peran pemerintah daerah dalam...
TRANSCRIPT
dr. Hasto Wardoyo, Sp.OG (K)Bupati Kulonprogo
PERAN PEMERINTAH DAERAH DALAM
MEMPERKUAT KESEHATAN MENTAL

UU.KES. No 36 Tahun 2009
Adalah keadaan sehat baik secara fisik,
mental, spiritual maupun sosial yang
memungkinkan setiap orang untuk hidup
produktif secara sosial dan ekonomis.
UNSUR KESEHATAN PARIPURNA
DEFINISI KESEHATAN

UU KESWA NO 18 / 2014
• Terwujudnya derajat kesehatan yang setinggi-tingginya.
• Perlu berbagai upaya kesehatan termasuk upaya kesehatan
jiwa dengan pendekatan promotif, preventif, kuratif, dan
rehabilitatif.
• Upaya kesehatan jiwa harus diselenggarakan secara
terintegrasi, komprehensif, dan berkesinambungan oleh
Pemerintah, Pemda, dan/atau masyarakat.
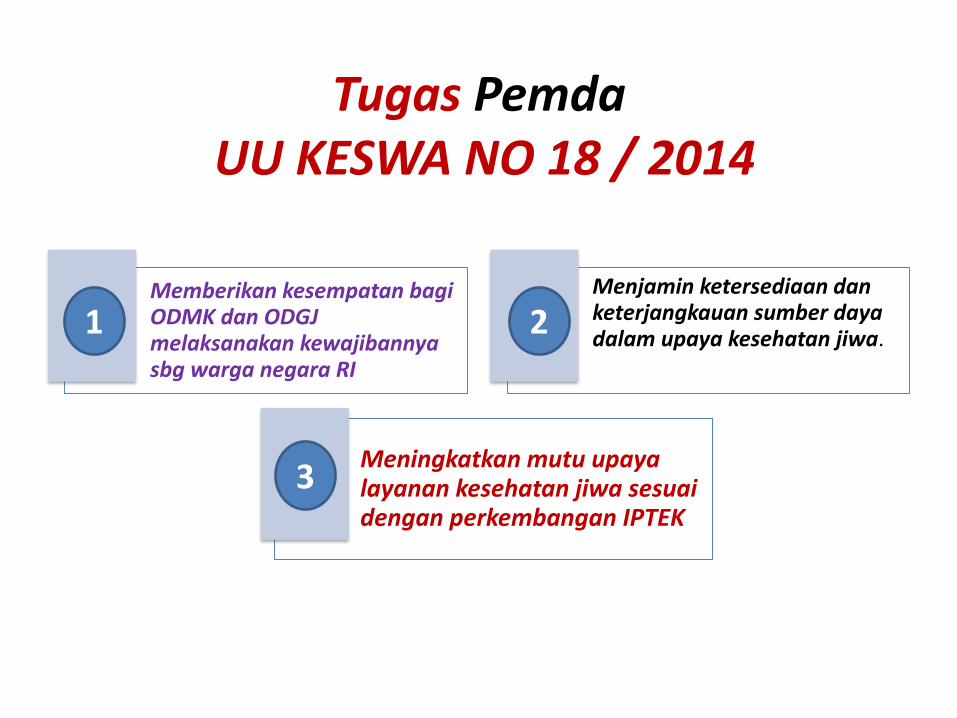
Tugas PemdaUU KESWA NO 18 / 2014
Memberikan kesempatan bagiODMK dan ODGJ melaksanakan kewajibannyasbg warga negara RI
Menjamin ketersediaan danketerjangkauan sumber dayadalam upaya kesehatan jiwa.
Meningkatkan mutu upayalayanan kesehatan jiwa sesuaidengan perkembangan IPTEK
1 2
3

BURDEN OF DISEASE IN INDONESIA
1990 –2010 AND 2015
Year 1990 Year 2010 Year 2015
Increasing/decreasing Burden of Disease
8. Depresi 8. Depresi10. Depresi
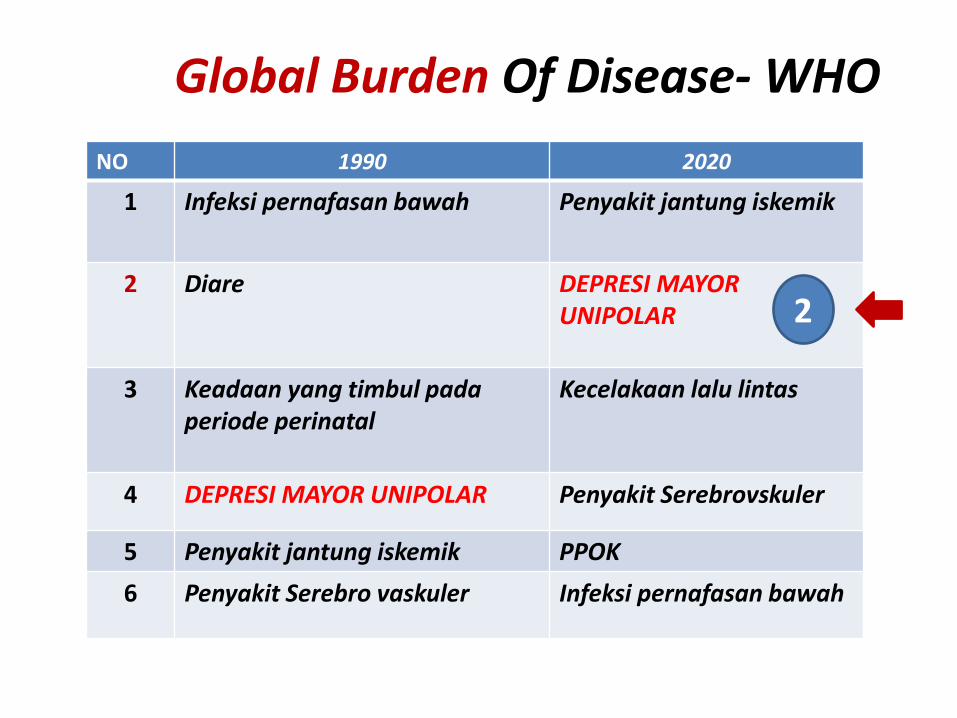
Global Burden Of Disease- WHO
NO 1990 2020
1 Infeksi pernafasan bawah Penyakit jantung iskemik
2 Diare DEPRESI MAYOR UNIPOLAR
3 Keadaan yang timbul padaperiode perinatal
Kecelakaan lalu lintas
4 DEPRESI MAYOR UNIPOLAR Penyakit Serebrovskuler
5 Penyakit jantung iskemik PPOK
6 Penyakit Serebro vaskuler Infeksi pernafasan bawah
2

MASALAH KESEHATAN JIWA DI INDONESIA, DIY & KULON PROGO
Indonesia DIY
Gangguan Mental Emosional(termasuk Depresi & Ansietas)
6 % 8,1 %
Gangguan Jiwa Berat(Psikosis) : ODGJ
1,7 permil
2,7 permil
Riskesdas 2013



No Kabupaten/
Kota
Jumlah
penduduk
Preva-
Lensi
(Permil)
Gangguan
jiwa psikotik
1 Kulon Progo 455.222 4,67 1.892
2 Bantul 968.632 4 3.875
3 Gunung Kidul 698.825 2,05 1.433
4 Sleman 1.163.970 1,52 1.769
5 Kota 400.467 2,14 857
DIY 3.637.116 2,7 9.820
Prevalensi Gangguan Jiwa Berat/Psikotikdi Daerah Istimewa Yogyakarta
Riskesdas 2013
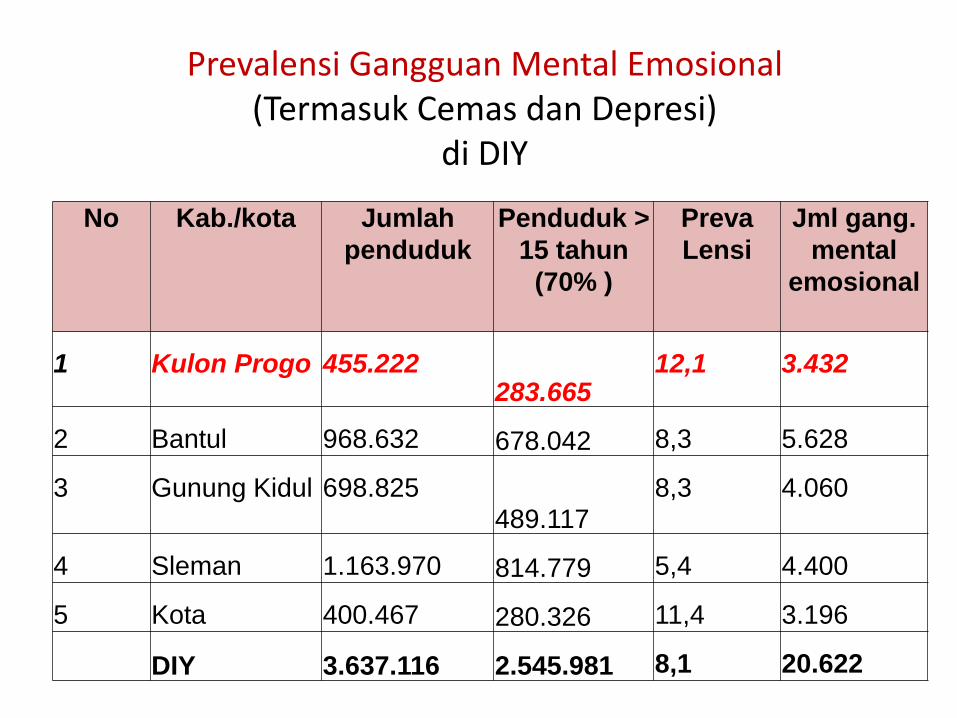
Prevalensi Gangguan Mental Emosional(Termasuk Cemas dan Depresi)
di DIY
No Kab./kota Jumlah
penduduk
Penduduk >
15 tahun
(70% )
Preva
Lensi
Jml gang.
mental
emosional
1 Kulon Progo 455.222283.665
12,1 3.432
2 Bantul 968.632 678.042 8,3 5.628
3 Gunung Kidul 698.825489.117
8,3 4.060
4 Sleman 1.163.970 814.779 5,4 4.400
5 Kota 400.467 280.326 11,4 3.196
DIY 3.637.116 2.545.981 8,1 20.622

Kasus ODGJ di Daerah Istimewa Yogyakarta(Jumlah yang membutuhkan rawat inap & yang di Komunitas )
NOKabupaten/
Kota
Jumlah
psikotik
Akut : Perlu
rawat inap
(10%)
Di komunitas
1 Kulon Progo1892 189 1703
2 Bantul3875 388 3487
3 Gunung Kidul1433 143 1290
4 Sleman1769 177 1592
5 Kota 857 86 771
DIY (total) 9.820 982 8.838


Lima Besar Kasus Gangguan JiwaDi Kabupaten Kulon Progo
Tahun 2016

Skizofrenia berdasarkan golongan Umurdi Kulon Progo Tahun 2016
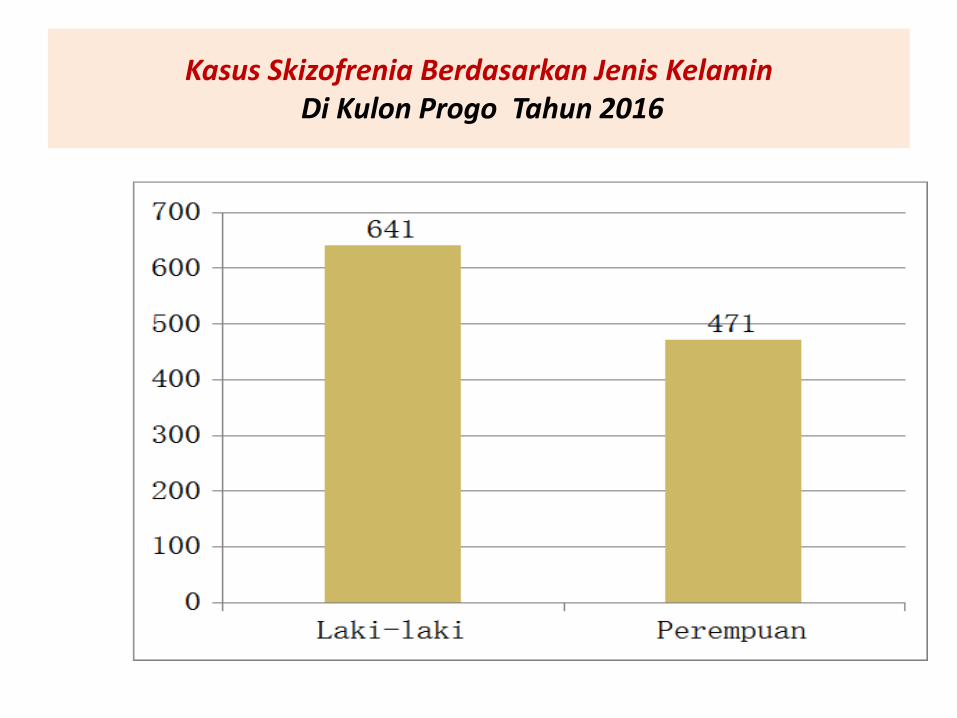
Kasus Skizofrenia Berdasarkan Jenis KelaminDi Kulon Progo Tahun 2016
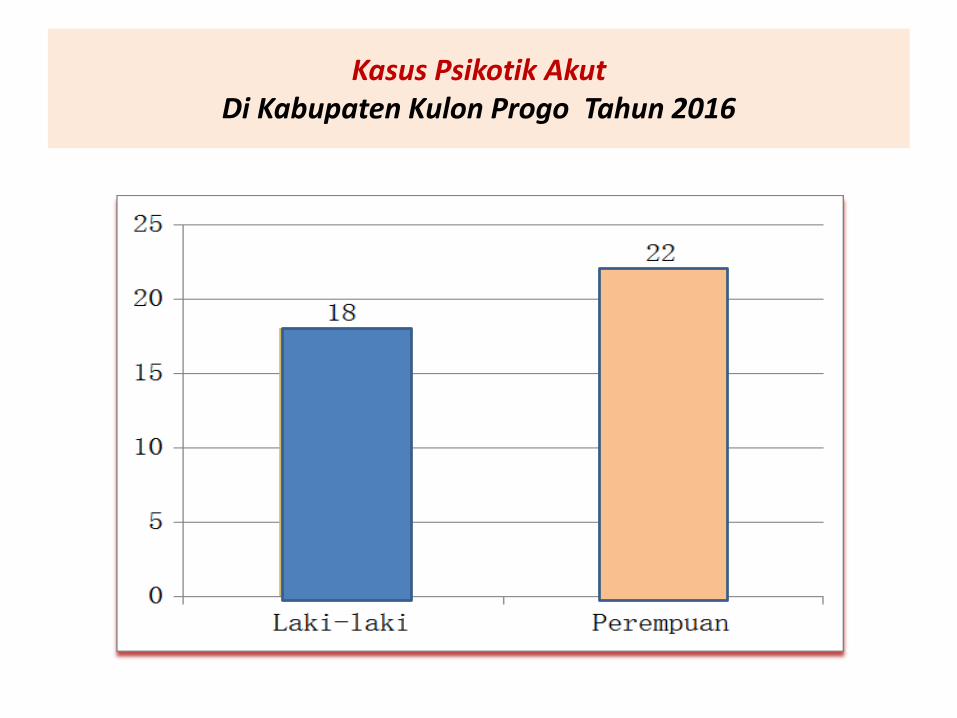
Kasus Psikotik AkutDi Kabupaten Kulon Progo Tahun 2016

Kasus Yang perlu pengawasan langsung(Risiko terjadi Pemasungan)
NO TAHUN JUMLAH
1 2014 22
2 2015 8
3 2016 16
4 2017 19
Peran Pemerintah Daerah
• Sesuai dengan UU.Keswa
• Pasal 75
Pemerintah dan Pemerintah Daerah memiliki tugas, dan tanggung jawabterhadap penyelenggaraan Upaya Kesehatan
Jiwa.
BAB VIITUGAS, TANGGUNG JAWAB, DAN WEWENANG
Pasal 761. Pemerintah dan Pemerintah Daerah bertugas dan bertanggung
jawab mengadakan komunikasi, 1nformasi, dan edukasitentang Kesehatan Jiwa kepada masyarakat secara menyeluruhdan berkesinambungan.
2. Pemerintah dan Pemerintah Daerah dalam mengadakankomunikasi, informasi, dan edukasi tentang Kesehatan Jiwasebagaimana dimaksud pada ayat (1) wajib berkoordinasidengan pemangku kepentingan.
3. Komunikasi, informasi, dan edukasi tentang Kesehatan Jiwasebagaimana dimaksud pada ayat (1) dapat diselenggarakandengan melibatkan peran serta masyarakat.
TUGAS, TANGGUNG JAWAB, DAN WEWENANG.....
Pasal 77Pemerintah dan Pemerintah Daerah bertugas dan bertanggung jawab menyediakan sarana dan prasarana dalam penyelenggaraan Upaya Kesehatan Jiwa.
Pasal 78Pemerintah dan Pemerintah Daerah bertugas dan bertanggung jawab terhadap ketersediaan dan kesejahteraan sumber daya manusia di bidang Kesehatan Jiwa.
TUGAS, TANGGUNG JAWAB, DAN WEWENANG.....
Pasal 79
(1) Pemerintah dan Pemerintah Daerah mengatur ketersediaan obat
psikofarmaka yang dibutuhkan oleh ODGJ sesuai standar.
(2) Obat psikofarmaka yang dibutuhkan oleh ODGJ sesuai standar
sebagaimana dimaksud pada ayat (1) harus tersedia secara merata
di seluruh Indonesia dengan harga terjangkau oleh masyarakat.
(3) Ketersediaan, pemerataan, dan keterjangkauan obat psikofarmaka
sebagaimana dimaksud pada ayat (2) dapat dilakukan dengan
melibatkan peran swasta.

TUGAS, TANGGUNG JAWAB, DAN WEWENANG.....
Pasal 80
Pemerintah dan Pemerintah Daerah bertanggung jawabmelakukan penatalaksanaan terhadap ODGJ yang terlantar, menggelandang, mengancam keselamatan dirinya dan/atauorang lain, dan/atau mengganggu ketertiban dan/ataukeamanan umum.
TUGAS, TANGGUNG JAWAB, DAN WEWENANG.....
Pasal 81
1. Pemerintah dan Pemerintah Daerah wajib melakukan upaya rehabilitasiterhadap ODGJ terlantar, menggelandang, mengancam keselamatan dirinya dan/atau orang lain, dan / atau mengganggu ketertiban dan/atau keamanan
umum.
2. ODGJ terlantar, menggelandang, mengancam keselamatandirinya dan/atau orang lain, dan/atau mengganggu
ketertiban dan/atau keamanan umum sebagaimanadimaksud pada ayat (1) meliputi ODGJ: a. tidak mampu;b. tidak mempunyai keluarga, wali atau pengampu;
dan/atau tidak diketahui keluarganya.
TUGAS, TANGGUNG JAWAB, DAN WEWENANG.....
Pasal 82
Pemerintah dan Pemerintah Daerah wajib melakukan
penampungan di fasilitas pelayanan di luar sektor kesehatanbagi ODGJ yang telah sembuh atau terkendali gejalanya yang tidak memiliki keluarga dan/atau terlantar.
Peraturan Gurbenur Pedoman Penanggulangan Pemasungan81/2014
Daerah Istimewa Yogyakarta
Pemerintah Daerah bertugas :
a. Membentuk Tim Pengarah Kesehatan Jiwa Masyarakat
b. Memberikan layanan serta akses komunikasi, informsi dan
edukasi yang benar kepada masyarakat tentang kesehatan jiwa
c. Mengkoordinasikan lintas program dan lintas sektoral upaya
penanggulangan pemasungan pada pihak pemangku kepentingan
d. Menyusun perencanaan, pengadaan dan peningkatan mutu,
penempatan dan pendayagunaan serta pembinaan sumber daya
manusia d bidang kesehatan
Peraturan Gurbenur Pedoman Penanggulangan Pemasungan81/2014
Daerah Istimewa Yogyakarta
e. Menyediakan akses pelayanan yang berkesinambungan meliputi
pengobatan, pemulihan, psikososial, rehabilitasi, pendampingan, dan
atau dukungan lain yang memadai untuk ODMK atau ODGJ
f. Melakukan pembinaan dan pengawasan pelaksanaan program
penanggulangan pasung kepada Pemerintah Kabupatan / Kota;
g. Menyediakan pengobatan dan perawatan ODGJ di Rumah Sakit Jiwa,
Rumah Sakit, dan Puskesmas
ODMK : orang dengan masalah kejiwaanODGJ. : Orang dengan gangguan Jiwa
Peraturan Gurbenur Pedoman Penanggulangan Pemasungan81/2014
Daerah Istimewa Yogyakarta
h. Menyediakan panti sosial untuk penempatan sementara bagi
ODGJ paska perawatan.
i. Menjamin cadangan ketersediaan obat untuk ODGJ;
j. Mencegah timbulnya stigmatisasi dan diskriminasi bagi ODGJ;
dan
k. Menyusun dan meyebarluaskan panduan praktis tentang
penanggulangan pemasungan
Peraturan Gurbenur Pedoman Penanggulangan Pemasungan81/2014
Daerah Istimewa Yogyakarta
Pemerintah Kabupaten/ kota bertugas:
a. Membentuk Tim Pelaksana Kesehatan Jiwa Masyarakat;
b. Memfasilitasi pembentukan kelompok bantu diri, forum
komunikasi, atau kelompok peduli ODGJ;
c. Menyediakan akses pelayanan yang berkesinambungan meliputi
pengobatan, pemulihan psikososial, rehabilitasi, pendampingan,
dan/ atau dukungan lainnya yang memadai bagi kepada ODMK
atau ODGJ

Peraturan Gurbenur Pedoman Penanggulangan Pemasungan81/2014
Daerah Istimewa Yogyakarta
d. Meningkatkan jumlah puskesmas yang memberikan pelayanan
kesehatan jiwa terutama untuk ODGJ;
e. Meningkatkan cakupan pelayanan kesehatan jiwa dan
ketersediaan tempat pelayanan kesehatan jiwa di rumah sakit;
f. Menjamin ketersediaan obat untuk ODGJ;
g. Menjamin ketersediaan peralatan kegawatdaruratan psikiatri

KEGIATAN UPAYA KESEHATAN JIWADI KULON PROGO
Upaya Kesehatan Jiwa dilakukan melalui kegiatan:
a. Promotif
b. Preventif
c. Kuratif
d. Rehabilitatif

PEMBENTUKAN TPKJM TINGKAT KECAMATANTAHUN 2017
NO KECAMATAN TPKJM
SUDAH BELUM
1 Temon V
2 Wates V
3 Panjatan V
4 Galur V
5 Lendah V
6 Kokap V
7 Pengasih V
8 Sentolo V
9 Girimulyo V
10 Nanggulan V
11 Kalibawang V
12 Samigaluh V

Kebijakan Pemda terhadappembiayaan pasien jiwa
1. BPJS : pemilik kartu BPJS
2. Jamkesda : penduduk Kulon Progo :
a. Pembebasan biaya layanan puskesmas bagi semua warga Kulon Progo
b. Pembiayaan rawat inap di RSUD : Rp 7.500.000 juta/orang/tahun
3. Jamkesus (Bapel jamkesos DIY) : pasien yang dirujuk ke RS Grasia dan RS dr Sarjito
DINAS KESEHATAN
1. Pertemuan TPKJM
2. Refreshing keswa bagi dokter umum Puskesmas
3. Refreshing keswa bagi pemegang program keswa
Puskesmas
4. Bimbingan teknis ke Puskesmas
5. Pertemuan surveilans keswa
6. Koordinasi penanganan kasus pasung dengan RSJGrhasia
7.Sosialisasi Pergub DIY no 81 tahun 2014 tentang Pedoman
Penanggulangan Pemasungan

PUSKESMAS
1. Deteksi dini gangguan jiwa
2. Konseling bagi penderita gangguan jiwa
3. Pengobatan bagi penderita gangguan jiwa
4. Kunjungan rumah ke penderita jiwa
5. Rujukan kasus gangguan jiwa ke RSUD Wates dan
RS Grhasia / RSUP dr. Sardjito
6. Pembentukan dan pembinaan Desa Siaga Sehat Jiwa (DSSJ)
3 desa di wilayah Puskesmas Galur II : Banaran, Kranggan,
Nomporejo

Puskesmas
7. Pelatihan kader : Puskesmas Temon I, Pengasih II, Pengasih
I, Lendah I, Galur II
8. Family Gathering : Puskesmas Galur II, Galur I
9. Self Help Group (SHG) : Puskesmas Galur II
10. Psikoedukasi : Pusk. Galur II
11. Institusi Penerima Wajib Lapor (IPWL) : Pusk. Wates
12. Rehabilitasi rawat jalan bagi pecandu NAPZA : Pusk. Temon I
Bentuk Terapi Rehabilitasi
1. Living Skills (ketrampilan hidup)
2. Learning Skills (ketrampilan belajar)
3. Working Skills (ketrampilan kerja)
RSUD WATES
1. Pengobatan penderita jiwa
2. Konseling
3. Pelayanan Psikologi
4. Rujukan ke RSJ Ghrasia / RSUP dr. Sardjito
5. Menyediakan tenaga ahli untuk transfer of knowledge
6.Bekerjasama dengan dinas kesehatan untuk melakukan
pembinaan kesehatan jiwa di masyarakat
7.Melakukan promosi kesehatan jiwa melalui kegiatan
PKMRS (Penyuluhan Kesehatan Masyarakat)
Kegiatan Promotif, Preventif,RehabilitatifRSUD Wates
PAGUYUBAN PANDAWA
• Dibentuknya beberapa kegiatan yang positif dalam
mendukung perawatan penderita gangguan jiwa
• Meningkatkan pengetahuan keluarga penderita gangguan jiwa
• Sebagai sarana promosi kesehatan jiwa kepada masyarakat
• Meningkatkan pengetahuan keluarga pasien gangguan jiwa
dalam merawat dan menghadapi pasien

PAGUYUBAN SEHAT JIWA PANDAWARSUD – WATES
Mulai Tahun 2012

Kegiatan Penyuluhan Jiwadi Lingkungan RSUD-Wates
KEGIATAN KUNJUNGAN RUMAHRSUD-WATES
• Dilakukan pada pasien yang mengalami berbagai hambatan dalam pengobatan

PROGRAM 100 HARI KERJA BUPATI
KULON PROGO BEBAS PASUNG

Kasus Pasung Bp. D (Pusk. Lendah II)

Kasus Pasung Bp M(Pusk. Pengasih II)

Kasus Pasung Bp R (Pusk. Wates)

Kasus Pasung Bp. S (Pusk. Kalibawang)
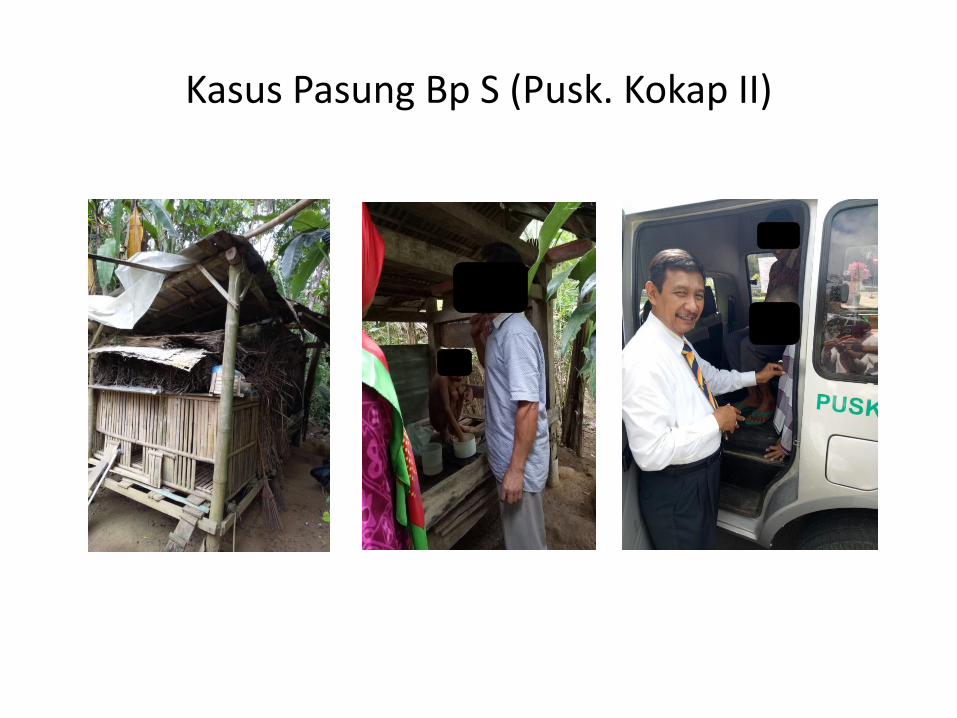
Kasus Pasung Bp S (Pusk. Kokap II)

Kasus Pasung Bp S (Pusk Lendah I)

Kasus Pasung Ny. S (Pusk Nanggulan)

Kasus Pasung Bp T (Pusk Girimulyo II)
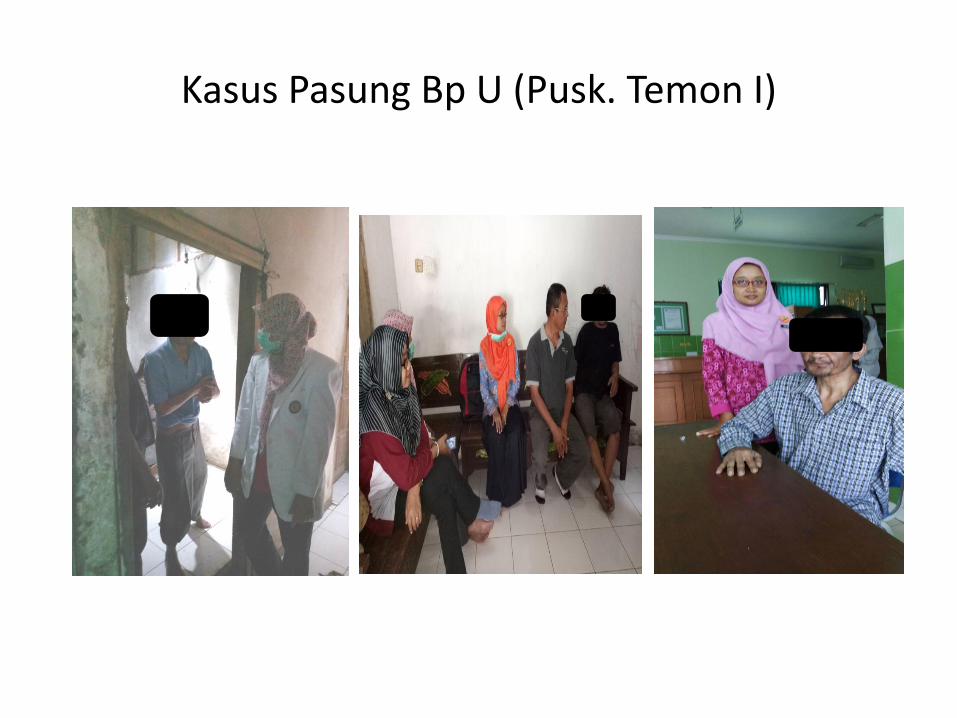
Kasus Pasung Bp U (Pusk. Temon I)

KEGIATAN EVALUASI BEBAS PASUNG

BHAKTI SOSIAL HKN KE ODGJ PASCA PASUNG (20-10-2017)
RUJUKAN ODGJ KE RSJ GRHASIA OLEH TPKJM KEC KALIBAWANG ( 3-11-2017)

KEGIATAN KESWA TH 2017
NO KEGIATAN FREKUENSI SUMBER DANA
1 Rakor & pembinaan keswa 2 kali APBD II
2 Rakor NAPZA 2 kali APBD II
3 Sosialisasi NAPZA 1 kali APBD II
4 Sosialisasi keswa 1 kali APBD II
5 Bimtek keswa 4 kali APBD II
6 Konsultasi ke Dinkes DIY 7 kali APBD II
7 Konsultasi ke Kemenkes 1 kali APBD II
8 Workshop deteksi dini gg. jiwa 1 kali DAK NON FISIK
9 Evaluasi Target Bebas Pasung 1 kali DAK NON FISIK
10 Sosialisasi RBM 1 kali/2 Puskesmas
APBD I
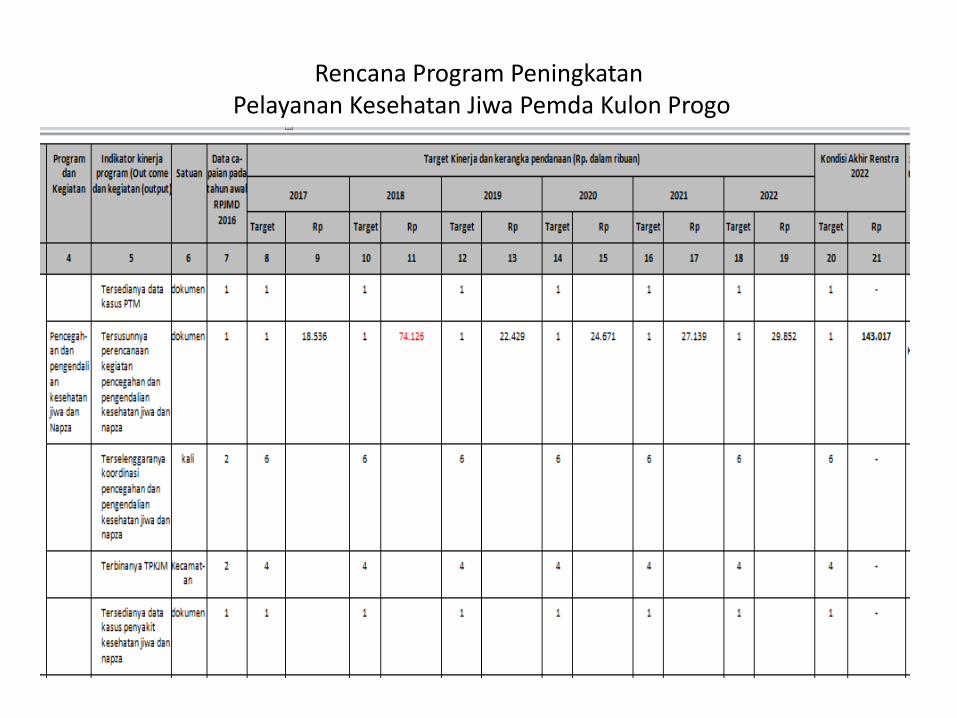
Rencana Program PeningkatanPelayanan Kesehatan Jiwa Pemda Kulon Progo
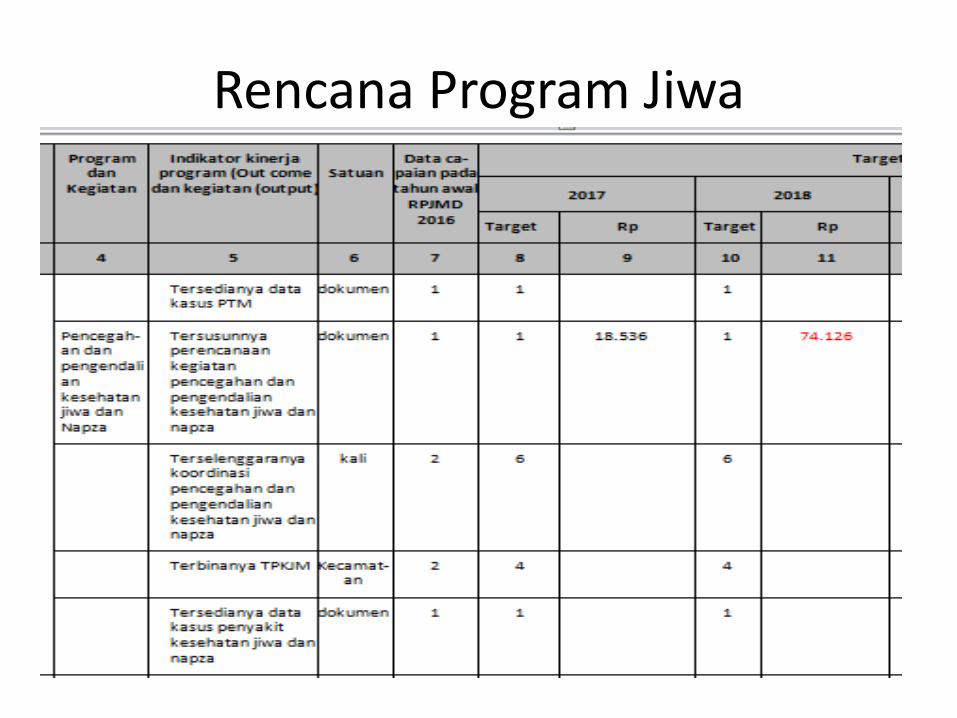
Rencana Program Jiwa
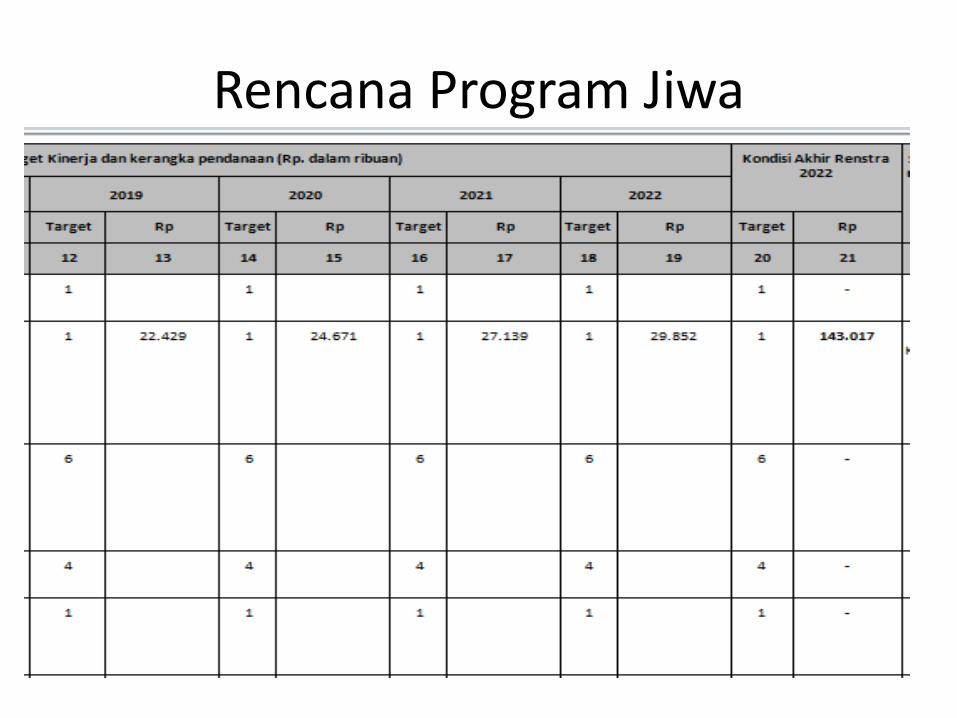
Rencana Program Jiwa

KESIMPULAN
• Upaya kesehatan jiwa harus diselenggarakan secara terintegrasi, komprehensif dan berkesinambungan oleh Pemerintah, Pemda, dan Masyarakat agar dapat tercapai terwujudnya derajat kesehatan yang setinggi-tingginya
Langkah-langkah Pencegahan(Prevention approach and
evidence based information about mental heath treatments)

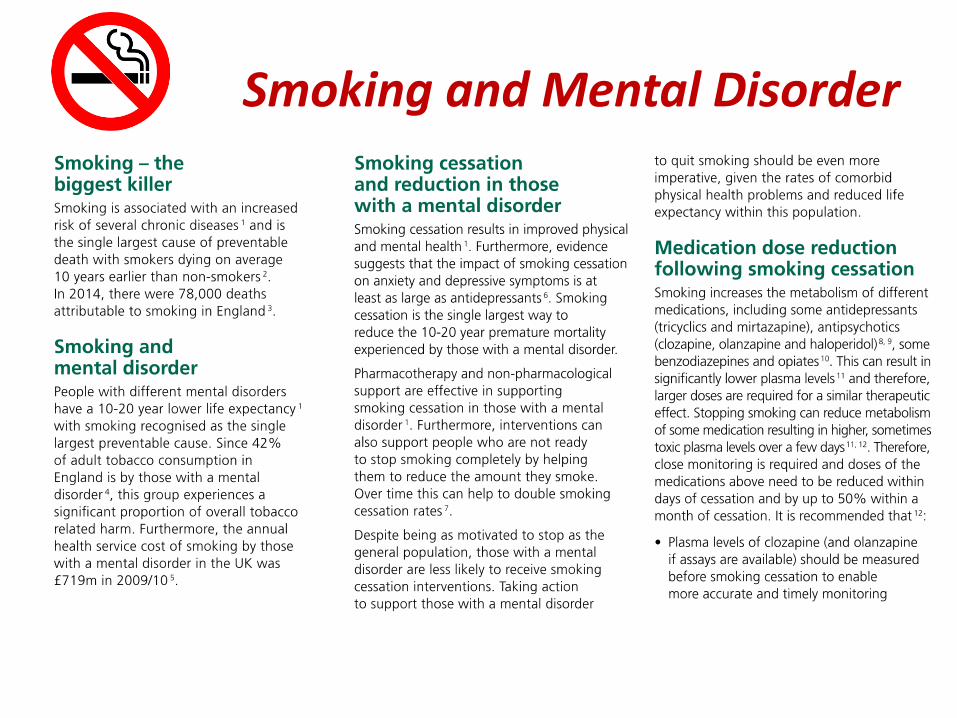
Smoking and Mental Disorder

Indonesia's smoking epidemic 0 an old problem gett ingyounger
Kate Hodal in Jakarta
A cloud of smoke hovers above his small f rame, a cigarette dangling at his l ips. As he blows
rings high above his head, 14-year-old Faisan explains why he has just bought his third
cigarette of the day. "When I have a problem to solve – and I have so many problems at
school – I have a smoke," he says. "It relaxes me and makes me forget."
In most other countries, the fact Faisan is an underage and regular smoker would be
start l ing. But in Indonesia, he is but one of thousands across the archipelago – a nat ion of
islands where nearly 70% of men aged 20 and over smoke, and where the average start ing
age has fallen f rom 19 a decade ago to just seven today, act iv ists say.
There is no minimum age limit on smoking or buying cigarettes in Indonesia, which
explains why videos of smoking Indonesian t oddlers exist on YouTube – such as that of two-
year-old Sumatran Ardi Rizal, who regularly smoked 40 cigarettes a day before undergoing
treatment.
Many male smokers now start their habit at age seven, with activists blaming weak
regulations and the tobacco industry
Thu 22 Mar 20 12 16.39 GMT
Indonesia's smoking epidemic 0 an old problem gett ingyounger
Kate Hodal in Jakarta
A cloud of smoke hovers above his small f rame, a cigaret te dangling at his l ips. As he blows
rings high above his head, 14-year-old Faisan explains why he has just bought his third
cigarette of the day. "When I have a problem to solve – and I have so many problems at
school – I have a smoke," he says. "It relaxes me and makes me forget."
In most other countries, the f act Faisan is an underage and regular smoker would be
start l ing. But in Indonesia, he is but one of thousands ac ross the archipelago – a nat ion of
islands where nearly 70% of men aged 20 and over smoke, and where the average start ing
age has fallen f rom 19 a decade ago to just seven today, act iv ists say.
There is no minimum age l imit on smoking or buy ing cigarettes in Indonesia, which
explains why v ideos of smoking Indonesian t oddlers exist on YouTube – such as that of two-
year-old Sumatran Ardi Rizal, who regularly smoked 40 cigarettes a day before undergoing
treatment.
Many male smokers now start their habit at age seven, with activists blaming weak
regulations and the tobacco industry
Thu 22 Mar 20 12 16.39 GMT
Indonesia's smoking epidemic 0 an old problem gett ingyounger
Kate Hodal in Jakarta
A cloud of smoke hovers above his small f rame, a cigarette dangling at his l ips. As he blows
rings high above his head, 14-year-old Faisan explains why he has just bought his third
cigarette of the day. "When I have a problem to solve – and I have so many problems at
school – I have a smoke," he says. "It relaxes me and makes me forget."
In most other countries, the fact Faisan is an underage and regular smoker would be
start l ing. But in Indonesia, he is but one of thousands across the archipelago – a nat ion of
islands where nearly 70% of men aged 20 and over smoke, and where the average start ing
age has fallen f rom 19 a decade ago to just seven today, act ivists say.
There is no minimum age limit on smoking or buying cigarettes in Indonesia, which
explains why videos of smoking Indonesian t oddlers exist on YouTube – such as that of two-
year-old Sumatran Ardi Rizal, who regularly smoked 40 cigarettes a day before undergoing
treatment.
Many male smokers now start their habit at age seven, with activists blaming weak
regulations and the tobacco industry
Thu 22 Mar 20 12 16.39 GMT
Too Young

Too Poor to SmokeThis does not fit between desire and ability
Can not afford health insurance (BPJS) that is only 50 thousand rupiah per month
But ironically able to pay a cigarette that is expensive 300 thousand rupiah per monthThis is unmet need .with a reason to get happiness because the poor can be happy only through smokingThey say: "I do not have luxury homes, luxury cars and can not eat well and recreation"

Cigarettes contributed povertyNews : Kompas daily national Media ( July 2017)
We know almost half the population of Indonesia survives on less than US $ 1 a dayBut cigarettes are the second largest household expenditure
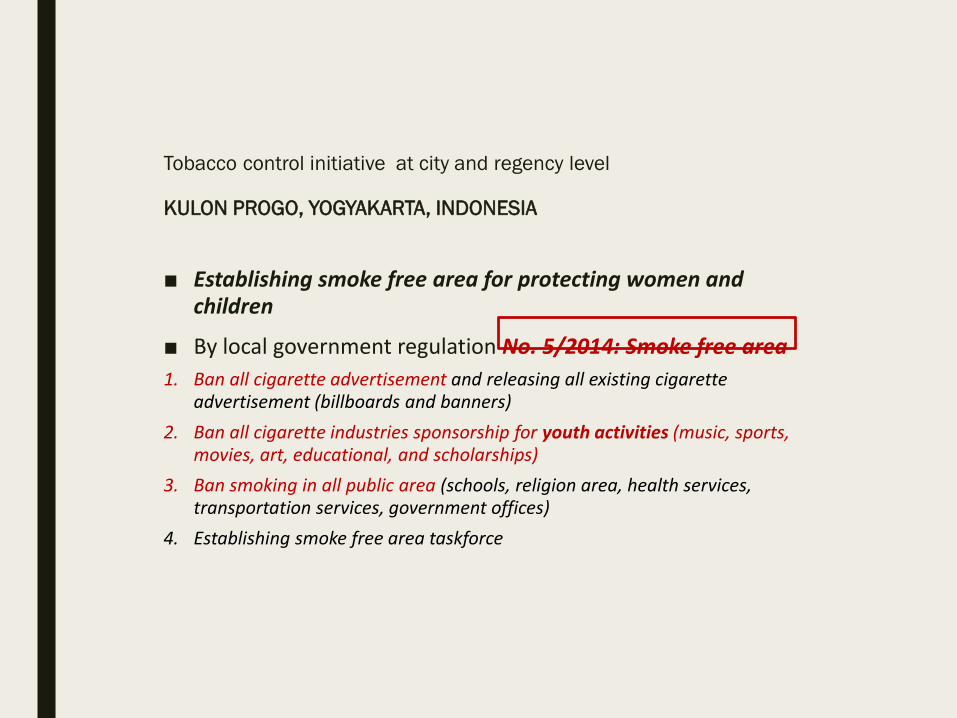
Tobacco control initiative at city and regency level
KULON PROGO, YOGYAKARTA, INDONESIA
■ Establishing smoke free area for protecting women and children
■ By local government regulation No. 5/2014: Smoke free area
1. Ban all cigarette advertisement and releasing all existing cigarette advertisement (billboards and banners)
2. Ban all cigarette industries sponsorship for youth activities (music, sports, movies, art, educational, and scholarships)
3. Ban smoking in all public area (schools, religion area, health services, transportation services, government offices)
4. Establishing smoke free area taskforce

RELEASING AND REPLACING CIGARETTE ADVERTISEMENT
. Replacing Cigarette advertisement with health promotion baliho

Perda Kulon Progo No. 5 tahun 2014 tentang KTR
(Kawasan Tanpa Rokok)
Tabel 1. Total Pengeluaran Rumah Tangga Setahun Menurut Jenis Pengeluaran dan Quintile Pengeluaran Rumah Tangga di Kulon
Progo Tahun 2013
Jenis PengeluaranQuintile Pengeluaran Rumah Tangga per Tahun (Rp)
JumlahQuintile 1 Quintile 2 Quintile 3 Quintile 4 Quintile 5
(1) (2) (3) (4) (5) (6) (7)
A Makanan103,537,507,01
1
176,229,109,10
5
228,780,039,51
3289,057,089,708 469,691,663,518 1,267,295,408,855
B Non makanan 48,716,976,452 88,315,402,667113,726,446,78
5195,416,103,888 571,419,273,203 1,017,594,202,995
CTotal
pengeluaran
152,254,483,46
2
264,544,511,77
1
342,506,486,29
8484,473,193,595
1,041,110,936,72
22,284,889,611,848
1 Alkohol 0 0 0 0 82,403,316 82,403,316
2 Rokok 3,400,824,210 9,968,989,473 14,701,749,087 21,094,943,319 47,408,918,301 96,575,424,390
3 Sirih 1,989,433,539 2,182,530,305 1,851,662,403 2,556,307,557 1,332,105,162 9,912,038,966
4 Pendidikan 1,933,617,367 6,414,686,580 9,481,439,275 14,319,339,737 60,864,290,035 93,013,372,994
5 Kesehatan 1,954,889,538 7,476,080,984 4,765,496,854 15,351,421,831 43,132,818,824 72,680,708,031
6 Pulsa 1,842,256,763 4,067,417,213 5,574,301,868 9,946,649,874 28,430,289,195 49,860,914,913
Sumber: Survei Sosial Ekonomi Nasional (SUSENAS) 2013, BPS
Tahun 2013 Meningkat(Orang miskin hidup boros : Rokok & Pulsa Dominan)

Program pencegahan merokokDi sekolah
Kerjasama Pemda Kulon Progo dan Nanyang University

HASIL SURVEISubyek 1408 siswa kelas 7 di 36 SMP

HASIL SURVEISubyek 1408 siswa kelas 7 di 36 SMP

Tobacco control initiative at city level
KULON PROGO, YOGYAKARTA, INDONESIA
Target Total Smoke Free
Area
%
Public health 21 21 100
Hospital 6 6 100
Elementary school 368 368 100
Religious facilities 1276 854 67
Government offices 46 36 74
Sub villages 937 16 2
This is the result data of the local regulations implementation in Kulonprogo
In the schools and health facilities more easily but in other places still need a
struggle

Treatment For Gambling Disorder
4
MEDICATION Naltrexone can be used to reduce gambling severity in problem gamblers. It should
be prescribed by an experienced practitioner, with appropriate skills and training, and careful consideration must be given within the clinical encounter to
contraindications. Antidepressant medication should not be used to reduce gambling severity in
people presenting with problem gambling alone. It is however appropriate to prescribe Selective Serotonin Re-uptake Inhibitors (SSRIs) in people with comorbid
depression and gambling disorder, but there is no evidence that this improves gambling outcomes. RECOMMENDATIONS
The Royal College of Psychiatrists recommends the following:
1. Randomised controlled trials assessing the impact of psychological therapies and medication should be conducted in the UK rather than allowing US-based
studies alone to inform clinical practice. The experiences of gambling-related harm and the use of gambling-related products and treatment provision differ widely from country to country, so it would be preferable to base
national recommendations on UK-based research.
2. Gambling disorder is a mental disorder that needs to be regarded as an addiction like any other, with significant levels of harm to the individual and to society. Treatment services for problem gambling should have parity of
esteem with other mental disorders, in particular alcohol, drug and tobacco addiction, and should be a core element of addictions treatment provision
within the NHS.
3. Naltrexone, as the treatment intervention of choice for treatment-resistant
pathological gamblers, should be made available to all patients whose lives are affected negatively by their illness.
4. NICE Guidelines for the treatment of gambling disorder are required to
address a pathology that affects almost half a million people in England but has not been sufficiently prioritised by the NHS.
5. Training in identifying and treating problem gambling symptoms should be a component of all medical school curricula and the postgraduate psychiatry
training curriculum.
December 2016

Improving the lives of people with mental illness
Treatments and wellbeing
Readable, user friendly and evidence based information about mental health
treatments.
A | B | C | D | E | F | G | H | I | J | K | L | M | N | O | P | Q | R | S | T | U | V | W
| X | Y | Z
A
Alzheimer's: Drug treatments in Alzheimer's
Antidepressants
Antidepressants: key facts
Antidepressants – coming off antidepressants
Antipsychotics
B
Being Seen and Heard: CD ROM
Benzodiazepines
C
Caring for young carers
Caring around the Clock: Booklet with information and support for young people who care for others
Checklist for carers of people with mental health problems: a leaflet for carers
Checklist for parents with children with mental health problems: a leaflet for carers
Checklist for people with mental health problems: a leaflet for carers
Checklist for professionals coming into contact with children of parents with mental health
problems: a leaflet for carers
Checklist for psychiatrists: a leaflet for carers
Cognitive Behavioural Therapy
Cognitive Behavioural Therapy (CBT): information for young people
Eating Disorder
Good Parenting Approach(Pengasuhan)

Therapeutic approaches
5Royal College of Psychiatrists
Executive summary and recommendations
Eating disorders are serious mental disorders with high levels of physical and psychological comorbidity, disability and mortality. Two previous Royal College of Psychiatrists surveys of services for patients with eating disorders were published in 1992 (Council Report CR14) and 2000 (Council Report CR87). Both identified poor provision of specialist eating disorder services and that patients often had to travel long distances from home for treatment.
To review national provision for eating disorders, a further survey was undertaken of services providing specialist treatment for patients with eating disorders in the UK and the Republic of Ireland, including services for children, adolescents and adults in the National Health Service (NHS) and the private sector. Services for obesity were not surveyed. Overall, 83 services from all parts of the UK and Ireland participated; 62 (75%) were NHS services. This is an increase in the number of services compared with the earlier reports. Twenty-three services catered for both children and adolescents; 23 for adolescents only; 7 for children and adults (including one treating 13- to 25-year-olds); and 29 for adults only. One service did not provide information on the age range of people treated.
The majority of services were led by a consultant psychiatrist (82%). Multidisciplinary teams included a wide range of health professionals, most commonly specialist nurses (81%) and clinical psychologists (76%); 54% of teams had a dietician, 51% had a psychotherapist, 49% had a social worker and 47% an occupational therapist.
Therapeutic approaches used by services most often were:
� for anorexia nervosa – individual cognitive–behavioural therapy (CBT) (84%), nutritional advice and monitoring (82%) and family-based treatment (77%)
� for bulimia nervosa – individual CBT (79%), self-help literature (67%) and selective serotonin-reuptake inhibitors (SSRIs) (65%)
� for binge eating disorder – self-help interventions (58%), nutritional advice and monitoring (54%) and individual CBT (54%)
� for eating disorder not otherwise specified (EDNOS) – individual CBT (67%), nutritional advice and monitoring (62%) and self-help interventions (54%)
� for in-patients – nutritional advice and monitoring (63%), individual CBT (58%) and anxiety management/relaxation (54%).
Of 447 in-patient beds identified in the UK (226 NHS, 221 private sector), 330 (74%) were in specialist units (166 NHS, 164 private sector).
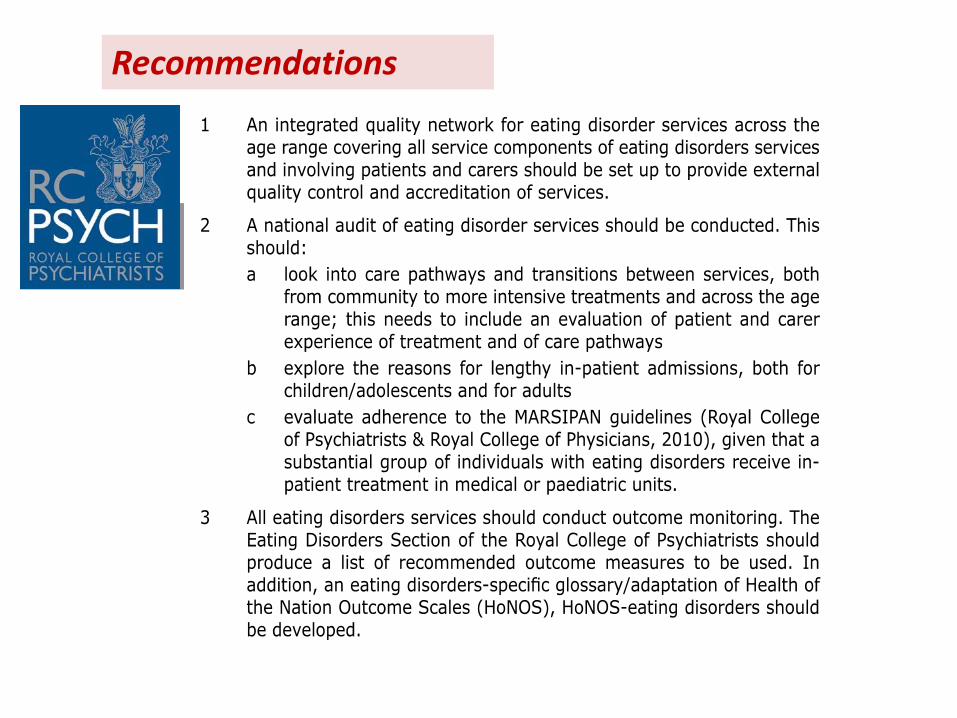
Recommendations

Improving the lives of people with mental illness
Cognitive Behavioural Therapy
This leaflet is for anyone who wants to know more about Cognitive Behavioural Therapy (CBT). It
discusses how it works, why it is used, its effects, its side-effects, and
alternative treatments. If you can't find what you want here, there are
sources of further information at the end of this leaflet.
What is CBT?
It is a way of talking about:
how you think about yourself, the world and other people
how what you do affects your thoughts and feelings.
CBT can help you to change how you think ('Cognitive') and what you
do ('Behaviour'). These changes can help you to feel better. Unlike some
of the other talking treatments, it focuses on the 'here and now'
problems and difficulties. Instead of focusing on the causes of your
distress or symptoms in the past, it looks for ways to improve your state of mind now.
When does CBT help?
CBT has been shown to help with many different types of problems. These include: anxiety, depression,
panic, phobias (including agoraphobia and social phobia), stress, bulimia, obsessive compulsive
disorder, post-traumatic stress disorder, bipolar disorder and psychosis. CBT may also help if you have
difficulties with anger, a low opinion of yourself or physical health problems, like pain or fatigue.
How does it work?
CBT can help you to make sense of overwhelming problems by breaking them down into smaller parts.
This makes it easier to see how they are connected and how they affect you. These parts are:
A Situation - a problem, event or difficult situation. From this can follow:
Thoughts
Emotions
Physical feelings
Actions
Each of these areas can affect the others. How you think about a problem can affect how you feel
physically and emotionally.
Improving the lives of people with mental illness
Cognitive Behavioural Therapy
This leaflet is for anyone who wants to know more about Cognitive Behavioural Therapy (CBT). It
discusses how it works, why it is used, its effects, its side-effects, and
alternative treatments. If you can't find what you want here, there are
sources of further information at the end of this leaflet.
What is CBT?
It is a way of talking about:
how you think about yourself, the world and other people
how what you do affects your thoughts and feelings.
CBT can help you to change how you think ('Cognitive') and what you
do ('Behaviour'). These changes can help you to feel better. Unlike some
of the other talking treatments, it focuses on the 'here and now'
problems and difficulties. Instead of focusing on the causes of your
distress or symptoms in the past, it looks for ways to improve your state of mind now.
When does CBT help?
CBT has been shown to help with many different types of problems. These include: anxiety, depression,
panic, phobias (including agoraphobia and social phobia), stress, bulimia, obsessive compulsive
disorder, post-traumatic stress disorder, bipolar disorder and psychosis. CBT may also help if you have
difficulties with anger, a low opinion of yourself or physical health problems, like pain or fatigue.
How does it work?
CBT can help you to make sense of overwhelming problems by breaking them down into smaller parts.
This makes it easier to see how they are connected and how they affect you. These parts are:
A Situation - a problem, event or difficult situation. From this can follow:
Thoughts
Emotions
Physical feelings
Actions
Each of these areas can affect the others. How you think about a problem can affect how you feel
physically and emotionally.
Improving the lives of people with mental illness
Cognitive Behavioural Therapy
This leaflet is for anyone who wants to know more about Cognitive Behavioural Therapy (CBT). It
discusses how it works, why it is used, its effects, its side-effects, and
alternative treatments. If you can't find what you want here, there are
sources of further information at the end of this leaflet.
What is CBT?
It is a way of talking about:
how you think about yourself, the world and other people
how what you do affects your thoughts and feelings.
CBT can help you to change how you think ('Cognitive') and what you
do ('Behaviour'). These changes can help you to feel better. Unlike some
of the other talking treatments, it focuses on the 'here and now'
problems and difficulties. Instead of focusing on the causes of your
distress or symptoms in the past, it looks for ways to improve your state of mind now.
When does CBT help?
CBT has been shown to help with many different types of problems. These include: anxiety, depression,
panic, phobias (including agoraphobia and social phobia), stress, bulimia, obsessive compulsive
disorder, post-traumatic stress disorder, bipolar disorder and psychosis. CBT may also help if you have
difficulties with anger, a low opinion of yourself or physical health problems, like pain or fatigue.
How does it work?
CBT can help you to make sense of overwhelming problems by breaking them down into smaller parts.
This makes it easier to see how they are connected and how they affect you. These parts are:
A Situation - a problem, event or difficult situation. From this can follow:
Thoughts
Emotions
Physical feelings
Actions
Each of these areas can affect the others. How you think about a problem can affect how you feel
physically and emotionally.
Rekomendasi dari RC PSYCH

Perencanaan (perumahanlLH) KotaBerwawasan Kesehatan

Perencanaan (perumahanlLH) KotaBerwawasan Kesehatan

....Bedah Rumah murni Gotong Royong
tanpa APBD di Kulonprogo
Angka Harapan Hidup di KP tertinggi 75 tahun