obesity and coronary heart disease: psychology throughout
TRANSCRIPT

Obesity and Coronary Heart Disease:
Psychology Throughout the Course of Illness
PSIKOLOGI KESEHATAN
2016

Ruang Lingkup
• Obesity
• How Common Is Obesity?
• Obesity Treatment
• Should Obesity be Treated at All?
• Coronary Heart Disease
• Rehabilitation of Patients with CHD
• Predicting Patient Health Outcomes
• Assumptions in Health Psychology

OBESITY – The Role of Psychological Factors
• Peranan obesitas dalam onset terjadinya obesitas dan peran dalam membentuk keyakinan dan perilaku, bagaimana seseorang mengatasi dan menyesuaikan keadaannya, bagaimana tatalaksanan dan konsekuensi seseorang dalam segi fisik dan psikologis.
• Peranan psikologi dalam obesitas akan meliputi :• Konsekuensi
• Penyebab
• Penatalaksanaan
What is Obesity?
• Population means
Stunkard (1984) suggested that obesity should be categorized
as either mild (20–40 per cent overweight), moderate (41–100 per cent overweight) or severe (100 per cent overweight).
• BMI
normal weight (20–24.9); overweight (grade 1,25–29.9); clinical obesity (grade 2, 30–39.9); and severe obesity (grade 3, 40)

• Waist circumference• For men, low waist circumference is < 94cm; high is 94−102cm and very high
is > 102cm.
• For women, low waist circumference is < 80cm; high is 80−88cm and veryhigh is > 88cm.
• Percentage body fat• As health is mostly associated with fat rather than weight per se, researchers
and clinicians have also developed methods of measuring percentage body fat directly.


How Common is Obesity?



What Are The Problems With Obesity?
• Physical Problems : Cardiovascular disease, diabetes, joint trauma, back pain, cancer, hypertension and mortality
• Psychological Problems : contemporary cultural obsession with thinness, the aversion to fat low self esteem and poor self image, deppression, bipolar disorder, panic disorder or agoraphobia

What Causes Obesity?
• Physiological Theories :• Genetic Theories
• Twin studies : genetic factors accounted for 66-70 % in variance in body weight
• Adoptee studies : biological mother’s weight
• Metabolic Rate TheoryResting metabolic rate : kecepatan penggunaan energi ketika tubuh manusia sedang tidak melakukan aktivitas. Teori ini mengatakan pada orang obesitas mempunyai metabolic rate yang rendah, dan hanya membakar energi dalam jumlah sedikit ketika sedang beristirahat sehingga hanya perlu sedikit asupn makanan untuk aktivitas sehari-hari.
• Appetite Regulation

• The Obesogenic Environment : understanding the environmental factors which promote obesity does not seem to be a sufficient explanatory model.
• Behavioural Theories• Physical Activity : decreases in daily energy expenditure due to
improvements in transport systems, and a shift from an agricultural society to an industrial and increasingly information-based one.
Do the obese exercise less?
• It is possible that the obese take less exercise due to factors such as embarrassment and stigma and that exercise plays a part in the maintenance of obesity but not in its cause.
• exercise may have psychological and general health effects, which could benefit the obese either in terms of promoting weight loss or simply by making them feel better about themselves

Eating Behaviour
• These perspectives emphasize mechanisms such as exposure, modelling and associative learning, beliefs and emotions, body dissatisfaction and dieting, all of which can help explain obesity. For example, it is possible that the obese have childhoods in which food is used to reward good behaviour, or have parents who overeat, or hold cognitions about food which drive eating behaviour. It is also possible that dieting when moderately overweight (or just feeling fat) triggers episodes of overeatingwhich themselves cause increases in body fat
• Original studies of obesity were based on the assumption that the obese ate for different reasons than people of normal weight (Ferster et al. 1962). Schachter’s externality theory suggested that, although all people were responsive to environmental stimuli such as the sight, taste and smell of food, and that such stimuli might cause overeating, the obese were highlyand sometimes uncontrollably responsive to external cues

emotionality theory of eating behaviour
• Bruch (e.g. 1974) developed a psychosomatic theory of eatingbehaviour and eating disorders which argued that some people interpret the sensations of such emotions as emptiness as similar to hunger and that food is used as a substitute for other forms of emotional comfort.
• Van Strien et al. (2009) explored the relationship between dietary restraint, emotional and external eating, overeating and BMI to assess how people resist (or not) the opportunity to become overweight offered by the obesogenic environment.

Conclusion for the causes of obesity :
• There is good evidence for a genetic basis to obesity. The evidence for how this is expressed is weak.
• The prevalence of obesity has increased at a similar rate to decreases in physical activity.
• There is some evidence that the obese exercise less than the non-obese.
• The prevalence of obesity has increased at a rate unrelated to the overall decrease in calorie consumption (but measured in the home).
• There is inconsistent evidence as to whether the obese eat more calories than the non-obese.
• The obese may eat differently and for different reasons than the non-obese.
• The relative increase in fat is parallel to the increase in obesity.
• The obese may eat proportionally more fat than the non-obese.

OBESITY TREATMENT
• Traditional Treatment ApproachesThe programme aimed to encourage eating in response to physiological hunger and not in response to mood cues such as boredom or depression, or in response to external cues such as the sight and smell of food or the sight of other people eating.
• Multidimensional Behavioural ProgrammesProgrammes aim to encourage the obese to eat less than they do usually rather than encouraging them to eat less than the non-obese.

The Role of Dieting
• Psychological Problems and Obesity Treatment• Suggests that the obese respond to dieting in the same way as the non-obese, with
lowered mood and episodes of overeating, both of which are detrimental to attempts at weight loss.
• Physiological Problems and Obesity Treatment• In addition to the psychological consequences of imposing a dieting structure on the
obese, there are physiological changes which accompany attempts at food restriction. Heatherton et al. (1991) reported that restraint in the non-obese predicts weight fluctuation, which parallels the process of weight cycling or ‘yo-yo’ dieting in the obese. Research has also found that weight fluctuation may have negative effectson health, with reports suggesting an association between weight fluctuation and mortality and morbidity from CHD (Hamm et al. 1989) and all-cause mortality (Lissner et al. 1991).

• Dieting, Obesity and Health• Restraint theory (see Chapter 5) suggests that dieting has negative
consequences, and yet the treatmentof obesity recommends dieting as a solution. This paradox can be summarized as follows:• Obesity is a physical health risk, but restrained eating may promote weight cycling, which
is also detrimental to health.
• Obesity treatment aims to reduce food intake, but restrained eating can promote overeating.
• The obese may suffer psychologically from the social pressures to be thin (although evidence of psychological problems in the non-dieting obese is scarce), but failed attempts to diet may leave them depressed, feeling a failure and out of control. For those few who do succeed in their attempts at weight loss, Wooley and Wooley (1984: 187) suggest that they ‘are in fact condemned to a life of weight obsession, semi-starvation and all the symptoms produced by chronic hunger . . . and seem precariously close to developing a frank eating disorder’.
Should Obesity Be Treated At All?
• The Benefits• dieting may be rejected as a treatment but weight loss may still be seen as
beneficial.

The Treatment Alternatives
• Drug Treatments
• Surgical Treatments

CORONARY HEART DISEASE

Introduction
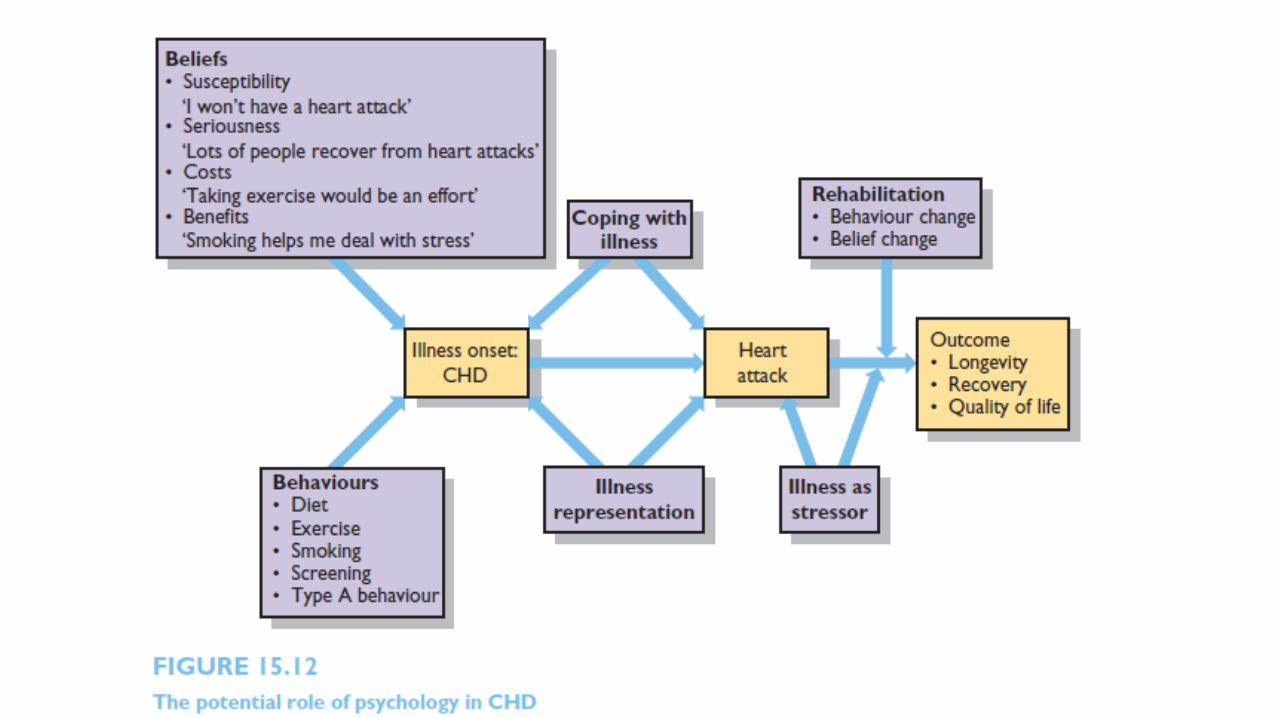
• CHD is another example of chronic illness which shows a strong role for a range of psychological factors.

Risk Factors for CHD
• Smoking
• Diet
• High blood Pressure
• Type A behaviour and hostility
• Stress

Beliefs About CHD
• The results also showed some changes over time, with patients being less likely to blame their behaviour and/or personality as time went on.
• Therefore both sufferers and non-sufferers of CHD seem to hold beliefs about the cause of MI which might influence their subsequent risky behaviour and reflect a process of adjustment once they have become ill.
The Psychological Impact of CHD
• Anxiety and Depression
• PTSD
• Finding Meaning
Rehabilitation of Patients With CHD
• Predicting uptake of rehabiliation
• Modifying Risk Factors• Exercise
• Type A Behaviour
• General Lifestyle Factors
• Illness Cognitions
• Stress

Predicting Patient Health Outcomes
• Quality of Life and Level Functioning• Perception of control
• Goal Disturbance
• Depression
• Social Support
• Illnes Cognitions
• Mortality• Health Behaviours
• Depression
Conclusion
Illnesses such as obesity and CHD illustrate the role of psychology throughout the course of an illness. For example, psychological factors play a role in illness onset (e.g. health beliefs, health behaviours, personality, coping mechanisms), illness progression (e.g. psychological consequences, adaptation, health behaviours) and longevity (e.g. health behaviours, coping mechanisms, quality of life). These psychological factors are also relevant to a multitude of other chronic and acute illnesses, such as diabetes, asthma, chronic fatigue syndrome and multiple sclerosis. This suggests that illness is best conceptualized not as a biomedical problem but as a complex interplay of physiological and psychological factors.
Assumptions in Health Psychology
1. The role of behaviour in illness. Throughout the twentieth century there was an increasing emphasis on behavioural factors in health and illness. Research examined the problem of obesity from the same perspective and evaluated the role of overeating as a causal factor. However, perhaps not all problems are products of behaviour.
2. Treatment as beneficial. Drug and surgical interventions are stopped if they are found to be either ineffective or to have negative consequences. However, behavioural interventions to promote behaviour change, such as smoking cessation, exercise and weight loss programmes, are developed and promoted even when the evidence for their success is poor. Within health psychology,
behavioural programmes are considered neutral enough to be better than nothing. However, obesity treatment using dieting is an Example of the potential negative side-effects of encouraging individual responsibility for health and attempting to change behaviour. Perhaps behavioural interventions can have as many negative consequences as other medical treatments.
• The mind–body problem. Research into obesity and CHD raises the problem of the relationship between the mind and the body. Theories are considered either physiological or psychological and treatment perspectives are divided in a similar fashion, thereby maintaining a dualistic model of individuals.

THANK YOU