dr. pande putu januraga. 2 september pemaparan perkuliahan dan pengantar manajemen kesehatan 9...
TRANSCRIPT
WELCOME, STUDENTS!Dr. Pande Putu Januraga
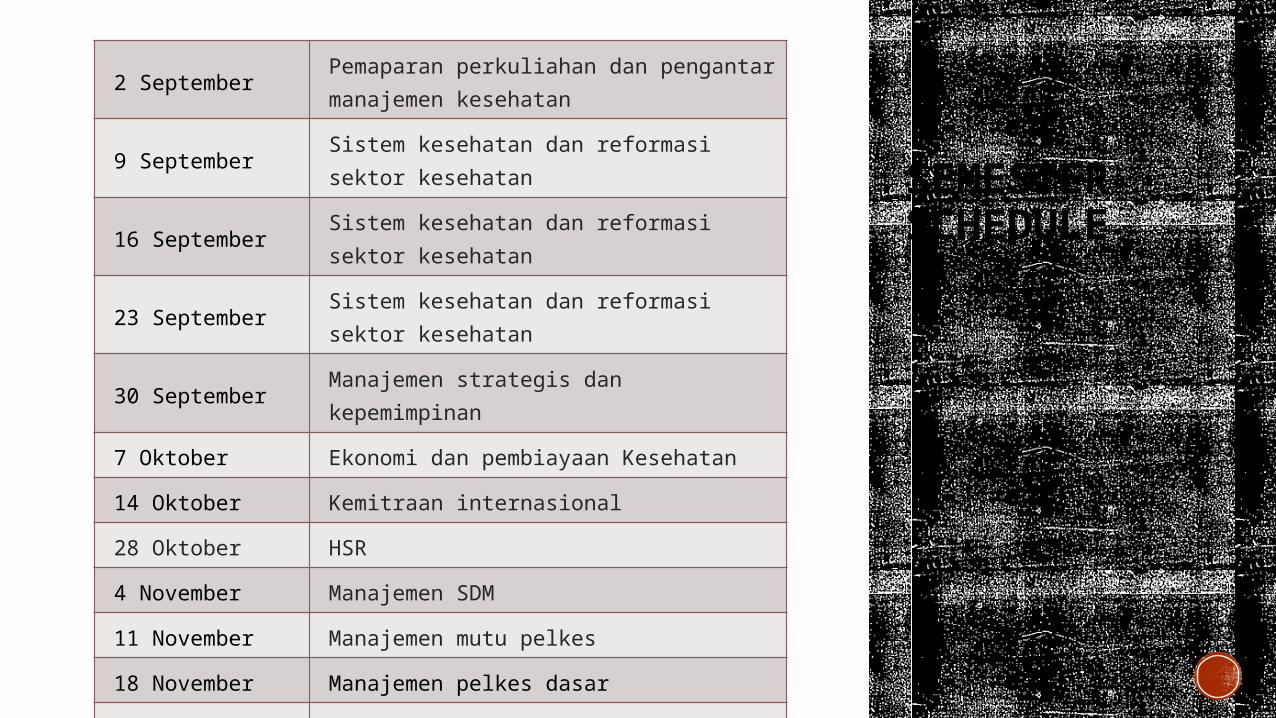
SEMESTER SCHEDULE
2 SeptemberPemaparan perkuliahan dan pengantar manajemen kesehatan
9 September Sistem kesehatan dan reformasi sektor kesehatan
16 September Sistem kesehatan dan reformasi sektor kesehatan
23 September Sistem kesehatan dan reformasi sektor kesehatan
30 September Manajemen strategis dan kepemimpinan
7 Oktober Ekonomi dan pembiayaan Kesehatan
14 Oktober Kemitraan internasional
28 Oktober HSR
4 November Manajemen SDM
11 November Manajemen mutu pelkes
18 November Manajemen pelkes dasar
25 November Manajemen RS
2 Desember Tutorial
9 Desember Tutorial
LEARN ABOUT OUR CLASS
The lecturers?Goals?Assignments?Supplies?Getting help?Questions
Study guide
ASSIGNMENTS UTS (40%)
Telaah kritis artikel jurnal (15%)
Essay (35%)
GET TO KNOW ME
Academic background
Dokter 2003 Universitas Udayana
M.Kes 2008 Universitas Diponogoro
DrPH 2014 Flinders University
RESEARCH EXPERIENCES• 2014-??? Study coordinator for Bali site: HIV-AIDS Test and Treat Indonesia (HATI project)
• 2012-2014 Thesis for DrPH: an exploratory study of social capital among brothels based FSWs in Bali
• 2011 Principal investigator: Evaluation Study of the Strategic Planning of Bali Provincial AIDS Committee
• 2010-2011 Principal investigator: Feasibility Study of Cohort on Risk Factors of HIV on FSWs in Bali; Method for enrolling and retaining participants (FRTP-2010-2011)
• 2009-2010 Principal investigator: Evaluation of HIV surveillance system; a case study of Bali Province’s sero-surveys (FRTP-2009-2010)
• 2009 Principal investigator: Development of Comprehensive Primary-HealthCare-Based services for Female Sex Workers in Bali
• 2008 Quality assessor: Benefit, Monitoring and Evaluation Study of First Decentralized Health Services (DHS-1) Project, Bali Province
• 2007-2008 Thesis for MPH: Cost per Capita and Premium Analysis to Advocate Policy Maker of JKJ; Case Study of Health Financing Program in Jembrana
• 2007 Principal investigator: Physical Risk Factor of Non Communicable Disease in Age Group 25-64 Years at Baha Village, Mengwi Sub District, Badung Regency
• 2005-2006 Co-investigator: Organizations structures of Dinas Kesehatan and Puskesmas; Case Study of Post Decentralization in Bali
• 2004-2005 Co-investigator: Developing Puskesmas (Primary Health Center) by Strategic Management
• 2004 Field coordinator: Survey of basic data Bali provincial health
KEY PUBLICATIONJANURAGA, P. P., MOONEY-SOMERS, J. & WARD, P. 2014. Newcomers in a hazardous environment: a qualitative inquiry into sex worker
vulnerability to HIV in Bali, Indonesia. BMC Public Health, 14, 832.
JANURAGA PP, WULANDARI LPL, MULIAWAN P, et al. (2013) Sharply rising prevalence of HIV infection in Bali: a critical assessment of
the surveillance data. International Journal of STD & AIDS 24: 633-637.
JANURAGA, P.P., INDRAYATHI, P.A., SUARJANA, K. 2010. The Impact Of The Bali Mandara Health Insurance To The Presence Of District
Level Health Insurance In Bali And Achievement Of Universal Coverage. The Indonesian Journal of Health Services Management. June
Edition.
JANURAGA, P. P., SURYAWATI, C., LISTYOWATI, R. & NOPIYANI, M. S. 2010. Cost Per Capita Analysis to Control The Cost Of Jembrana
Health Insurance. The Indonesian Journal of Health Service Management. March edition.
JANURAGA, P. P., SURYAWATI, C. & ARSO, S. P. 2009. Stakeholders Perception toward Background of Premium Subsidy, Capitation
System and Premium Payment of Jembrana Health Insurance. The Indonesian Journal of Health Service Management.
JANURAGA, P. P., SURYAWATI, C. & ARSO, S. P. 2008. Premium Tariff Calculation to Advocate the Reallocation of Premium Subsidy for
PPK I of Jembrana Health Insurance. The Indonesian Journal of Health Service Management, 11.
YESSI, MUNINJAYA, A. A., ANSHORI, Y. & JANURAGA, P. P. 2006. Organizations Structure Variations of Public Health Institutions: Case
Study of Post Decentralization in Bali. The Indonesian Journal of Health Service Management, 09.
HEALTH MANAGEMENTintroduction
To be sure, the fundamental task of management remains the same: to make people capable of joint performance through common goals, common values, the right structures, and the training and development they need to perform and to respond to change. (Drucker 1990)
BASIC MANAGEMENT
Planning
Organising
Actuating
Controlling
MANAGEMENT SKILLS
Defining strategy and goals
Developing people
Measuring performance
Marketing services
Management
MANAGEMENT DIMENSIONS
Culture, value and principle
Structure
TechniqueSetting or
infrastructure
Management
THE CULTUREManagement is about people
Management is about securing commitment to shared values
Management is about developing staff
Management is about achieving results
THE STRUCTURE Close vs open system
Tight about ends and loose about means
THE TECHNIQUES communication skills (consultation, negotiation, and conflict management)
management by objectives
human resource management
economics, finance, and accounting
(strategic) planning and marketing
project management
quality assurance.
THE SETTINGSModel of management
Traditional bureaucracy—with an emphasis on clear structure, hierarchical chains of command, clear accountability for performance
New public management—with an emphasis on making organizations more like firms operating in markets through the introduction of competition to improve performance (Hood 1991)
‘Japanese' organization model or 'clan'—'solidarity' model of organization in which a sense of identity with, and pride in, the organization itself is the main source of motivation
Professionalism—shares the 'Japanese' model's assumption that people work better when they are trusted and their performance is not closely monitored;
The sense of identity is with the profession rather than with the organization, or possibly dual loyalty to both exists.
Management is not a purely technical enterprise. Ideas, culture, and ideologies make a real difference.
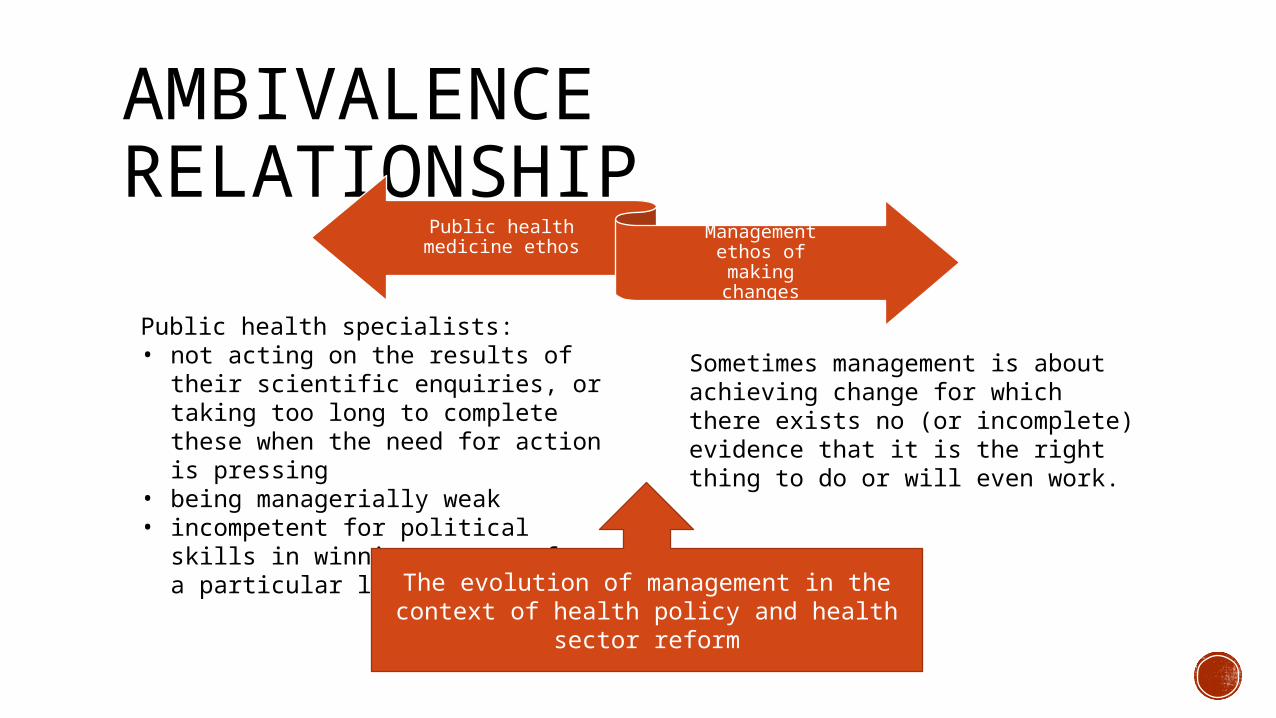
AMBIVALENCE RELATIONSHIP
Public health medicine ethos
Management ethos of making changes
Public health specialists:• not acting on the results of their
scientific enquiries, or taking too long to complete these when the need for action is pressing
• being managerially weak• incompetent for political skills in
winning support for a particular line of action.
Sometimes management is about achieving change for which there exists no (or incomplete) evidence that it is the right thing to do or will even work.
The evolution of management in the context of health policy and health sector
reform
MANAGEMENT IN A HEALTH-CARE CONTEXTKey differences, Shortell and Kaluzny (1983):
defining and measuring output are difficult
the work involved is felt to be more highly variable and complex than in other organizations
more of the work is of an emergency and non-deferrable nature
the work permits little tolerance for ambiguity or error
the work activities are highly interdependent, requiring a high degree of co-ordination among diverse professional groups
the work involves an extremely high degree of specialization
organizational participants are highly professional, and this primary loyalty belongs to the profession rather than to the organization
there exists little effective organizational or managerial control over the group most responsible for generating work and expenditure: clinicians
in many health-care organizations, particularly hospitals, there exist dual lines of authority, which create problems of co-ordination and accountability, and confusion of roles.
NEXT Evolution of theories of management, planning, and organization and to
show how these have impacted upon public management, health system and health-care services.
QUESTIONS?
LET’S HAVE AGREAT SEMESTER!