pemberian obat rematik yang aman bagi penderita geriatri - copy
DESCRIPTION
Slide presentasi tentang obat-obat rematik dan cara pemberiannya yang amanTRANSCRIPT
1
PEMLIHAN OBAT REMATIK PEMLIHAN OBAT REMATIK YANG AMAN UNTUK YANG AMAN UNTUK
PENDERITA GERIATRIPENDERITA GERIATRI
EDU TEHUPEIORYEDU TEHUPEIORY
SUB-DEVISI REUMATOLOGI SUB-DEVISI REUMATOLOGI BAGIAN ILMU PENYAKIT DALAM BAGIAN ILMU PENYAKIT DALAM
FAKULTAS KEDOKTERAN FAKULTAS KEDOKTERAN UNIVERSITAS HASANUDDINUNIVERSITAS HASANUDDIN
MAKASSARMAKASSAR
2
PENDAHULUANPENDAHULUAN
Mukosa lambung sangat rentang alami Mukosa lambung sangat rentang alami injuryinjury oleh hiperproduksi asam, garam oleh hiperproduksi asam, garam empedu, alkohol dan NSAIDS.empedu, alkohol dan NSAIDS.
Untuk melindungi mukosa lambung Untuk melindungi mukosa lambung terdapat terdapat cytoprotection cytoprotection yang dimediasi yang dimediasi oleh prostaglandin PG2.oleh prostaglandin PG2.
3
Nonsteroidal anti-inflammatory Nonsteroidal anti-inflammatory Drugs (NSAID) are the most used Drugs (NSAID) are the most used classes of medication world wide.classes of medication world wide.
NSAID Gastro – Enteropathy are the NSAID Gastro – Enteropathy are the most prevalent of adverse drug most prevalent of adverse drug reactions.reactions.
4
Goals of Arthritis TherapyGoals of Arthritis Therapy
Relieve pain/inflammation
Minimize risks of therapy
Retard disease progression
Provide patient education
Prevent work disability
Enhance quality of life and functional independence
Relieve pain/inflammation
Minimize risks of therapy
Retard disease progression
Provide patient education
Prevent work disability
Enhance quality of life and functional independence
5
An Historical Perspective of An Historical Perspective of NSAID-Associated GI UlcerationNSAID-Associated GI Ulceration
Endoscopic ulcer point prevalence:
10–20%1
Symptomatic ulcers/ulcer complications: 2–4% per year2
Most hospitalizations occur without previous symptoms3
Endoscopic ulcer point prevalence:
10–20%1
Symptomatic ulcers/ulcer complications: 2–4% per year2
Most hospitalizations occur without previous symptoms3
1Lichtenstein et al. Arthritis Rheum. 1995;38:5–18;2FDA Drug Bull. 1989;19:3–4; 3Armstrong, Blower. Gut. 1987;28:527–532.
1Lichtenstein et al. Arthritis Rheum. 1995;38:5–18;2FDA Drug Bull. 1989;19:3–4; 3Armstrong, Blower. Gut. 1987;28:527–532.
6
NSAID Induced Serious GI NSAID Induced Serious GI ComplicationComplication
NSAID can cause serious GI complicationNSAID can cause serious GI complicationsuch as :such as :
- Perforation- Perforation- Ulcer / obstruction- Ulcer / obstruction- Serious bleeding- Serious bleeding
Complication rate in placebo group in the Complication rate in placebo group in the MUCOSA study at six months was 0,95%MUCOSA study at six months was 0,95%
Close to FDA estimates at 2-4 % per annumClose to FDA estimates at 2-4 % per annum
7
Do Different NSAID formulations Do Different NSAID formulations Reduce Reduce
Risk of GI Complication?Risk of GI Complication? Non-acetyliated salicylates or ibuprofenNon-acetyliated salicylates or ibuprofen
@ diminishes GI complication, possibly due to @ diminishes GI complication, possibly due to use use
of lower dosageof lower dosage Enteric-coated and buffered aspirinEnteric-coated and buffered aspirin
@ similar GI toxicity to plain aspirin@ similar GI toxicity to plain aspirin Other routes of administration (IM. PR)Other routes of administration (IM. PR)
@ no reduction in risk of ulcer complications@ no reduction in risk of ulcer complications ProdrugsProdrugs
@ no reduction in risk of ulcer complications@ no reduction in risk of ulcer complications
8
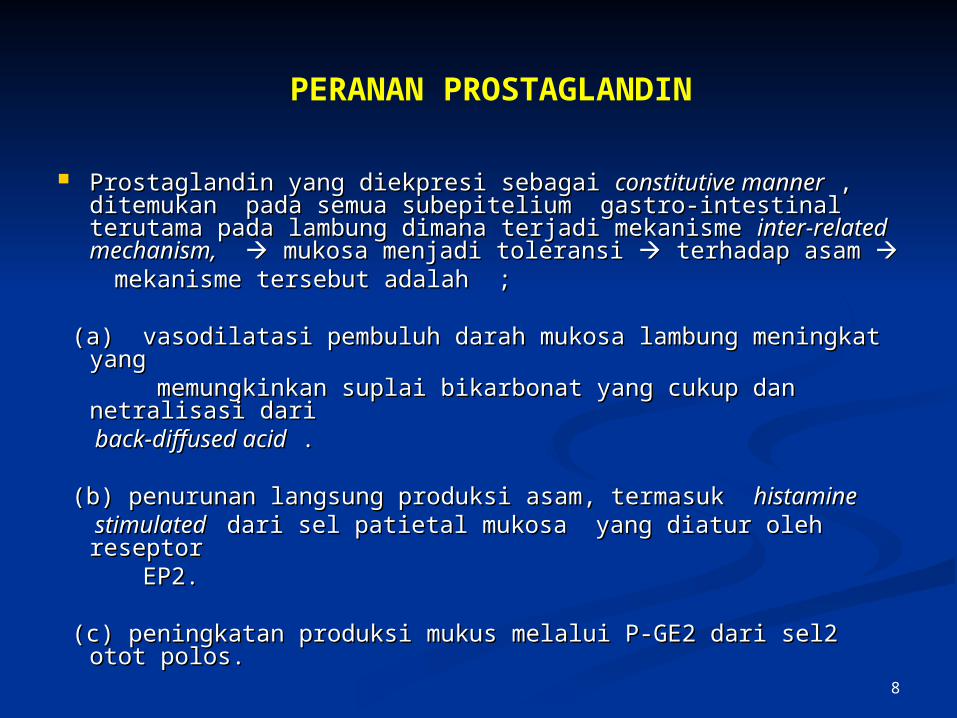
Prostaglandin yang diekpresi sebagai Prostaglandin yang diekpresi sebagai constitutive mannerconstitutive manner , , ditemukan pada semua subepitelium gastro-intestinal ditemukan pada semua subepitelium gastro-intestinal terutama pada lambung dimana terjadi mekanisme terutama pada lambung dimana terjadi mekanisme inter-related inter-related mechanism,mechanism, mukosa menjadi toleransi mukosa menjadi toleransi terhadap asam terhadap asam
mekanisme tersebut adalah ;mekanisme tersebut adalah ;
(a) vasodilatasi pembuluh darah mukosa lambung meningkat (a) vasodilatasi pembuluh darah mukosa lambung meningkat yang yang
memungkinkan suplai bikarbonat yang cukup dan netralisasi memungkinkan suplai bikarbonat yang cukup dan netralisasi dari dari
back-diffused acidback-diffused acid . .
(b) penurunan langsung produksi asam, termasuk (b) penurunan langsung produksi asam, termasuk histamine histamine stimulated stimulated dari sel patietal mukosa yang diatur oleh reseptor dari sel patietal mukosa yang diatur oleh reseptor EP2.EP2.
(c) peningkatan produksi mukus melalui P-GE2 dari sel2 otot (c) peningkatan produksi mukus melalui P-GE2 dari sel2 otot polos.polos.
PERANAN PROSTAGLANDIN
9
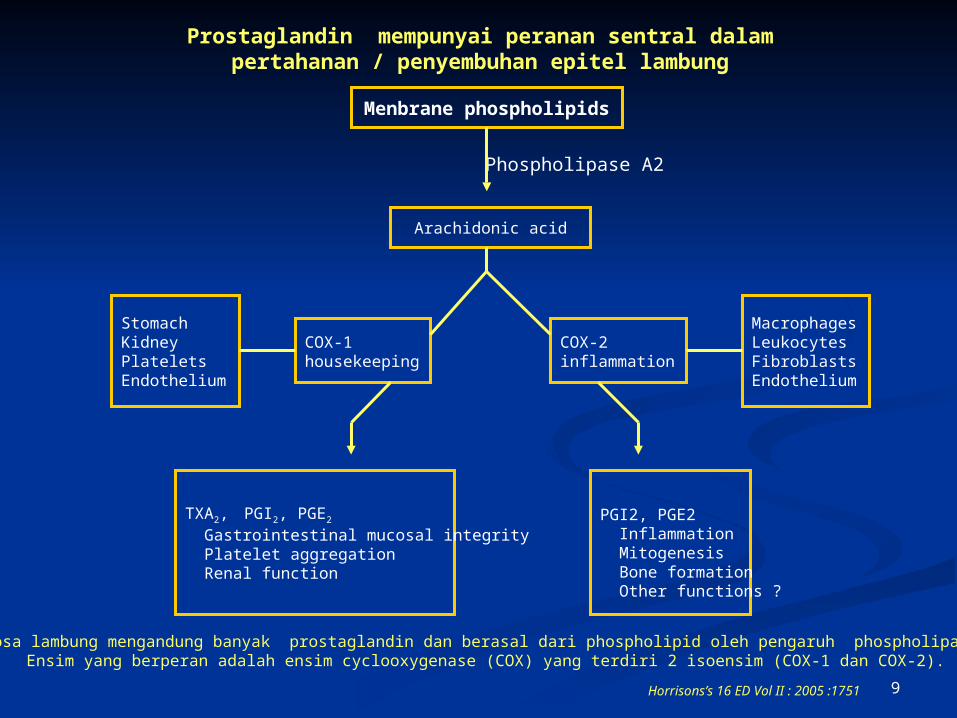
Menbrane phospholipids
Arachidonic acid
StomachKidneyPlateletsEndothelium
COX-1housekeeping
COX-2inflammation
MacrophagesLeukocytesFibroblastsEndothelium
TXA2, PGI2, PGE2
Gastrointestinal mucosal integrity Platelet aggregation Renal function
PGI2, PGE2 Inflammation Mitogenesis Bone formation Other functions ?
Phospholipase A2
Prostaglandin mempunyai peranan sentral dalam pertahanan / penyembuhan epitel lambung
Horrisons’s 16 ED Vol II : 2005 :1751
Mukosa lambung mengandung banyak prostaglandin dan berasal dari phospholipid oleh pengaruh phospholipase A2.Ensim yang berperan adalah ensim cyclooxygenase (COX) yang terdiri 2 isoensim (COX-1 dan COX-2).
10
Improving the GI Tolerability of Improving the GI Tolerability of NSAID TherapyNSAID Therapy
Take with foodTake with food Take with waterTake with water Take in upright positionTake in upright position Reduce Gastritis-inducing agentsReduce Gastritis-inducing agents
e.g alcohol, smokinge.g alcohol, smoking
11
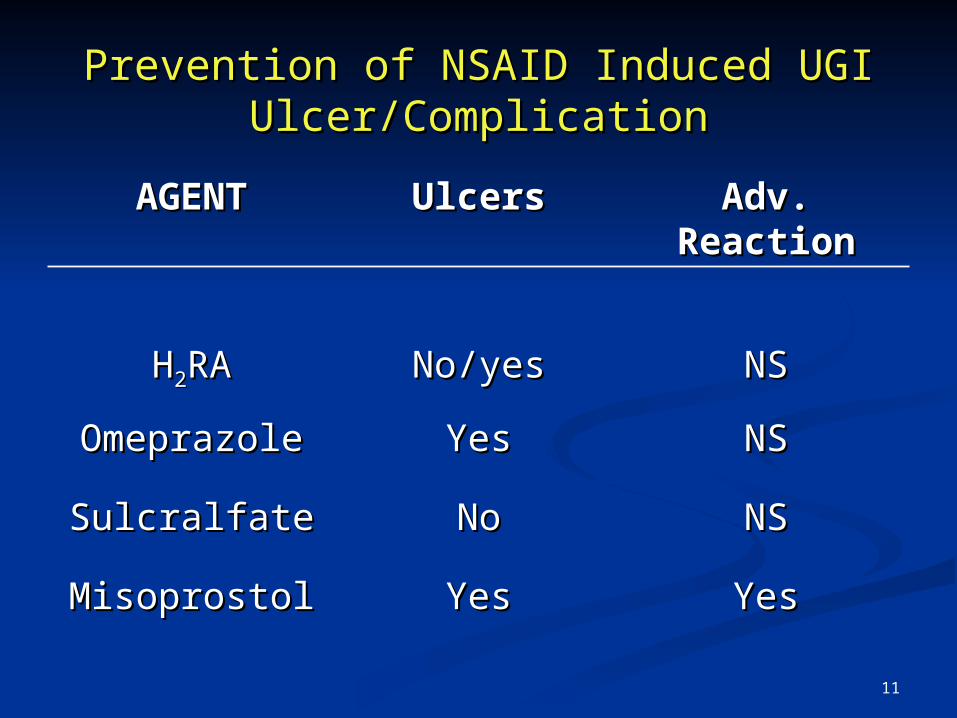
Prevention of NSAID Induced UGIPrevention of NSAID Induced UGIUlcer/ComplicationUlcer/Complication
AGENTAGENT UlcersUlcers Adv. Adv. ReactionReaction
HH22RARA No/yesNo/yes NSNS
OmeprazoleOmeprazole YesYes NSNS
SulcralfateSulcralfate NoNo NSNS
MisoprostolMisoprostol YesYes YesYes
12
Major Risk Factors for Major Risk Factors for GIT ToxicityGIT Toxicity
Age, level of disability.Age, level of disability. Previous history peptic ulcer disease.Previous history peptic ulcer disease. History of taking anti ulcer medications.History of taking anti ulcer medications. NSAID dosage.NSAID dosage. Concomitant Glucocorticoid use.Concomitant Glucocorticoid use.
13
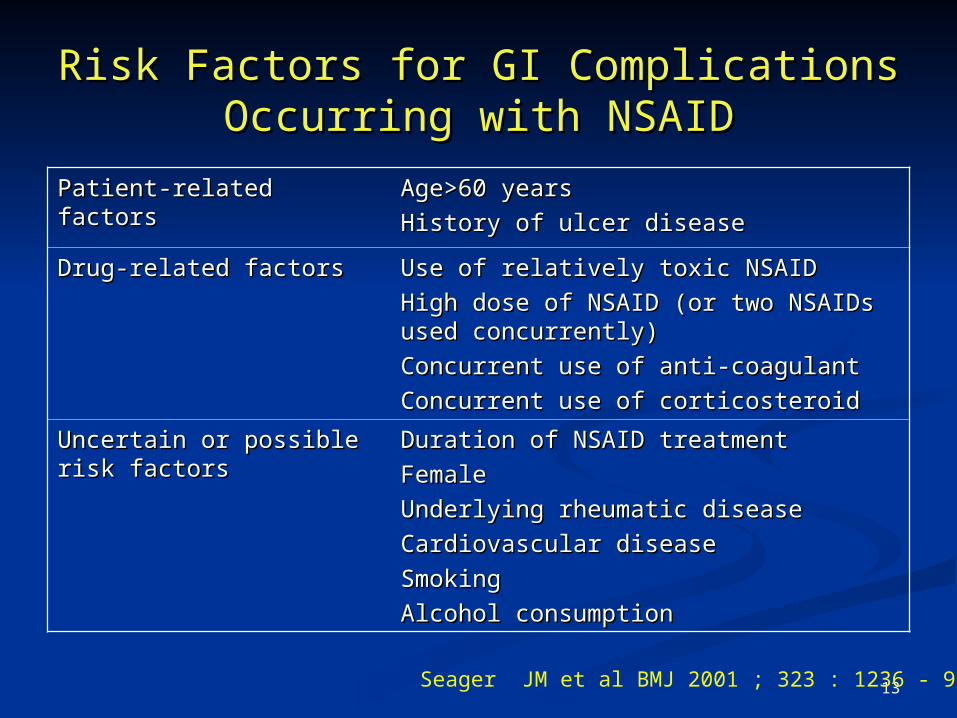
Risk Factors for GI ComplicationsRisk Factors for GI ComplicationsOccurring with NSAIDOccurring with NSAID
Patient-related factorsPatient-related factors Age>60 yearsAge>60 years
History of ulcer diseaseHistory of ulcer disease
Drug-related factorsDrug-related factors Use of relatively toxic NSAIDUse of relatively toxic NSAID
High dose of NSAID (or two NSAIDs High dose of NSAID (or two NSAIDs used concurrently)used concurrently)
Concurrent use of anti-coagulantConcurrent use of anti-coagulant
Concurrent use of corticosteroidConcurrent use of corticosteroid
Uncertain or possible risk Uncertain or possible risk factorsfactors
Duration of NSAID treatmentDuration of NSAID treatment
FemaleFemale
Underlying rheumatic diseaseUnderlying rheumatic disease
Cardiovascular diseaseCardiovascular disease
SmokingSmoking
Alcohol consumptionAlcohol consumption
Seager JM et al BMJ 2001 ; 323 : 1236 - 9
14
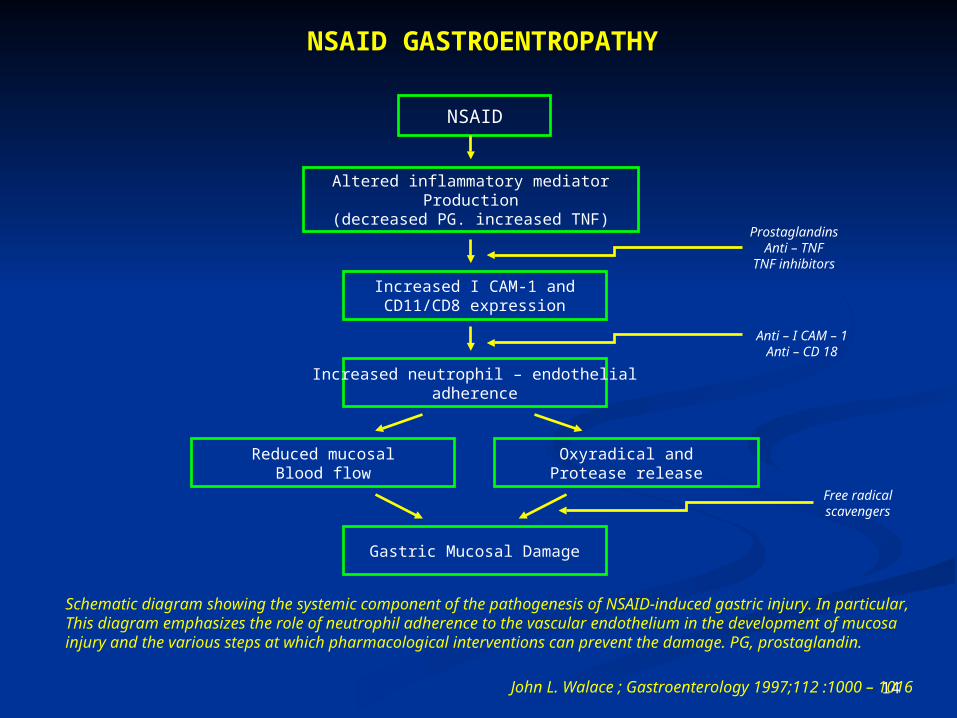
Altered inflammatory mediatorProduction
(decreased PG. increased TNF)
NSAID
Increased I CAM-1 andCD11/CD8 expression
Increased neutrophil – endothelialadherence
Reduced mucosalBlood flow
Oxyradical andProtease release
Gastric Mucosal Damage
ProstaglandinsAnti – TNF
TNF inhibitors
Anti – I CAM – 1Anti – CD 18
Free radicalscavengers
NSAID GASTROENTROPATHY
Schematic diagram showing the systemic component of the pathogenesis of NSAID-induced gastric injury. In particular, This diagram emphasizes the role of neutrophil adherence to the vascular endothelium in the development of mucosa injury and the various steps at which pharmacological interventions can prevent the damage. PG, prostaglandin.
John L. Walace ; Gastroenterology 1997;112 :1000 – 1016
15
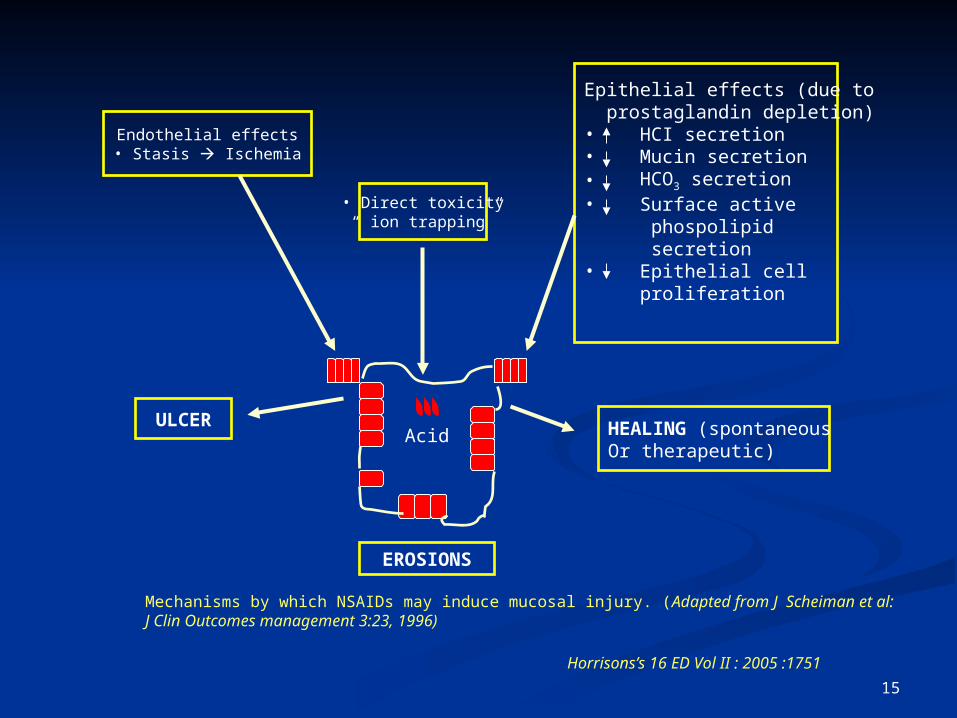
Acid
EROSIONS
HEALING (spontaneousOr therapeutic)
Epithelial effects (due to prostaglandin depletion)• HCI secretion• Mucin secretion• HCO3 secretion• Surface active phospolipid secretion• Epithelial cell proliferation
• Direct toxicity“ ion trapping”
Endothelial effects• Stasis Ischemia
ULCER
Mechanisms by which NSAIDs may induce mucosal injury. (Adapted from J Scheiman et al: J Clin Outcomes management 3:23, 1996)
Horrisons’s 16 ED Vol II : 2005 :1751
16
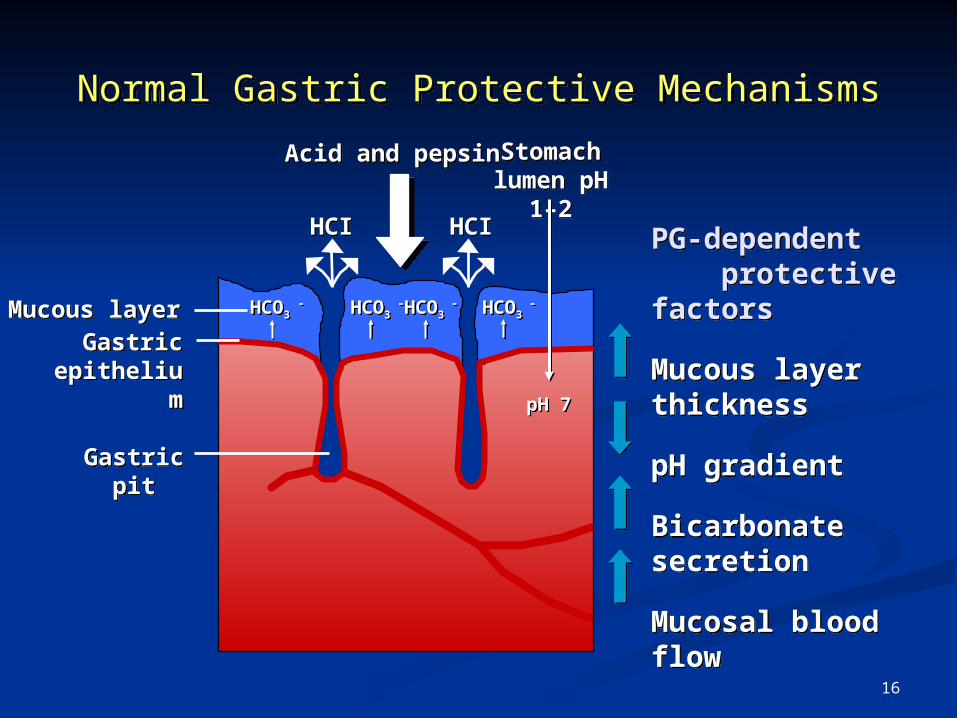
Normal Gastric Protective MechanismsNormal Gastric Protective Mechanisms
Acid and pepsinAcid and pepsin Stomach lumen pH 1–
2
Stomach lumen pH 1–
2PG-dependent protective factors
Mucous layer thickness
pH gradient
Bicarbonate secretion
Mucosal blood flow
PG-dependent protective factors
Mucous layer thickness
pH gradient
Bicarbonate secretion
Mucosal blood flow
Mucous layerMucous layer
Gastric epithelium
Gastric epithelium
Gastric pitGastric pit
HCO3 -HCO3 -HCO3
-HCO3 -HCO3
-HCO3 -HCO3
-HCO3 -
HCIHCIHCIHCI
pH 7pH 7
17
APAKAH SATU OAINS LEBIH BAIK DARI APAKAH SATU OAINS LEBIH BAIK DARI YANG LAINNYA SEHUBUNGAN DENGAN YANG LAINNYA SEHUBUNGAN DENGAN
KEMUNGKINAN MENIMBULKAN KEMUNGKINAN MENIMBULKAN KERUSAKAN PADA SALURAN CERNA ?KERUSAKAN PADA SALURAN CERNA ?
Lebih 10 tahun berbagai macam penelitian farmako-epidemiologik Dan meta-analisis yang memungkinkan a ranking of sorts sesuai dengan
pengalaman klinik ( lihat tabel) :
18
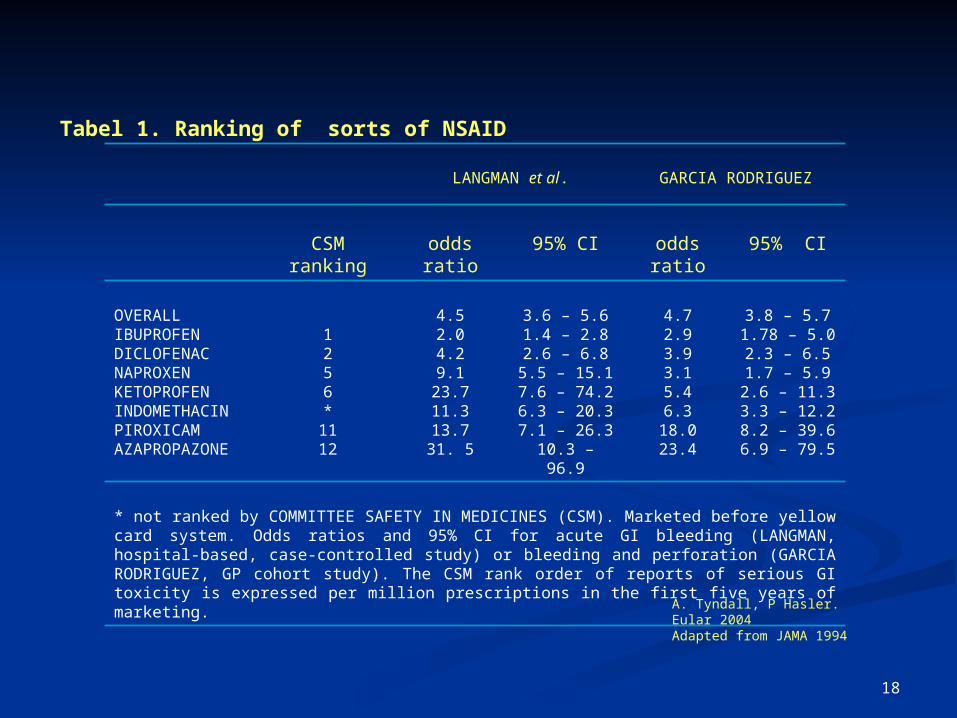
Tabel 1. Ranking of sorts of NSAID
LANGMAN et al. GARCIA RODRIGUEZ
CSM ranking odds ratio 95% CI odds ratio 95% CI
OVERALLIBUPROFENDICLOFENACNAPROXENKETOPROFENINDOMETHACINPIROXICAMAZAPROPAZONE
1256*
1112
4.52.04.29.1
23.711.313.731. 5
3.6 – 5.61.4 – 2.82.6 – 6.8
5.5 – 15.17.6 – 74.26.3 – 20.37.1 – 26.3
10.3 – 96.9
4.72.93.93.15.46.3
18.023.4
3.8 – 5.71.78 – 5.02.3 – 6.51.7 – 5.9
2.6 – 11.33.3 – 12.28.2 – 39.66.9 – 79.5
* not ranked by COMMITTEE SAFETY IN MEDICINES (CSM). Marketed before yellow card system. Odds ratios and 95% CI for acute GI bleeding (LANGMAN, hospital-based, case-controlled study) or bleeding and perforation (GARCIA RODRIGUEZ, GP cohort study). The CSM rank order of reports of serious GI toxicity is expressed per million prescriptions in the first five years of marketing.
A. Tyndall, P Hasler. Eular 2004Adapted from JAMA 1994
19
The Available Anti-Ulcer The Available Anti-Ulcer Strategies IncludeStrategies Include
Prevention of gastric acid secretion.Prevention of gastric acid secretion. Neutralization of gastric acid.Neutralization of gastric acid. Mucosal cytoprotectionMucosal cytoprotection
20
Ensim COX berperan penting pada pembentukan Ensim COX berperan penting pada pembentukan prostaglandin.prostaglandin.
Terdapat 2 isoform ensim COX, yaitu : Terdapat 2 isoform ensim COX, yaitu : COX-1 : diekpresikan COX-1 : diekpresikan constitutive manner constitutive manner berperan berperan
menjaga integritas mukosa lambung, ginjal dll menjaga integritas mukosa lambung, ginjal dll ( ( housekeeping housekeeping ). ).
COX-2 : COX-2 : inducibleinducible berperan pada proses inflamasi yang berperan pada proses inflamasi yang diekresi dalam makrofag, lekosit, fibroblast dan sel diekresi dalam makrofag, lekosit, fibroblast dan sel sinovia.sinovia.
Kedua ensim ini dihambat OAINS dan inhibisi terhadap Kedua ensim ini dihambat OAINS dan inhibisi terhadap cox-1 dapat mengakibatkan kerusakan pada saluran cerna cox-1 dapat mengakibatkan kerusakan pada saluran cerna terutama lambung sedangkan inhibisi COX-2 tidak terutama lambung sedangkan inhibisi COX-2 tidak menimbulkan kerusakan pada saluran cerna.menimbulkan kerusakan pada saluran cerna.
ENSIM CYCLOOXYGENASE
21
Untuk menghindarkan kerusakan pada saluran Untuk menghindarkan kerusakan pada saluran cerna terutama lambung, dibuat berbagai COX-2 cerna terutama lambung, dibuat berbagai COX-2 inhibitor inhibitor ada yang ada yang selektifselektif dan dan spesifikspesifik : :
SelektifSelektif ; : ; : An in vitro measure of relative An in vitro measure of relative amounts of drug required to inhibit each each amounts of drug required to inhibit each each enzymeenzyme
Tells little about clinical relevanceTells little about clinical relevance
SpesifikSpesifik ; ; An in vivo conceptAn in vivo concept
Clinically relevant inhibition of COX-2 without Clinically relevant inhibition of COX-2 without inhibition of COX-1inhibition of COX-1
22
PERKEMBANGAN KLINIK DENGAN OAINSPERKEMBANGAN KLINIK DENGAN OAINS
Dengan dosis yang sesuai kemanjuran Dengan dosis yang sesuai kemanjuran dari berbagai OAINS adalah sama.dari berbagai OAINS adalah sama.
Respons penderita secara individu jelas Respons penderita secara individu jelas sekali berbeda.sekali berbeda.
Seorang penderita respons yang lain Seorang penderita respons yang lain tidak.tidak.
Hipotesis : (a) variasi dalam absorpsi obat Hipotesis : (a) variasi dalam absorpsi obat (b) bioavailability (c) efek biologis obat.(b) bioavailability (c) efek biologis obat.
23
EFEK SAMPINGEFEK SAMPING
Bisa pada lambung dan duodenum.Bisa pada lambung dan duodenum. Dispepsi, mual, nausea , ulkus lambung.Dispepsi, mual, nausea , ulkus lambung. Hanya berkisar 1 – 2 %,Hanya berkisar 1 – 2 %, Terdapat beberapa mekanisme oleh Terdapat beberapa mekanisme oleh
OAINS pada saluran cerna :OAINS pada saluran cerna : (a) OAINS menekan produksi PG (b) (a) OAINS menekan produksi PG (b)
menurunkan aliran mikro-sirkulasi (c) menurunkan aliran mikro-sirkulasi (c) menaikkan menaikkan leucocyte adherens leucocyte adherens terhadap terhadap endotil vaskuler (d) mempengaruhi endotil vaskuler (d) mempengaruhi produksi mediator inflamasi.produksi mediator inflamasi.

24
GI Events* Associated With NSAIDsGI Events* Associated With NSAIDs
Most Patients AsymptomaticMost Patients Asymptomatic
N = 141N = 141 N = 1,921N = 1,921
Armstrong, Blower.Gut. 1987;28:527–532.Armstrong, Blower.
Gut. 1987;28:527–532.Singh et al.
Arch Intern Med.1996;156:1530–1536.
Singh et al.Arch Intern Med.
1996;156:1530–1536.
WithoutsymptomsWithoutsymptoms
WithsymptomsWithsymptoms
42%58%58% 81%81%19%
*Bleeding, perforation, and gastric outlet obstruction*Bleeding, perforation, and gastric outlet obstruction
25
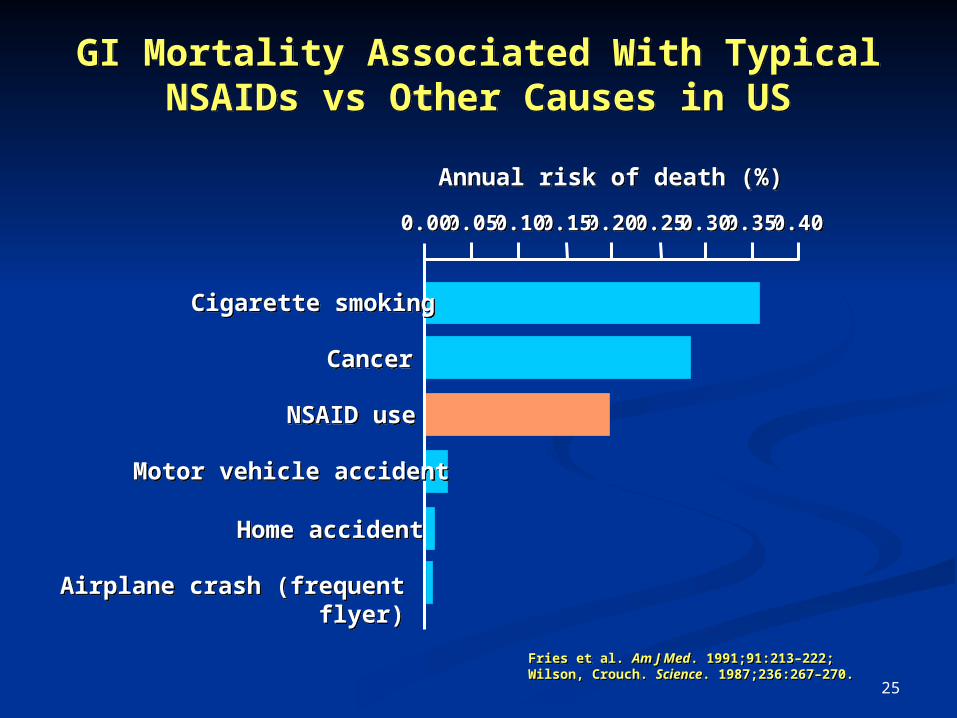
GI Mortality Associated With TypicalNSAIDs vs Other Causes in US
GI Mortality Associated With TypicalNSAIDs vs Other Causes in US
Fries et al. Am J Med. 1991;91:213–222;Wilson, Crouch. Science. 1987;236:267–270.Fries et al. Am J Med. 1991;91:213–222;Wilson, Crouch. Science. 1987;236:267–270.
Annual risk of death (%)Annual risk of death (%)
0.250.250.200.200.150.150.100.100.050.050.000.00 0.400.400.350.350.300.30
Cigarette smokingCigarette smoking
CancerCancer
NSAID useNSAID use
Motor vehicle accidentMotor vehicle accident
Home accidentHome accident
Airplane crash (frequent flyer)Airplane crash (frequent flyer)
26
GI complications associated with nonselective NSAIDs remain an
important public health issue
• Most prominent toxicity is GI ulceration, bleeding, and perforation
• Serious NSAID-related GI complications result in 107,000 hospitalizations and 16,500 deaths annually in the US1
• Up to 80% of those hospitalized for NSAID- related GI complications had non prior GI adverse event1
Singh G, Triadafilopoulos G. Epidemiology of NSAID induced gastrointestinal
complication. J Rheumatol. 1999; 26 : 18 - 24
27
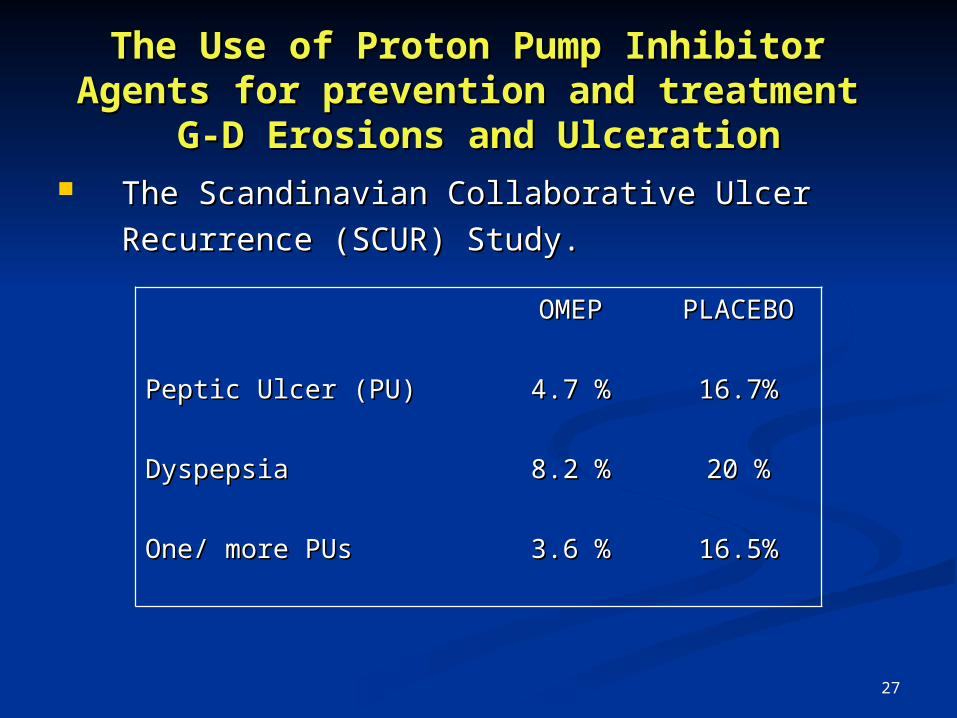
The Use of Proton Pump Inhibitor The Use of Proton Pump Inhibitor Agents for prevention and treatment Agents for prevention and treatment
G-D Erosions and UlcerationG-D Erosions and Ulceration The Scandinavian Collaborative UlcerThe Scandinavian Collaborative Ulcer
Recurrence (SCUR) Study.Recurrence (SCUR) Study.
OMEPOMEP PLACEBOPLACEBO
Peptic Ulcer (PU)Peptic Ulcer (PU) 4.7 %4.7 % 16.7%16.7%
DyspepsiaDyspepsia 8.2 %8.2 % 20 %20 %
One/ more PUsOne/ more PUs 3.6 %3.6 % 16.5%16.5%
28
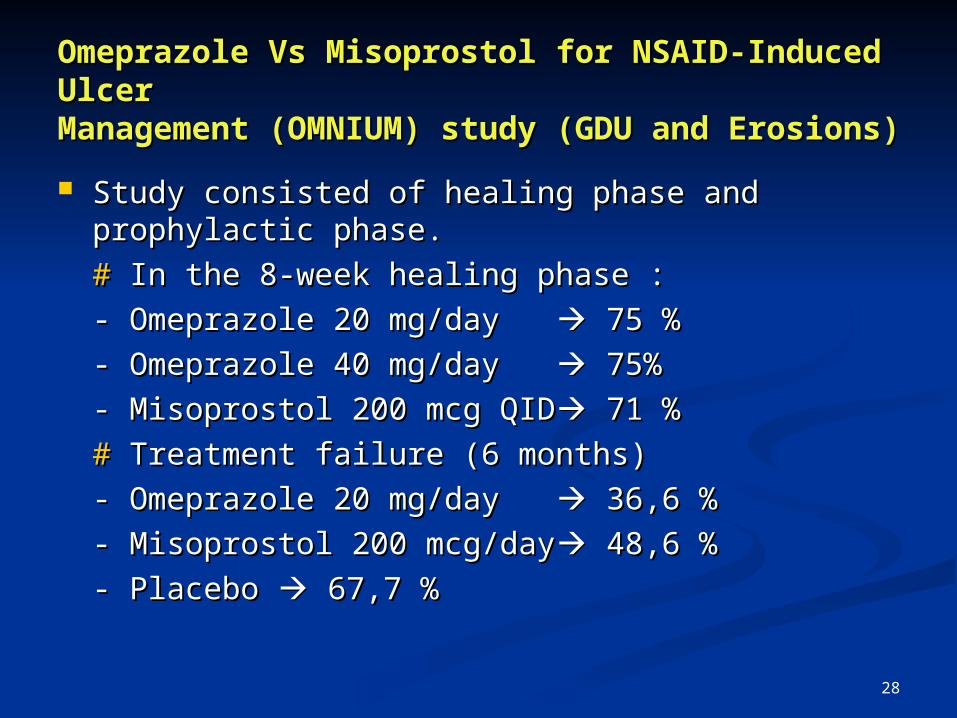
Omeprazole Vs Misoprostol for NSAID-Omeprazole Vs Misoprostol for NSAID-Induced UlcerInduced UlcerManagement (OMNIUM) study (GDU and Management (OMNIUM) study (GDU and Erosions)Erosions) Study consisted of healing phase and Study consisted of healing phase and
prophylactic phase.prophylactic phase.
## In the 8-week healing phase : In the 8-week healing phase :
- Omeprazole 20 mg/day - Omeprazole 20 mg/day 75 % 75 %
- Omeprazole 40 mg/day - Omeprazole 40 mg/day 75% 75%
- Misoprostol 200 mcg QID- Misoprostol 200 mcg QID 71 % 71 %
## Treatment failure (6 months) Treatment failure (6 months)
- Omeprazole 20 mg/day - Omeprazole 20 mg/day 36,6 % 36,6 %
- Misoprostol 200 mcg/day- Misoprostol 200 mcg/day 48,6 % 48,6 %
- Placebo - Placebo 67,7 % 67,7 %
29
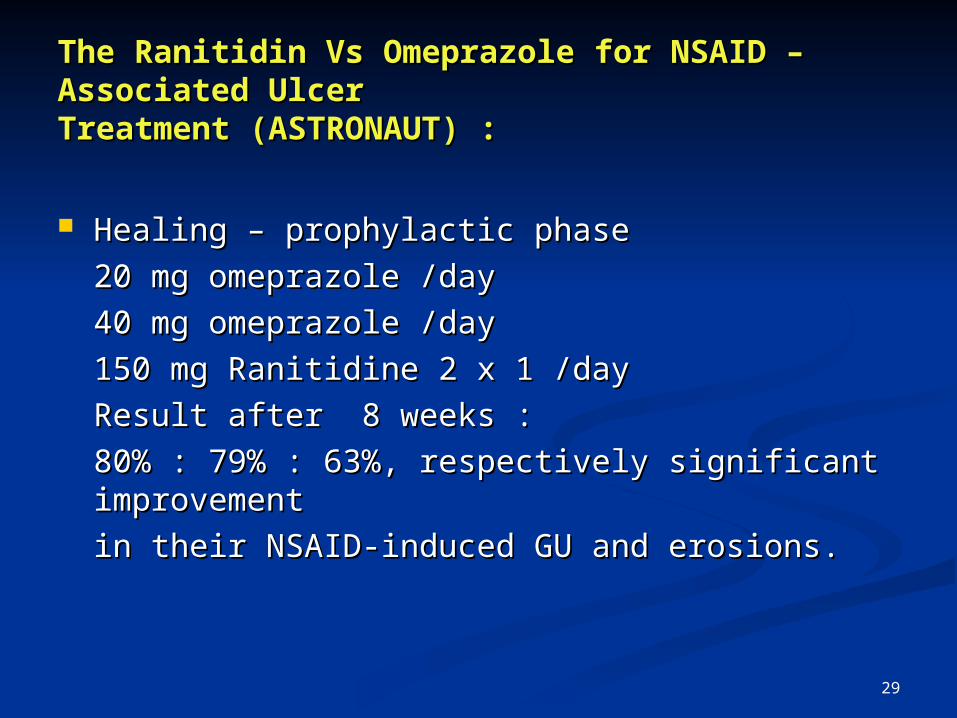
The Ranitidin Vs Omeprazole for NSAID – The Ranitidin Vs Omeprazole for NSAID – Associated UlcerAssociated UlcerTreatment (ASTRONAUT) :Treatment (ASTRONAUT) :
Healing – prophylactic phaseHealing – prophylactic phase
20 mg omeprazole /day20 mg omeprazole /day
40 mg omeprazole /day40 mg omeprazole /day
150 mg Ranitidine 2 x 1 /day150 mg Ranitidine 2 x 1 /day
Result after 8 weeks :Result after 8 weeks :
80% : 79% : 63%, respectively significant 80% : 79% : 63%, respectively significant improvementimprovement
in their NSAID-induced GU and erosions.in their NSAID-induced GU and erosions.
30
SUMMARYSUMMARY
Improving the GI tolerability of NSAID Improving the GI tolerability of NSAID Therapy : Take with food, take with water, Therapy : Take with food, take with water, take in upright position and reduced take in upright position and reduced inducing agents e.g alcohol and smoking.inducing agents e.g alcohol and smoking.
PPI is the most effective empiric therapy PPI is the most effective empiric therapy for NSAID associated dyspepsia.for NSAID associated dyspepsia.
PPI 40 and 20 mg/day have the same PPI 40 and 20 mg/day have the same effectiveness in patient with gastrophaty effectiveness in patient with gastrophaty induced by selective and non selective induced by selective and non selective NSAIDs.NSAIDs.