fisiologi jantung
DESCRIPTION
ppt tugas individu untuk presentasi tutorial blok Cardio Vaskular System, FKUPN Veteran jakartaTRANSCRIPT

Physiology of The HeartPhysiology of The Heart
Cecep kurnia.sCecep kurnia.s11102110671110211067
Fakultas Kedokteran UPN Veteran JakartaFakultas Kedokteran UPN Veteran Jakarta
Lauralee Sherwood,Lauralee Sherwood, Human Physiology: From Cells to Human Physiology: From Cells to
Systems,Systems,77thth Ed, 2010 Ed, 2010
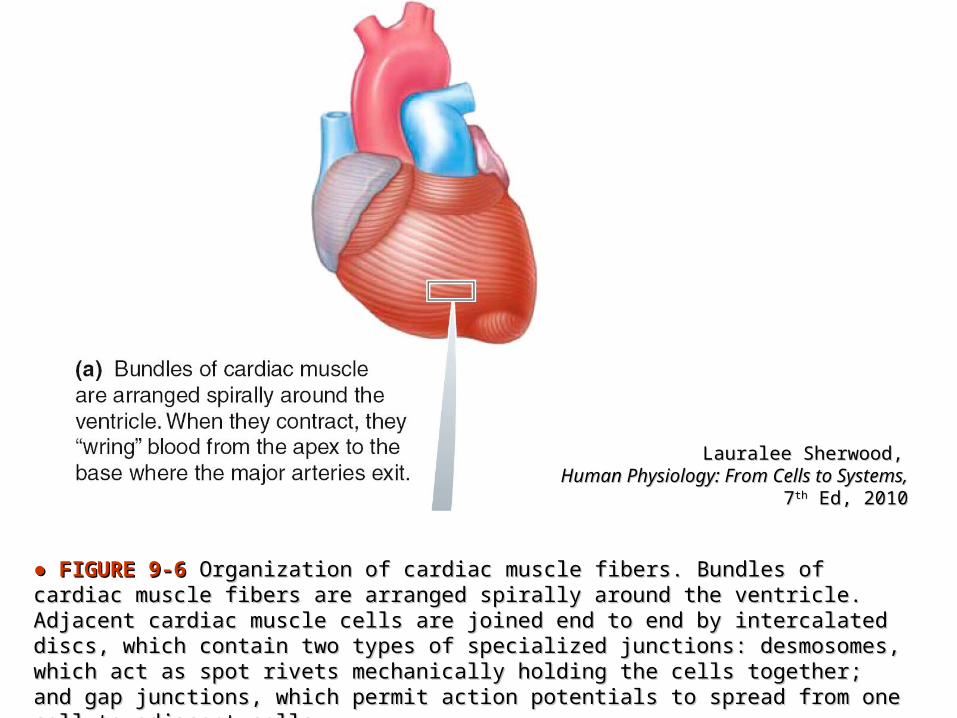
● ● FIGURE 9-6FIGURE 9-6 Organization of cardiac muscle fibers. Bundles of cardiac muscle Organization of cardiac muscle fibers. Bundles of cardiac muscle fibers are arranged spirally around the ventricle. Adjacent cardiac muscle cells fibers are arranged spirally around the ventricle. Adjacent cardiac muscle cells are joined end to end by intercalated discs, which contain two types of are joined end to end by intercalated discs, which contain two types of specialized junctions: desmosomes, which act as spot rivets mechanically holding specialized junctions: desmosomes, which act as spot rivets mechanically holding the cells together; and gap junctions, which permit action potentials to spread the cells together; and gap junctions, which permit action potentials to spread from one cell to adjacent cells.from one cell to adjacent cells.

Anatomi-Fisiologi Otot Jantung
• Miokardium:- otot atrium- otot ventrikel- serat otot khusus: sistem eksitasi otot jantung
• Otot tak sadar• Cara kontraksi: mirip otot rangka
• Singsisium
Lauralee Sherwood,Lauralee Sherwood, Human Physiology: From Cells to Human Physiology: From Cells to
Systems,Systems,77thth Ed, 2010 Ed, 2010
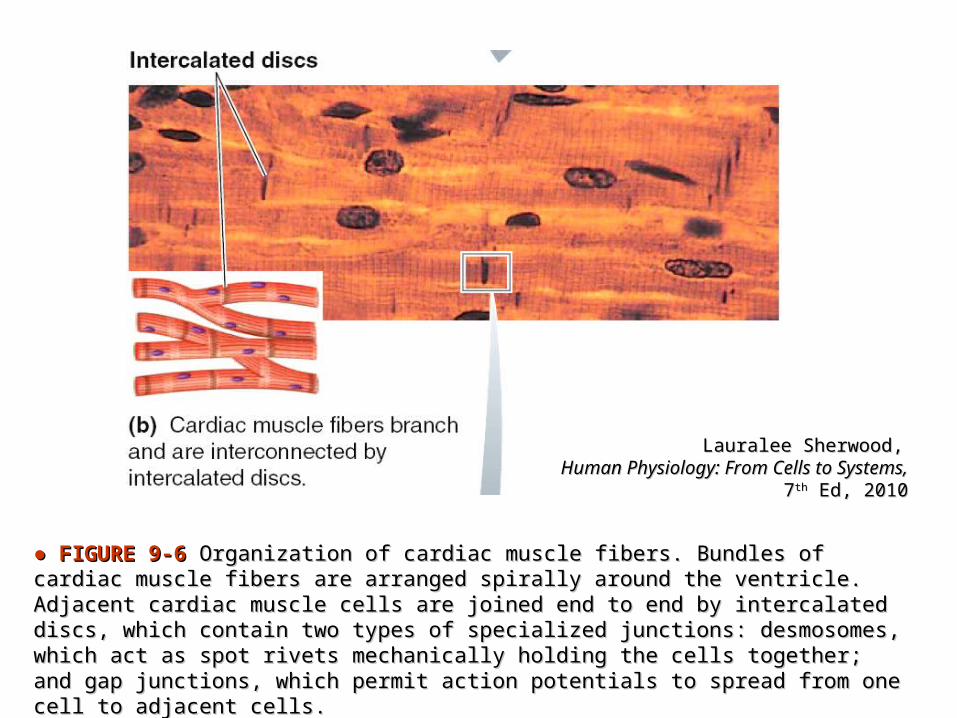
● ● FIGURE 9-6FIGURE 9-6 Organization of cardiac muscle fibers. Bundles of cardiac muscle Organization of cardiac muscle fibers. Bundles of cardiac muscle fibers are arranged spirally around the ventricle. Adjacent cardiac muscle cells fibers are arranged spirally around the ventricle. Adjacent cardiac muscle cells are joined end to end by intercalated discs, which contain two types of are joined end to end by intercalated discs, which contain two types of specialized junctions: desmosomes, which act as spot rivets mechanically holding specialized junctions: desmosomes, which act as spot rivets mechanically holding the cells together; and gap junctions, which permit action potentials to spread the cells together; and gap junctions, which permit action potentials to spread from one cell to adjacent cells.from one cell to adjacent cells.

Struktur Otot Jantung
• Sarkolema
• Miofibril
• Filamen: - Aktin- Miosin
• Sarkoplasma
• Retikulum sarkoplasmik

Struktur Otot Jantung

Lauralee Sherwood,Lauralee Sherwood, Human Physiology: From Cells to Human Physiology: From Cells to
Systems,Systems,77thth Ed, 2010 Ed, 2010
● ● FIGURE 9-6FIGURE 9-6 Organization of cardiac muscle fibers. Bundles of cardiac muscle Organization of cardiac muscle fibers. Bundles of cardiac muscle fibers are arranged spirally around the ventricle. Adjacent cardiac muscle cells fibers are arranged spirally around the ventricle. Adjacent cardiac muscle cells are joined end to end by intercalated discs, which contain two types of are joined end to end by intercalated discs, which contain two types of specialized junctions: desmosomes, which act as spot rivets mechanically holding specialized junctions: desmosomes, which act as spot rivets mechanically holding the cells together; and gap junctions, which permit action potentials to spread the cells together; and gap junctions, which permit action potentials to spread from one cell to adjacent cells.from one cell to adjacent cells.

Despopoulos, Color Atlas of Physiology 5Despopoulos, Color Atlas of Physiology 5THTH ed © 2003 Thieme ed © 2003 Thieme

AKTIVITAS LISTRIK JANTUNG
• Sel otoritmik• Sel Kontraktil (Miokardium)


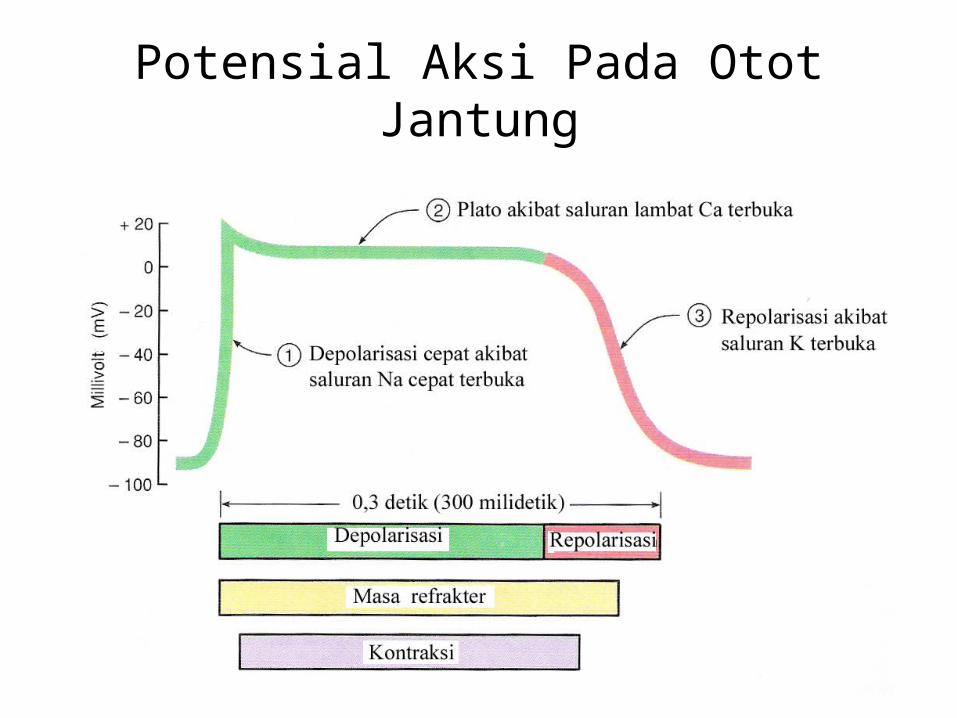
Potensial Aksi Pada Otot Jantung
• Polarisasi
• Depolarisasi: - Plato
- Ritmisitas
• Repolarisasi
• Kecepatan konduksi
• Masa Refrakter

Potensial Aksi Pada Otot Jantung
Potensial Aksi Pada Otot Jantung
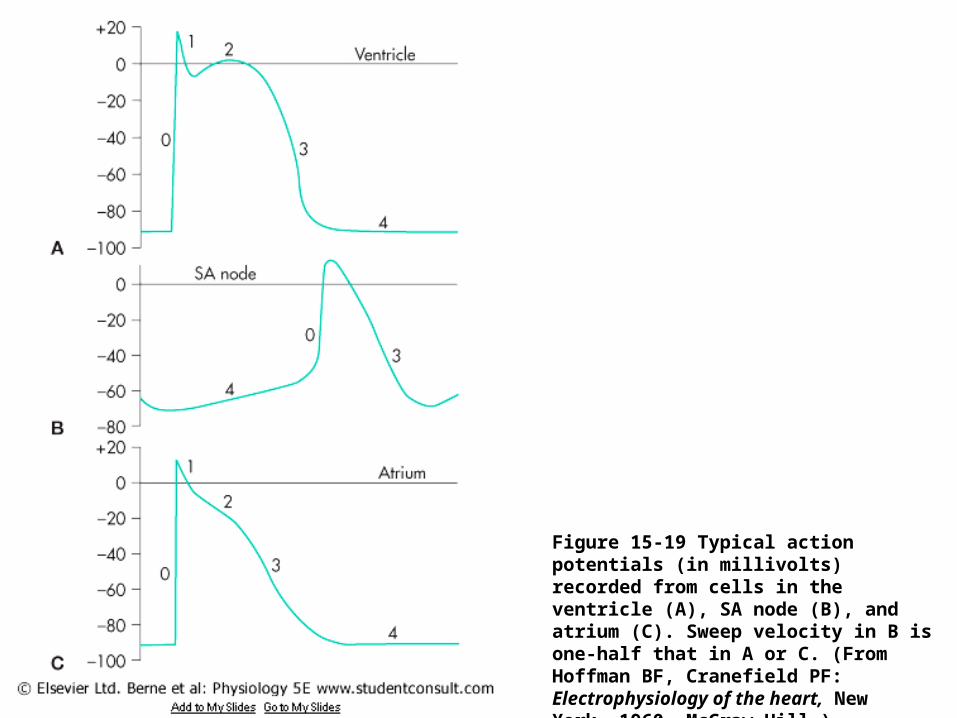
Figure 15-19 Typical action potentials (in millivolts) recorded from cells in the ventricle (A), SA node (B), and atrium (C). Sweep velocity in B is one-half that in A or C. (From Hoffman BF, Cranefield PF: Electrophysiology of the heart, New York, 1960, McGraw-Hill.)
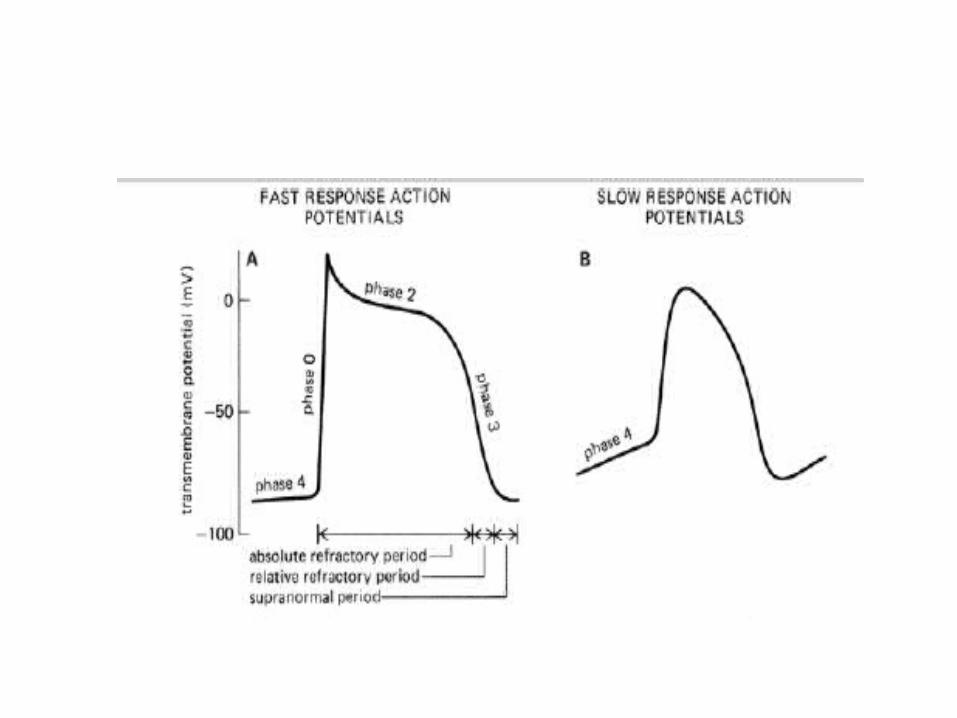

Figure 2–2. Figure 2–2. Action potentials from these cell types are referred to as "fast Action potentials from these cell types are referred to as "fast response" and "slow response" action potentials, respectively.response" and "slow response" action potentials, respectively.
• Panel A: fast response action potentials are characterized by Panel A: fast response action potentials are characterized by a rapid depolarization (phase 0) with a substantial overshoot a rapid depolarization (phase 0) with a substantial overshoot
(positive inside voltage), (positive inside voltage), a rapid reversal of the overshoot potential (phase 1), a rapid reversal of the overshoot potential (phase 1), a long plateau (phase 2), a long plateau (phase 2), and a repolarization (phase 3)and a repolarization (phase 3) a stable, high (ie, large negative) resting membrane potential a stable, high (ie, large negative) resting membrane potential
(phase 4). (phase 4).
• Panel B: the slow response action potentials are characterized Panel B: the slow response action potentials are characterized by a slower initial depolarization phase, a lower amplitude by a slower initial depolarization phase, a lower amplitude overshoot, a shorter and less stable plateau phase, and a overshoot, a shorter and less stable plateau phase, and a repolarization to an unstable, slowly depolarizing "resting" repolarization to an unstable, slowly depolarizing "resting" potential. The unstable resting potential seen in pacemaker cells potential. The unstable resting potential seen in pacemaker cells with slow response action potentials is variously referred to as with slow response action potentials is variously referred to as the the phase 4 depolarization, diastolic depolarization,phase 4 depolarization, diastolic depolarization, or or pacemaker potential.pacemaker potential.

Figure 10–2Figure 10–2Rhythmical discharge of a Rhythmical discharge of a sinus nodal fiber. sinus nodal fiber. Also, the sinus nodal action potential is Also, the sinus nodal action potential is compared with that of a ventricular muscle fiber.compared with that of a ventricular muscle fiber.
Guyton & Hall: Textbook of Med Physiol 11Guyton & Hall: Textbook of Med Physiol 11thth ed, 2006ed, 2006

● ● FIGURE 9-8 FIGURE 9-8 Specialized conduction system of the heart and spread of cardiac Specialized conduction system of the heart and spread of cardiac excitation.excitation.
Human Physiology: Human Physiology: From Cells to Systems,From Cells to Systems,
Seventh Edition, Seventh Edition, Lauralee Sherwood, 2010Lauralee Sherwood, 2010


Impulse TransmissionImpulse Transmission
AV delayAV delayAV node conduction:AV node conduction: 0.09 sec0.09 secPenetrating portion of AV bundle:Penetrating portion of AV bundle: 0.04 sec0.04 sec------------------------------------------------------------------------
PR segment PR segment 0.13 sec0.13 sec Atrial impulse conductionAtrial impulse conduction
SA node SA node Internodes Internodes AV node: AV node: 0.03 sec0.03 sec------------------------------------------------------------------------
PR interval PR interval 0.16 sec0.16 sec

AV Node – Slow ConductionAV Node – Slow Conduction
Small cellsSmall cellsThin cell membrane Thin cell membrane slow conduction velocity slow conduction velocity
Resting EResting Em < m < Myocardium Myocardium resting Eresting Em m
Small amplitude of action potentialSmall amplitude of action potential slow slow conduction conduction velocityvelocity
Few intercalated discFew intercalated discGreat intercellular electrical resistance Great intercellular electrical resistance slow slow conduction conduction velocityvelocity


Human Physiology: Human Physiology: From Cells to Systems,From Cells to Systems,
Seventh EditionSeventh EditionLauralee Sherwood, 2010Lauralee Sherwood, 2010

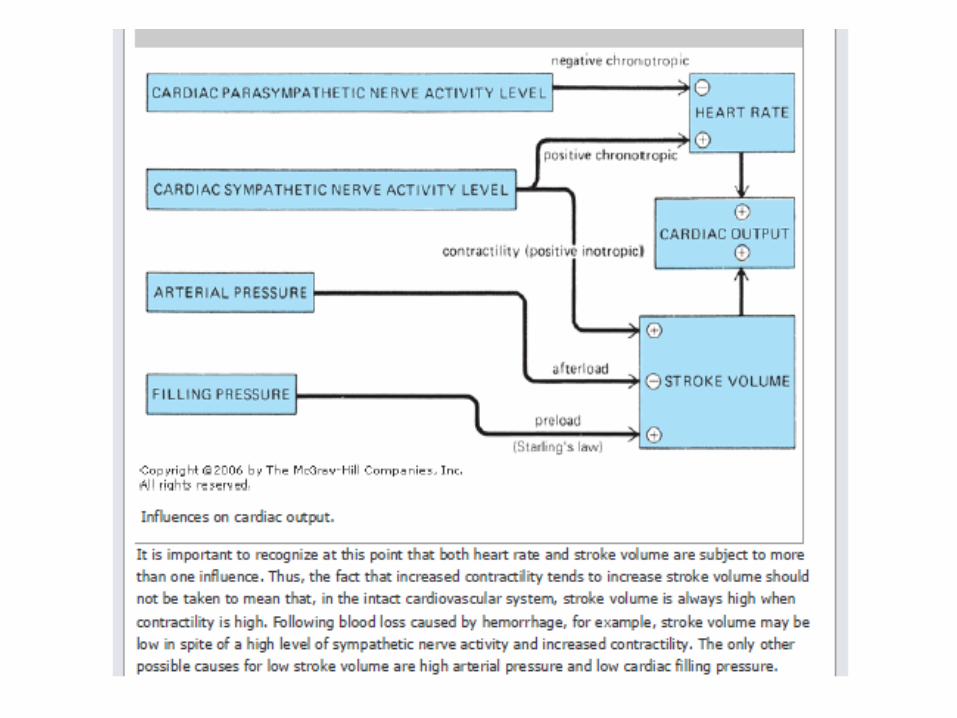
Cardiac OutputDefinisi : volume darah yang dipompa oleh masing2 ventrikel per menit
Cardiac Output dipengaruhi 2 faktor :
- Stroke Volume = volume darah yang dipompa per denyut- Heart Rate = denyut jantung per menit
Cardiac Output = SV x HRCO = 70 ml/b (SV) x 70 b/m (HR)
= 4900 ml/m = 4,9 l/m

Heart RateNilai HR dapat naik / turun
Naik : Efek Stimulasi SimpatisTurun : Efek Stimulasi Parasimpatis
Untuk meningkatkan HR :1. Memblock input parasimpatik = HR 100 b/m2. Menambahkan input simpatik = HR 100++ b/m
Stroke VolumeSV = End Diastolic Volume (135 ml) – End Sistolic Volume (65 ml)
EDV = Volume darah yang mengisi ventrikel selama diastoleEDV dipengaruhi : aliran balik vena , kemampuan jantung mengembang
ESV = Volume darah sisa setelah sistoleESV dipengaruhi : Kontraktilitas , afterload

Hukum Frank StarlingSemakin jantung teregang, kontraksi semakin kuat
Jika aliran balik vena meningkat --> banyak darah di ventrikel (ventrikel mengembang) ->> kontraksi semakin kuat

End Sistolic VolumeAfterload : beban kerja yg dibebankan kepada jantung setelah
kontraksi dimulai (hipertensi, stenosis katup)
Kontraktilitas : kekuatan kontraksi di setiap EDVNaik : Efek stimulus NE , ETurun : B-Blocker
EFEK SISTEM SARAF OTONOM OTOT JANTUNG
• Efek Parasimpatis• mempengaruhi nodus SA yang mengurangi kecepatan
jantung.Asetikolin yang dibebaskan pada pengaktifan parasimpatis meningkatkan permeabilitas nodus SA terhadap ion Kalium dengan cara memperlambat penutpan saluran kalium
• Efek Simpatis• mempengaruhi nodus SA dengan cara mempercepat
depolarisasi sehingga ambang batas lebih cepat tercapai.Norepinefrin yang dikeluarkan ujung saraf simpatis ini mempengaruhi penurunan permeabilitas terhadap kalium dengan cara mempercepat inaktivasi saluran kalium.