atrial fibrillation epidemiology, pathogenesis, diagnosis and treatment
TRANSCRIPT
Atrial fibrillation
Epidemiology, pathogenesis, diagnosis and treatment
Dr. dr. Hendro Darmawan, MSc, SpJP
RS BMC, 31 October 2012

DR. Dr. H. Hendro Darmawan, MSc, SpJP, FIHA
Pekerjaan :
Direktur Utama RS Bogor Medical Center
Pendidikan :
* Dokter Umum FKUI Jakarta 1980
* Dokter Spesialis Jantung dan Pembuluh Darah FKUI Jakarta 1989
* MSc in Epidemiology, University of Illinois Urbana Champaign, USA 1991
* Doktor Epidemiologi Klinis FKM UI 2007
Organisasi :
* Anggota IDI
* Anggota PERKI
* Anggota American Heart Association, Council of Epidemiology
* Ketua PERSI Cabang Bogor
Disorganised electrical and mechanical
activity that originates in the atria with an
irregular ventricular response
AF is an arrhythmia characterized by
uncoordinated atrial activation, with
consequent deterioration of atrial mechanical
function
Condition in which the normal contractions of
the atria are replaced by a rapid irregular
twitching
Atrial fibrillation
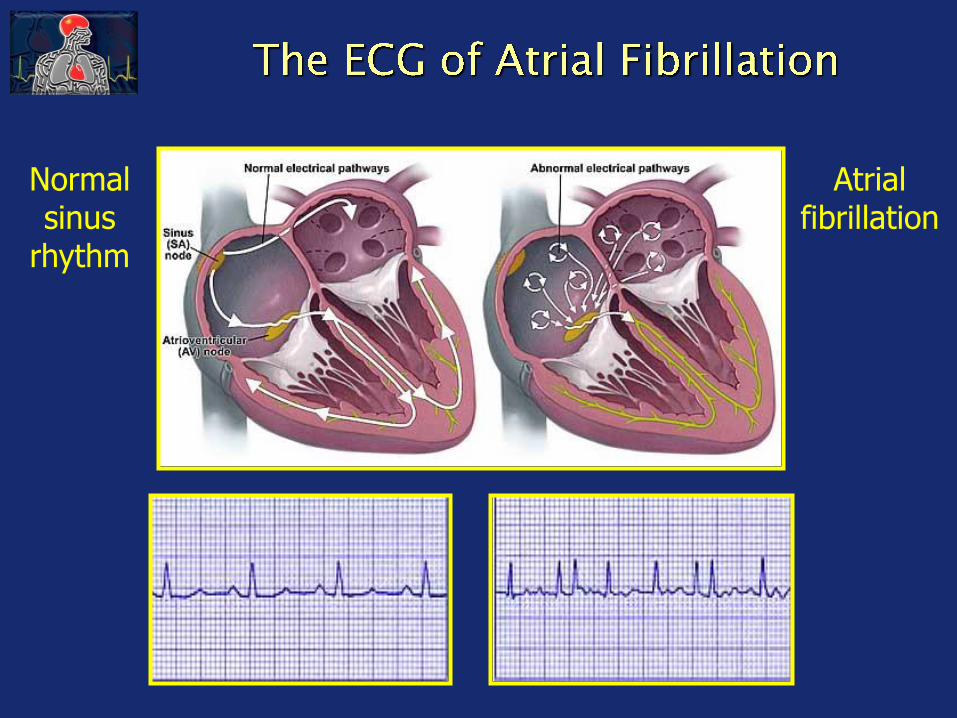
Normal sinus
rhythm
Atrial fibrillation
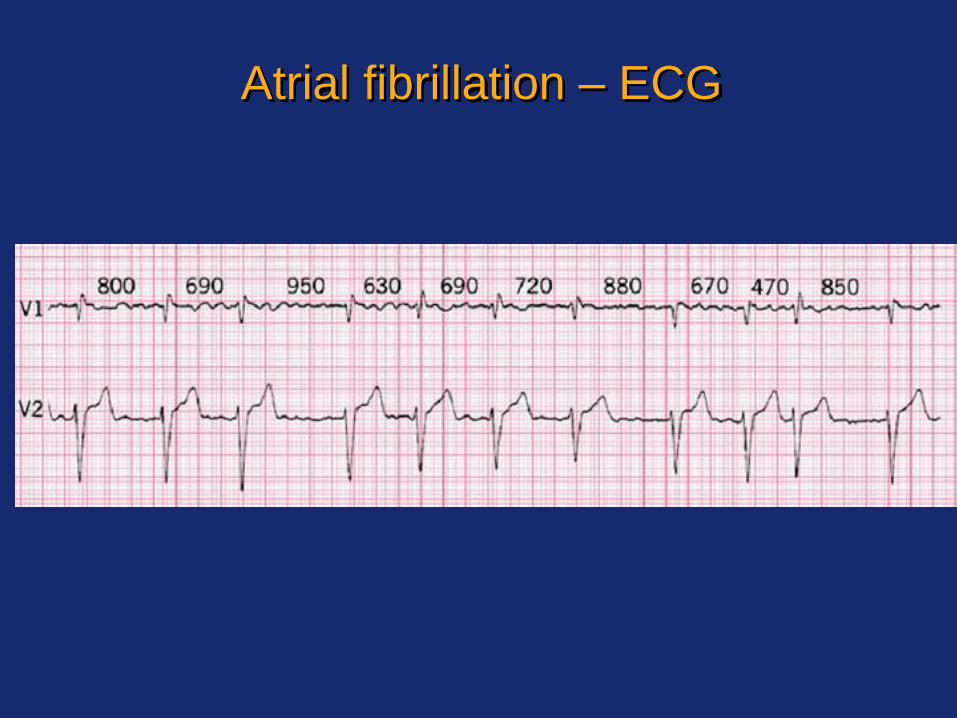
Atrial fibrillation – ECG

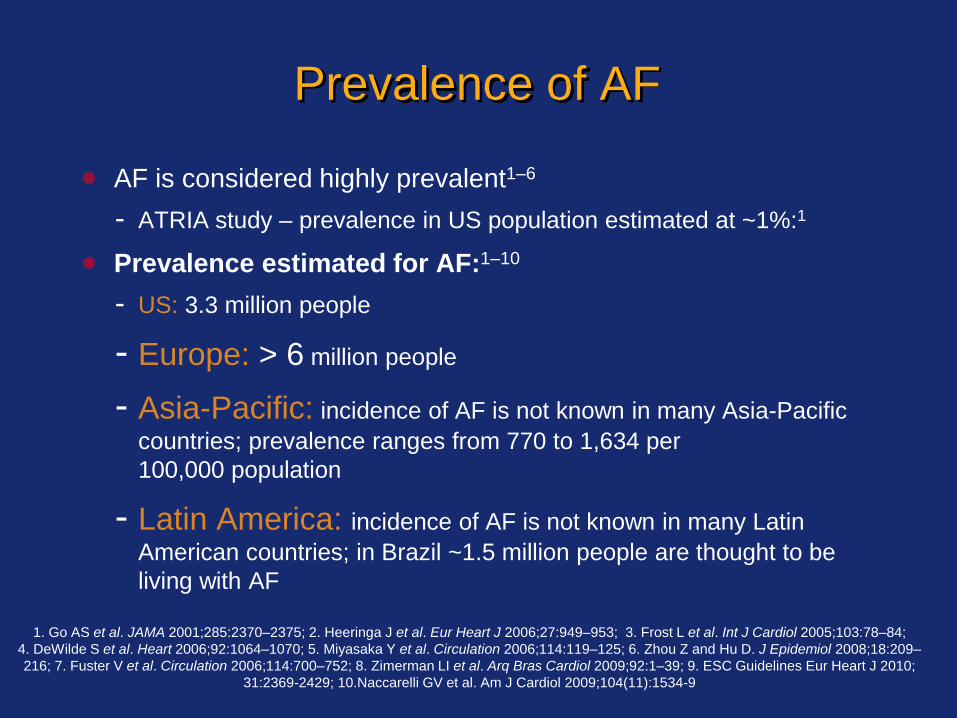
Prevalence of AF
AF is considered highly prevalent1–6
- ATRIA study – prevalence in US population estimated at ~1%:1
Prevalence estimated for AF:1–10
- US: 3.3 million people
- Europe: > 6 million people
- Asia-Pacific: incidence of AF is not known in many Asia-Pacific
countries; prevalence ranges from 770 to 1,634 per
100,000 population
- Latin America: incidence of AF is not known in many Latin
American countries; in Brazil ~1.5 million people are thought to be
living with AF
1. Go AS et al. JAMA 2001;285:2370–2375; 2. Heeringa J et al. Eur Heart J 2006;27:949–953; 3. Frost L et al. Int J Cardiol 2005;103:78–84;
4. DeWilde S et al. Heart 2006;92:1064–1070; 5. Miyasaka Y et al. Circulation 2006;114:119–125; 6. Zhou Z and Hu D. J Epidemiol 2008;18:209–
216; 7. Fuster V et al. Circulation 2006;114:700–752; 8. Zimerman LI et al. Arq Bras Cardiol 2009;92:1–39; 9. ESC Guidelines Eur Heart J 2010;
31:2369-2429; 10.Naccarelli GV et al. Am J Cardiol 2009;104(11):1534-9
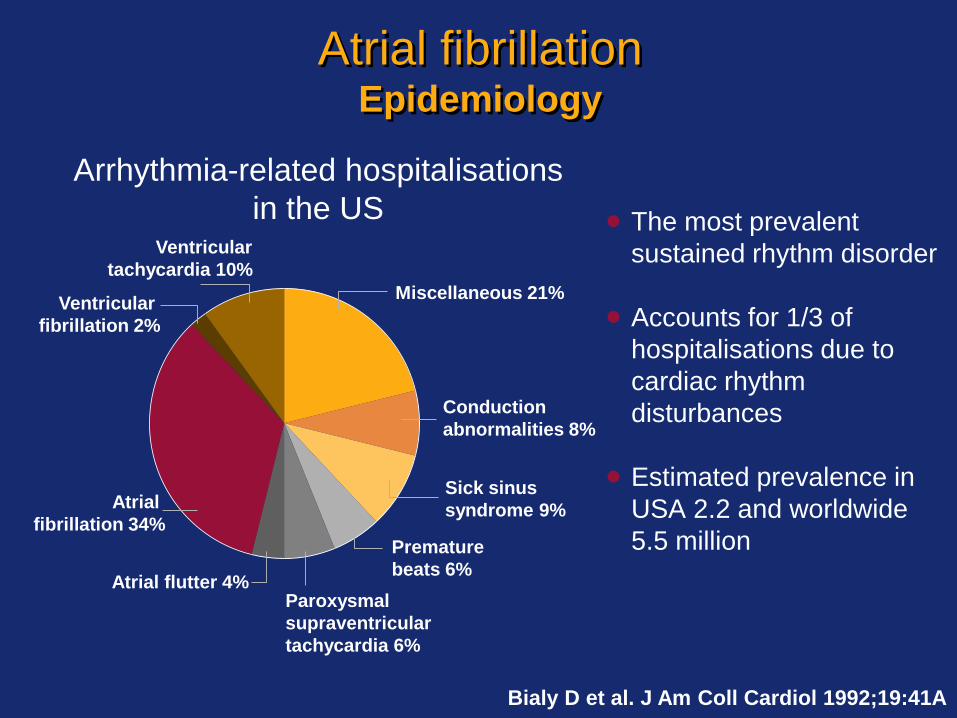
Atrial fibrillationEpidemiology
The most prevalent
sustained rhythm disorder
Accounts for 1/3 of
hospitalisations due to
cardiac rhythm
disturbances
Estimated prevalence in
USA 2.2 and worldwide
5.5 million
Arrhythmia-related hospitalisations
in the US
Atrial flutter 4%Paroxysmal
supraventricular
tachycardia 6%
Atrial
fibrillation 34%
Ventricular
fibrillation 2%
Ventricular
tachycardia 10%
Miscellaneous 21%
Conduction
abnormalities 8%
Sick sinus
syndrome 9%
Premature
beats 6%
Bialy D et al. J Am Coll Cardiol 1992;19:41A

Age (years)
Prevalence%
Prevalence of atrial fibrillation increases
with age
0.5
1.8
4.8
8.8
0
2
4
6
8
10
50-59 60-69 70-79 80-89
Wolf PA et al. Stroke 1991;22:983-8
Framingham Study

Atrial fibrillation increases mortality
50
40
30
20
10
0
0 1 2 3 4 5 6 7
Subjects dead in follow-up
(%)
Years of follow-up
Men AF
Women AF
Men no AF
Women no AF
0
0.4
0.8
1.2
1.6
2.0
Adjusted odds ratio
Men Women
95% Cl 1.2–1.8 1.5–2.2
Odds ratio for death
Benjamin EJ et al. Circulation 1998;98:946–52
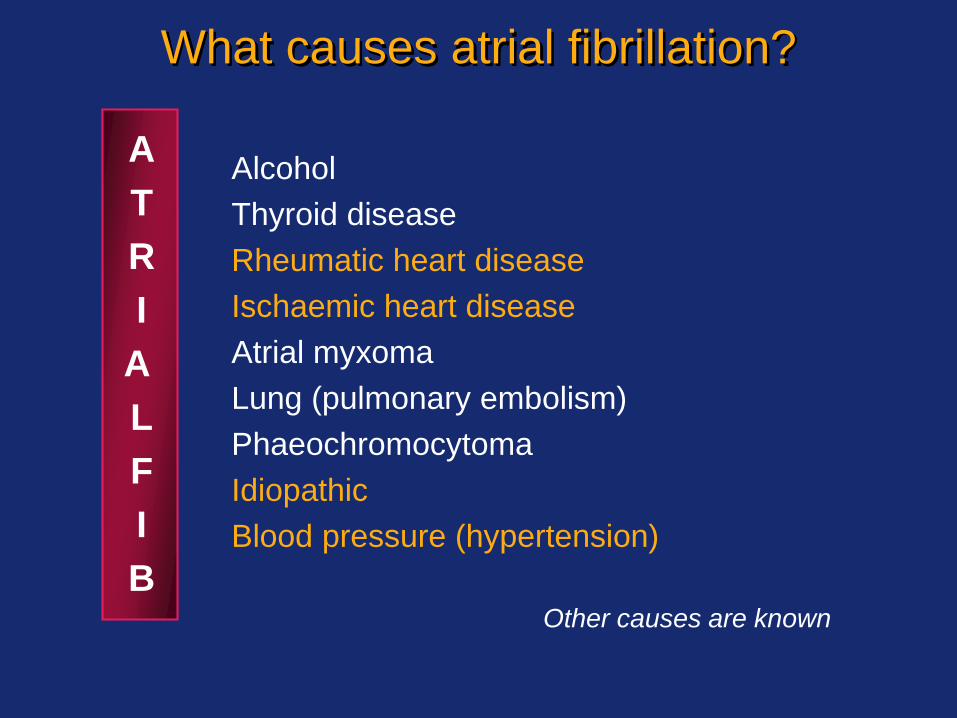
A
T
R
I
A
L
F
I
B
Alcohol
Thyroid disease
Rheumatic heart disease
Ischaemic heart disease
Atrial myxoma
Lung (pulmonary embolism)
Phaeochromocytoma
Idiopathic
Blood pressure (hypertension)
Other causes are known
What causes atrial fibrillation?
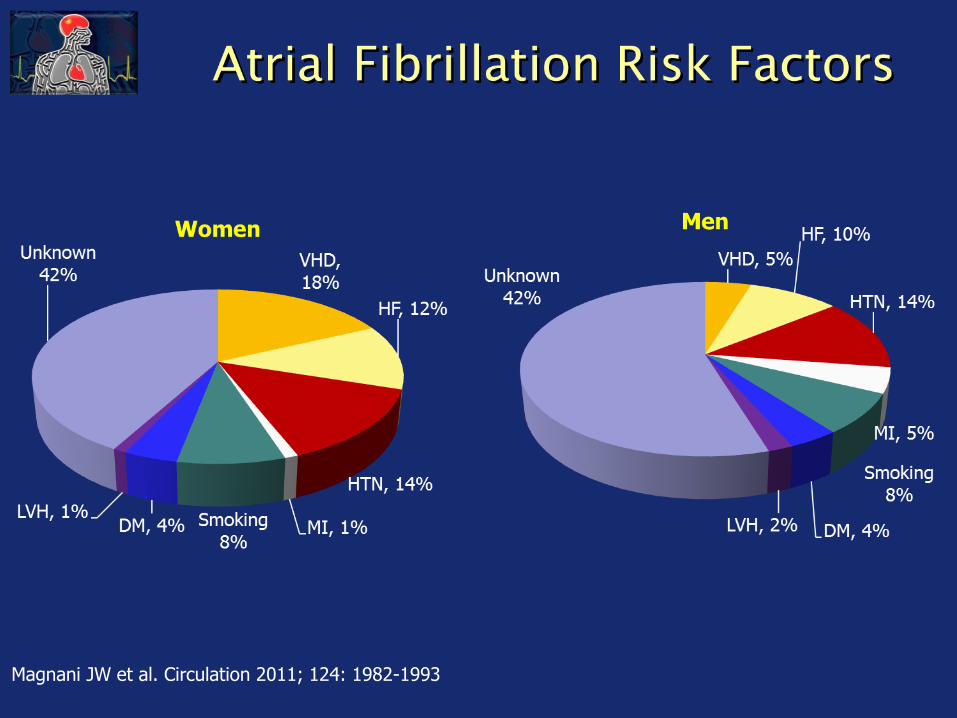
Magnani JW et al. Circulation 2011; 124: 1982-1993

Increased potential
for atrial fibrillation
Increased atrial
pressures
Hypertension
High left
ventricular pressures
Hypertension increases the risk of developing
atrial fibrillation almost two-fold
Slowing of atrialconduction velocity
Impaired ventricular filling
Left atrial enlargement
Left ventricular hypertrophy

Patients with AF have an approximately
fivefold increased risk of ischaemic stroke 2
-year
ag
e-a
dju
ste
d
incid
en
ce o
f str
oke/1
,000
Individuals
with AF*
Individuals
without AF
Risk ratio=4.8
p<0.001
0
10
20
30
40
50
60
Framingham Heart Study (N=5,070)
Wolf PA et al. Stroke 1991;22:983–988
*Patients were untreated with antithrombotic therapy when this study was performed in line with clinical
practice at the time

Wolf PA, et al. Stroke 1991; 22: 983-988
%
AF prevalence
Strokes attributable to AF
Age Range (years)
0
10
20
30
50–59 60–69 70–79 80–89
Framingham
Approximately 5-fold increased risk of stroke
Quantify stroke risk: CHADS2/ CHA2DS2-VASc
AF strokes have worse outcomes
Costly health care ~ $16 billion/year

Lone AF (younger persons without evidence of cardiovascular or
precipitating disease)
Transient AF (caused by reversible disorders)
First detected
ParoxysmalSelf-terminating
PersistentNot self-terminating
Permanent
Recurrent AF
(two or more episodes)
Atrial fibrillation – clinical classification
Fuster V et al. Eur Heart J 2006;27:1979–2030
Classification
Paroxysmal: terminates in < 7 days
Persistent: fails to terminate within 7 days
Permanent: > 1 year
Lone: Individuals without structural heart
disease, < 60 yrs old

Paroxysmal
Self-Terminating
Persistent
Lasts > 7 Days
Permanent
Cardioversion
Failed or Not
Attempted
Normal Sinus Rhythm
Atrial Fibrillation
Paroxysmal AF is as likely to cause stroke as
persistent or permanent AF
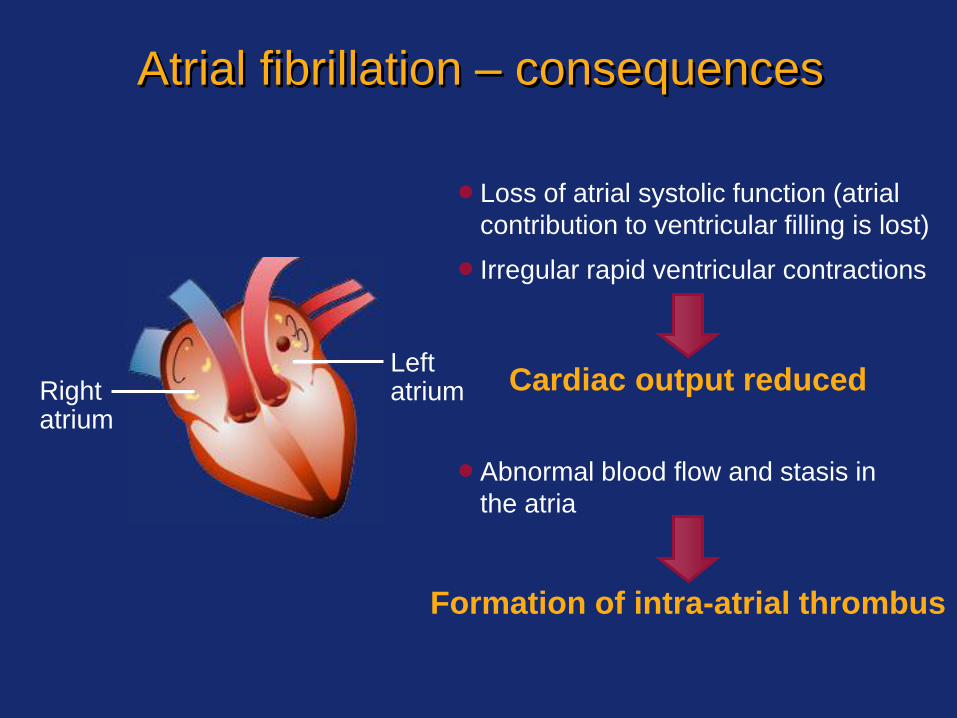
Atrial fibrillation – consequences
Loss of atrial systolic function (atrial
contribution to ventricular filling is lost)
Irregular rapid ventricular contractions
Abnormal blood flow and stasis in
the atria
Cardiac output reduced
Formation of intra-atrial thrombus
Rightatrium
Leftatrium
Atrial fibrillation – manifestations
Palpitations
Rapid heartbeat
Sudden pounding in the chest
Dizziness
Syncope
Chest discomfort
Shortness of breath
Symptoms of AF

Strategies for treating atrial fibrillation
Rhythm control (including cardioversion)
OR
Rate control
PLUS
Anticoagulation therapy
Hemodynamic stabilization

Rhythm and rate control approaches
Rhythm control
Cardioversion
(electrical or
pharmacological)
Pharmacological agents
(Class IC and III
antiarrhythmics)
Surgery
(maze procedure, ablation)
Device implantation
(pacemaker)
Rate control
Pharmacological agents
(AV node blockers)
Surgery with device
implantation (ablation plus
pacemaker insertion)
Pacemaker image courtesy of
St Jude Medical, Inc
Rate Control
Medications
- Metoprolol / Esmolol: IV or Oral
- Diltiazem: IV or Oral
- Verapamil: Oral Only
- Digoxin: Patients with hypotension
- Amiodarone: Also for rhythm control

Rhythm Control
Synchronized DC cardioversion
- Emergencies/Hemodynamic instability
- Greater efficacy than medications
Pharmacologic cardioversion
- If AF < 7days – dofetilide, flecainide, ibutilide,
propaferone or amiodarone
- If AF > 7 day – dofetilide or amiodarone

Electrical cardioversion
Recommendations for successful cardioversion:
Antiarrhythmic drugs to maintain normal sinus rhythm
Anticoagulation >3 weeks before and >1 month after chemical or electrical cardioversion, or permanently if necessary
Transoesophageal echocardiogram (TEE) to detect any clot in the left atrial appendage before cardioversion
Successful cardioversion is more likely if the patient:- has no other cardiovascular problems- has normal sized atria- has been in atrial fibrillation for a relatively short period- had factors contributing to atrial fibrillation (e.g., hyper- or
hypothyroidism)
Heart rhythm
in atrial fibrillation
Cardioversion
shock
Normal heart
rhythm
ECGMetal
paddle
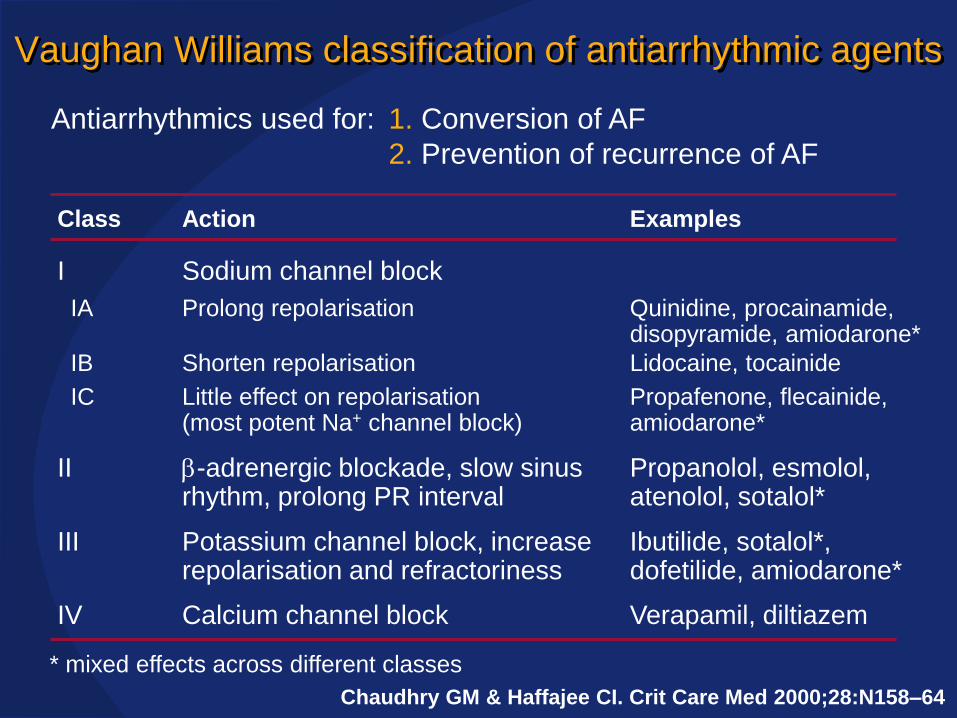
Vaughan Williams classification of antiarrhythmic agents
Verapamil, diltiazemCalcium channel blockIV
Ibutilide, sotalol*, dofetilide, amiodarone*
Potassium channel block, increase repolarisation and refractoriness
III
Propanolol, esmolol, atenolol, sotalol*
b-adrenergic blockade, slow sinus rhythm, prolong PR interval
II
Propafenone, flecainide,amiodarone*
Little effect on repolarisation(most potent Na+ channel block)
IC
Lidocaine, tocainideShorten repolarisationIB
Quinidine, procainamide, disopyramide, amiodarone*
Prolong repolarisationIA
Sodium channel blockI
ExamplesActionClass
Antiarrhythmics used for: 1. Conversion of AF
2. Prevention of recurrence of AF
* mixed effects across different classes
Chaudhry GM & Haffajee CI. Crit Care Med 2000;28:N158–64
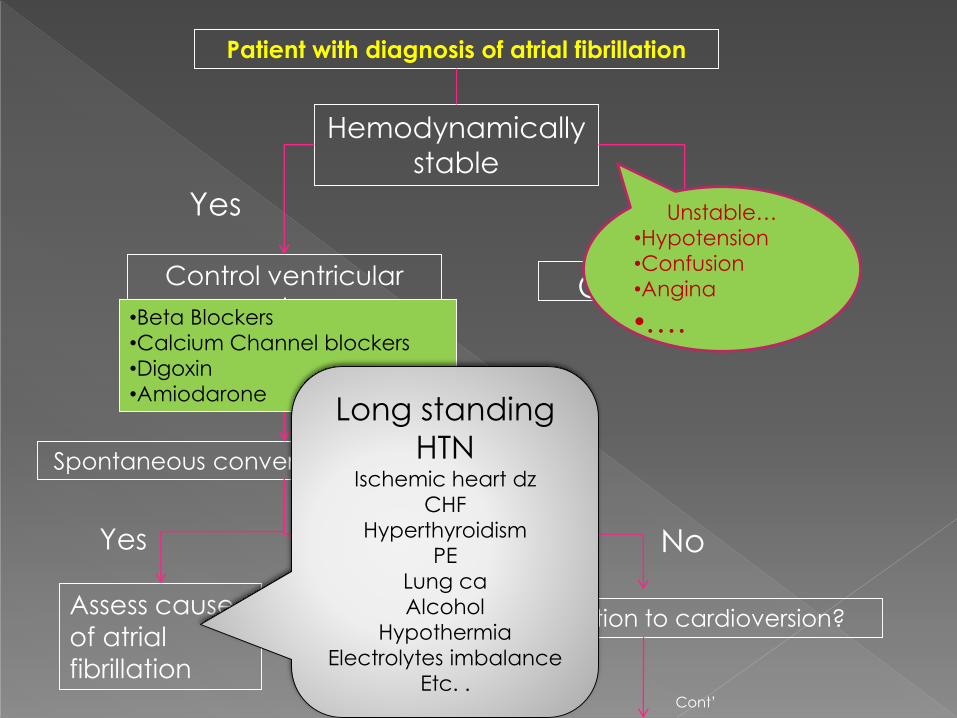
Patient with diagnosis of atrial fibrillation
Hemodynamically
stable
Control ventricular
rate:
Diltiazem
Cardioversion
Yes No
Spontaneous conversion to sinus rhythm
Assess cause
of atrial
fibrillation
Yes No
Contraindication to cardioversion?
Cont’
•Beta Blockers
•Calcium Channel blockers
•Digoxin
•Amiodarone
Unstable…
•Hypotension
•Confusion
•Angina
•….
Long standing
HTNIschemic heart dz
CHF
Hyperthyroidism
PE
Lung ca
Alcohol
Hypothermia
Electrolytes imbalance
Etc. .

UCLA Family Medicine Department IMG Program Carlos Yoo
Consider long-term
anticoagulation
Cardioversion
Yes No
>48hs<48hs
Start Heparin IV
•Immediate
medical or
electrical cardioversion
•Later elective
cardioversion after
3weeks of warfarin
• Early TEE-guided
cardioversion
Atrial fibrillation persist?
Assess cause of atrial
fibrillation
Yes
No
Cont’
Long standing HTN
Ischemic heart dz
CHF
Hyperthyroidism
PE
Lung ca
Alcohol
Hypothermia
Electrolytes imbalance
Etc. .
Warfarin Aspirin

ESC 2012 guidelines: selection of patients
for OACs
Non-valvular atrial fibrillation Valvular atrial fibrillation
< 65 years and lone AF including women
Stroke risk assessment using CHA2DS2-VASc
0 1 ≥2
Assess bleeding risk (HAS-BLED score);
consider patient values/preferences
New oral anticoagulant;
rivaroxaban, dabigatran
apixaban
Vitamin K antagonistNo antithrombotic therapy
Oral anticoagulant
Yes
Camm AJ et al. Eur Heart J 2012 Slide line preferred; dotted line alternative
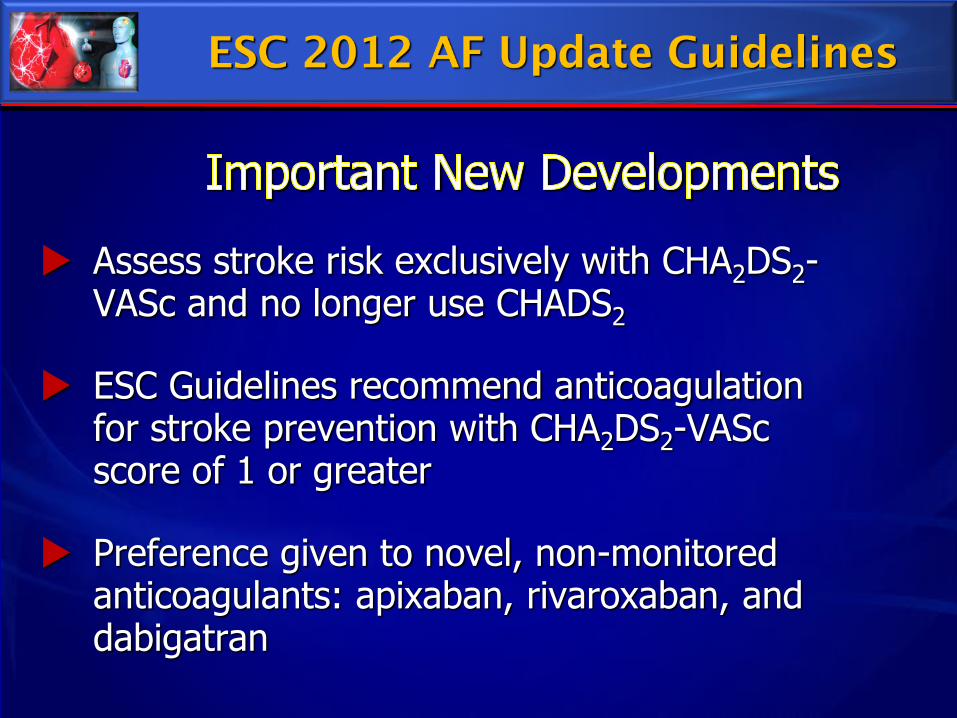
Assess stroke risk exclusively with CHA2DS2-VASc and no longer use CHADS2
ESC Guidelines recommend anticoagulation for stroke prevention with CHA2DS2-VASc score of 1 or greater
Preference given to novel, non-monitored anticoagulants: apixaban, rivaroxaban, and dabigatran

Congestive heart failure or LVEF < 35% 1
Hypertension 1
Age > 75 years 2
Diabetes mellitus 1
Stroke/TIA/systemic embolism 2
Vascular Disease (MI/PAD/Aortic plaque) 1
Age 65-74 years 1
Sex category (female) 1
Moderate-High risk > 2
Low risk 0-1
Lip GYH, Halperin JL. Am J Med 2010; 123: 484.
Weight (points)
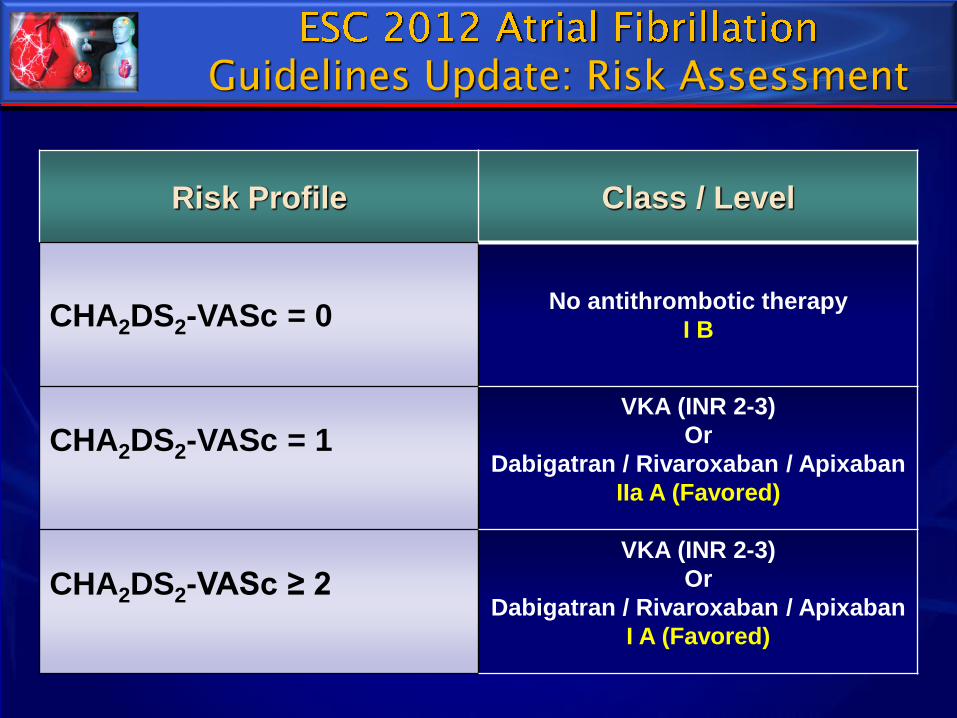
Risk Profile Class / Level
CHA2DS2-VASc = 0No antithrombotic therapy
I B
CHA2DS2-VASc = 1VKA (INR 2-3)
Or
Dabigatran / Rivaroxaban / Apixaban
IIa A (Favored)
CHA2DS2-VASc ≥ 2VKA (INR 2-3)
Or
Dabigatran / Rivaroxaban / Apixaban
I A (Favored)
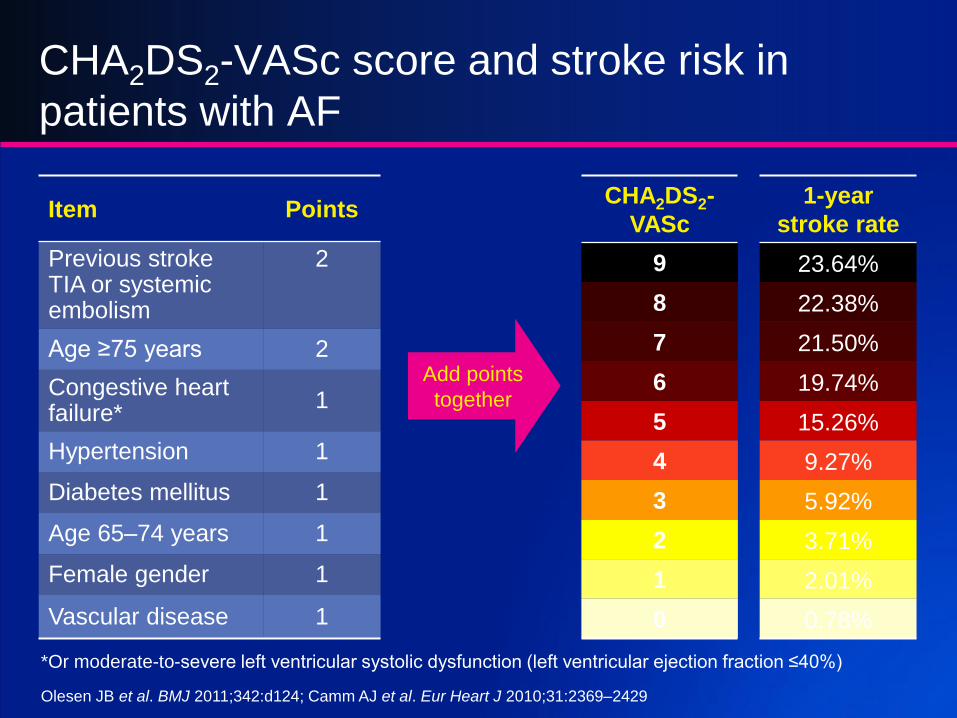
CHA2DS2-VASc score and stroke risk in
patients with AF
Item Points
Previous strokeTIA or systemic embolism
2
Age ≥75 years 2
Congestive heart failure*
1
Hypertension 1
Diabetes mellitus 1
Age 65–74 years 1
Female gender 1
Vascular disease 1
CHA2DS2-
VASc
1-year
stroke rate
9 23.64%
8 22.38%
7 21.50%
6 19.74%
5 15.26%
4 9.27%
3 5.92%
2 3.71%
1 2.01%
0 0.78%
*Or moderate-to-severe left ventricular systolic dysfunction (left ventricular ejection fraction ≤40%)
Olesen JB et al. BMJ 2011;342:d124; Camm AJ et al. Eur Heart J 2010;31:2369–2429
Add points
together
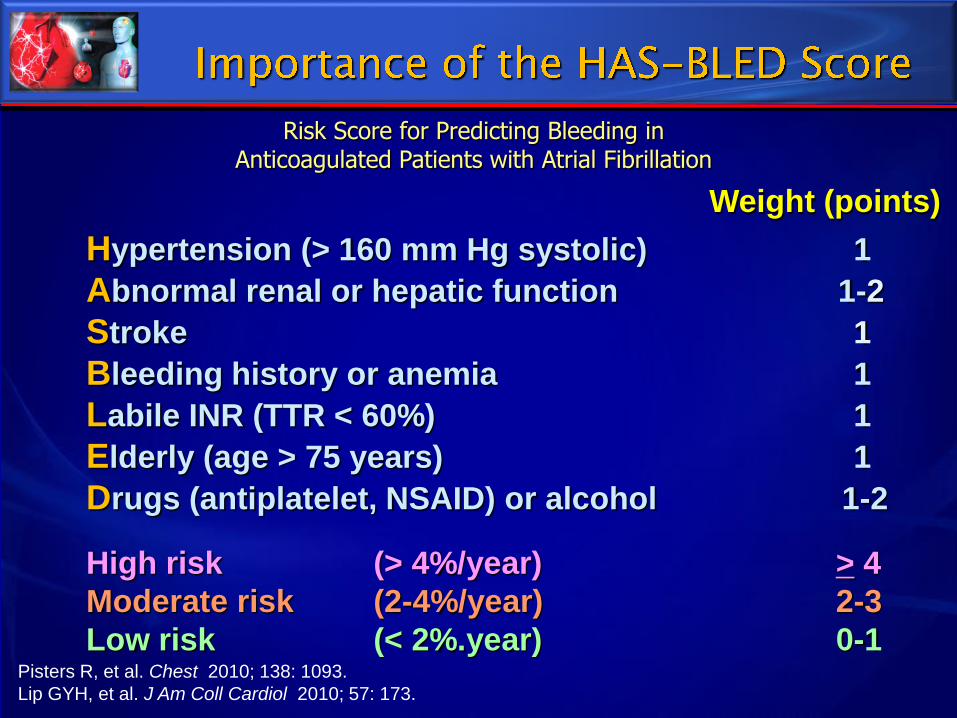
Hypertension (> 160 mm Hg systolic) 1
Abnormal renal or hepatic function 1-2
Stroke 1
Bleeding history or anemia 1
Labile INR (TTR < 60%) 1
Elderly (age > 75 years) 1
Drugs (antiplatelet, NSAID) or alcohol 1-2
High risk (> 4%/year) > 4
Moderate risk (2-4%/year) 2-3
Low risk (< 2%.year) 0-1 Pisters R, et al. Chest 2010; 138: 1093.
Lip GYH, et al. J Am Coll Cardiol 2010; 57: 173.
Weight (points)
Risk Score for Predicting Bleeding inAnticoagulated Patients with Atrial Fibrillation

Hankey GJ and Eikelboom JW. Circulation. 2011; 123: 1436-1450
Patients with bleeding on NOAC therapy
Mild bleedingModerate-Severe
bleedingLife-threatening
bleeding
• Delay next dose or discontinue treatment as appropriate
• Mechanical compression• Surgical intervention• Fluid replacement and
hemodynamic support• Blood product transfusion• Oral charcoal • Hemodialysis• ? Prothrombin Complex
Concentrate?(Circulation 2011; 2011: 124: 1573-9)
• Consideration of rFVIIa or PCC
• Charcoal filtration• ? Prothrombin Complex
Concentrate(Circulation 2011; 2011: 124:
1573-9)
► CHA2DS2-VASc has replaced CHADS2 as the predominant assessment tool to predict stroke risk (ESC 2012 AF Guidelines Update).
► HAS-BLED has gained dominance as the most predictive bleeding index. It is best used as a cautionary “yellow flag” rather than as a reason to withhold anticoagulation (ESC 2012).
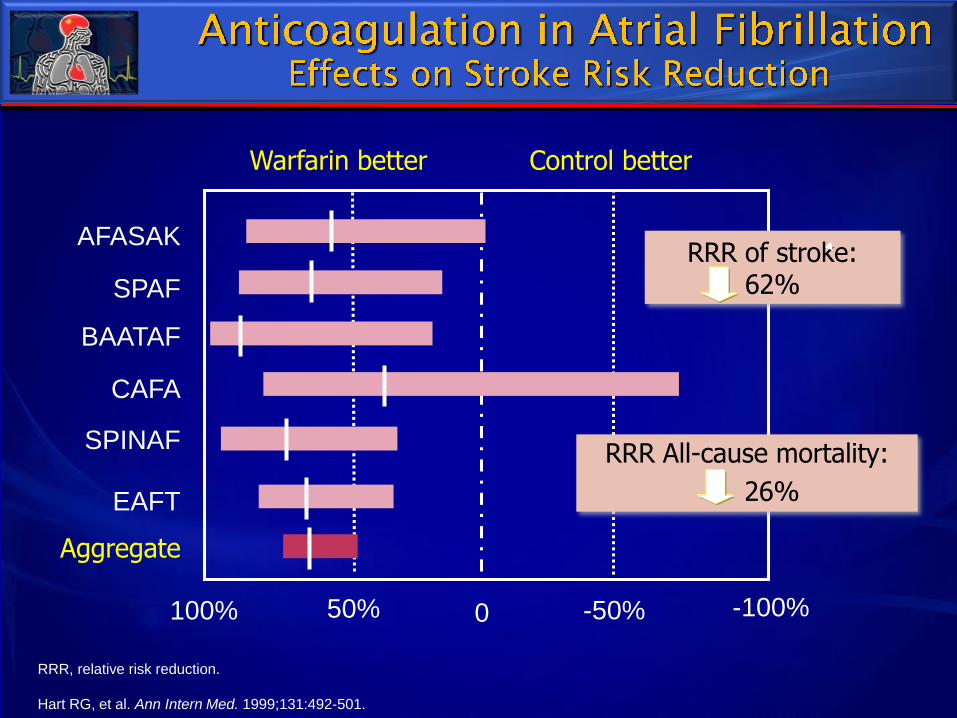
Warfarin better Control better
AFASAK
SPAF
BAATAF
CAFA
SPINAF
EAFT
100% 50% 0 -50% -100%
Aggregate
RRR of stroke: 62%
RRR All-cause mortality:
26%
RRR, relative risk reduction.
Hart RG, et al. Ann Intern Med. 1999;131:492-501.
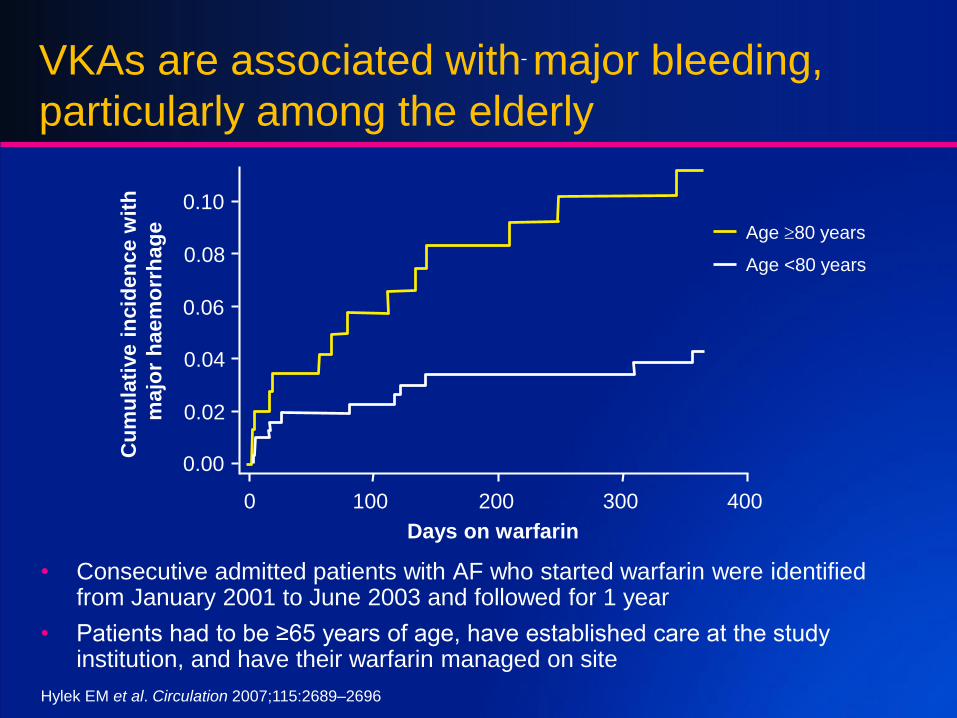
VKAs are associated with major bleeding,
particularly among the elderly
• Consecutive admitted patients with AF who started warfarin were identified from January 2001 to June 2003 and followed for 1 year
• Patients had to be ≥65 years of age, have established care at the study institution, and have their warfarin managed on site
Days on warfarin
Cu
mu
lati
ve i
ncid
en
ce w
ith
majo
r h
ae
mo
rrh
ag
e
0.10
0.08
0.06
0.04
0.02
0.00
0 100 200 300 400
Age 80 years
Age <80 years
Hylek EM et al. Circulation 2007;115:2689–2696

VKAs have a narrow therapeutic window
• INR below 2 is associated with
an increased risk of ischaemia
• INR above 3 is associated
with an increased risk of
haemorrhagic stroke
1. Amouyel P et al. Eur J Intern Med 2009;20:63–69; 2. Pouyanne P et al. BMJ 2000;320:1036
VKA-related haemorrhage is the leading cause of iatrogenic hospitalization,
accounting for 13% of hospitalizations due to drug-related adverse events2
Ischaemic stroke1 Haemorrhagic stroke1
0 1 2 3 4 5 60
2
4
6
8
10
12
Str
oke r
ate
per
100
pa
tie
nt-
ye
ars
0 1 2 3 4 5 60
2
4
6
8
12
16
Str
ok
e r
ate
pe
r
100
pa
tie
nt-
ye
ars
ObservedPredicted95% CI
ObservedPredicted95% CI
10
14
1) Delayed onset/offset
2) Unpredictable dose response
3) Narrow therapeutic index
4) Drug-drug, drug-food interactions
5) Problematic monitoring
6) High bleeding rate
7) Slow reversibility

VKAs have many drug–drug interactions
Increased INR response Decreased INR response
Coumadine Package Insert US revised January 2010
Despite continued use of warfarin, NOACs are considered by many professional medical organizations to be the “best option” for anticoagulation of SPAF patients:
► ESC 2012 AF Update Guidelines
► ACCP 2012 Guidelines
► Canadian AF Guidelines
“ ”

Targets for anticoagulants
VKA VKA
Inactive Factor
Active Factor
Transformation
Catalysis
X IX
IXa
Thrombin
X
a
Fibrinogen Fibrin
Prothrombin
VIITF VIIa
Clot formation
Initiation
Propagation VKA
Direct Factor Xa inhibitionRivaroxaban
Apixaban
Edoxaban
Betrixaban
Direct Factor IIa inhibitionDabigatran
II
IIa
Piccini JP et al. Curr Opin Cardiol 2010;25:312–320; Spyropoulos AC et al. Expert Opin Investig Drugs 2007;16:431–440
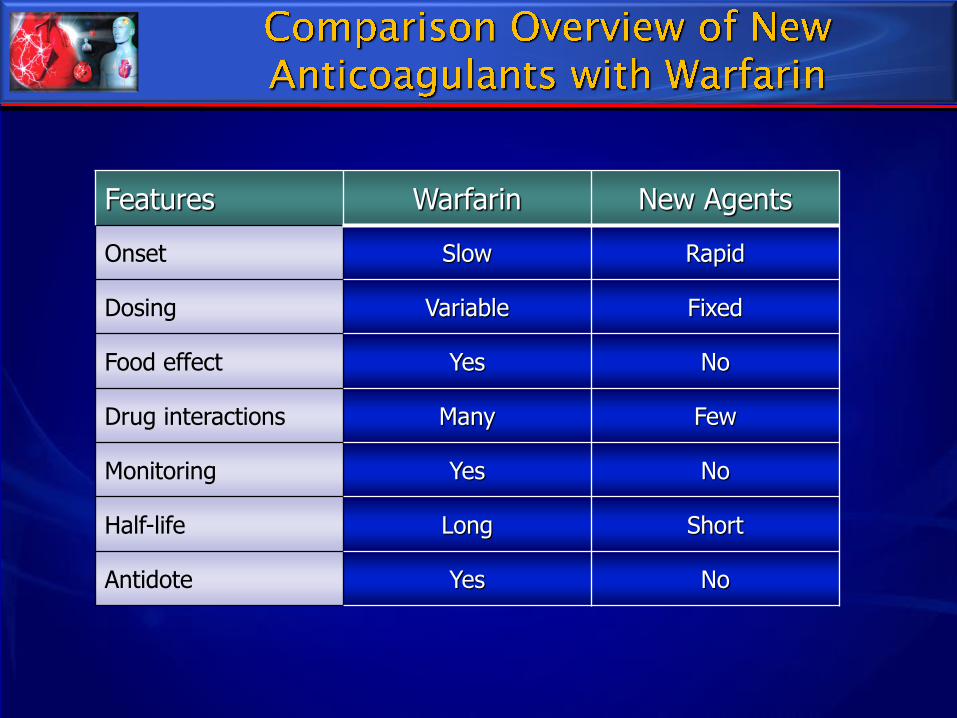
Features Warfarin New Agents
Onset Slow Rapid
Dosing Variable Fixed
Food effect Yes No
Drug interactions Many Few
Monitoring Yes No
Half-life Long Short
Antidote Yes No
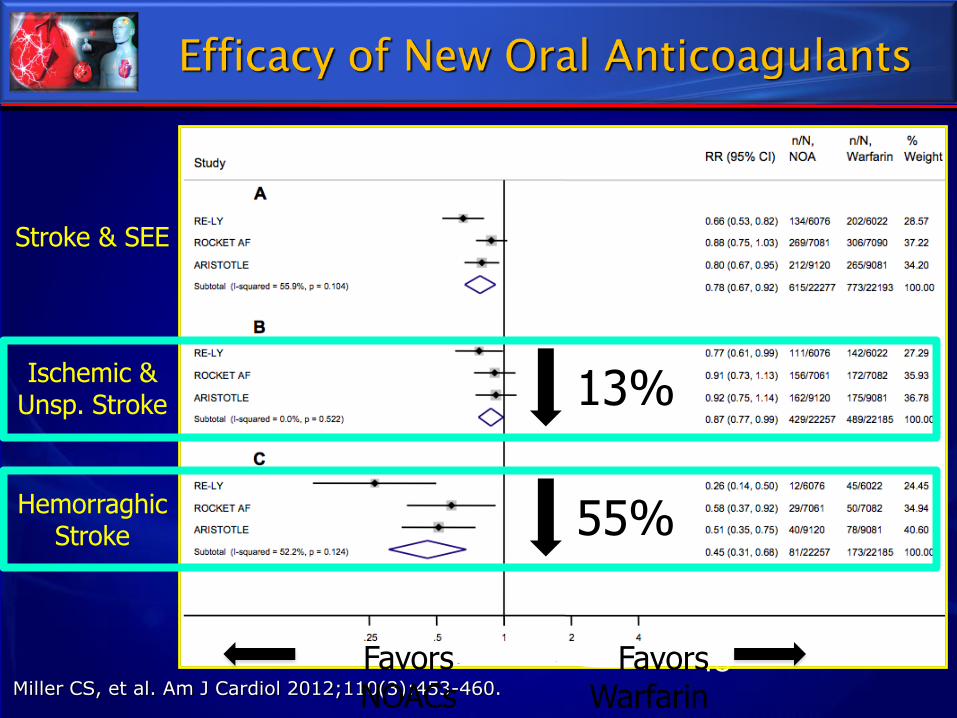
45
Stroke & SEE
Ischemic & Unsp. Stroke
Hemorraghic Stroke
Miller CS, et al. Am J Cardiol 2012;110(3):453-460.
Favors NOACs
Favors Warfarin
13%
55%

Major
ICH
GI
Bleeding
Miller CS, et al. Am J Cardiol 2012;110(3):453-460.
51%
Favors NOACs
Favors Warfarin
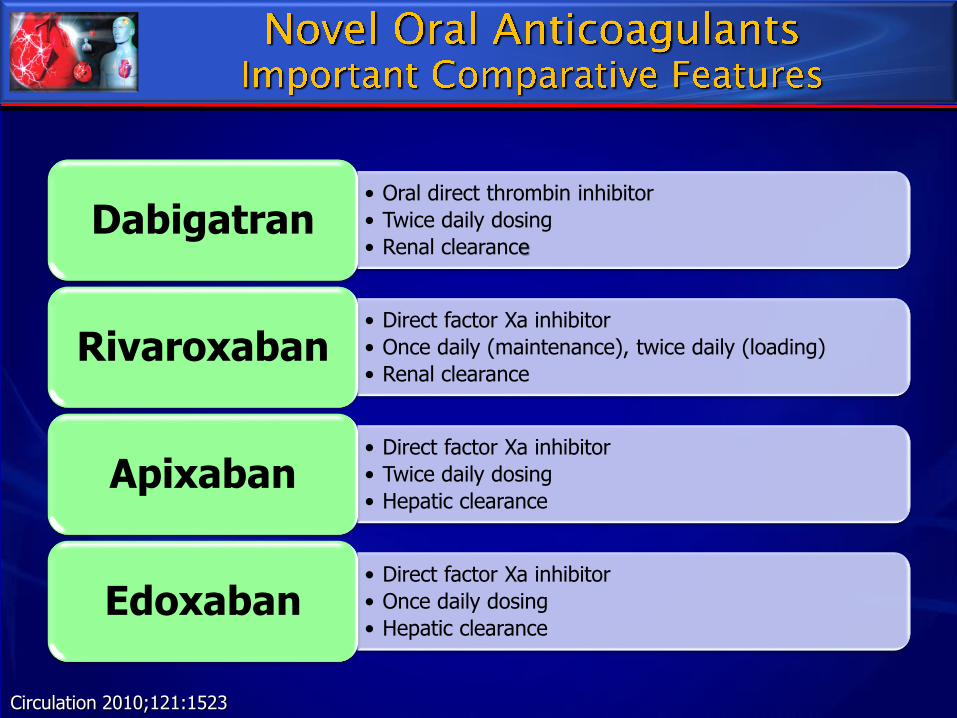
• Oral direct thrombin inhibitor
• Twice daily dosing
• Renal clearanceDabigatran
• Direct factor Xa inhibitor
• Once daily (maintenance), twice daily (loading)
• Renal clearanceRivaroxaban
• Direct factor Xa inhibitor
• Twice daily dosing
• Hepatic clearanceApixaban
• Direct factor Xa inhibitor
• Once daily dosing
• Hepatic clearanceEdoxaban
Circulation 2010;121:1523

ESC 2012 guidelines: recommendations for new OACS
• Dabigatran 150 mg bid
• Dabigatran 110 mg bid in:
• ≥ 80 years
• Concomitant use of
interacting drugs
• HAS-BLED ≥ 3
• CrCl 30-49 mL/min
• Peri-cardioversion
• No recommendation in
severe renal impairment
CrCl < 30 mL/min
• Apixaban
• No recommendation in
severe renal impairment
CrCl <30 mL/min
• No recommendation for
cardioversion *
• Approved by FDA on
Dec. 28, 2012 and by
EMA on Nov 20, 2012..
All NOACs are recommended for SPAF in patients at risk of
stroke (CHA2DS2-VASc≥2) in preference over a VKA
• Rivaroxaban 20 mg od
• Rivaroxaban 15 mg od
with:
• HAS-BLED ≥3
• CrCl 30-49 mL/min
• No recommendation in
severe renal impairment
CrCl < 30 mL/min
• No recommendation for
cardioversion*
Camm AJ et al. Eur Heart J 2012; od=once daily; bid=twice daily*based on lack of published data
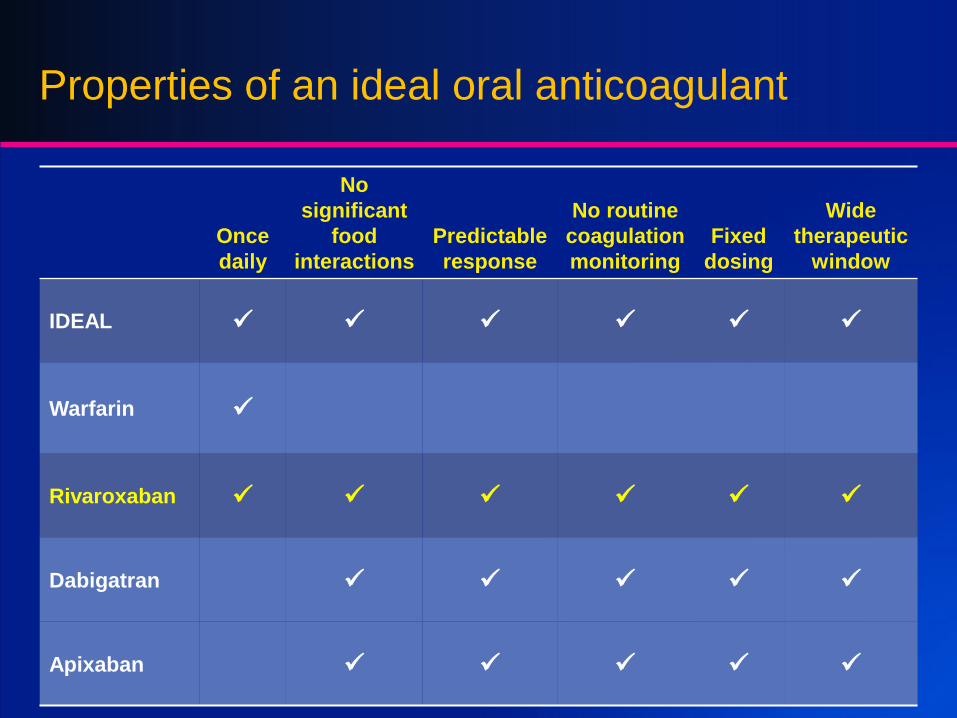
Properties of an ideal oral anticoagulant
Once
daily
No
significant
food
interactions
Predictable
response
No routine
coagulation
monitoring
Fixed
dosing
Wide
therapeutic
window
IDEAL
Warfarin
Rivaroxaban
Dabigatran
Apixaban

ESC 2012 guidelines: ASA/DAPT
• Antiplatelet therapy for SPAF should be limited to patients who
refuse/cannot take VKAs/NOACs
– Consider in patients who refuse OAC and at low bleeding risk
• DAPT (ASA/clopidogrel) or
• less effectively ASA
• No evidence for the decrease in total or CV mortality with ASA (or
antiplatelet drugs) in SPAF
• Antiplatelet therapy (including ASA monotherapy) carries a similar
risk of major bleeding and ICH as OAC, particularly in the elderly
Camm AJ et al. Eur Heart J 2012; DAPT=dual antiplatet therapy; ICH=intracranial haemorrhage

ROCKET AF
Rivaroxaban Once Daily Oral Direct Factor Xa Inhibition
Compared with Vitamin K Antagonism for Prevention of
Stroke and Embolism Trial in Atrial Fibrillation
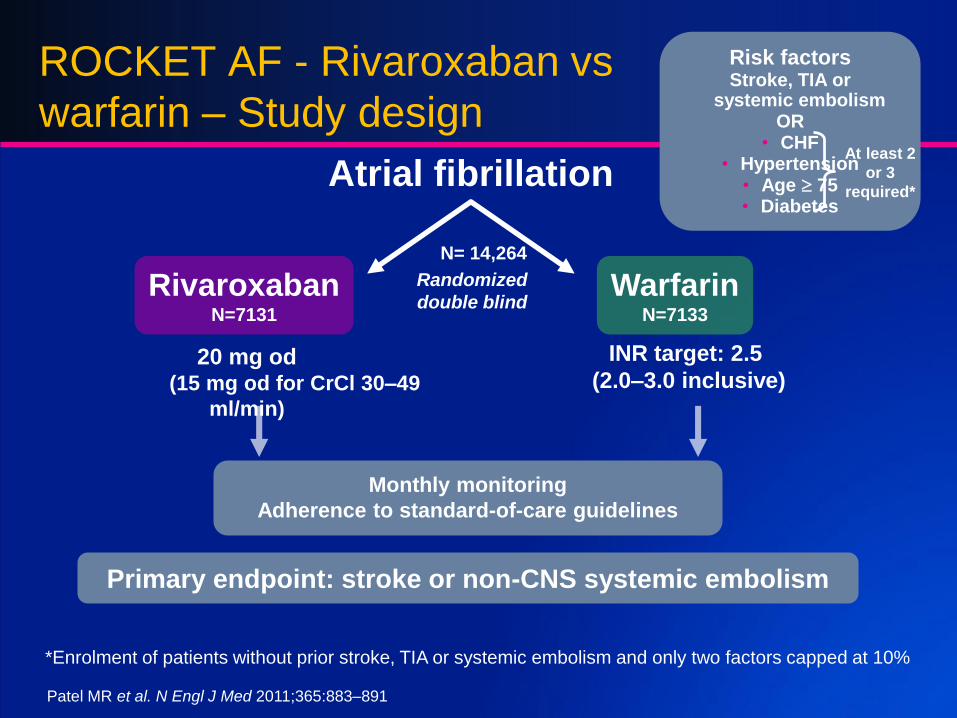
ROCKET AF - Rivaroxaban vs
warfarin – Study design
RivaroxabanN=7131
WarfarinN=7133
Primary endpoint: stroke or non-CNS systemic embolism
INR target: 2.5
(2.0–3.0 inclusive)20 mg od
(15 mg od for CrCl 30–49
ml/min)
Atrial fibrillation
Randomized
double blind
Monthly monitoring
Adherence to standard-of-care guidelines
*Enrolment of patients without prior stroke, TIA or systemic embolism and only two factors capped at 10%
Risk factorsStroke, TIA or
systemic embolism OR
• CHF • Hypertension
• Age 75 • Diabetes
At least 2
or 3
required*
Patel MR et al. N Engl J Med 2011;365:883–891
N= 14,264
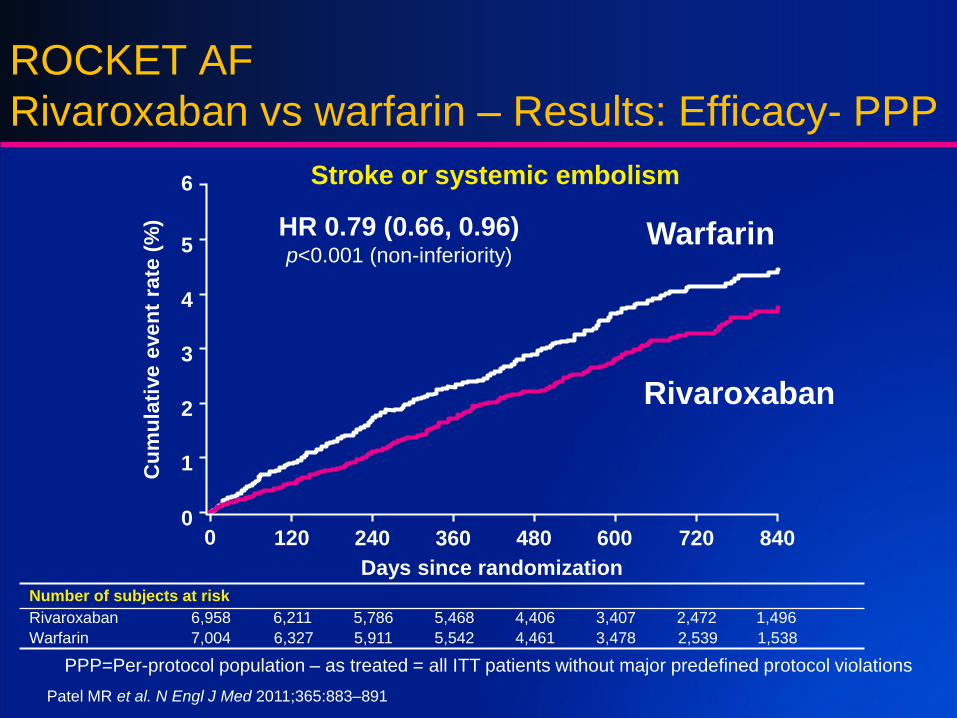
Number of subjects at risk
Rivaroxaban 6,958 6,211 5,786 5,468 4,406 3,407 2,472 1,496
Warfarin 7,004 6,327 5,911 5,542 4,461 3,478 2,539 1,538
ROCKET AF
Rivaroxaban vs warfarin – Results: Efficacy- PPP
PPP=Per-protocol population – as treated = all ITT patients without major predefined protocol violations
Days since randomization
Warfarin
Rivaroxaban
HR 0.79 (0.66, 0.96)p<0.001 (non-inferiority)
0 120 240 480 600 7200
1
2
3
4
5
6
840360
Cu
mu
lati
ve e
ven
t ra
te (
%)
Stroke or systemic embolism
Patel MR et al. N Engl J Med 2011;365:883–891
ROCKET AF
Rivaroxaban vs warfarin – Conclusions
• Based on the prespecified primary efficacy outcome:
– A once-daily fixed-dose regimen of rivaroxaban was non-inferior to warfarin for
prevention of stroke or non-CNS systemic embolism
– Rivaroxaban was superior to warfarin while patients were taking study drug
– A sensitivity analysis in the ITT population that followed all patients in the trial until
completion showed a benefit for rivaroxaban, but did not reach superiority
• Safety:
– Similar overall incidence of bleeding and adverse events
– Increase in gastrointestinal bleeds but fewer intracranial haemorrhages and less
fatal bleeding with rivaroxaban
• Implication:
– Rivaroxaban, administered once daily, has demonstrated non-inferiority to
warfarin in the prevention of stroke or systemic embolism, with similar overall
bleeding and fewer intracranial haemorrhages and fatal bleeds
Patel MR et al. N Engl J Med 2011;365:883–891
KEY POINTS
► VKA is a very effective for SPAF but related to some limitations that can lead to underuse by both patient and physician.
► Novel Oral Anticoagulants offer favourable risk–benefit profile compare to VKA, with significant reductions in stroke, intracranial haemorrhage, and mortality, and with similar major bleeding as for warfarin.
• Rivaroxaban, administered once daily, has demonstrated non-inferiority to warfarin, both in primary and secondary prevention of stroke or systemic embolism with similar overall bleeding and fewer intracranial haemorrhages and fatal bleeds