Download - CAPD Twin Bag System P

1
DHS
CAPD – Twin Bag System
Bandung; 26 – 27 April 2013
dr.Harvian Satya D
Departemen Medical
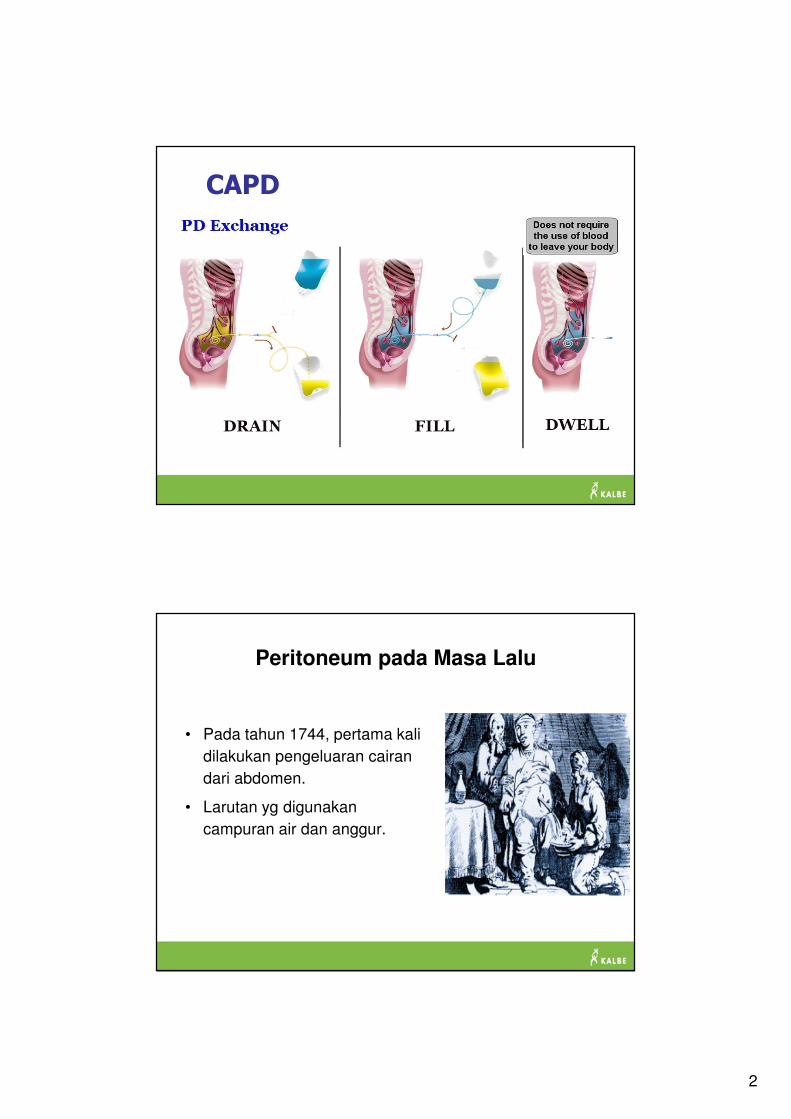
CAPD (Continuous Ambulatory Peritoneal Dialysis )
Darah dibersihkan melalui pembuluh darah kecil peritoneum
Dipasang kateter ke rongga perut untuk memasukkan dialisat
Waste dan cairan keluar dari kapiler ke dialisat � dibuang ke luar tubuh
Cairan didiamkan dalam kavum peritoneum selama 3-5 jam (dwelling time)
Dilakukan 3-5 kali sehari, setiap kali sekitar 30 menit.
Drugs.com.Peritoneal Dialysis Catheter Care.
2
CAPD
Peritoneum pada Masa Lalu
• Pada tahun 1744, pertama kali
dilakukan pengeluaran cairan
dari abdomen.
• Larutan yg digunakan
campuran air dan anggur.
3
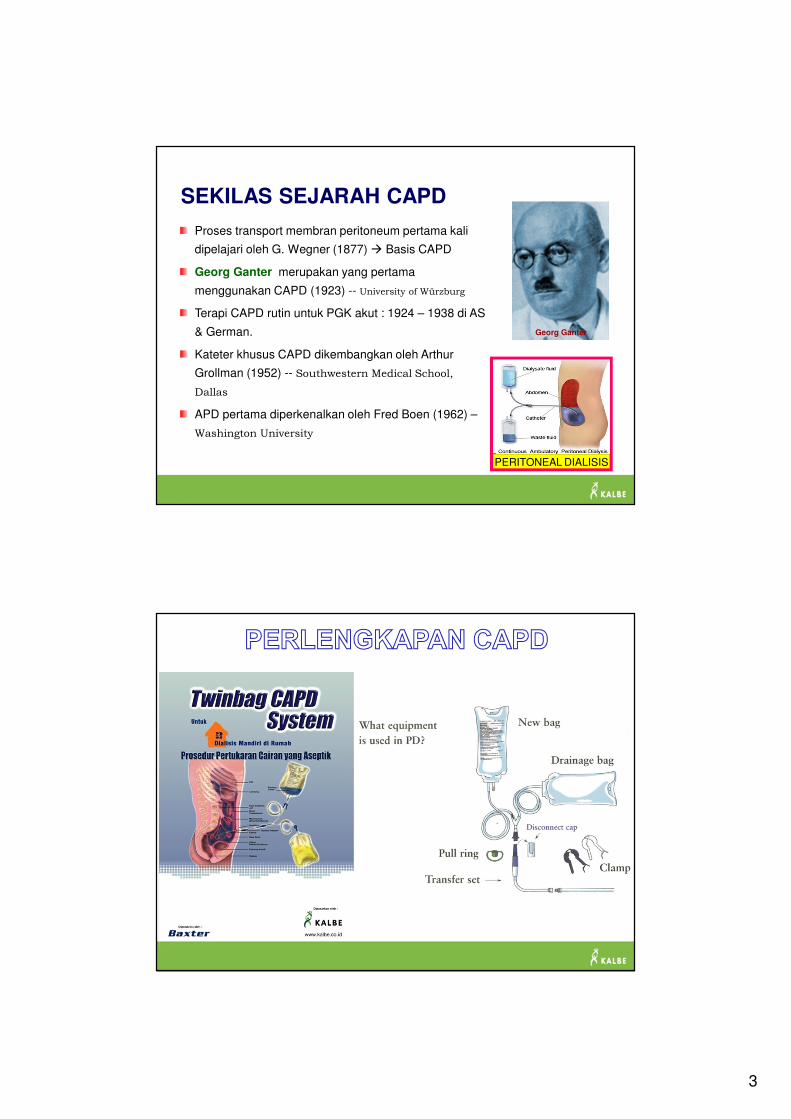
SEKILAS SEJARAH CAPD
PERITONEAL DIALISIS
Proses transport membran peritoneum pertama kali
dipelajari oleh G. Wegner (1877) � Basis CAPD
Georg Ganter merupakan yang pertama
menggunakan CAPD (1923) -- University of Würzburg
Terapi CAPD rutin untuk PGK akut : 1924 – 1938 di AS
& German.
Kateter khusus CAPD dikembangkan oleh Arthur
Grollman (1952) -- Southwestern Medical School,
Dallas
APD pertama diperkenalkan oleh Fred Boen (1962) –
Washington University
Georg Ganter
4
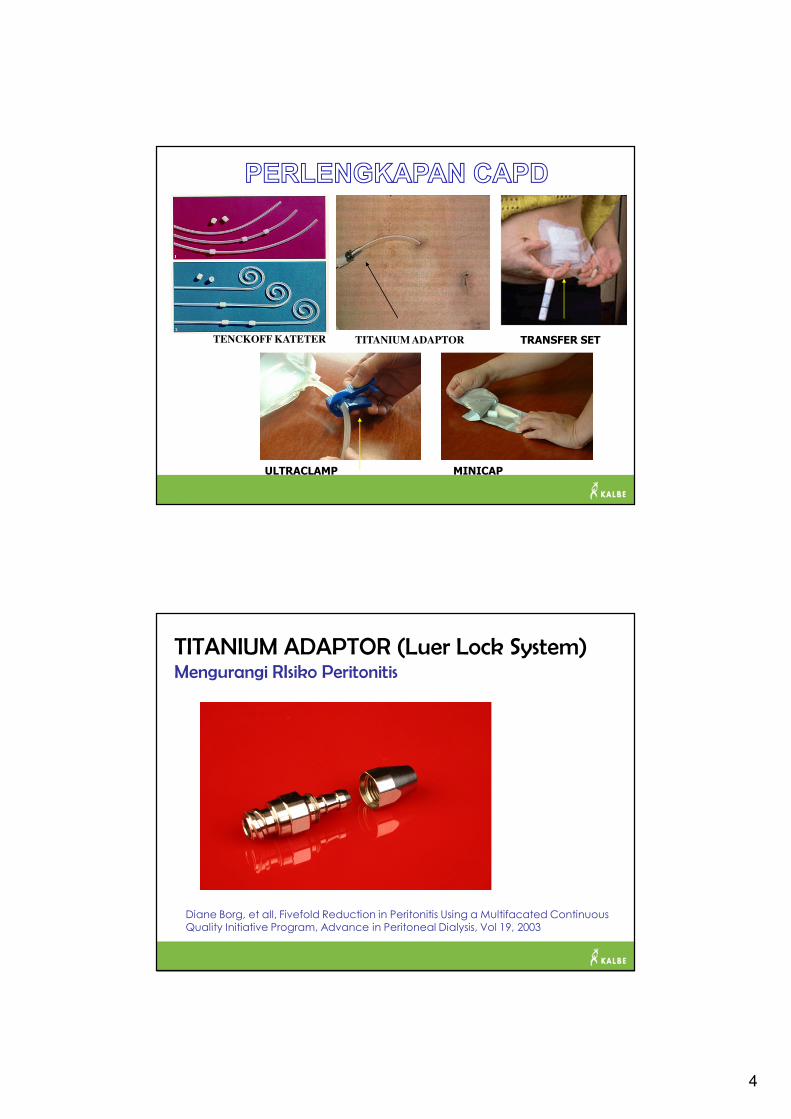
TENCKOFF KATETER TITANIUM ADAPTOR TRANSFER SET
ULTRACLAMP MINICAP
TITANIUM ADAPTOR (Luer Lock System)Mengurangi RIsiko Peritonitis
Diane Borg, et all, Fivefold Reduction in Peritonitis Using a Multifacated Continuous Quality Initiative Program, Advance in Peritoneal Dialysis, Vol 19, 2003
5
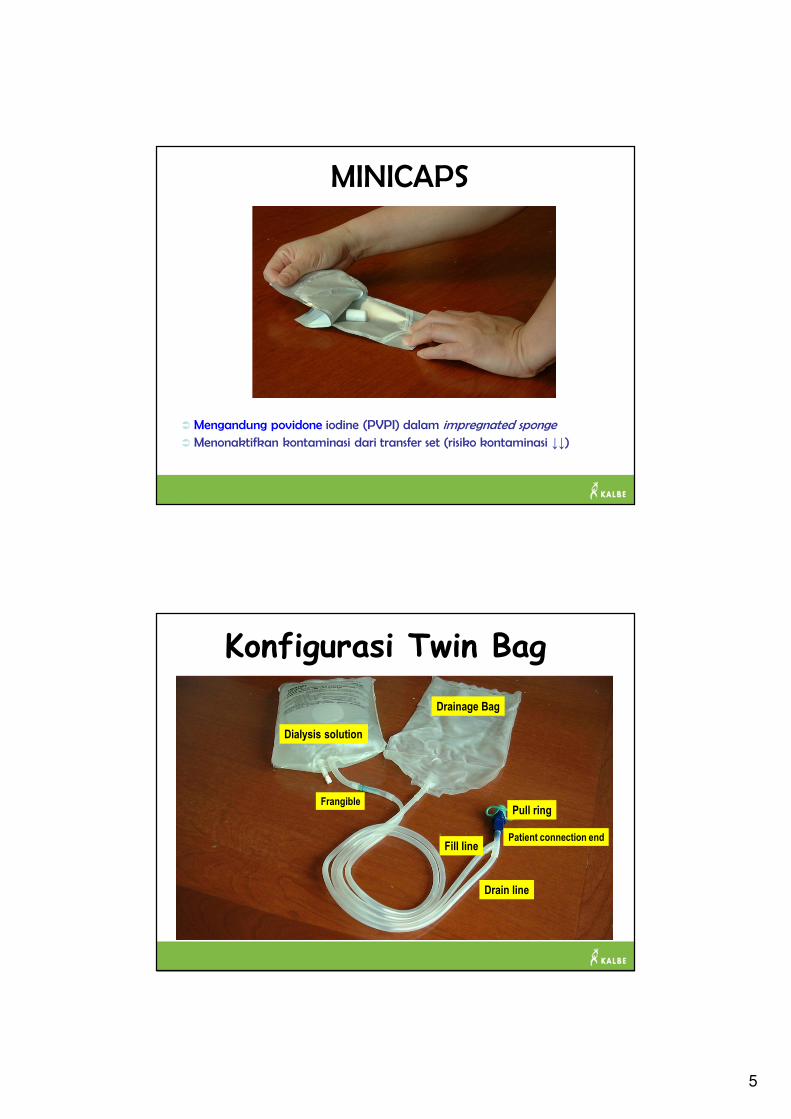
MINICAPS
� Mengandung povidone iodine (PVPI) dalam impregnated sponge
� Menonaktifkan kontaminasi dari transfer set (risiko kontaminasi ↓↓)
Dialysis solutionDrainage Bag
Frangible
Drain line
Fill linePatient connection end
Pull ring
Konfigurasi Twin Bag
Dialysis solution
6
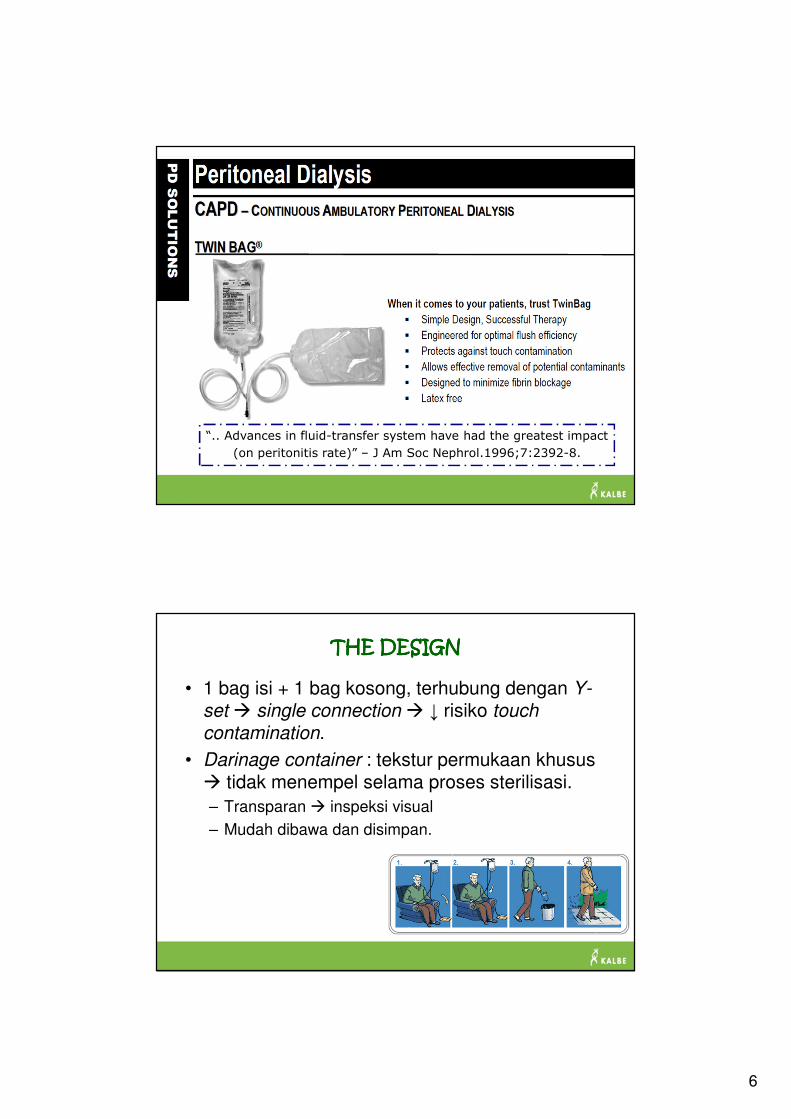
“.. Advances in fluid-transfer system have had the greatest impact
(on peritonitis rate)” – J Am Soc Nephrol.1996;7:2392-8.
THE DESIGNTHE DESIGNTHE DESIGNTHE DESIGN
• 1 bag isi + 1 bag kosong, terhubung dengan Y-
set � single connection � ↓ risiko touch
contamination.
• Darinage container : tekstur permukaan khusus � tidak menempel selama proses sterilisasi.
– Transparan � inspeksi visual
– Mudah dibawa dan disimpan.
7
SISTEM TWIN BAGSISTEM TWIN BAGSISTEM TWIN BAGSISTEM TWIN BAG
• Tujuan : Mengurangi risiko peritonitis (connectology)
• Insidens peritonitis lebih ↓ pada twin bag dibandingkan
single-bag
– 1-yr peritonitis free rate : 79% vs 66%
• (Harris DCH, et al.1996) twin bag vs single bag (n=631 pts-mth)
– time to first infection lebih baik (HR 2,4; p<0,04)
– Insidens peritonitis kumulatif lebih ↓ 3,6 x lipat (p=0,004)
– Total biaya lebih murah (termasuk biaya untuk terapi peritonitis)
Patients on the twin-bag system showed a significant increase in the
peritonitis-free interval in comparison with other systems (non-twin
bag group). – Tielens E, et al.Nephrol Dial Transplant.1993;11:1237-43
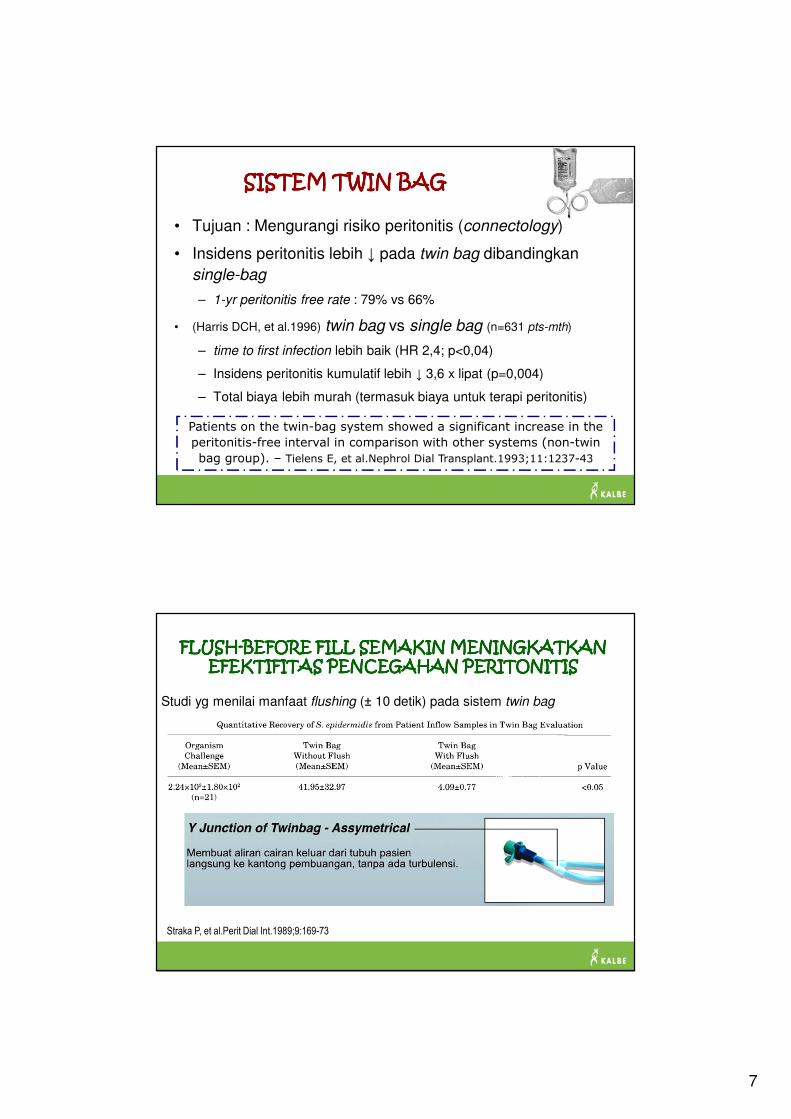
FLUSHFLUSHFLUSHFLUSH----BEFORE FILL SEMAKIN MENINGKATKAN BEFORE FILL SEMAKIN MENINGKATKAN BEFORE FILL SEMAKIN MENINGKATKAN BEFORE FILL SEMAKIN MENINGKATKAN EFEKTIFITAS PENCEGAHAN PERITONITISEFEKTIFITAS PENCEGAHAN PERITONITISEFEKTIFITAS PENCEGAHAN PERITONITISEFEKTIFITAS PENCEGAHAN PERITONITIS
Studi yg menilai manfaat flushing (± 10 detik) pada sistem twin bag
“Flushing of the y -junction before drain primes the solution line
� minimizes entrapment of microorganisms in the solution line
segment of the Y -junction during the patient drain procedure.”
Straka P, et al.Perit Dial Int.1989;9:169-73
8
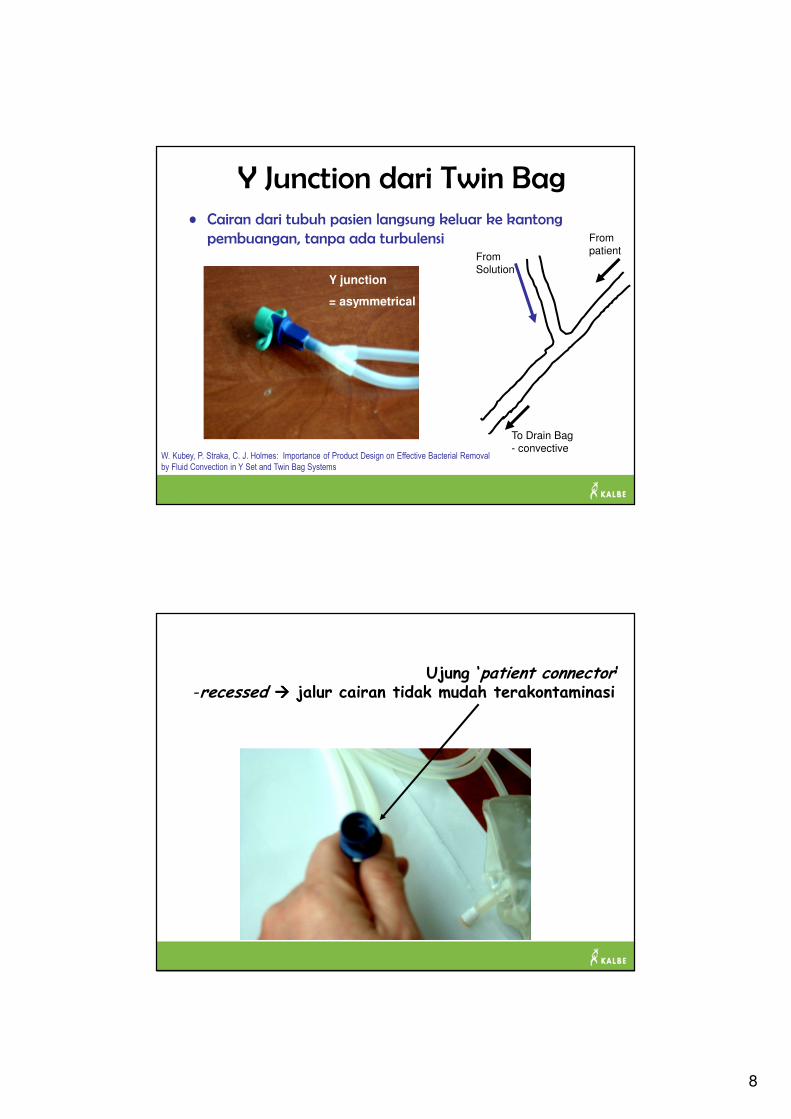
Y Junction dari Twin Bag• Cairan dari tubuh pasien langsung keluar ke kantong
pembuangan, tanpa ada turbulensi
Y junction
= asymmetrical
W. Kubey, P. Straka, C. J. Holmes: Importance of Product Design on Effective Bacterial Removal
by Fluid Convection in Y Set and Twin Bag Systems
To Drain Bag- convective
From patient
From Solution
Ujung ‘patient connector’-recessed ���� jalur cairan tidak mudah terakontaminasi
9
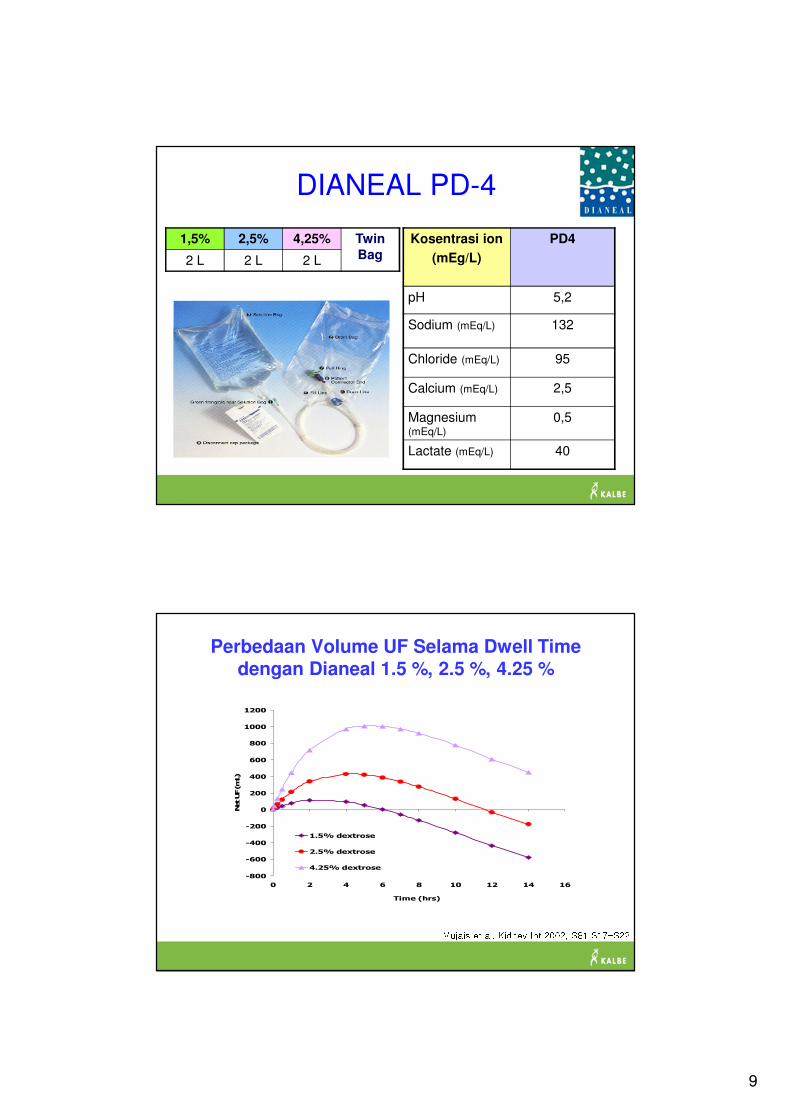
DIANEAL PD-4
Kosentrasi ion
(mEg/L)
PD4
pH 5,2
Sodium (mEq/L) 132
Chloride (mEq/L) 95
Calcium (mEq/L) 2,5
Magnesium(mEq/L)
0,5
Lactate (mEq/L) 40
1,5% 2,5% 4,25% Twin
Bag2 L 2 L 2 L
Perbedaan Volume UF Selama Dwell Time dengan Dianeal 1.5 %, 2.5 %, 4.25 %
-800
-600
-400
-200
0
200
400
600
800
1000
1200
0 2 4 6 8 10 12 14 16
Time (hrs)
Net UF (mL)
1.5% dextrose
2.5% dextrose
4.25% dextrose Mujais et al. Kidney Int 2002, S81 S17-S22
10
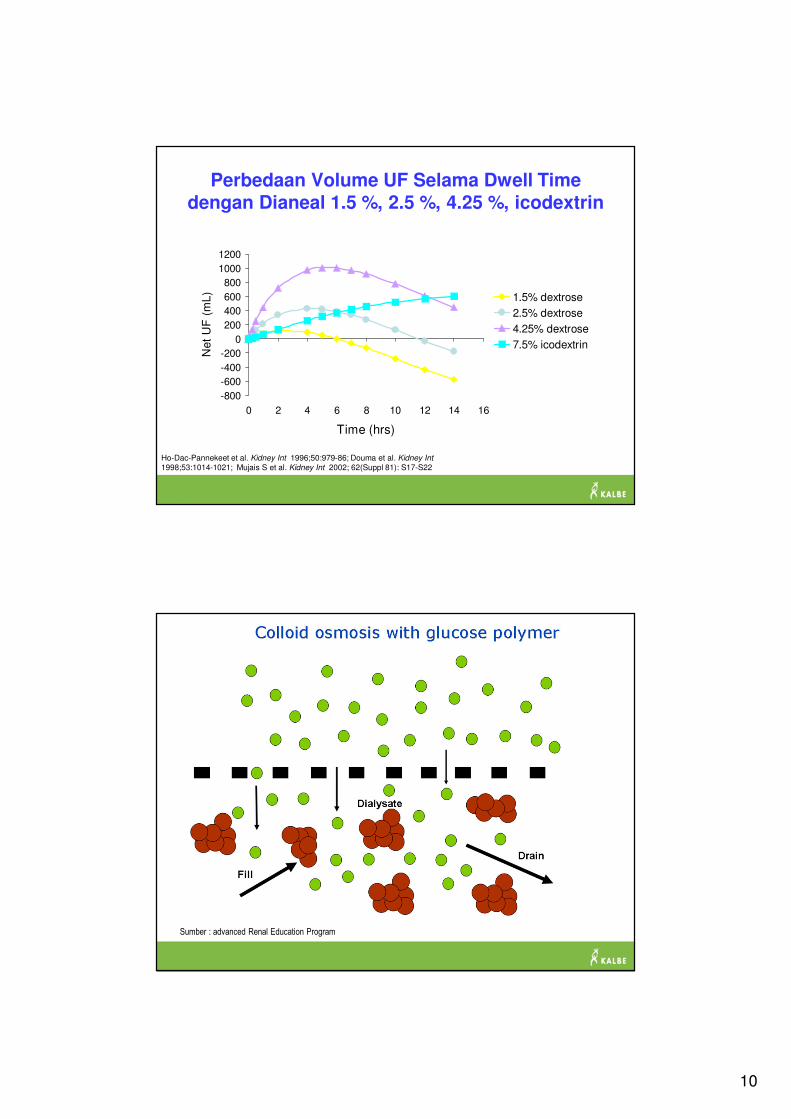
Perbedaan Volume UF Selama Dwell Time dengan Dianeal 1.5 %, 2.5 %, 4.25 %, icodextrin
-800
-600
-400
-200
0
200
400
600
800
1000
1200
0 2 4 6 8 10 12 14 16
Time (hrs)
Net
UF
(m
L) 1.5% dextrose
2.5% dextrose
4.25% dextrose
7.5% icodextrin
Ho-Dac-Pannekeet et al. Kidney Int 1996;50:979-86; Douma et al. Kidney Int
1998;53:1014-1021; Mujais S et al. Kidney Int 2002; 62(Suppl 81): S17-S22
Sumber : advanced Renal Education Program
11
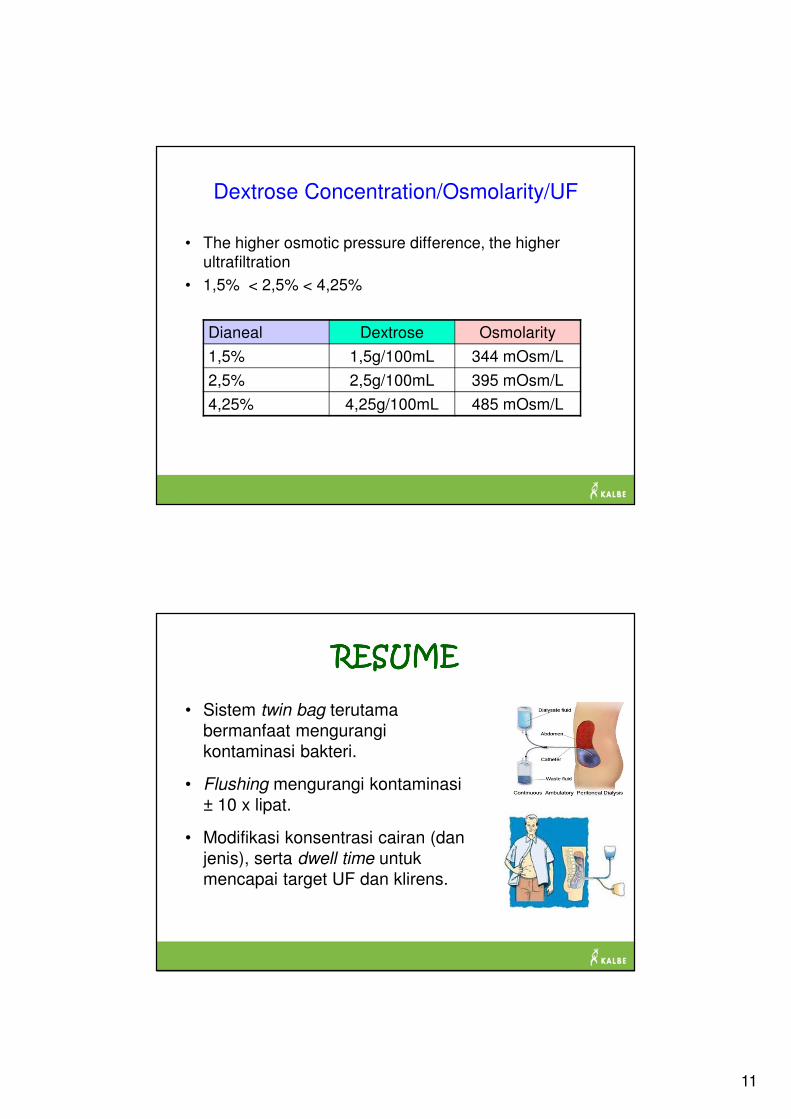
Dextrose Concentration/Osmolarity/UF
• The higher osmotic pressure difference, the higher
ultrafiltration
• 1,5% < 2,5% < 4,25%
Dianeal Dextrose Osmolarity
1,5% 1,5g/100mL 344 mOsm/L
2,5% 2,5g/100mL 395 mOsm/L
4,25% 4,25g/100mL 485 mOsm/L
RESUMERESUMERESUMERESUME
• Sistem twin bag terutama
bermanfaat mengurangi
kontaminasi bakteri.
• Flushing mengurangi kontaminasi
± 10 x lipat.
• Modifikasi konsentrasi cairan (dan
jenis), serta dwell time untuk
mencapai target UF dan klirens.
12
TERIMA KASIHTERIMA KASIHTERIMA KASIHTERIMA KASIHSEMOGA BERMANFAATSEMOGA BERMANFAATSEMOGA BERMANFAATSEMOGA BERMANFAAT







