kuliah pengantar epi,pato,klinik, diagnosis malaria
TRANSCRIPT
Epidemiology,
Pathogenesis, Clinical Features, and
Diagnosis of
Malaria

NextPrevious
Human malaria : Sp Plasmodium
1. Plasmodium falciparum2. Plasmodium vivax3. Plasmodium ovale4. Plasmodium malariae
Animal – Monkey• Plasmodium knowlesi,
INTRODUCTION
The majority of malaria infection is caused by :
P. falciparum orP. Vivax
Most malaria-associated deaths are due to P. falciparum
Mixed infection due to more than one malarial species occurs in 5 to 7 percent of infections.
Malaria infection has been increasing over recent years due to a combination of factors including:
• Increasing resistance of malarial parasites to chemotherapy • Increasing resistance of the Anopheles mosquito vector to insecticides
• Ecologic and climate changes
• Increased international travel to malaria-endemic areas
EPIDEMIOLOGY
• Approximately 300 to 500 million cases of malaria and• 700,000 to 2.7 million deaths occur annually worldwide –
in children in tropical developing countries
• P. falciparum predominates in tropical Africa, Southeast Asia, Oceania, Haiti, the Amazon basin of
South America, and the Dominican Republic,
• P. vivax is most prevalent in Central America, the Middle East, and India.
Approximately 30,000 travelers from industrialized countries contract malaria each year
The intensity of transmission in different regions affects the risk of acquiring malaria for travelers.
The approximate relative risk of malaria for travelers who stay in an endemic region for one month and
do not take chemoprophylaxis is as follows:
Oceania — 1:30 or higher Sub-Saharan Africa — 1:50 Indian subcontinent — 1:250 Southeast Asia — 1:1,000 South America — 1:2,500 Central America — 1:10,000
TRANSMISSION
Malaria transmission is predominantly via the bite of a female Anopheles sp. Mosquito
Other potential mechanisms for transmission include:
• congenitally acquired disease, • blood transfusion,
• sharing of contaminated needles, and • organ transplantation
LIFE CYCLE
Human infection by all four Plasmodia spp occurs by transmission of sporozoites via a bite from an infected anopheline mosquito.
The sporozoites travel from the salivary glands of the mosquito through the bloodstream of the host to the liver.
In the liver, they invade hepatocytes and divide many 1000-fold until mature tissue schizonts, each containing thousands of daughter merozoites, are formed.
This exoerythrocytic stage is asymptomatic.
The liver schizonts rupture after 6 to 16 days and release thousands of merozoites into the bloodstream, where they interact with specific erythrocyte membrane proteins and invade red blood cells
This the erythrocytic stage is symptomatic
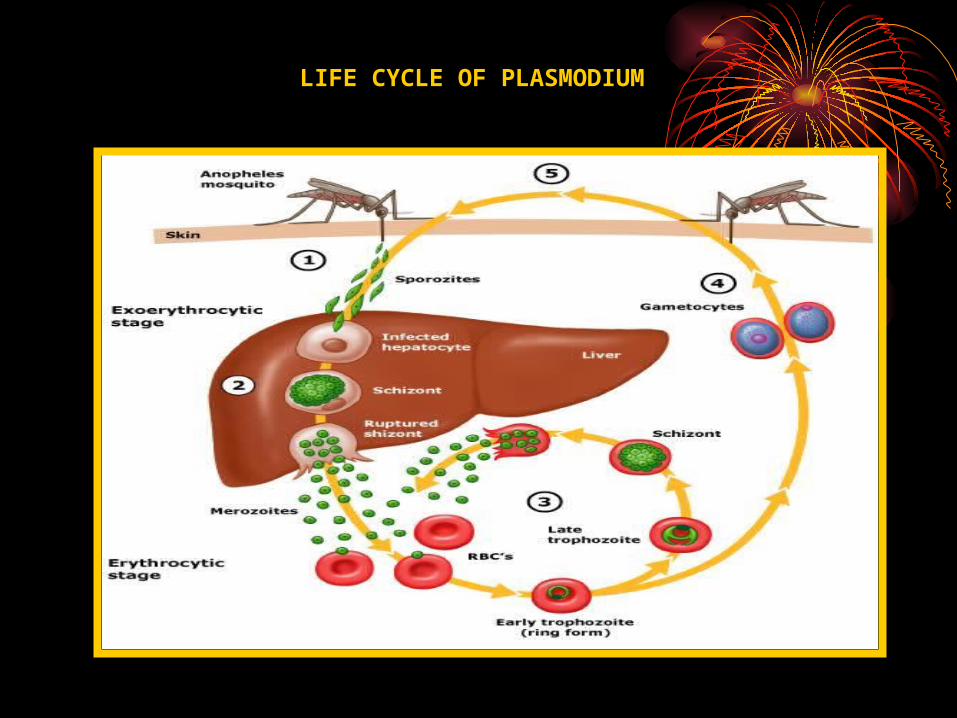
LIFE CYCLE OF PLASMODIUM
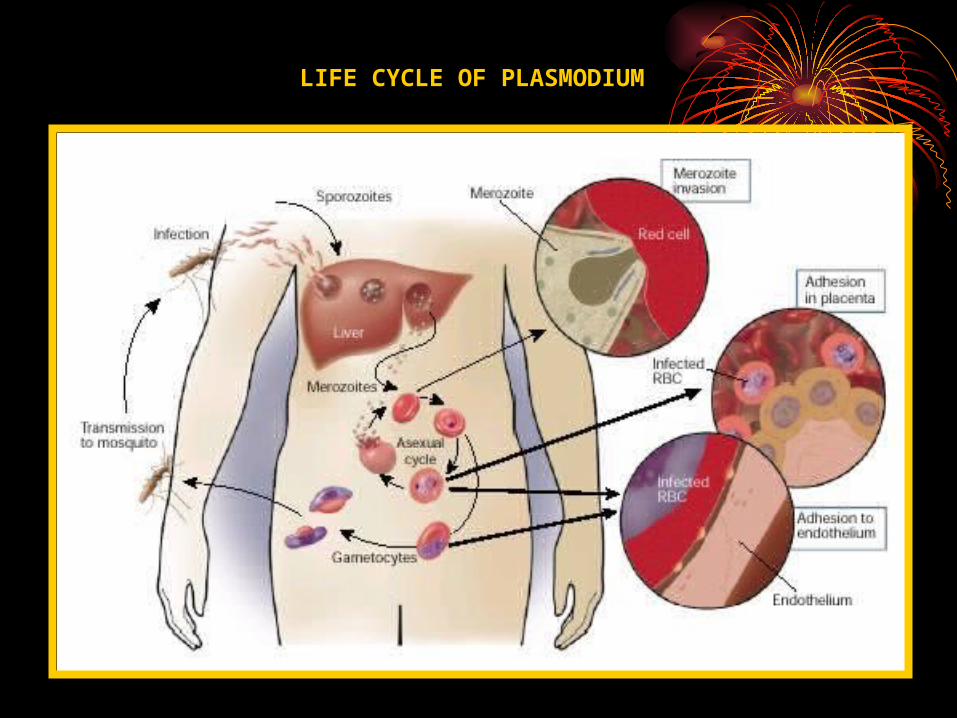
LIFE CYCLE OF PLASMODIUM
• Four malaria parasite species digest red cell proteins and hemoglobin.
• The parasites derive energy from anaerobic glycolysis of glucose to lactic acid, which can cause hypoglycemia and lactic acidosis.
• The parasites also alter the red cell membrane, making it less deformable and resulting in hemolysis and accelerated splenic clearance, which ultimately causes anemia.
• Release of proinflammatory cytokines, • Tumor necrosis factor (TNF)-alpha, is stimulated by red cell lysis, • TNF-alpha suppresses hematopoiesis - anemia.
• The liver and spleen enlarge over time; the latter may become massively enlarged [ 12] .
• Thrombocytopenia is caused by increased splenic sequestration and decreased platelet survival time (ie, hypersplenism).
PATHOGENESIS
Microvascular disease and sequestration
• P. falciparum potential to cause severe or fatal disease. • P falciparum parasites mature within red blood cells,
• P falcifarum induce the formation of sticky knobs - erythrocytes• These knobs bind to receptors on endothelial cells in capillaries
and venules - sequestration of red cells within these small vessels –
obstruction to blood flow.• The cytoadherence and sequestration of red cells within these small
vessels leads to microvascular pathology and obstruction to blood flow.
• Infected red cells also stick to uninfected red cells and form rosettes that clog the microcirculation.
•
• Rosetting is mediated by an interaction between P. falciparum erythrocyte membrane protein 1, which is exposed to the exterior at the knobs on the surface of infected red cells, and receptors on the surface of uninfected red cells, such as complement-receptor 1 (CR1)
• Ultimately, secondary organ dysfunction and severe complications in the host can occur. Of interest, it has been reported that a promoter polymorphism of red cell CR1 leads to CR1 deficiency and decreased red cell rosetting, and is significantly associated with protection from P. falciparum malaria
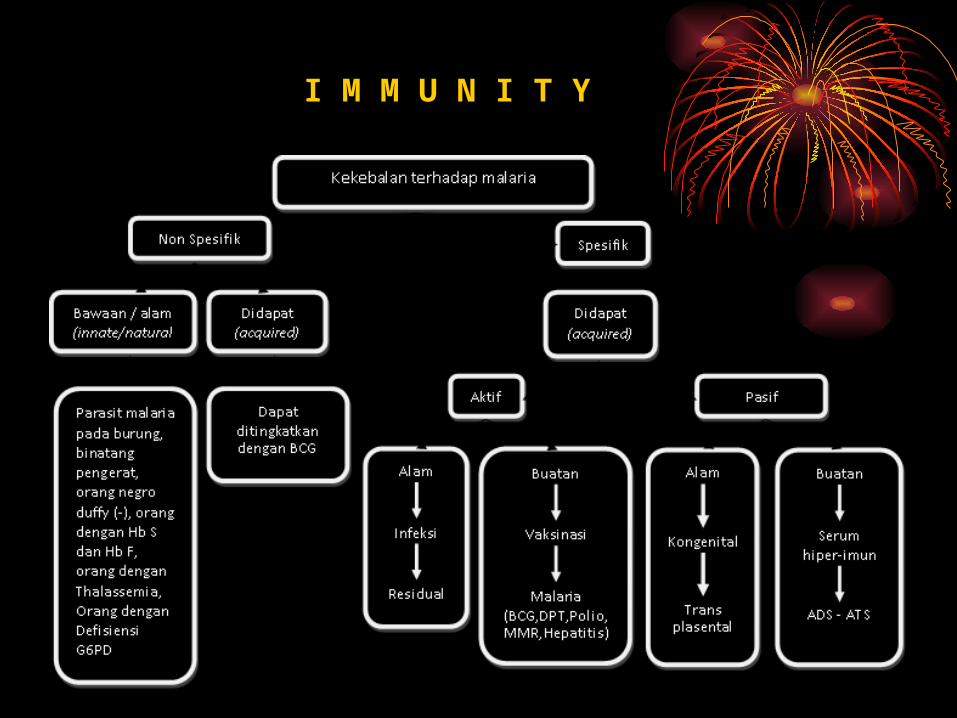
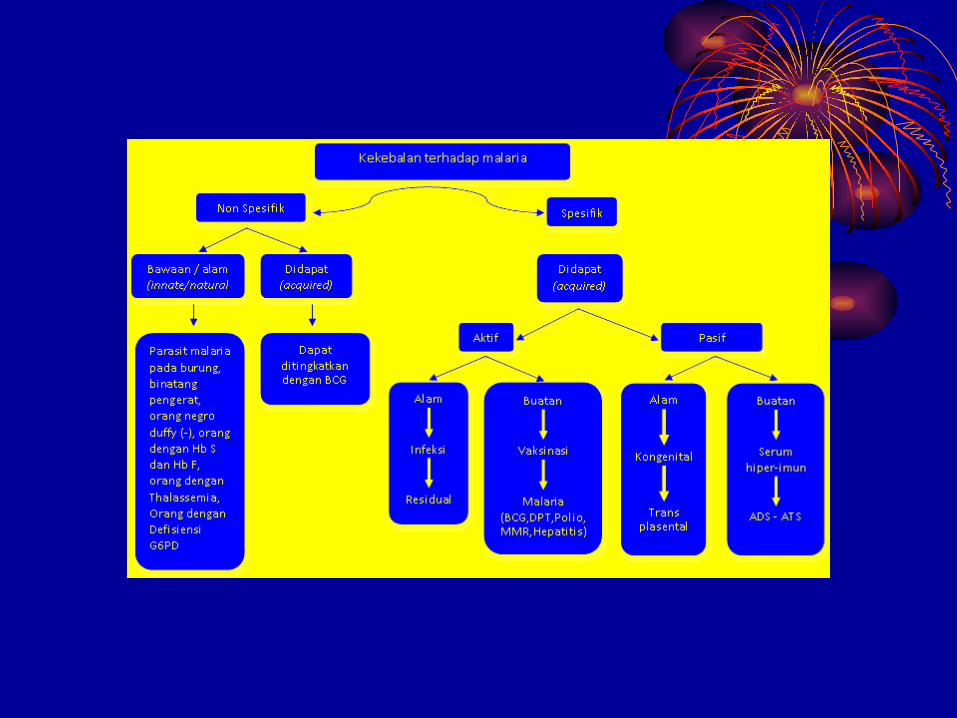
I M M U N I T Y
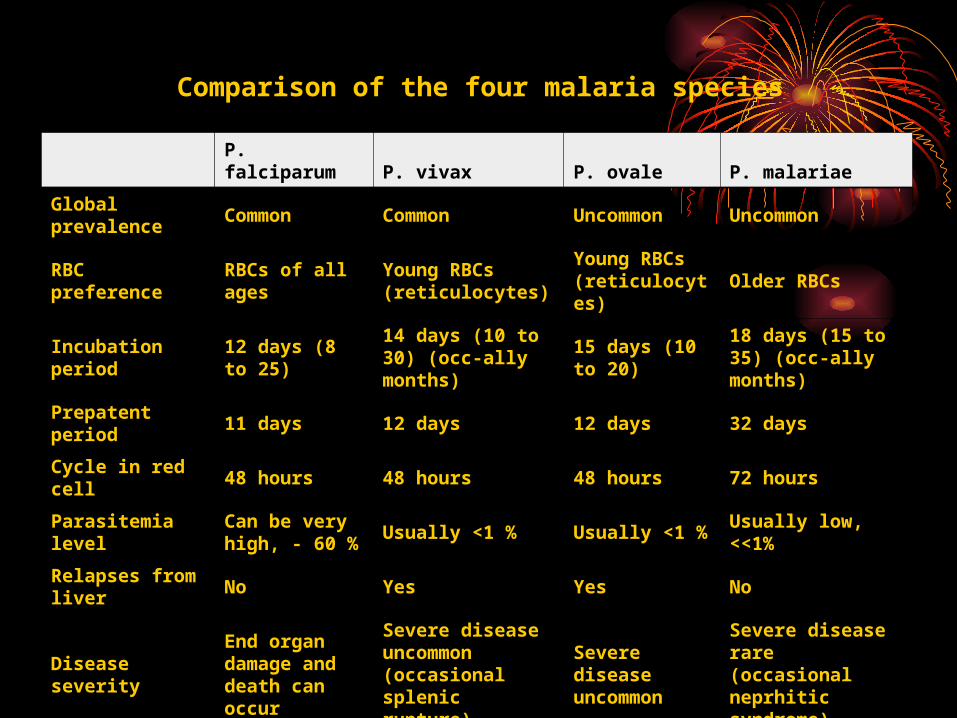
Comparison of the four malaria species
P. falciparum P. vivax P. ovale P. malariae
Global prevalence Common Common Uncommon Uncommon
RBC preference
RBCs of all ages
Young RBCs (reticulocytes)
Young RBCs (reticulocytes)
Older RBCs
Incubation period
12 days (8 to 25)
14 days (10 to 30) (occ-ally months)
15 days (10 to 20)
18 days (15 to 35) (occ-ally months)
Prepatent period 11 days 12 days 12 days 32 days
Cycle in red cell 48 hours 48 hours 48 hours 72 hours
Parasitemia level
Can be very high, - 60 % Usually <1 % Usually <1
%Usually low, <<1%
Relapses from liver No Yes Yes No
Disease severity
End organ damage and death can occur
Severe disease uncommon (occasional splenic rupture)
Severe disease uncommon
Severe disease rare (occasional neprhitic syndrome)
Clinical and laboratory indicators of poor prognosis
• Age <3 years• Deep coma• Convulsions• Papilloedema and/or retinal oedema• Absent corneal reflexes, decerebrate/decorticate rigidity or opisthotonus• Organ dysfunction, respiratory distress or circulatory collapse• Hyperparasitmeia (>250,000/ul or >5 percent)• Peripheral schizonts and/or mature pigmented parasites• Haematocrit <15 percent and/or haemoglobin <5 g/dl
• Peripheral white cell count >12,000/ul• Blood glucose <2.2 mmol/l (<40 g/dl)• Serum urea >60 mg/dl or creatinine >265 umol/l (>3.0 mg/dl)• Venous lactic acid >5 mmol/l• Aminotransferases >3-times normal• High CSF lactic acid (>6 mmol/l) and low CSF glucose• Increased plasma 5'-nucleotidase• Low antithrombin III levels• High plasma TNF concentration
Clinical and laboratory indicators of poor prognosis