16. antivirus & antifungi (dr. evi sovia)
TRANSCRIPT

Antifungal DrugsEvi Sovia
Pharmacology Departement
Sasaran belajar Mengetahui klasifikasi obat-obat antijamur Mengatahui farmakokinetik dan
farmakodinamik obat-obat antijamur Mengetahui efek samping obat-obat
antijamur Mengetahui interaksi obat-obat antijamur
Antifungal drugs Drugs for Cutaneus Mycoses Drugs For Subcutaneus And Sistemic
Mycoses
Drugs for Cutaneus Mycoses
Butoconazole Clotrimazole Econazole Griseofulvin Miconazole Nystatin Terbinafine Terconazole
Tebinafine D.o.c for dermatophytoses, especially
onychomyccoses (fungal infections of nails) Better tolerated Requires shorter d.o.a of therapy More effective than either itaconazole or
groseofulvin
MOA inhibits fungal squalene epoxidase, thereby
decreasing the synthesis of ergosterol. This plus the accumulation of toxic amounts
of squalene result in the death of the fungal cell
Antifungal spectrum: fungicidal Antifungal activity is limited to
dermatophytes and Candida albicans. Therapy is prolonged usually about 3
months but consederably shorter than that with griseofulvin
Pharmacokinetics orally active bioavailability 40% due to first pass metabolism Absorption is not significantly enhanced by
food Greater than 99% bound to plasma protein
Deposited in the nails, skin and fat Accumulates in breast milk, should not be
given to nursing mothers T1/2 200-400 hours Extensively metabolized Excretion: urinary
Adverse effects Gastrointestinal disturbance (diarrhea,
dyspepsia, and nausea) Headache Rash Taste and visual disturbance Transient elevated in serum liver enzyme
levels Resolve upon drug discontinuation
Drugs interaction Rifampin decreased blood levels of
terbinafine Cimetidine increased blood levels of
terbinafine
Griseofulvin Has been largely replaced by terbinafine for
the treatment of dermatophytic infection of the nails.
Duration of treatment: 6-12 months
MOA Accumulates in newly synthesized, keratin-
containing tissue, causes disruption of the mitotis spindle and inhibition of fungal mitosis
Duration of therapy is dependent on the rate of replacement of healthy skin or nails.
Ultrafine crystalline preparations are absorbed adequately from the GI tract
Absorption is enhanced by high fat meals Induces hepatic cytochrome P450 activity Increases the rate metabolism of number of
drugs, including anticoagulants
Exacerbate intermittent porphyria Patients should not drink alcoholic
beverages during therapy because potentiates the intoxicating effect of alcohol
Nystatin Polyene antibiotic Structure, MOA, resistance resemble those
to amphotericin B Usage is restricted to topical treatment of
candida infections because of its systemic toxicity
Negligibly absorbed from the GI tract, and its never used parenterally
Administered as an oral agent (swish and swallow) for the treatment of oral candidiasis
Excretion in the feses Adverse efect is rare because of the lack
absorption, but nausea and vomitting occasionally occur
Miconazole and other topical agent Miconazole, clotrimazole, butoconazole and
terconazole Topically active drugs Rarely administered parenteral because of
their severe toxicity MOA = ketoconazole Topical use is associated with contact
dermatitis, vulvar irritation, and edema
Potent inhibitor of warfarin metabolism, resulted in bleeding in warfarin-treated patients even when miconazole is applied topically
No significant difference in clinical outcomes is associated with any azole or nystatin in the treatment of vulvar candidiasis
Drugs For Subcutaneus And Sistemic Mycoses
Amphotericin B Caspofungin Fluconazole Flucytosine Itraconazole Ketoconazole Voriconazole
Amphotericin B MOA
Bind to ergosterol in the plasma membranes of sensitive fungal cells → they form pores → disrupt membrane function → electrolytes and small molecules leak from the cell → cell death
Antifungal spectrum Fungicidal and fungistatic depending on the
organism and the concentration of the drug. Effective against C. albicans, H.
capsulatum, C. neoformans, C. immitis, B. dermatitidis, and many strains of aspergillus
Resistance Infrequent Associated with decreased ergosterol
content of the fungal membrane
Pharmacokinetics ROA: iv infusion Insoluble in water → sodium deoxycholate Extensively bound to plasma proteins Distributed throughout the body Excretion: urine
Adverse effects Low therapeutic index Total daily dose should not exceed 1.5 mg/kg
Fever and chills Renal impairment Hypotension Anemia Neurologic effects thrombophlebitis
Flucytosine (5-FC) MOA: 5-FC → 5-FdUMP → inhibits
thymidylate synthase → depriving essential DNA component
Antifungal spectrrum Effective in combination with itraconazole
→ chromoblastomycosis With amphotericin B → candidiasis or
cryptococcosis
Resistance Decreased levels of any of the enzymes in
the conversion of 5-FC to 5-FU
Pharmacokinetics Well absorbed by the oral route Distributed throughout the body Excretion: urine The dose must be adjusted in patients with
compromised renal function
Adverse effects Neutropenia Thrombocytopenia Occasional bone marrow depresion Reversible hepatic dysfunction GI disturbances : nausea, vomitting, and
diarrhea, enterocolitis
Ketoconazole MOA: inhibits C-14 -demethylase (cyt P-
450 enzyme) → blocking the demethylation of lanosterol to ergosterol (the principal sterol of fungal membranes)
Antifungal spectrum Active against histoplasma, blastomyces,
candida, and coccidioides but not aspergillus sp
Itraconazole: broader spectrum, greater potency and fewer adverse effects
Resistance Mutation in tne C-14 -demethylase gene
→ decreased azole binding
Pharmacokinetics Only administered orally Requires gastric acid for dissolution and is
absorbed through the gastric mucosa antacids, AH2, PPI → impair absorption Administering acidifying agent → improve
absorption Extensively bound to plasma proteins Does not enter the CSF Metabolism : liver Excretion : primarily through the bile
Adverse effects Allergies GI disturbances: nausea, anorexia,
vomiting Gynecomastia, decreased libido, impotence
and menstrual irregularities Increased of serum transminase
Drugs interactions and contraindication
Inhibiting cyt P450 → potentiate the toxicities of drugs such as cyclosporine, phenitoin, tolbutamide, and warfarin
Rifampin → shorter the DOA of ketoconazole
Teratogenic CI: pregnancy
Fluconazole Lack of the endocrine side effect Excellent penetrability into the CSF DOC for C. neoformans, candidemia and
coccidioidomycosis Administered orally or iv Absorption is excellent, not dependent on
gastric acidity
Binding to plasma proteins is minimal Poorly metabolized Excreted via the kidney
Itraconazole Broad antifungal spectrum Lack of endocrine side effects Effective in AIDS associated histoplasmosis Well absorbed orally, requires acid for
dissolution Extensively bound to plasma proteins Distributed well throughout most tissue
Extensively metabolized by the liver but does not inhibit androgen synthesis
CI: pregnancy Inhibits the metabolism of many drugs
(anticoagulans, statins, quinidine)
Caspofungin Echinocandins class of antifungal drugs Interfere with the synthesis of (1,3)-D-
glucan → lysis and cell death Spectrum: limited to aspergillus and
candida sp Not active by the oral route Highly bound to serum proteins
T1/2 : 9-11 hr Slowly metabolized by hydrolysis and N-
acetylation Elimination: urine and fecal route Adverse effects: fever, rash, nausea, and phlebitis Second line antifungal for those who have failed
or cannot tolerate amphotericin B or itraconazole Very expensive
ANTI VIRUS

Inhibitors of viral DNA and RNA synthesis
1. Asiklovir (analog guanosin sintesis) Antiherpesvirus Obat lain: famsiklovir, valasiklovir Harus mengalami fosforilasi (monofosfat →
trifosfat) oleh thymidine kinase untuk menjadi aktif
Thymidine kinase pada virus herpes simplek 1 dan 2 lebih sensitif terhadap asiklovir daripada thymidine kinase sel inang → asiklovir terakumulasi di dalam sel yang terinfeksi
Perubahan pada thymidine kinase → resistensi → Foscarnet
M.K: menghambat DNA polimerase
Farmakokinetik Asiklovir dapat diberikan secara topikal,
oral dan IV Valasiklovir dan famsiklovir: hanya oral Bioavailabilitas asiklovir 15-30%,
valasiklovir 2x lipat Makanan tidak mempengaruhi absorpsi Ikatan dengan protein 10-30% Distribusi baik
Absorpsi perkutan rendah dan hanya terjadi pada lesi luas
Valasiklovir dimetabolisme menjadi asiklovir di hepar
Valasiklovir diabsorpsi lebih baik → konsentrasi serum lebih tinggi (3-5x dari asiklovir)
Famsiklovir dimetabolisme menjadi pensiklovir (metabolit aktif)
Waktu paruh asiklovir 3,3-3,8 jam Dieksresi di urin
2. Gansiklovir ≈ asiklovir, tetapi toksik Diberikan secara oral atau IV Waktu paruh 3-4 jam >90% dieksresi dalam urin → penyesuaian
dosis pd gangguan fungsi ginjal
3. Foscarnet MK: menghambat DNA polimerase, RNA
polimerase, dan reverse transkriptase Efektif untuk herpesvirus, virus influenza,
dan HIV Bioavabilitas 20% Hanya diberikan secara IV Berikatan dengan kalsium → dideposit
dalam tulang 80-90% dieksresi di ginjal
4. Ribavirin (analog purin sintesis) Fosforilasi oleh adenosin kinase sel inang Bioavailabilitas 45% Konsentrasi plasma setelah pemberian IV
10x lebih besar daripada oral Diberikan secara inhalasi pada pengobatan
infeksi virus berat Eliminasi terutama di hati, 30% di urin
Interferon Merupakan glikoprotein alami yang dihasilkan oleh
limfosit, makrofag, fibroblast, dan sel lain Interferon ,, dan MK: menghambat sintesis protein virus, menghambat
penyusunan, dan menstimulasi respon imun Dapat melindungi sel yang tidak terinfeksi Digunakan untuk mengobati hepatitis dan papilloma Karena merupakan glikoprotein, farmakokinetiknya
sukar dinilai Diberikan secara IM atau SC Efektif bila disuntikan langsung ke kondiloma Distribusi ke seluruh tubuh Eliminasi kompleks, melalui hati, ginjal, jantung, paru-
paru, dan otot skelet dapat menginaktivasi senyawa ini
ImunoglobulinDigunakan sebagai antiviral,
terutama untuk pencegahan infeksi
Hepatitis B dan rabiesDiberikan secara SC, IM dan IVDistribusi ke seluruh tubuhWaktu paruh 20-30 hari
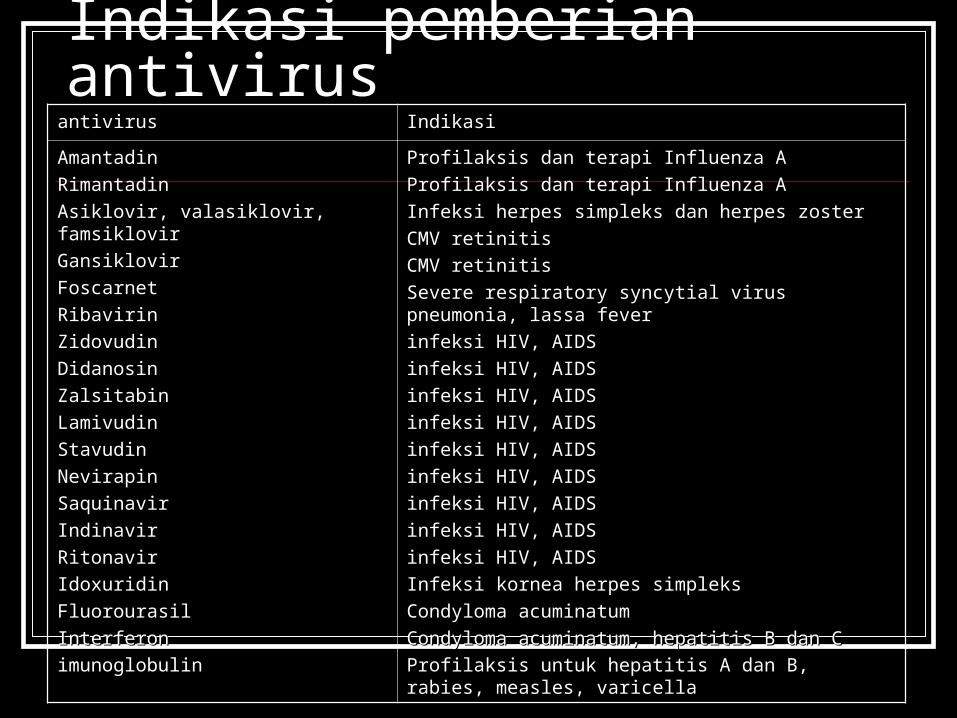
Indikasi pemberian antivirusantivirusantivirus Indikasi Indikasi
AmantadinAmantadin
RimantadinRimantadin
Asiklovir, valasiklovir, famsiklovirAsiklovir, valasiklovir, famsiklovir
GansiklovirGansiklovir
FoscarnetFoscarnet
RibavirinRibavirin
ZidovudinZidovudin
DidanosinDidanosin
ZalsitabinZalsitabin
LamivudinLamivudin
StavudinStavudin
NevirapinNevirapin
SaquinavirSaquinavir
IndinavirIndinavir
RitonavirRitonavir
IdoxuridinIdoxuridin
FluorourasilFluorourasil
InterferonInterferon
imunoglobulinimunoglobulin
Profilaksis dan terapi Influenza AProfilaksis dan terapi Influenza A
Profilaksis dan terapi Influenza AProfilaksis dan terapi Influenza A
Infeksi herpes simpleks dan herpes zosterInfeksi herpes simpleks dan herpes zoster
CMV retinitisCMV retinitis
CMV retinitisCMV retinitis
Severe respiratory syncytial virus pneumonia, lassa Severe respiratory syncytial virus pneumonia, lassa feverfever
infeksi HIV, AIDSinfeksi HIV, AIDS
infeksi HIV, AIDSinfeksi HIV, AIDS
infeksi HIV, AIDSinfeksi HIV, AIDS
infeksi HIV, AIDSinfeksi HIV, AIDS
infeksi HIV, AIDSinfeksi HIV, AIDS
infeksi HIV, AIDSinfeksi HIV, AIDS
infeksi HIV, AIDSinfeksi HIV, AIDS
infeksi HIV, AIDSinfeksi HIV, AIDS
infeksi HIV, AIDSinfeksi HIV, AIDS
Infeksi kornea herpes simpleksInfeksi kornea herpes simpleks
Condyloma acuminatumCondyloma acuminatum
Condyloma acuminatum, hepatitis B dan CCondyloma acuminatum, hepatitis B dan C
Profilaksis untuk hepatitis A dan B, rabies, Profilaksis untuk hepatitis A dan B, rabies, measles, varicellameasles, varicella
terimakasih