. Food and Drug Administration approved the claim that long-term low-dosage aspirin reduces the risk for recurrence of heart attack.[xxxiv]
Trials on people with other health conditions continue. Aspirin taken by patients while having a heart attack significantly reduces the chance of death. For people with various risk factors for heart diseases such as diabetes, obesity, or high blood pressure, aspirin lowers the probability of a first heart attack. For healthy people without cardiovascular risks, results on the effects of aspirin are inconclusive.[xxxv]
Chances are aspirin will make news again. Its continuing story celebrates the persistent advancement of science.