Download - Drnico Pcc 2014
Dr. Nico A. Lumenta, K.Nefro, MM, MHKes
• Konsep Filosofis Asuhan Pasien• Pelayanan Fokus Pasien / Patient Centered Care• Interprofessionality• Proses Asuhan Pasien, Asuhan Terintegrasi• Case Manager• BPIS
1
CURRICULUM VITAENama : Dr. Nico A. Lumenta, K.Nefro, MM, MHKes
Lahir : Magelang, 5 Nov 1943 Alamat : Jl. Kayu Mas I/4, Pulo Mas,Jkt TimurPendidikan : Dokter, 1970, FK.UKI, Jakarta •Konsultan Nefrologi (Ginjal-Hipertensi) 1982, Pernefri
(Perhimpunan Nefrologi Indonesia)•Magister Manajemen, 1994, Sekolah Tinggi Manajemen PPM,
Jkt.•Magister Hukum Kesehatan, 2013, Unika Soegijapranata,
SemarangJabatan RS : RS Mediros : Ketua Komite Medis, Koordinator
KSM PD.Ginjal-Hipertensi Organisasi:•KARS Kepala Bidang Publikasi & Pemasaran 2014 - 2018•KARS (Komisi Akreditasi Rumah Sakit) Dep Kes RI : Ketua
Bidang Akreditasi 2011-2014, Surveior / Pembimbing Akreditasi sejak 1995
•Member Advisory Council Asia Pacific, Joint Commission International, sejak 2009 2
• Ketua KKP-RS (Komite Keselamatan Pasien Rumah Sakit)-PERSI 2005-2012
• Wakil Ketua Komite (Nasional) Keselamatan Pasien RS 2012-2015
• Ketua IKPRS (Institut Keselamatan Pasien Rumah Sakit) - PERSI 2012-2015
• Pengurus PERSI Pusat, Ketua Kompartemen Akreditasi Nasional, 2012-2015
• PJ SubPokja Model Akreditasi Baru, Pokja Penyempurnaan Akreditasi RS, DitJen Bina Yan Med, 2010-2011
Penghargaan: Kadarman Award 2007 (untuk Patient Safety), Sekolah Tinggi
Manajemen PPM
Lain-lain :
• Sekretaris Jendral PERSI Pusat 1988–1990, 1990–1993, 1993–1996
• Direktur Ketua RS.PGI.Cikini, Jakarta, 1983 – 1993
• Dekan Fakultas Kedokteran UKI, 1988 – 1991
• Kepala Bagian Ilmu Penyakit Dalam FK-UKI, Jakarta, 1992 - 1995
• Kepala Renal Unit (Unit Ginjal) RS.PGI Cikini, 1973 – 1981 3
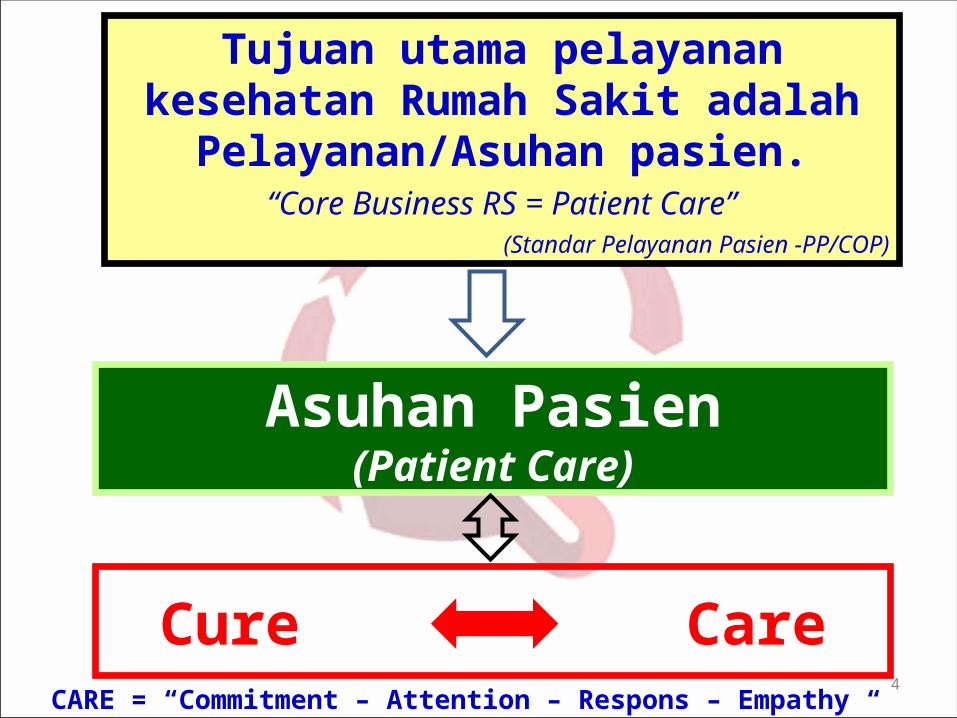
Tujuan utama pelayanan kesehatan Rumah Sakit adalah Pelayanan/Asuhan pasien.
“Core Business RS = Patient Care”(Standar Pelayanan Pasien -PP/COP)
Asuhan Pasien(Patient Care)
Cure CareCARE = “Commitment – Attention – Respons – Empathy “
4
Dalam konteksAsuhan Pasien Asuhan Pasien
(Patient Care)(Patient Care)
PCC merupakan induk dari Standar Akreditasi Rumah Sakit
v. 2012
!
5
6
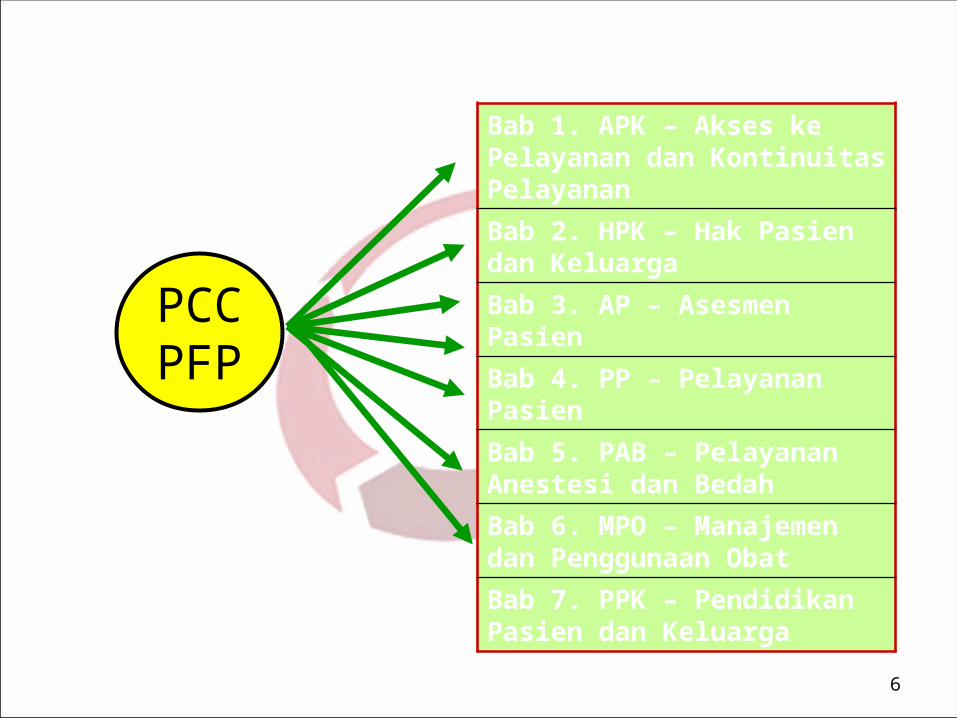
Bab 1. APK – Akses ke Pelayanan dan Kontinuitas Pelayanan
Bab 2. HPK – Hak Pasien dan Keluarga
Bab 3. AP – Asesmen Pasien
Bab 4. PP – Pelayanan Pasien
Bab 5. PAB – Pelayanan Anestesi dan Bedah
Bab 6. MPO – Manajemen dan Penggunaan Obat
Bab 7. PPK – Pendidikan Pasien dan Keluarga
PCCPFP
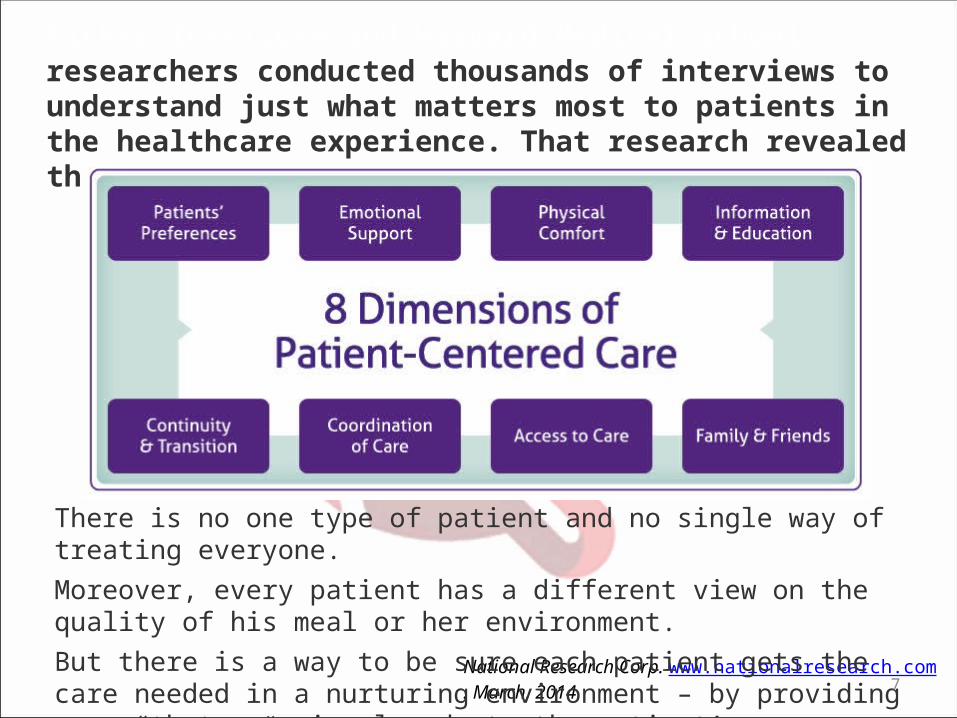
Picker Institute and Harvard Medical School researchers conducted thousands of interviews to understand just what matters most to patients in the healthcare experience. That research revealed the Eight Dimensions of Patient-Centered Care
National Research Corp. www.nationalresearch.com. March, 2014
There is no one type of patient and no single way of treating everyone.Moreover, every patient has a different view on the quality of his meal or her environment.But there is a way to be sure each patient gets the care needed in a nurturing environment – by providing care “that consciously adopts the patient’s perspective.”
7
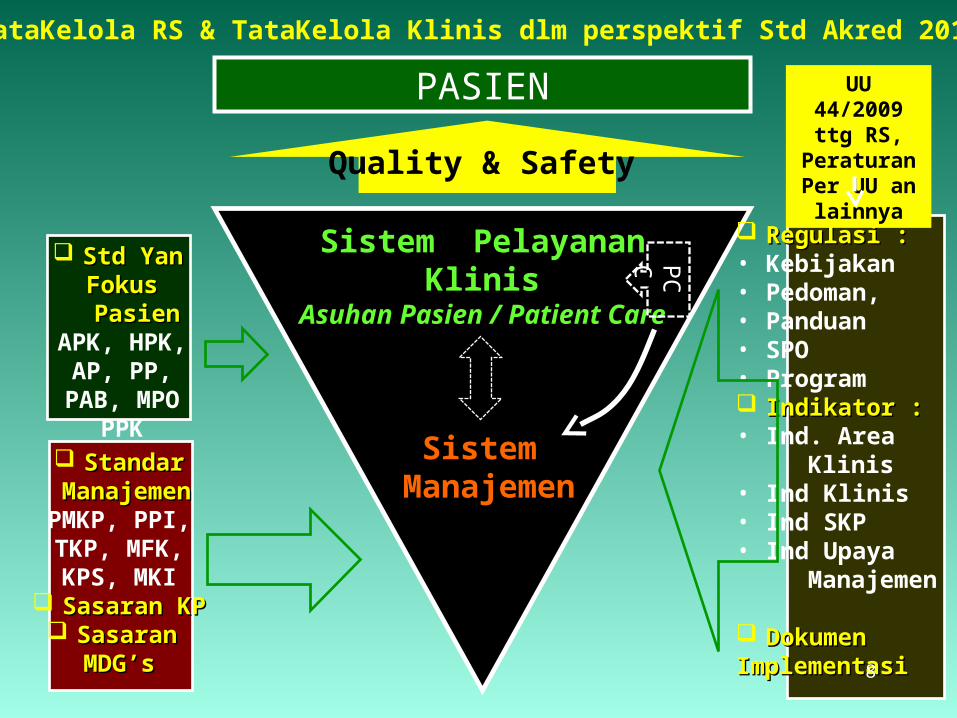
Sistem Manajemen
Sistem Pelayanan Klinis
Asuhan Pasien / Patient Care
Quality & Safety
PASIEN
StandarStandar ManajemenManajemenPMKP, PPI,TKP, MFK,KPS, MKI
Sasaran KPSasaran KP Sasaran Sasaran
MDG’sMDG’s
Std Yan Std Yan Fokus PasienFokus Pasien
APK, HPK,AP, PP,
PAB, MPOPPK
Regulasi :Regulasi :• Kebijakan• Pedoman,• Panduan• SPO• Program Indikator :Indikator :• Ind. Area Klinis• Ind Klinis• Ind SKP• Ind Upaya Manajemen
DokumenDokumenImplementasiImplementasi
TataKelola RS & TataKelola Klinis dlm perspektif Std Akred 2012
UU 44/2009 ttg RS, Peraturan
Per UU an lainnya
PC
C
8
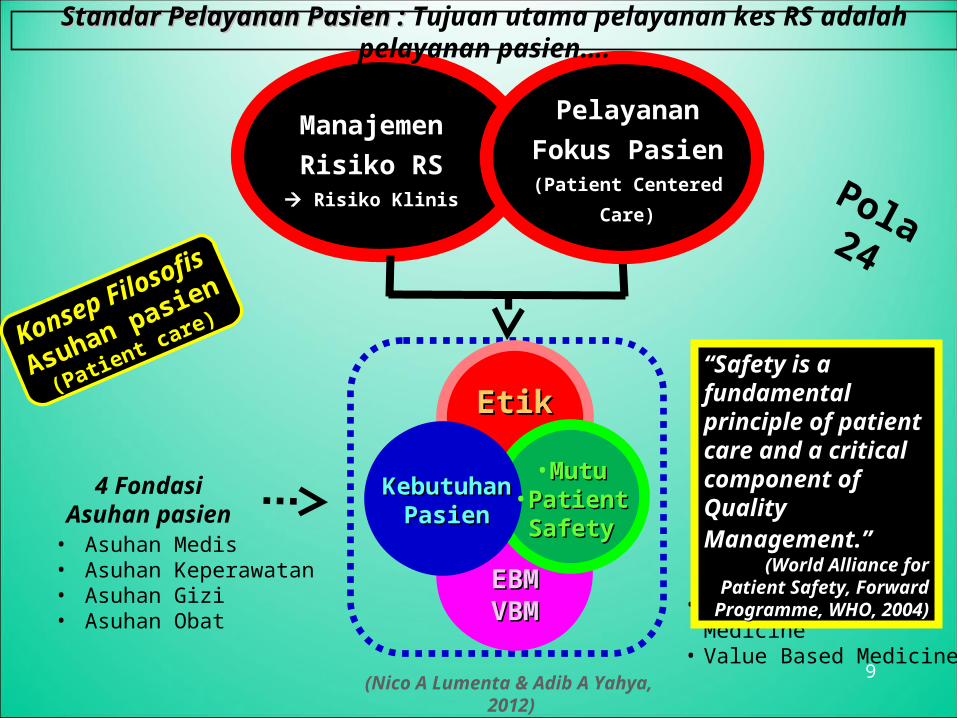
4 FondasiAsuhan pasien
Pelayanan
Fokus Pasien(Patient Centered(Patient Centered
Care)Care)
Manajemen
Risiko RS Risiko KlinisRisiko Klinis
• Asuhan Medis• Asuhan Keperawatan• Asuhan Gizi• Asuhan Obat
• Evidence Based Medicine
• Value Based Medicine
(Nico A Lumenta & Adib A Yahya, 2012)
Standar Pelayanan Pasien : Standar Pelayanan Pasien : Tujuan utama pelayanan kes RS adalah pelayanan pasien….
Konsep
Konsep FilosofiFilosofiss
Asuhan pasien
Asuhan pasien
(Patient care)
(Patient care)
EBMEBMVBMVBM
EtikEtik
KebutuhanKebutuhanPasienPasien
• MutuMutu• PatientPatientSafetySafety
Pola24
““Safety is a Safety is a fundamental principle fundamental principle of patient care and a of patient care and a critical component of critical component of Quality Management.” Quality Management.”
(World Alliance for Patient (World Alliance for Patient Safety, Forward Programme, Safety, Forward Programme,
WHO, 2004)WHO, 2004)
9
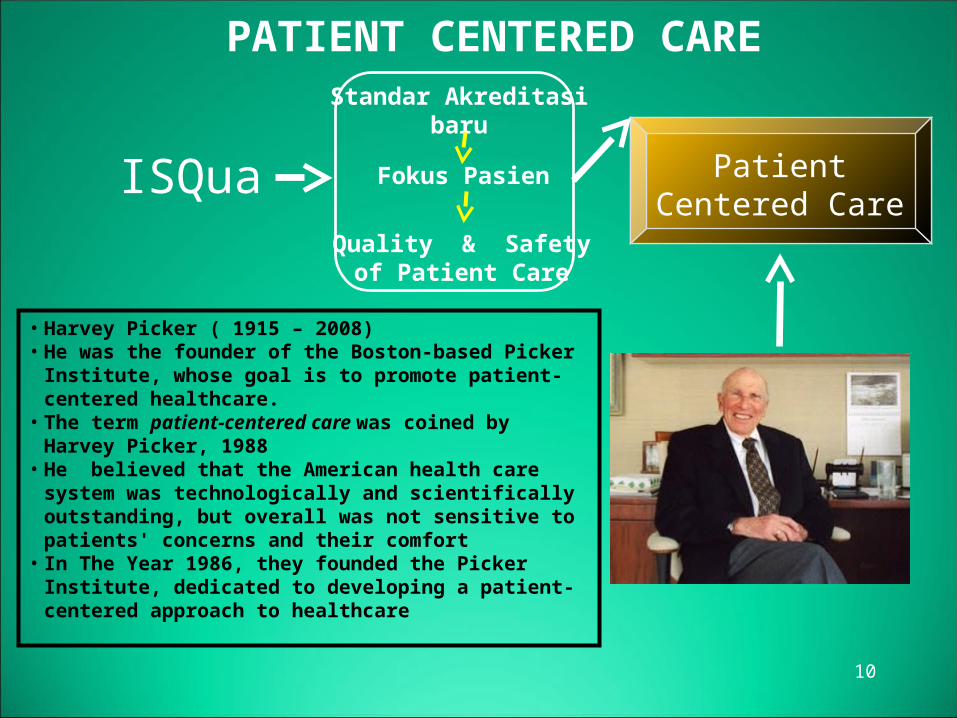
PATIENT CENTERED CARE
• Harvey Picker ( 1915 – 2008)• He was the founder of the Boston-based Picker Institute,
whose goal is to promote patient-centered healthcare.• The term patient-centered care was coined by Harvey
Picker, 1988• He believed that the American health care system was
technologically and scientifically outstanding, but overall was not sensitive to patients' concerns and their comfort
• In The Year 1986, they founded the Picker Institute, dedicated to developing a patient-centered approach to healthcare
Standar Akreditasibaru
Fokus Pasien
Quality & Safetyof Patient Care
ISQua PatientCentered Care
10
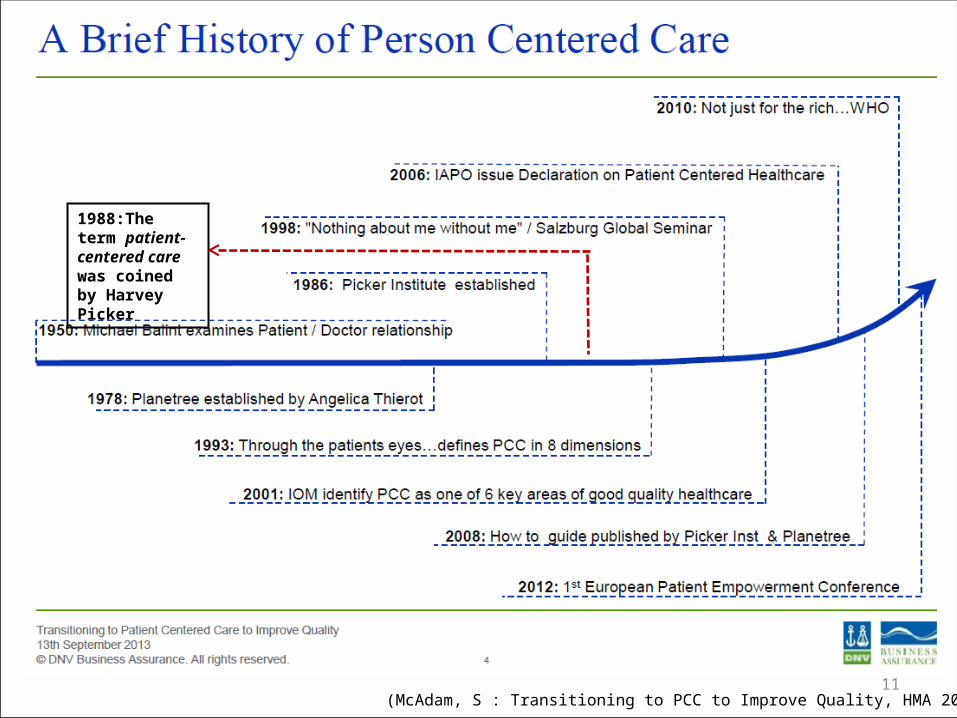
(McAdam, S : Transitioning to PCC to Improve Quality, HMA 2013, Bangkok)
1988:The term patient-centered care was coined by Harvey Picker
11
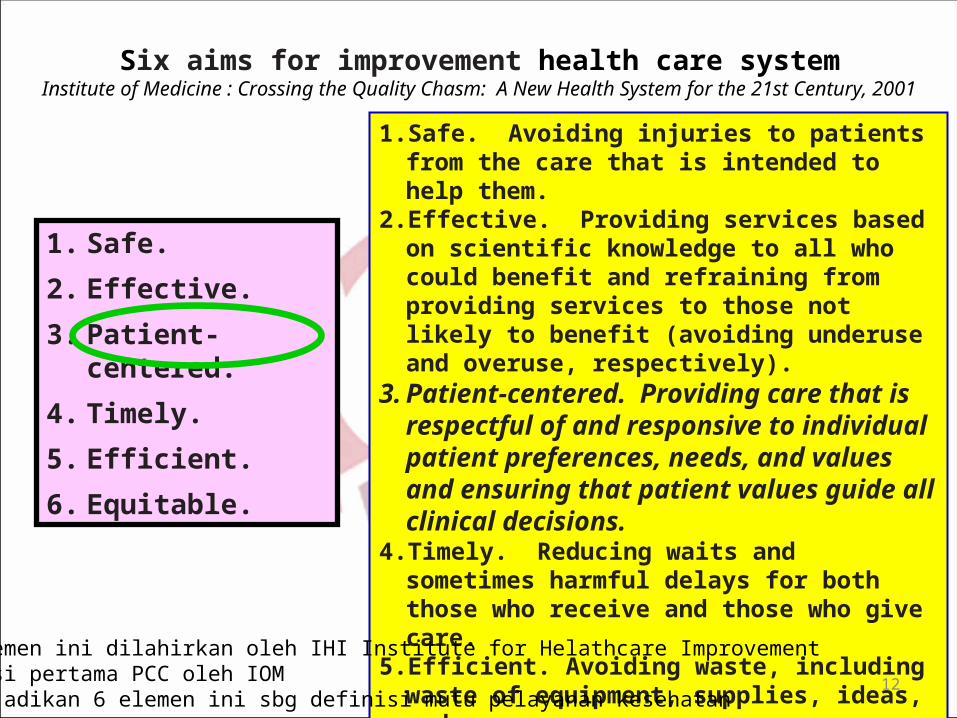
Six aims for improvement health care systemInstitute of Medicine : Crossing the Quality Chasm: A New Health System for the 21st Century,
2001
1. Safe.
2. Effective.
3. Patient-centered.
4. Timely.
5. Efficient.
6. Equitable.
1. Safe. Avoiding injuries to patients from the care that is intended to help them.
2. Effective. Providing services based on scientific knowledge to all who could benefit and refraining from providing services to those not likely to benefit (avoiding underuse and overuse, respectively).
3. Patient-centered. Providing care that is respectful of and responsive to individual patient preferences, needs, and values and ensuring that patient values guide all clinical decisions.
4. Timely. Reducing waits and sometimes harmful delays for both those who receive and those who give care.
5. Efficient. Avoiding waste, including waste of equipment, supplies, ideas, and energy.
6. Equitable. Providing care that does not vary in quality because of personal characteristics such as gender, ethnicity, geographic location, & socioeconomic status.
• Enam elemen ini dilahirkan oleh IHI Institute for Helathcare Improvement• Publikasi pertama PCC oleh IOM• WHO menjadikan 6 elemen ini sbg definisi mutu pelayanan kesehatan
12

MANAJEMEN RISIKOMANAJEMEN RISIKORUMAH SAKITRUMAH SAKIT
13
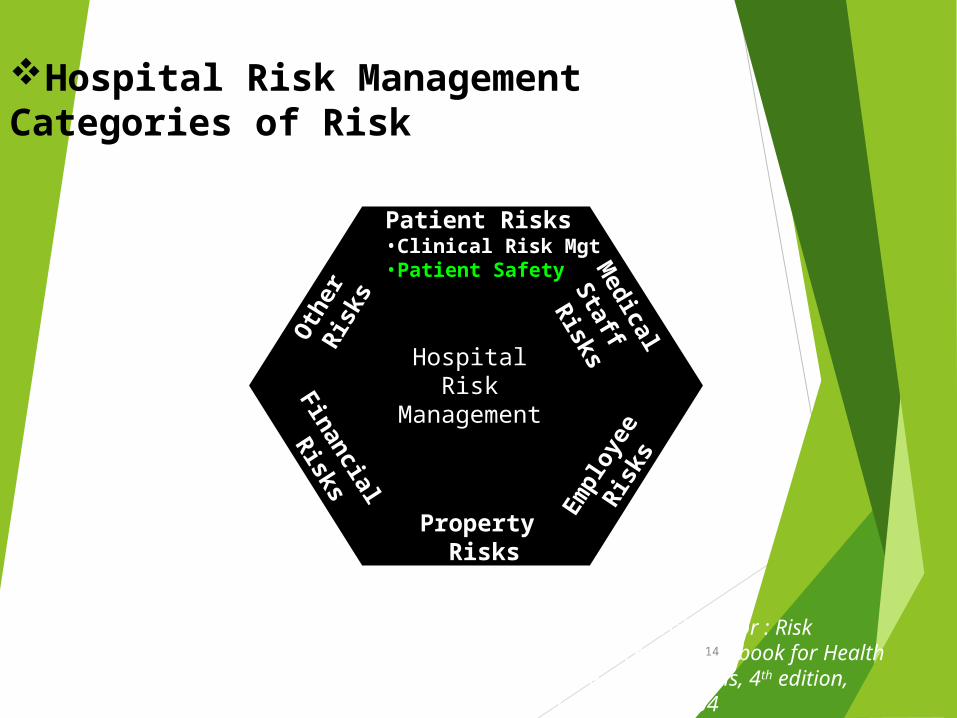
Roberta Caroll, editor : Risk Management Handbook for Health Care Organizations, 4th edition, Jossey Bass, 2004
HospitalRisk
Management
Patient Risks•Clinical Risk Mgt•Patient Safety M
edical
Staff
Risks
Finan
cial
Risks
Property Risks
Oth
er
Ris
ks
Emplo
yee
Ris
ks
Hospital Risk Management Categories of Risk
14
Kategori Risiko di Rumah Sakit
( Categories of Risk )
1. Patient care-related risks
2. Medical staff-related risks
3. Employee-related risks
4. Property-related risks
5. Financial risks
6. Other risks
Roberta Caroll, editor : Risk Management Handbook for Health Care Organizations, 4th edition, Jossey Bass, 2004
15

HospitalSafety
ofThe
Patient ofThe
Health CareWorker
of The
Facilities
of The
Environment
ofThe
Business
Scope of Hospital Risk Management (revised) :
16
1717
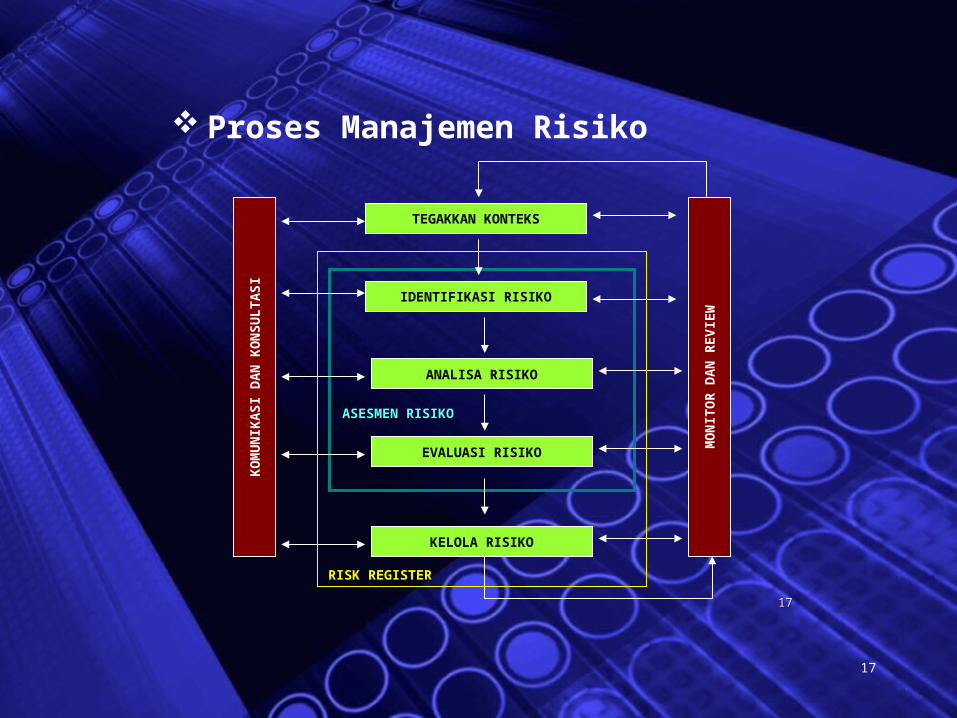
Proses Manajemen Risiko
KO
MU
NIK
AS
I DA
N K
ON
SU
LT
AS
I
MO
NIT
OR
DA
N R
EV
IEW
TEGAKKAN KONTEKS
IDENTIFIKASI RISIKO
ANALISA RISIKO
EVALUASI RISIKO
KELOLA RISIKO
ASESMEN RISIKOASESMEN RISIKO
RISK REGISTERRISK REGISTER
17
PATIENTPATIENT--CENTREDCENTREDCARECARE
(PELAYANAN(PELAYANAN FOKUSFOKUS PASIEN)PASIEN)
“BPIS”
18
Patient-Centered Care
IOM – Institute of Medicine
Patient-centered care as “care that is respectful of and
responsive to individual patient preferences, needs and values,
and ensuring that patient values guide all clinical decisions.”
‘Patient-centered care’ sebagai “asuhan yang menghormati dan
responsif terhadap pilihan, kebutuhan dan nilai-nilai pribadi
pasien. Serta memastikan bahwa nilai-nilai pasien menjadi
panduan bagi semua keputusan klinis”
Definisi
19
Picker Institute :
1.Respect for patients‘ values, preferences and expressed needs
2.Coordination and integration of care3.Information communication and education4.Physical comfort5.Emotional support and alleviation of fear and anxiety6. Involvement of family and friends7.Continuity of care and smooth transition8.Access to Care
1. Hormati nilai2, pilihan dan kebutuhan yg diutarakan oleh pasien2. Koordinasi dan integrasi asuhan3. Informasi, komunikasi dan edukasi4. Kenyamanan fisik5. Dukungan emosional dan penurunan rasa takut & kecemasan6. Keterlibatan keluarga & teman27. Asuhan yg berkelanjutan dan transisi yg lancar8. Akses thd pelayanan. 20
Asuhan Pasien
Model Traditional
Asuhan Pasien
ModelPatient Centered
Care21
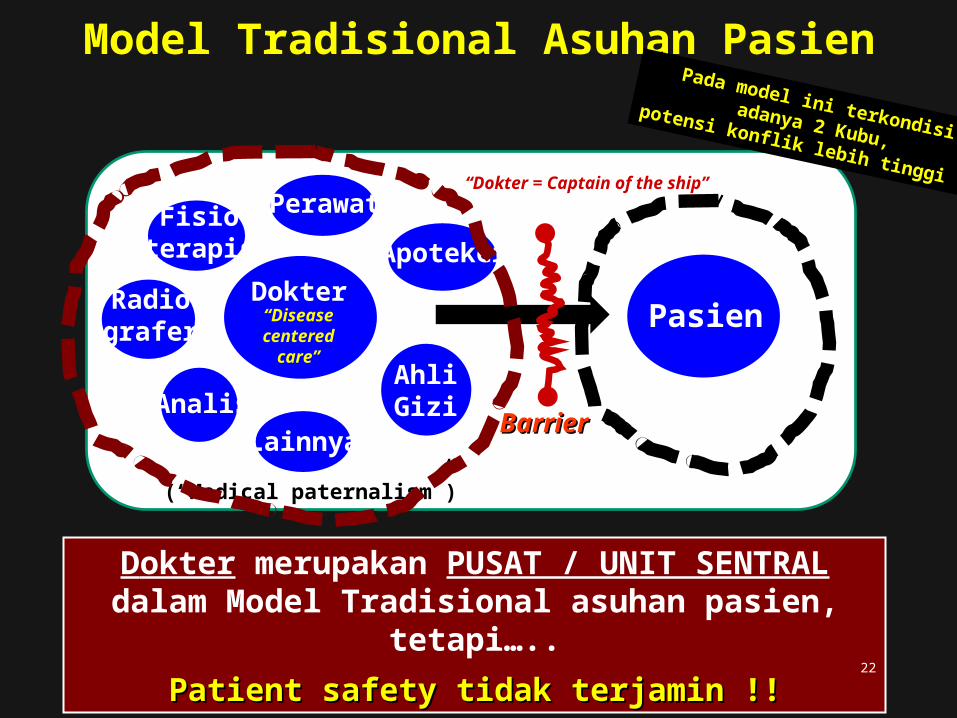
Dokter
Perawat
ApotekerFisio
terapis
AhliGizi
Lainnya
Radiografer Pasien
Dokter merupakan PUSAT / UNIT SENTRAL dalam Model Tradisional asuhan pasien, tetapi…..
Patient safety tidak terjamin !!Patient safety tidak terjamin !!
“Dokter = Captain of the ship”
Model Tradisional Asuhan Pasien
AnalisBarrierBarrier
“Diseasecentered
care”
(“Medical paternalism”)
Pada model ini terkondisi adanya 2 Kubu,
potensi konflik lebih tinggi !!
22
(Kohn LT, Corrigan JM, Donaldson MS, eds. To err is human: buildinga safer health system. Washington, D.C.: National Academy Press, 2000.)
LaporanLaporanInstitute of Medicine – IOMInstitute of Medicine – IOM
TO ERR IS HUMANTO ERR IS HUMANBuilding a Safer Health Building a Safer Health
System System
““Wake-up Wake-up Call”Call”…….bagi dunia pelayanan kesehatan…….
Patient s
afety
Patient s
afety
tidak te
rjamin !!
tidak te
rjamin !!
23
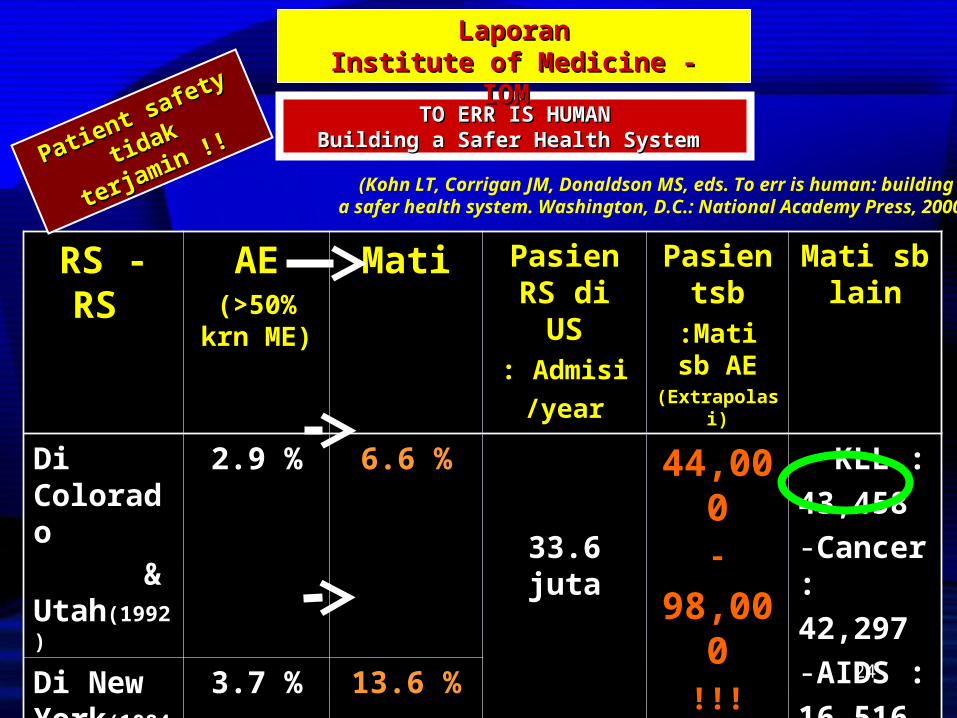
(Kohn LT, Corrigan JM, Donaldson MS, eds. To err is human: buildinga safer health system. Washington, D.C.: National Academy Press, 2000.)
RS - RS AE(>50% krn
ME)
Mati Pasien RS di US: Admisi
/year
Pasien tsb
:Mati sb AE
(Extrapolasi)
Mati sb lain
Di Colorado & Utah(1992)
2.9 % 6.6 %
33.6 juta
44,000-
98,000!!!
Estimasi biaya: $17 - $50 milyar
- KLL :
43,458
-Cancer :
42,297
-AIDS :
16,516Di New York(1984)
3.7 % 13.6 %
TO ERR IS HUMANTO ERR IS HUMANBuilding a Safer Health System Building a Safer Health System
LaporanLaporanInstitute of Medicine - IOM Institute of Medicine - IOM
Patient safety
Patient safety
tidak te
rjamin !!
tidak te
rjamin !!
24
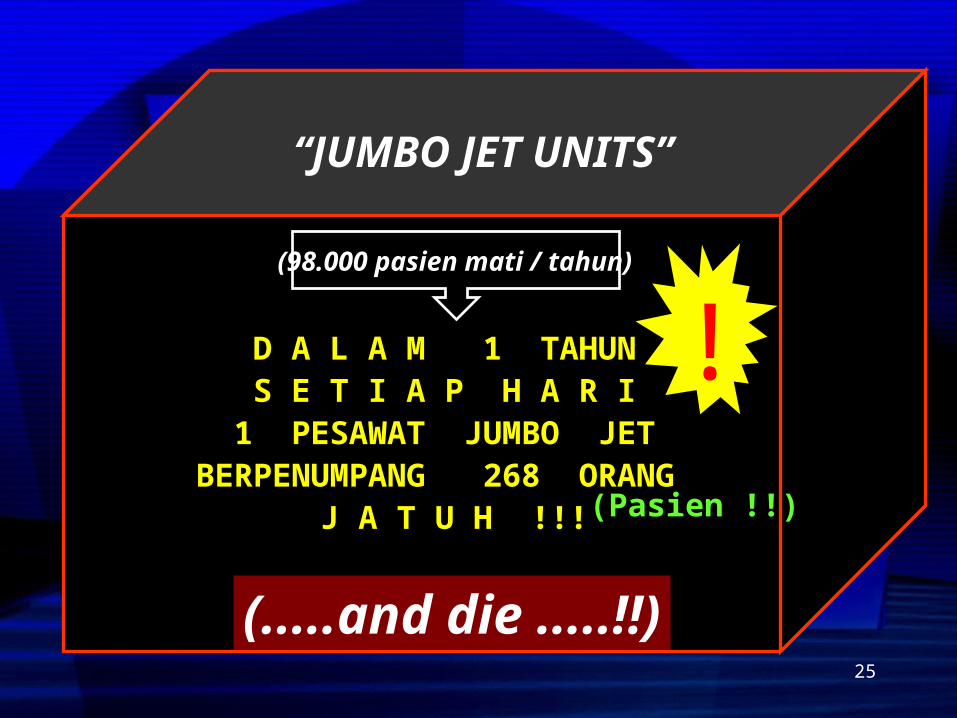
(98.000 pasien mati / tahun)
“JUMBO JET UNITS”
D A L A M 1 TAHUN S E T I A P H A R I
1 PESAWAT JUMBO JET BERPENUMPANG 268 ORANG
J A T U H !!!
(.....and die .....!!)
(Pasien !!)
!
25
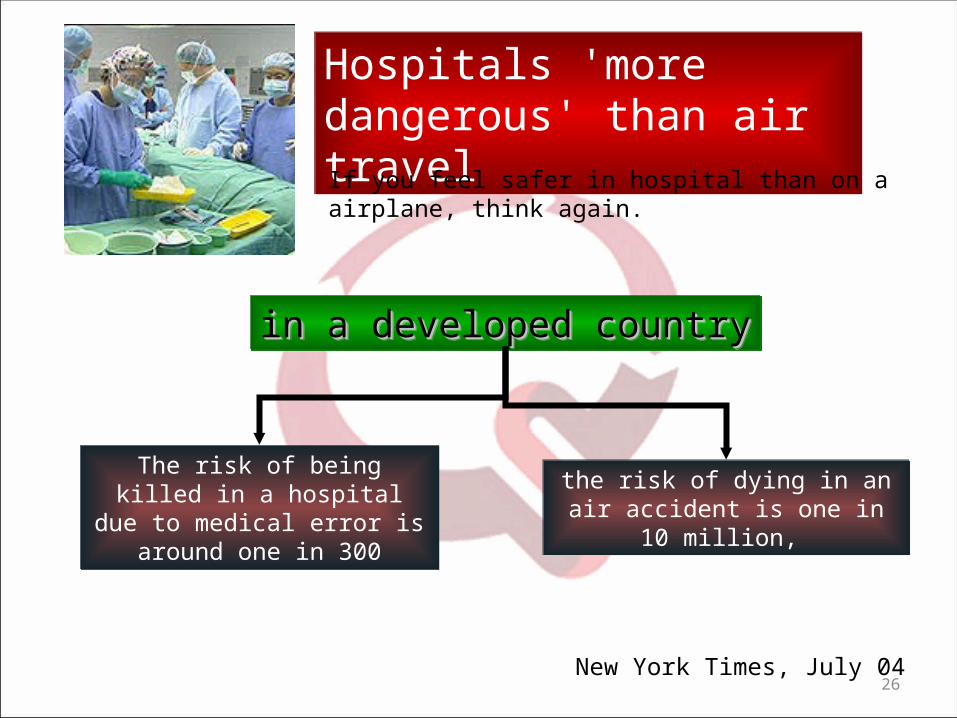
The risk of being killed in a hospital due to medical
error is around one in 300
The risk of being killed in a hospital due to medical
error is around one in 300
Hospitals 'more dangerous' than air travel
Hospitals 'more dangerous' than air travelIf you feel safer in hospital than on a airplane, think again.
in a developed countryin a developed countryin a developed countryin a developed country
the risk of dying in an air accident is one in 10 million,
the risk of dying in an air accident is one in 10 million,
New York Times, July 0426
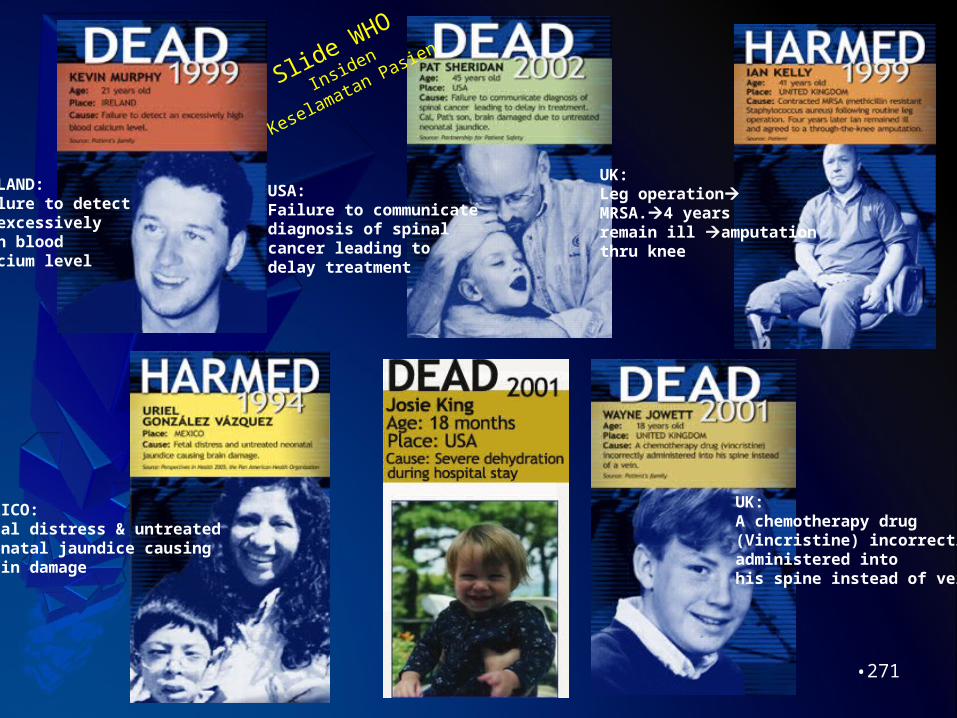
IRELAND:Failure to detect an excessivelyhigh blood calcium level
USA:Failure to communicate diagnosis of spinal cancer leading to delay treatment
MEXICO:Fetal distress & untreated neonatal jaundice causing brain damage
UK:A chemotherapy drug (Vincristine) incorrectly administered into his spine instead of vein
UK:Leg operationMRSA.4 years remain ill amputation thru knee
Slide WHO
Insiden
Keselamatan Pasien
•271
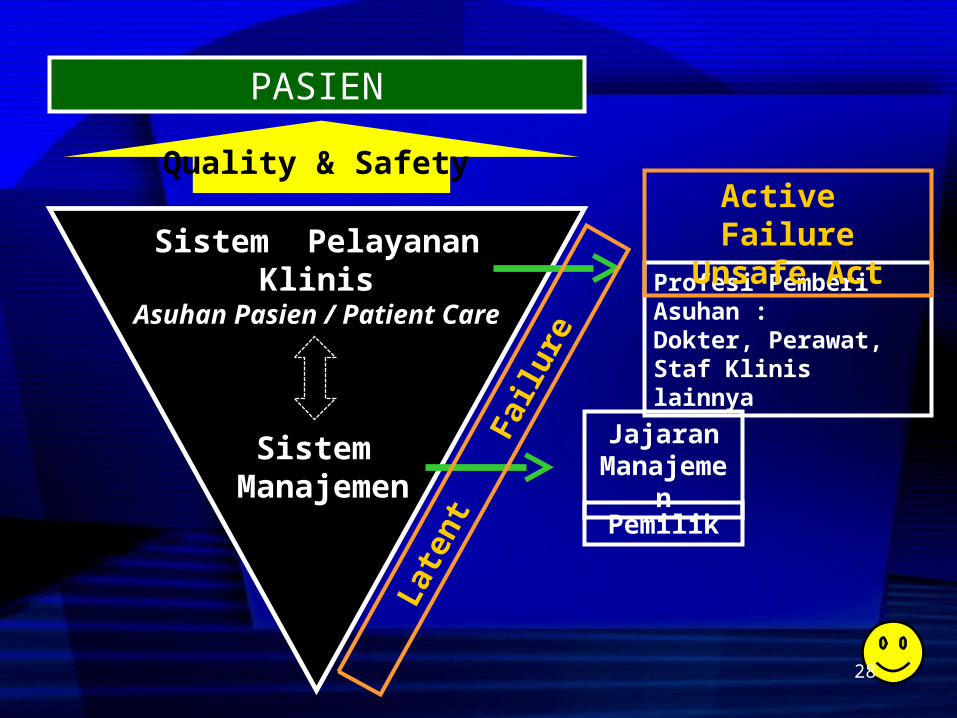
Sistem Manajemen
Sistem Pelayanan Klinis
Asuhan Pasien / Patient Care
Quality & Safety
PASIEN
Profesi Pemberi Asuhan :Dokter, Perawat, Staf Klinis lainnya
Jajaran Manajemen
Late
nt
Fai
lure
Active FailureUnsafe Act
Pemilik
28
Asuhan Pasien
Model Traditional
Asuhan Pasien
ModelPatient Centered
Care29
Pasien,Keluarga
Fisioterapis
Perawat Apoteker
AhliGizi
AnalisRadiografer
DPJP
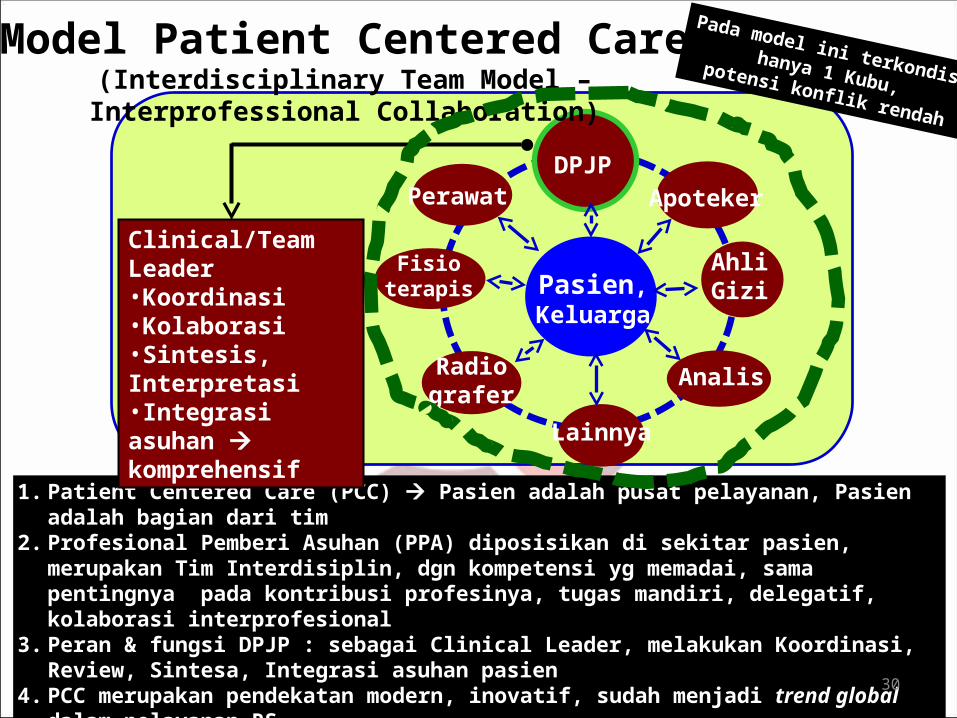
Model Patient Centered Care(Interdisciplinary Team Model – Interprofessional Collaboration)
Lainnya
1. Patient Centered Care (PCC) Pasien adalah pusat pelayanan, Pasien adalah bagian dari tim
2. Profesional Pemberi Asuhan (PPA) diposisikan di sekitar pasien, merupakan Tim Interdisiplin, dgn kompetensi yg memadai, sama pentingnya pada kontribusi profesinya, tugas mandiri, delegatif, kolaborasi interprofesional
3. Peran & fungsi DPJP : sebagai Clinical Leader, melakukan Koordinasi, Review, Sintesa, Integrasi asuhan pasien
4. PCC merupakan pendekatan modern, inovatif, sudah menjadi trend global dalam pelayanan RS
Pada model ini terkondisi hanya 1 Kubu,
potensi konflik rendah
Clinical/Team Leader•Koordinasi•Kolaborasi•Sintesis, Interpretasi•Integrasi asuhan komprehensif
30
1. Dignity and Respect. Health care practitioners listen to and honor patient and family perspectives and choices. Patient and family knowledge, values, beliefs and cultural backgrounds are incorporated into the planning and delivery of care.
2. Information Sharing. Health care practitioners communicate and share complete and unbiased information with patients and families in ways that are affirming and useful. Patients and families receive timely, complete, and accurate information in order to effectively participate in care and decision-making.
3. Participation. Patients and families are encouraged and supported in participating in care and decision-making at the level they choose.
4. Collaboration. Patients and families are also included on an institution-wide basis. Health care leaders collaborate with patients and families in policy and program development, implementation, and evaluation; in health care facility design; and in professional education, as well as in the delivery of care.
What are the Core Concepts of Patient Centered Care?
Partnering with Patients and Families to Design a Patient and Family-Centered Health Care System.Johnson, B et al. Institute for Family-Centered Care 2008
Sisi
Pasien
31
1. Martabat dan Respek. • Profesional Pemberi Asuhan mendengarkan, menghormati &
menghargai pandangan serta pilihan pasien & keluarga. • Pengetahuan, nilai-nilai, kepercayaan, latar belakang kultural
pasien & keluarga dimasukkan dlm perencanaan pelayanan dan pemberian pelayanan kesehatan
2. Berbagi informasi. • Profesional Pemberi Asuhan mengkomunikasikan dan berbagi
informasi secara lengkap pasien & keluarga. • Pasien & keluarga menerima informasi tepat waktu, lengkap, dan
akurat• Asesmen : metode, substansi / kebutuhan edukasi, konfirmasi
3. Partisipasi. • Pasien & keluarga didorong dan didukung utk berpartisipasi dlm
asuhan dan pengambilan keputusan / pilihan mereka
4. Kolaborasi / kerjasama. • Pimpinan pelayanan kesehatan bekerjasama dgn pasien &
keluarga dalam pengembangan, implementasi dan evaluasi kebijakan dan program; Partnering with Patients and Families to Design a Patient and Family-Centered Health Care System.
Johnson, B et al. Institute for Family-Centered Care 2008
What are the Core Concepts of Patient Centered Care?Sisi
Pasien
32
1. Interdisciplinary Team • Profesional Pemberi Asuhan diposisikan mengelilingi pasien• Kompetensi yang memadai • Berkontribusi setara dalam fungsi profesinya• Tugas mandiri, kolaboratif, delegatif, bekerja sebagai satu kesatuan
memberikan asuhan yang terintegrasi2. Interprofessionality
• Interprofessional Collaboration• Interprofessional Education• Interprofessional Collaborative Practice Competency
3. DPJP adalah Clinical Leader. • DPJP melakukan koordinasi, sintesis, review dan mengintegrasikan
asuhan pasien4. Personalized Care & BPIS (Bila Pasien Itu Saya)
• Keputusan klinis selalu diproses berdasarkan juga nilai-nilai pasien• Setiap Dr memperlakukan pasiennya sebagaimana ia sendiri ingin
diperlakukan(Sintesis berbagai refernsi, 2014)
Core Concepts of Patient Centered CareSisi
Profesional
Pemberi Asuhan
33

Patient- and family-centered care is a change in thinking • from serving patients and families • to partnering with patients and families.
•And that’s a very big difference !!Senior Vice President, Patient and Family Centered Care, MCG Health System
(Strategies for Leadership, ADVANCING THE PRACTICE OF Patient- and Family-Centered Care, A Resource Guide for Hospital S enior Leaders, Medical Staff and Governing Boards.
American Hospital Association and Institute for Family Centered Care, 2004)
34
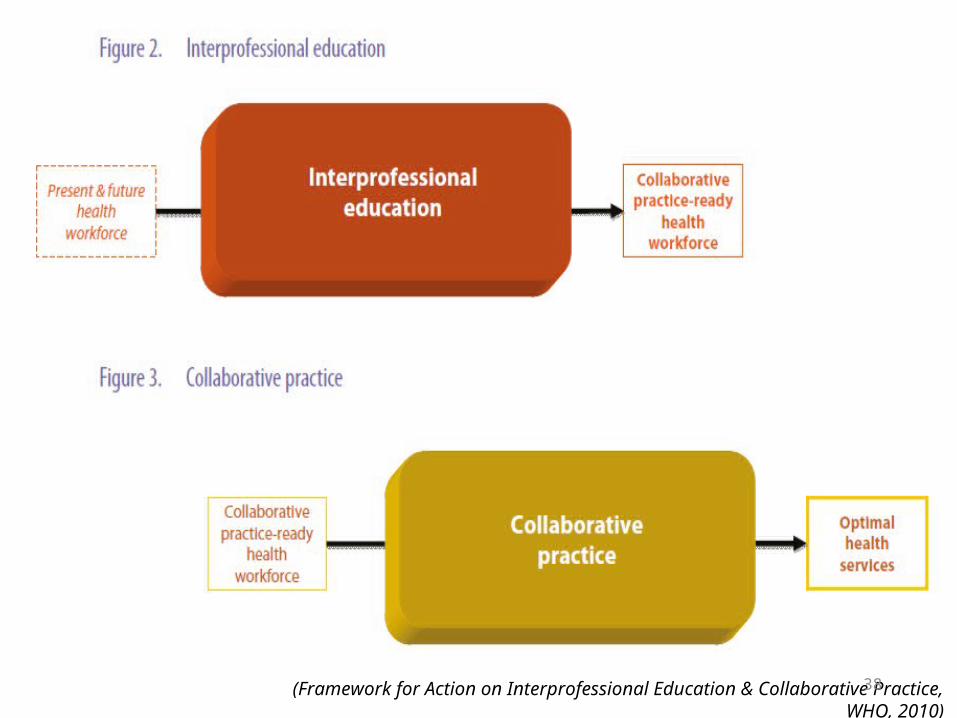
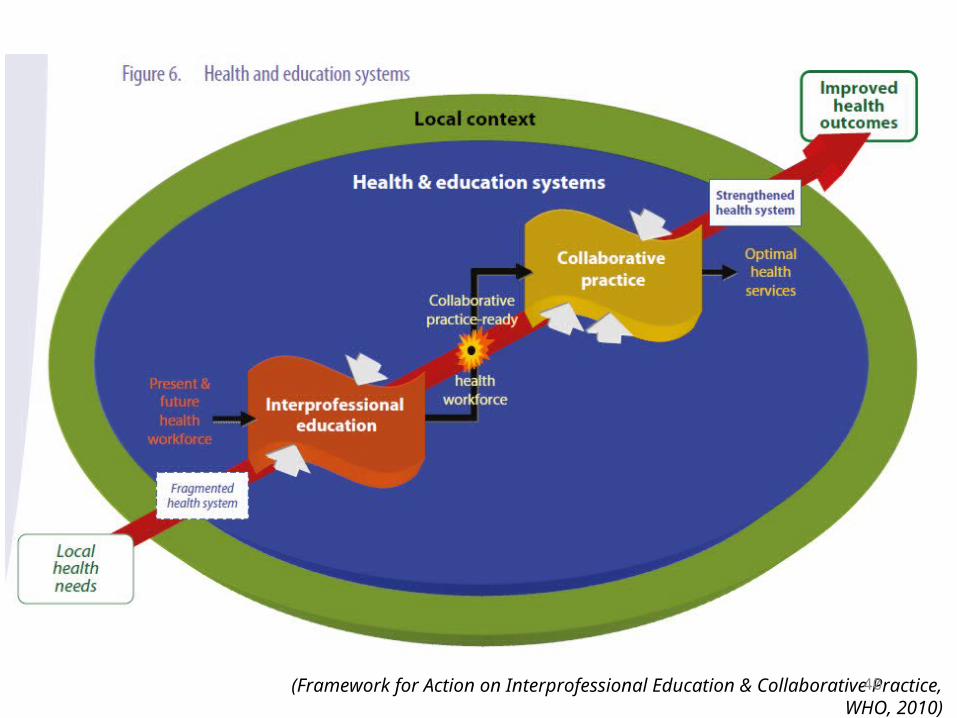
Interprofessional Collaboration (IPC)When multiple health workers from different professional backgrounds work together with patients, families, carers, and communities to deliver the highest quality of care
Interprofessionality
Interprofessional Education (IPE)When students from two or more professions learn about, from and with each other to enable effective collaboration and improve health outcomes
The World Health Organization recognizes interprofessional collaboration in education and practice as an innovative strategy that will play an important role in mitigating the global health crisis.
We know that interprofessional collaboration is key to providing the best in patient care.
(Framework for Action on Interprofessional Education & Collaborative Practice, WHO, 2010)
Sisi Prof. Pemberi
Asuhan
35
STANDAR KOMPETENSI DOKTER INDONESIA
Konsil Kedokteran Indonesia 2012
A. Area Kompetensi
1.Profesionalitas yang luhur2.Mawas Diri dan Pengembangan Diri3.Komunikasi Efektif4.Pengelolaan Informasi5.Landasan Ilmiah Ilmu Kedokteran6.Ketrampilan Klinis7.Pengelolaan Masalah Kesehatan
36
Sisi Pemberi
Asuhan : Dr
C. Penjabaran Kompetensi1. Profesionalitas yang Luhur Area Kompetensi1.1. Kompetensi Inti…1.2. Lulusan Dokter Mampu : 1. Berke-Tuhan-an (Yang Maha Esa/ Yang Maha Kuasa)2. Bermoral, beretika, dan berdisiplin3. Sadar dan taat hukum4. Berwawasan sosial budaya5. Berperilaku profesional• Menunjukkan karakter sebagai dokter yg profesional• Bersikap dan berbudaya menolong• Mengutamakan keselamatan pasien• Mampu bekerja sama intra- dan inter- profesional
dalam tim pelayanan kesehatan demi keselamatan pasien
• Melaksanakan upaya pelayanan kesehatan dalam kerangka sistem kesehatan nasional dan global.
STANDAR KOMPETENSI DOKTER INDONESIAKonsil Kedokteran Indonesia 2012
37
(Framework for Action on Interprofessional Education & Collaborative Practice, WHO, 2010)38
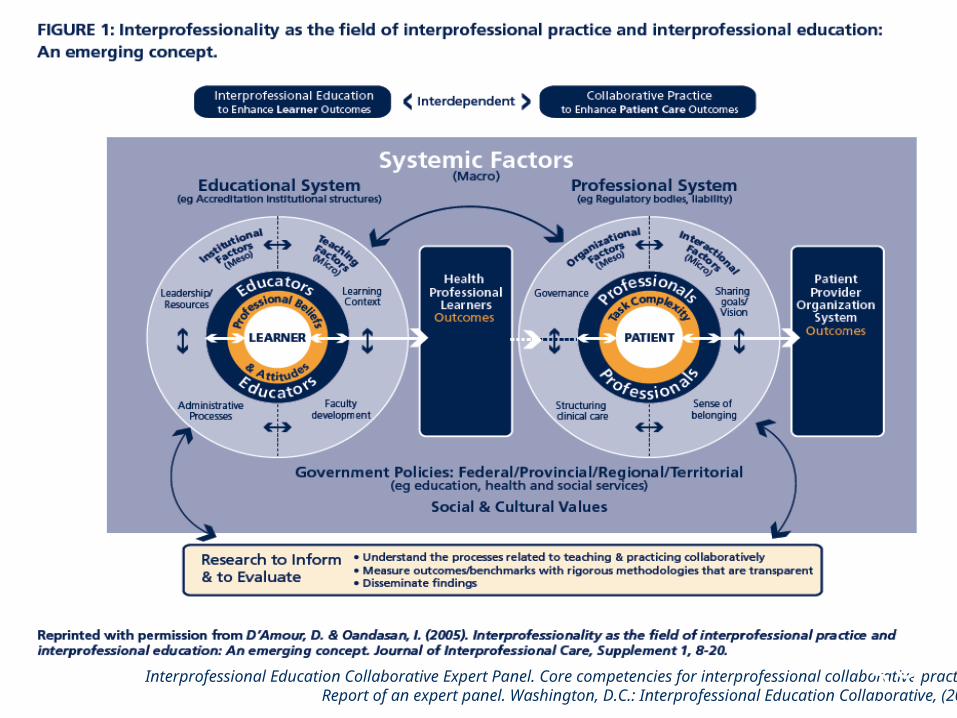
Interprofessional Education Collaborative Expert Panel. Core competencies for interprofessional collaborative practice: Report of an expert panel. Washington, D.C.: Interprofessional Education Collaborative, (2011)39
(Framework for Action on Interprofessional Education & Collaborative Practice, WHO, 2010)40
“Interprofessional
Education”
41
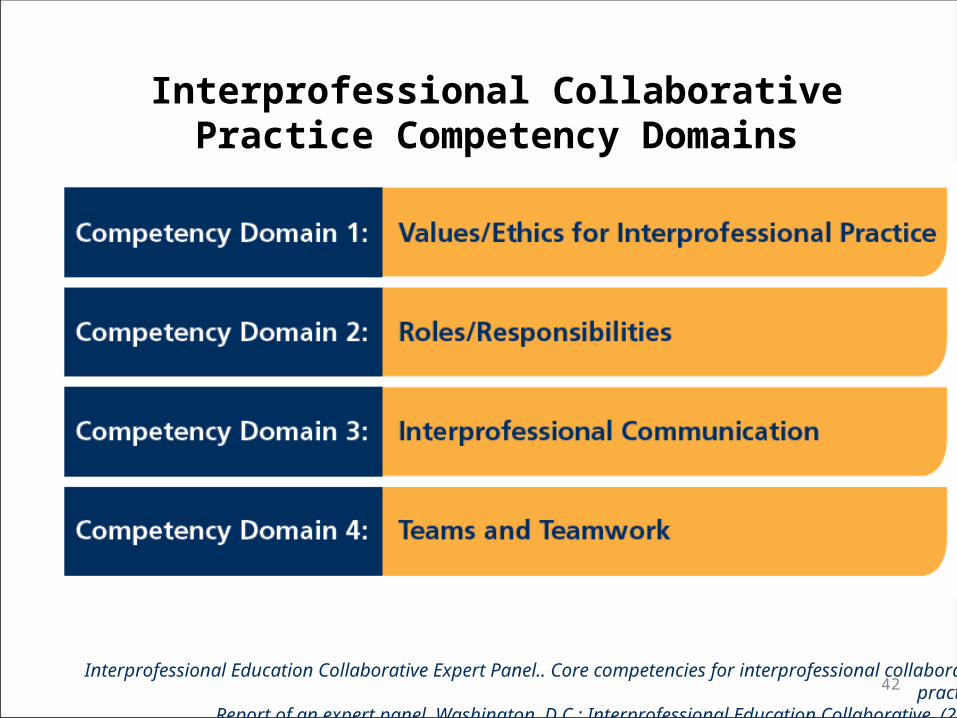
Interprofessional Collaborative Practice Competency Domains
Interprofessional Education Collaborative Expert Panel.. Core competencies for interprofessional collaborative practice: Report of an expert panel. Washington, D.C.: Interprofessional Education Collaborative, (2011)42
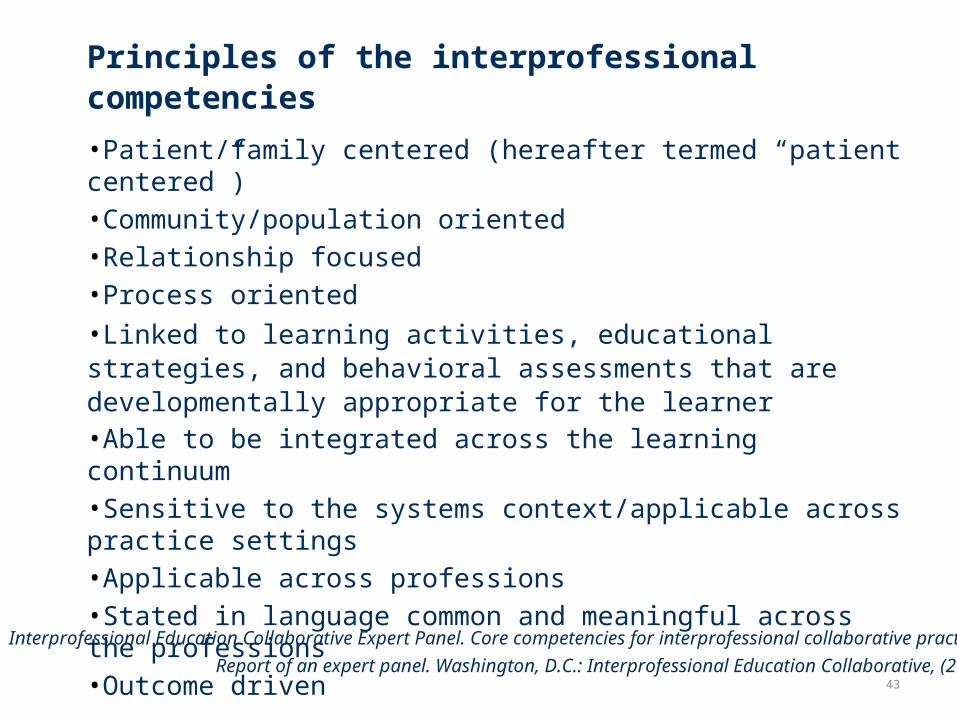
Principles of the interprofessional competencies •Patient/family centered (hereafter termed “patient centered”)•Community/population oriented•Relationship focused•Process oriented•Linked to learning activities, educational strategies, and behavioral assessments that are developmentally appropriate for the learner•Able to be integrated across the learning continuum•Sensitive to the systems context/applicable across practice settings•Applicable across professions•Stated in language common and meaningful across the professions•Outcome driven
Interprofessional Education Collaborative Expert Panel. Core competencies for interprofessional collaborative practice:
Report of an expert panel. Washington, D.C.: Interprofessional Education Collaborative, (2011)43
Professional Competency
Interprofessional Interprofessional CompetencyCompetency
Behavioral demonstrations of an integrated set of knowledge, skills, and attitudes that define the domains of work of a specific health profession applied in specific care contexts
Behavioral demonstrations of
•an integrated set of knowledge, skills and attitudes for
•working together across the professions, with other health care workers,
•and with patients/families / communities / populations
•to improve health outcomes in specific care contexts
44
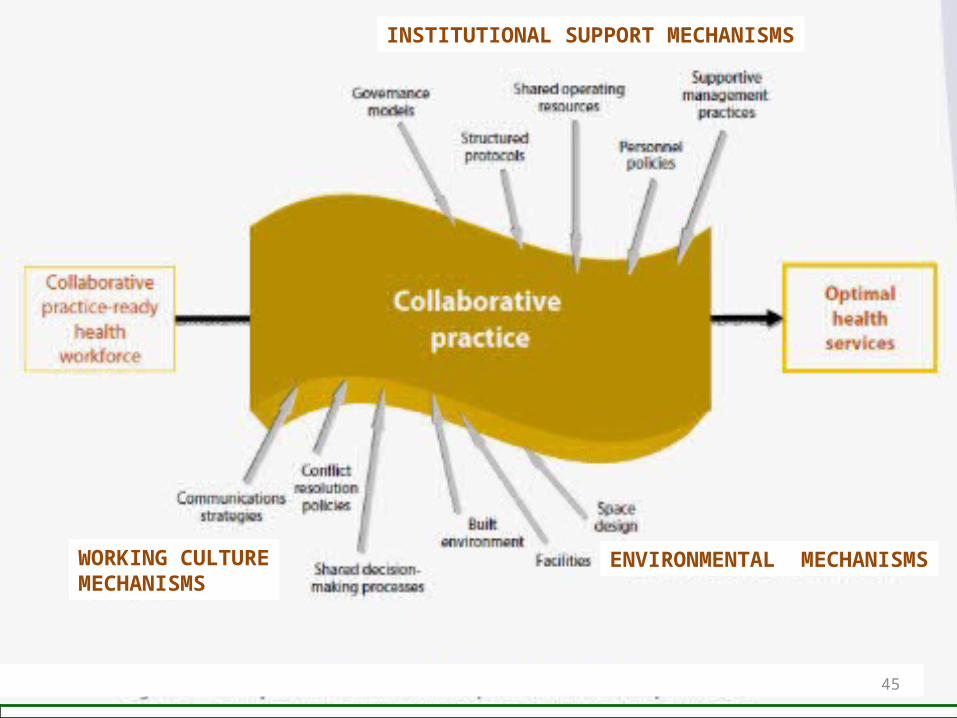
INSTITUTIONAL SUPPORT MECHANISMS
WORKING CULTUREMECHANISMS
ENVIRONMENTAL MECHANISMS
Figure 8. Examples of mechanisms that shape collaboration at the practice level 45
Elements of collaborative practice
(Kasperski M. Implementation strategies: ‘Collaboration in primary care - family doctors and nurse practitioners delivering shared care.’ Toronto, ON: Ontario College of Family Physicians, 2000)
1. Tanggung jawab - Responsibility
2. Akuntabel - Accountability
3. Koordinasi - Coordination
4. Komunikasi - Communication
5. Kerjasama - Cooperation
6. Asertif - Assertiveness
7. Otonomi - Autonomy
8. Percaya & Respek - Mutual trust and respect
46
Collaborative practice can decrease:o total patient complicationso length of hospital stayo tension and conflict among
caregiverso staff turnovero hospital admissionso clinical error rateso mortality rates
(Framework for Action on Interprofessional Education & Collaborative Practice, WHO, 2010)
47
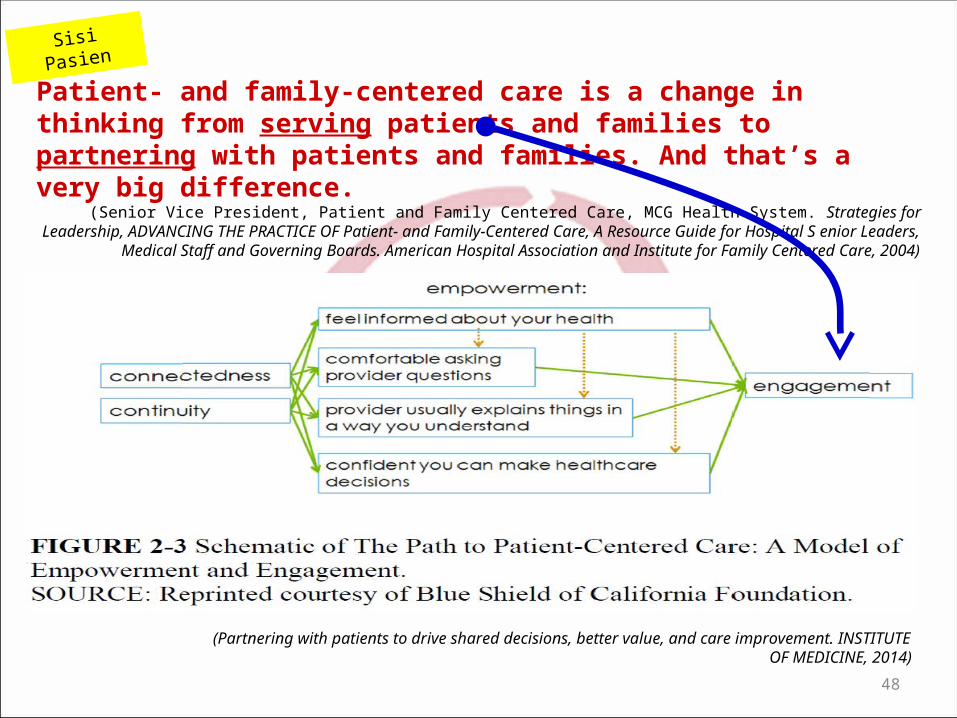
Patient- and family-centered care is a change in thinking from serving patients and families to partnering with patients and families. And that’s a very big difference.
(Senior Vice President, Patient and Family Centered Care, MCG Health System. Strategies for Leadership, ADVANCING THE PRACTICE OF Patient- and Family-Centered Care, A Resource Guide for Hospital S enior Leaders, Medical Staff and Governing Boards. American Hospital Association and
Institute for Family Centered Care, 2004)
(Partnering with patients to drive shared decisions, better value, and care improvement. INSTITUTE OF MEDICINE, 2014)
Sisi Pasien
48
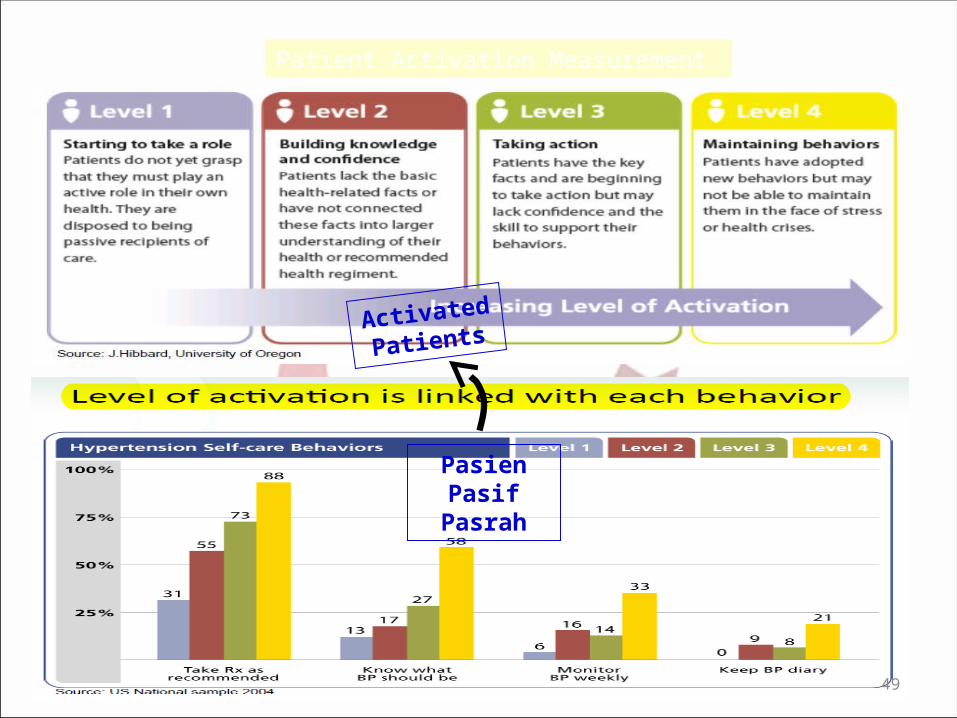
Patient Activation Measurement
Activated
Patients
PasienPasif
Pasrah
49
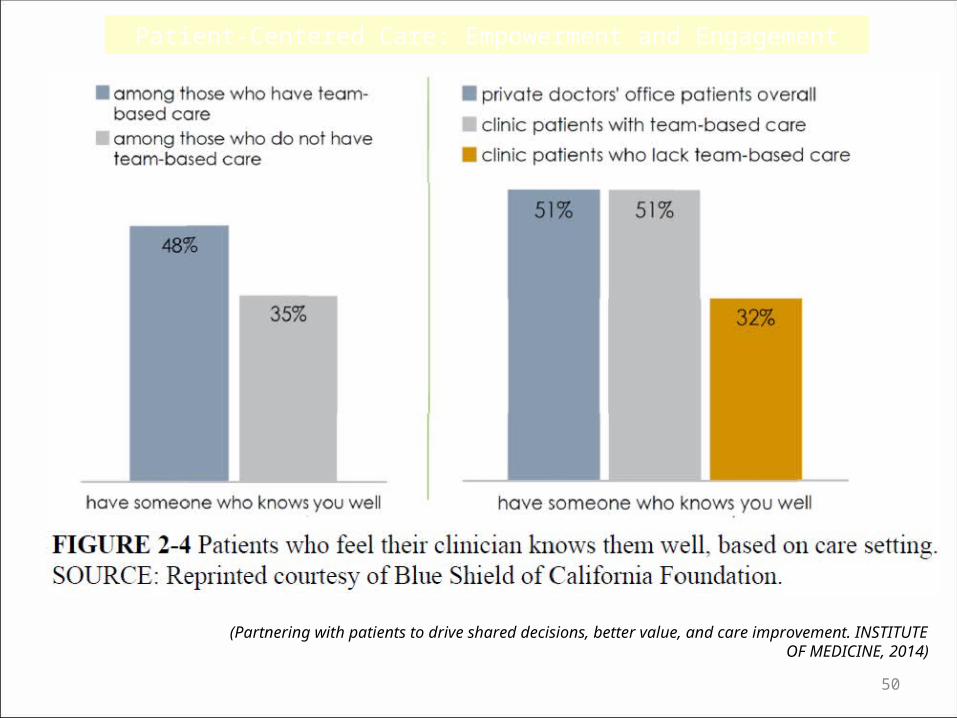
Patient-Centered Care: Empowerment and Engagement
(Partnering with patients to drive shared decisions, better value, and care improvement. INSTITUTE OF MEDICINE, 2014)
50
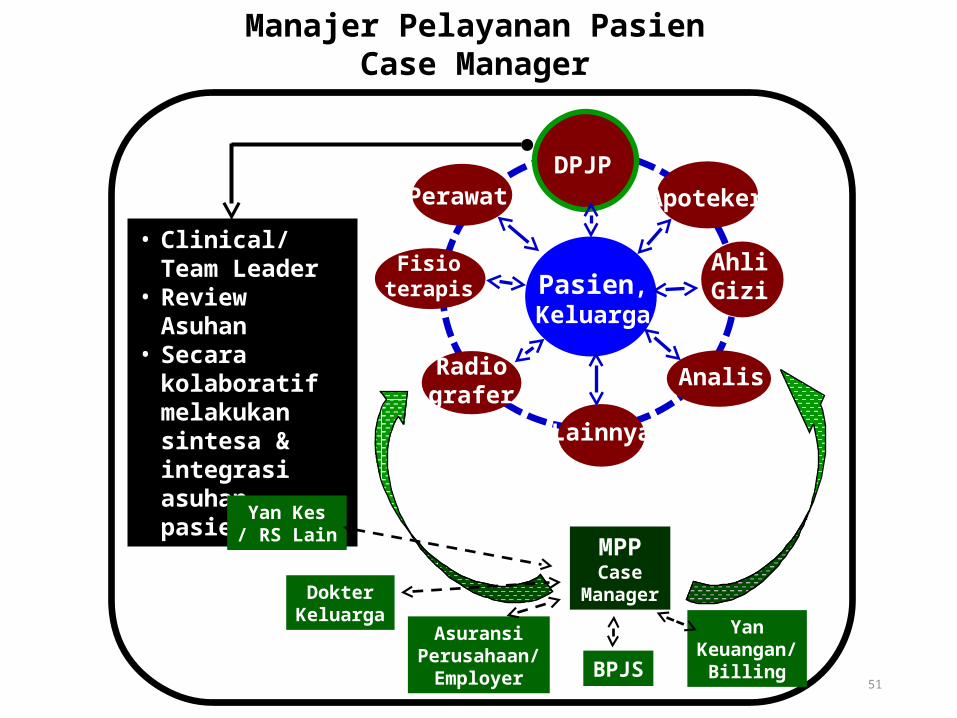
Pasien,Keluarga
Fisioterapis
Perawat Apoteker
AhliGizi
AnalisRadiografer
DPJP
Manajer Pelayanan PasienCase Manager
• Clinical/Team Leader
• Review Asuhan• Secara kolaboratif
melakukan sintesa & integrasi asuhan pasien
Lainnya
MPPCase
ManagerDokterKeluarga
YanKeuangan/
Billing
AsuransiPerusahaan/
Employer BPJS
Yan Kes/ RS Lain
51
• Dunn,N : Practical Issues Around Putting The Patient in Centre of Care, J R Soc Med. Jul 2003• Bensberg, M :Patient Centred Care Literatur Review, Dandenong District Division of General Practice, October 2007
52
Barrier to Patient Centered Care :
•Pasien
• Kurang percaya diri bertanya
• Tidak cukup pengetahuan utk analisis informasi
• Status social-ekonomi
•Dokter/Staf
• Kurang waktu, impractical
• Motivation
• Tidak terlatih menangkap ekspresi pasien ttg nilai, ide, perasaan
• Sulit diimplementasi, tidak jelas akan adanya perbaikan outcome
• Dunn,N : Practical Issues Around Putting The Patient in Centre of Care, J R Soc Med. Jul 2003• Bensberg, M :Patient Centred Care Literatur Review, Dandenong District Division of General Practice, October 2007
53
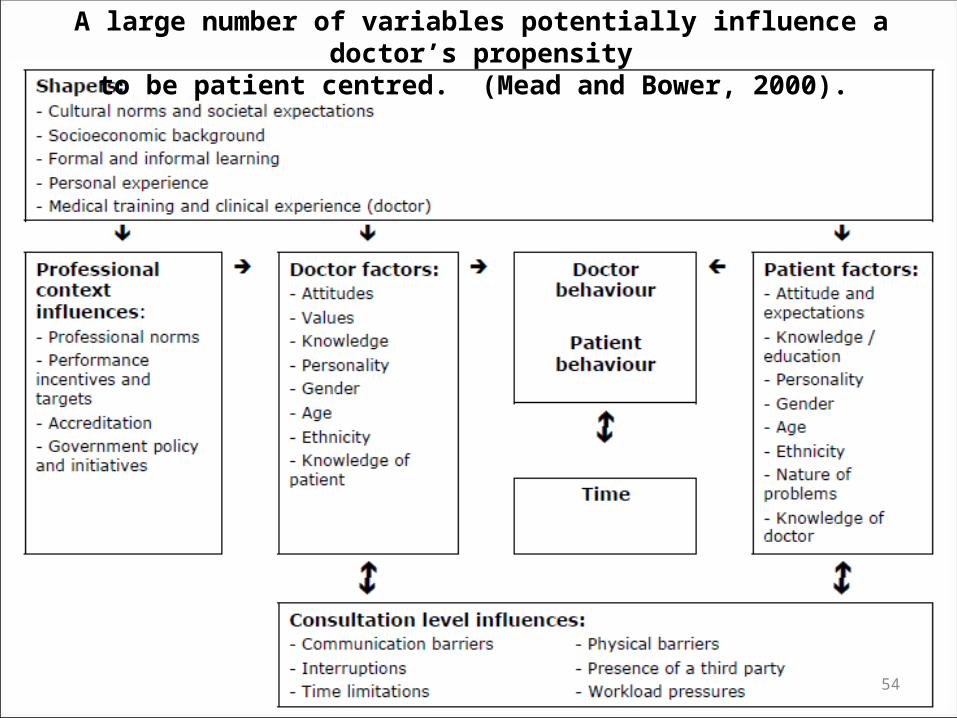
A large number of variables potentially influence a doctor’s propensityto be patient centred. (Mead and Bower, 2000).
54
Beberapa elemen pokok untuk keberhasilan RS menerapkan / melaksanakan asuhan berfokus pasien / PCC adalah :
1.Komitmen kuat senior leadership
2.Komunikasi yang jelas tentang visi strategis,
3.Keikutsertaan aktif dengan pasien dan keluarga di seluruh RS,
4.Fokus terhadap kepuasan staf,
5.Penilaian dan umpan balik secara aktif dalam pelaporan pengalaman pasien,
6.Sumber yg adekuat untuk redesain pemberian asuhan,
7.Capacity building staf,
8.Akuntabilitas dan insentif
9.Budaya yang kuat mendukung perubahan dan pembelajaran.
Promoting Patient-centered Care
(Luxford,K., Safran,DG., Delbanco,T . Promoting patient-centered care: a qualitative study of facilitators and barriers in healthcare organizations with a reputation for improving the patient experience.
Journal for Quality in Health Care, vol 23, 2011)55
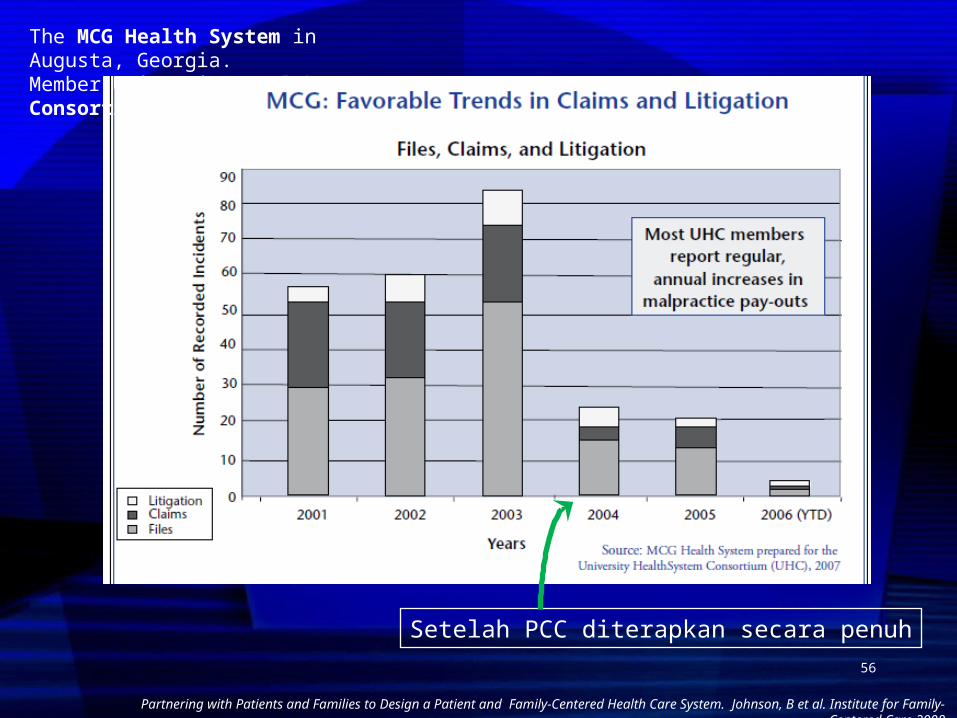
Partnering with Patients and Families to Design a Patient and Family-Centered Health Care System. Johnson, B et al. Institute for Family-Centered Care 2008
The MCG Health System in Augusta, Georgia. Member University HealthSystem Consortium
Setelah PCC diterapkan secara penuh56
1. Pasien = Pusat dalam proses asuhan pasien (patient care) PCC Patient Centered Care
2. Konsep inti PCC : A. Sisi Pasien : Martabat & Respek, Informasi, Partisipasi,
KolaborasiB. Sisi PPA : Tim Interdisiplin, Kolaborasi Interprofesional, DPJP
– Clinical Leader, Personalised care-BPIS3. Profesional Pemberi Asuhan (PPA) diposisikan mengelilingi
Pasien, menghormati dan responsif terhadap pilihan, kebutuhan & nilai-nilai pribadinya
4. PPA Tim Interdisiplin, dgn kompetensi memadai, termasuk Interproffesional Competency, dgn Kolaborasi Interprofesional (Interproffesional Collaboration), memberikan kontribusi profesinya yg setara. Tugas mandiri, delegatif dan kolaboratif
RINGKASAN CIRI POKOK PCC
57
5. DPJP adalah sbg Clinical/Team Leader : kerangka pokok asuhan pasien, review-sintesa-integrasi asuhan
6. PPA melakukan komunikasi-edukasi lengkap & adekuat ke Pasien-Keluarga sehingga paham secara komprehensif & adekuat
7. Pasien & keluarga adalah Mitra PPA bagian dari tim : mereka mereka ikut memilih alternatif ikut memilih alternatif ikut merasa memiliki keputusan ikut merasa memiliki keputusan ikut bertanggungjawabikut bertanggungjawab
8. Dalam konteks PCC, Manajer Pelayanan Pasien / Case Manager (berbasis klien) menjaga kontinuitas pelayanan serta kendali mutu – biaya utk memenuhi kebutuhan Ps dan keluarga
RINGKASAN CIRI POKOK PCC
58
1. Pada model asuhan pasien yang tradisional, Dokter merupakan pusat dari asuhan pasien, sebagai “Captain of the ship”, namun patient safety belum terjamin
2. Asuhan pasien terdiri dari 4 pilar : Etik, Kebutuhan Pasien, Mutu-Keselamatan Pasien, EBM-VBM, dpayungi oleh Manajemen Risiko RS dan PCC
3. Pada model PCC, pasien adalah pusat, profesional pemberi asuhan (PPA) diposisikan mengelilingi / melayani pasien, & semua PPA tsb berkolaborasi dlm fungsi yg setara, sehingga disebut “Interdisciplinary team” dgn Kolaborasi Interprofesional. Dr adalah “Team Leader / Coach”. Pasien memperoleh asuhan yg terbaik & bermanfaat bagi pasien
4. PCC dalam pelaksanaan asuhan pasien, masih belum dipahami sepenuhnya, belum sepenuhnya dihargai
5. Dengan PCC terjadi perubahan mendasar dlm cara Manajemen RS. Saat ini PCC merupakan “Mainstream model”, sdh menjadi “Trend global” pelayanan kesehatan di Rumah Sakit di dunia
6. Disadari atau tidak, akar masalah arus pasien keluar negeri adalah karena belum sepenuhnya RS di Indonesia menerapkan PCC
7. Standar Akreditasi RS v.2012 mengharuskan & mengoptimalkan penerapan PCC
8. Terapkan PCC langkah demi langkah - “one step at a time”
KESIMPULAN
59
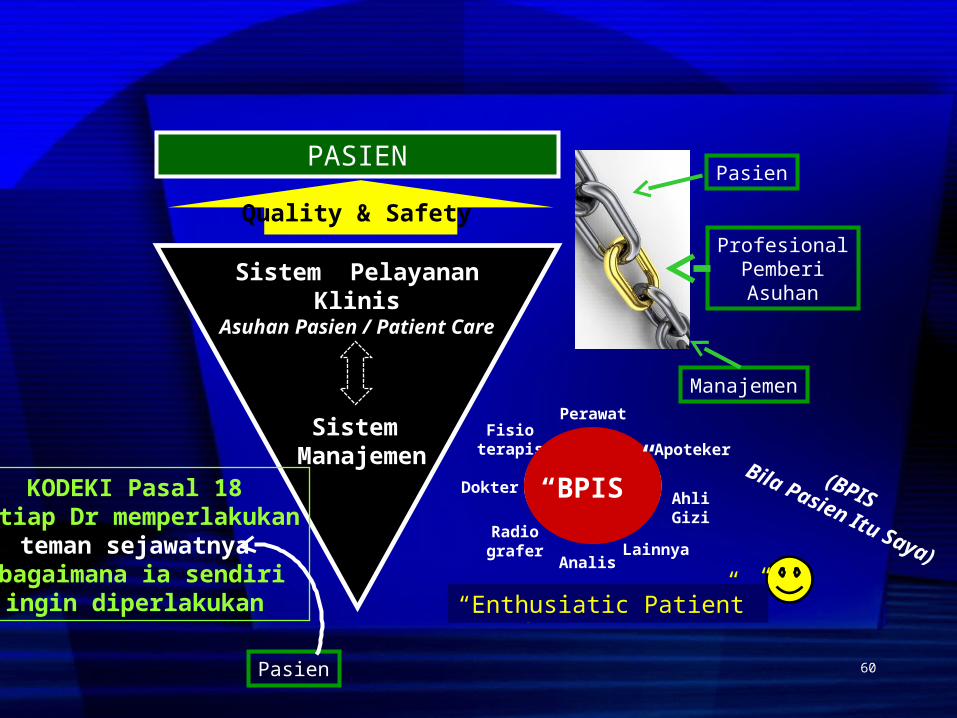
“Kepuasan Pasien”
Sistem Manajemen
Sistem Pelayanan Klinis
Asuhan Pasien / Patient Care
Quality & Safety
PASIEN
ProfesionalPemberiAsuhan
Manajemen
Pasien
Perawat
ApotekerFisio
terapis
AhliGizi
Radiografer
PasienDokter
Analis
“BPIS”
“Enthusiatic Patient”
Lainnya
KODEKI Pasal 18Setiap Dr memperlakukan
teman sejawatnyasebagaimana ia sendiri
ingin diperlakukan
Pasien
(BPISBila Pasien Itu Saya)
60
Dr. Nico A. Lumenta, K.Nefro, MM, MHKesKomisi Akreditasi Rumah Sakit
61







