hipertensão pulmonar
TRANSCRIPT
* CorrespondE-mail add
Dirven).
1760-2734/$ -http://dx.doi.
Journal of Veterinary Cardiology (2012) 14, 465e474
www.elsevier.com/locate/jvc
CASE REPORT
Reversible pulmonary hypertension associatedwith lungworm infection in a young cat
Mark Dirven, DVM a,b,*, Viktor Szatmari, Ph.D b, Ted van den Ingh, Ph.D c,Rolf Nijsse, DVM d
aDierenkliniek Rijen, Hoofdstraat 16, 5121 JE Rijen, The NetherlandsbDepartment of Clinical Sciences of Companion Animals, Faculty of Veterinary Medicine,Utrecht University, Yalelaan 108, 3508 TD Utrecht, The NetherlandscValuepath Veterinary Pathology, Verlengde Klinkerstraat 6, 6433 PL Hoensbroek, The NetherlandsdDepartment of Infectious Diseases and Immunology, Faculty of Veterinary Medicine,University of Utrecht, Yalelaan 1, 3508 TD Utrecht, The Netherlands
Received 20 February 2011; received in revised form 1 April 2012; accepted 18 April 2012
KEYWORDSFeline;Heart failure;Pneumonia;Echocardiography
ing author.ress: mark.dirven@d
see front matter ª 201org/10.1016/j.jvc.2012
Abstract Two ten-week-old kittens presented with dyspnea. Two weeks later dys-pnea had worsened and both kittens had developed a heart murmur. One kittendied and necropsy showed severe granulomatous pneumonia and moderate bronch-i(oli)tis and peribronchi(oli)tis caused by Aelurostrongylus abstrusus. The resultsfrom echocardiography, thoracic radiography and the other kitten’s fecal examina-tion were interpreted as severe parasitic pneumonia caused by A. abstrusus infec-tion with pulmonary hypertension. Repeated administration of milbemycine-oximeand praziquantel resulted in cessation of larvae shedding and resolution of clinical,radiographic and echocardiographic signs of bronchopneumonia and pulmonaryhypertension.ª 2012 Elsevier B.V. All rights reserved.
A litter of two European shorthaired kittens wasfound in a rural area near the town of Etten-Leur inthe southwestern part of the Netherlands. Thekittens were assigned to an adoption program run
ierenkliniekrijen.nl (M.
2 Elsevier B.V. All rights reser.04.005
by an animal shelter.e One kitten was male, theother female. Nine days after they were found,both kittens were examined by the animal shelterveterinarian. The kittens were now estimated tobe 10 weeks old. Body weight was 1.1 kg for the
e Dierenasiel Breda e.o.. Oude Baan 60, 4825 BL, Breda, TheNetherlands.
ved.

466 M. Dirven et al.
male and 1.0 kg for the female. Both animals weresneezing and had purulent nasal discharge. Onauscultation no heart murmur was noticed. Basedupon suspicion of viral and secondary bacterialrhinitis, both kittens were treated with amoxicil-line and clavulanic acid.f They were dewormedwith a single oral dose of milbemycine-oxime andpraziquantelg conforming to the protocol of theanimal shelter. One week later both animals werereexamined by the animal shelter veterinarianbecause of dyspnea. Four days after the lastexamination both kittens were brought to Dier-enkliniek Rijen for further diagnostic evaluation.
Case 1
Upon presentation, the male kitten weighed1.25 kg and was 12 weeks old. Rectal bodytemperature was 38.8 �C. It was severely dyspneicwithout stertor. Respiratory rate was 60 breaths/min with an abdominal breathing pattern; howeverthere was no open mouth breathing. Pulsefrequency was 180/min. Jugular venous distensionor pulsation was absent. Thoracic auscultationrevealed inspiratory crackles and a grade III/VIsystolic heart murmur with its point of maximumintensity on the right hemithorax. Thoracic radio-graphs showed severe broncho-alveolar infiltratesin the caudodorsal and cranioventral lung fields.Right-sided cardiomegaly was also observed.
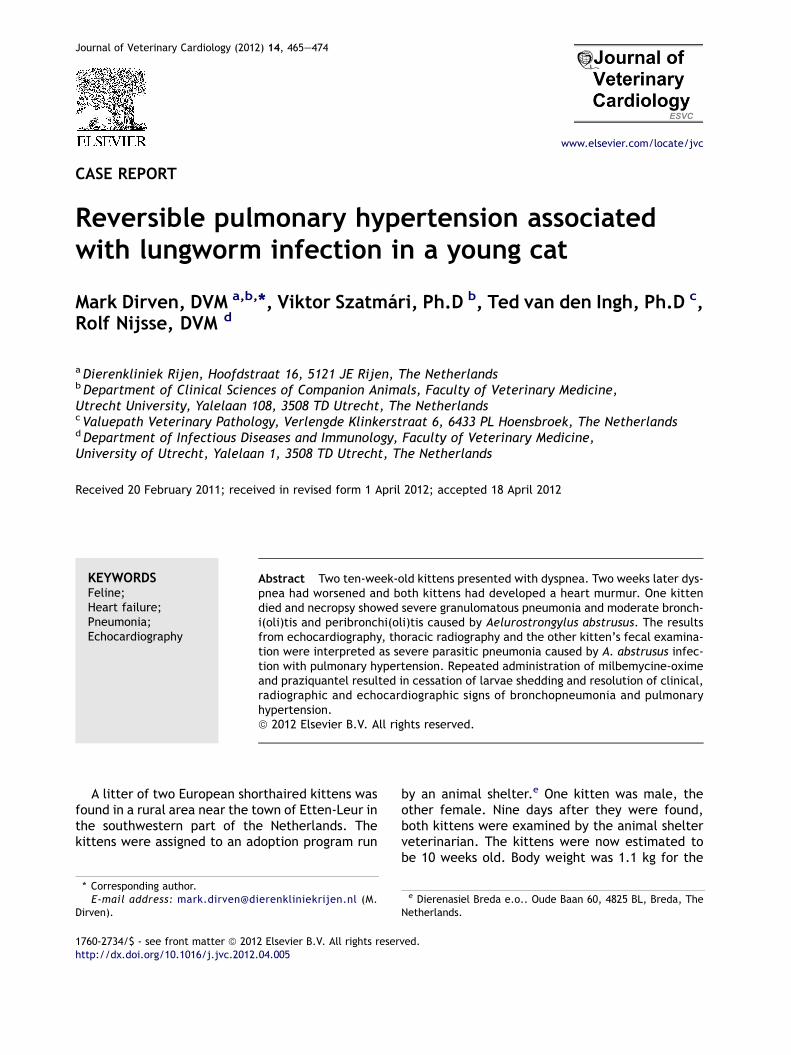
Echocardiographyh showed severe eccentrichypertrophy of the right ventricle and amoderatelydilated right atrium. No structural abnormalities ofthe tricuspid valve were detected. Color Dopplerechocardiography showed a large systolic regur-gitant jet originating from the tricuspid valve. Dueto increasing respiratory distress, the exam wasterminated. The kitten was put in an oxygen cagebut died later that day. A necropsy was performed.Multifocal granulomas distributed throughout thelungs were noted (Fig. 1A). Histopathologic evalu-ation of the lungs revealed a moderate amount ofeosinophils and neutrophils in the larger andsmaller bronchi as well as in the bronchioles. In theperibronchial tissue moderate to severe lympho-plasmacytic inflammation was seen. Extensivemultifocal and coalescing granulomatous
f Amoxicilline-trihydrate 20 mg/kg þ potassium-clavulanate5.25 mg/kg bid (Synulox� 50 mg tablet, Pfizer Animal HealthB.V., Capelle a/d IJssel, The Netherlands).g Milbemycine oxime 4 mg/kg þ Praziquantel 10 mg/kg single
dose (Milbemax�, Novartis Consumer Health B.V., Breda, TheNetherlands).h Esaote MyLab 50 X-vision with 7.5e10 Mhz PA transducer,
Esaote Pie Medical, Maastricht, The Netherlands.
inflammation extending in the adjacent paren-chyma was observed throughout the lung tissue.Many granulomas contained eggs (50e65 mm, con-taining 7e10 blastomeres) and/or L1 larvae. Thegranulomatous inflammation was composed of thefollowing: macrophages; multinucleated giant cellsoften surrounding or adjacent to eggs or larvae;lymphocytes and plasma cells; a slight to moderateinfiltration of eosinophils sometimes as eosinophilicmicroabcesses; few neutrophils and some fibrosis(Fig. 1B and C).
On the basis of these findings it was concludedthat the kitten had suffered from severe granulo-matous pneumonia and moderate bronchi(oli)tisand peribronchi(oli)tis due to Aelurostrongylusabstrusus infection.
Case 2
The female littermate weighed 1.25 kg and was12 weeks old. Rectal body temperature was38.6 �C. It was moderately dyspneic withoutstertor. Respiratory rate was 50 breaths/min withan abdominal breathing pattern. Arterial pulseswere of normal quality, pulse frequency was180 beats/min. Jugular venous distension orpulsation were not observed. Thoracic ausculta-tion revealed end-inspiratory crackles and a gradeIII/VI systolic heart murmur, with its point ofmaximum intensity on the right hemithorax.Thoracic radiographs showed a complex pulmo-nary pattern throughout the lung fields, predom-inantly characterized by marked bronchial andinterstitial changes but also some alveolar infil-trates. The heart showed right-sided car-diomegaly (Fig. 2A and B). Echocardiographyh
revealed moderate to severe right ventriculardilation (Fig. 3A) and a moderately enlarged rightatrium compared to the left atrium (Fig. 3C).Right ventricular diameter in diastole was 7.7 mm(average reference value: 2.6 mm, range:2.0e3.2 mm)i (Fig. 3A). Left atrial dimensionswere considered normal. The tricuspid valve didnot show structural abnormalities. Pulmonaryartery diameter was 6.8 mm (average referencevalue: 4.3, range: 4.0e4.5 mm)i whereas aorticdiameter was 5.8 mm (average reference value:6.3 mm, range: 5.7e6.9 mm).i This was inter-preted as pulmonary artery dilation (Fig. 4A).
Color Doppler echocardiography showed a largesystolic tricuspid regurgitation. Mild pulmonic valve
i Echocardiographic measurements of right ventricular, aorticand pulmonary artery dimensions in 5 12e13 week old healthykittens. Dirven M. Unpublished data: 2011.
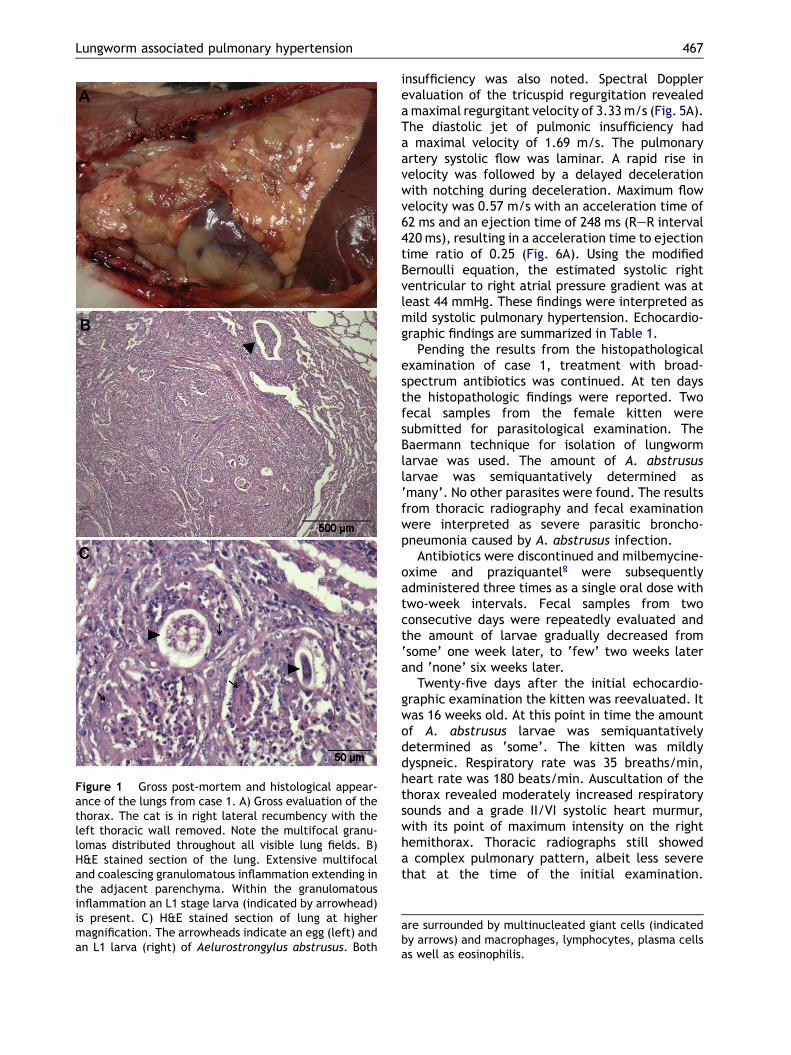
Figure 1 Gross post-mortem and histological appear-ance of the lungs from case 1. A) Gross evaluation of thethorax. The cat is in right lateral recumbency with theleft thoracic wall removed. Note the multifocal granu-lomas distributed throughout all visible lung fields. B)H&E stained section of the lung. Extensive multifocaland coalescing granulomatous inflammation extending inthe adjacent parenchyma. Within the granulomatousinflammation an L1 stage larva (indicated by arrowhead)is present. C) H&E stained section of lung at highermagnification. The arrowheads indicate an egg (left) andan L1 larva (right) of Aelurostrongylus abstrusus. Both
Lungworm associated pulmonary hypertension 467
insufficiency was also noted. Spectral Dopplerevaluation of the tricuspid regurgitation revealedamaximal regurgitant velocity of 3.33m/s (Fig. 5A).The diastolic jet of pulmonic insufficiency hada maximal velocity of 1.69 m/s. The pulmonaryartery systolic flow was laminar. A rapid rise invelocity was followed by a delayed decelerationwith notching during deceleration. Maximum flowvelocity was 0.57 m/s with an acceleration time of62 ms and an ejection time of 248 ms (ReR interval420 ms), resulting in a acceleration time to ejectiontime ratio of 0.25 (Fig. 6A). Using the modifiedBernoulli equation, the estimated systolic rightventricular to right atrial pressure gradient was atleast 44 mmHg. These findings were interpreted asmild systolic pulmonary hypertension. Echocardio-graphic findings are summarized in Table 1.
Pending the results from the histopathologicalexamination of case 1, treatment with broad-spectrum antibiotics was continued. At ten daysthe histopathologic findings were reported. Twofecal samples from the female kitten weresubmitted for parasitological examination. TheBaermann technique for isolation of lungwormlarvae was used. The amount of A. abstrususlarvae was semiquantatively determined as‘many’. No other parasites were found. The resultsfrom thoracic radiography and fecal examinationwere interpreted as severe parasitic broncho-pneumonia caused by A. abstrusus infection.
Antibiotics were discontinued and milbemycine-oxime and praziquantelg were subsequentlyadministered three times as a single oral dose withtwo-week intervals. Fecal samples from twoconsecutive days were repeatedly evaluated andthe amount of larvae gradually decreased from‘some’ one week later, to ‘few’ two weeks laterand ‘none’ six weeks later.
Twenty-five days after the initial echocardio-graphic examination the kitten was reevaluated. Itwas 16 weeks old. At this point in time the amountof A. abstrusus larvae was semiquantativelydetermined as ‘some’. The kitten was mildlydyspneic. Respiratory rate was 35 breaths/min,heart rate was 180 beats/min. Auscultation of thethorax revealed moderately increased respiratorysounds and a grade II/VI systolic heart murmur,with its point of maximum intensity on the righthemithorax. Thoracic radiographs still showeda complex pulmonary pattern, albeit less severethat at the time of the initial examination.
are surrounded by multinucleated giant cells (indicatedby arrows) and macrophages, lymphocytes, plasma cellsas well as eosinophilis.
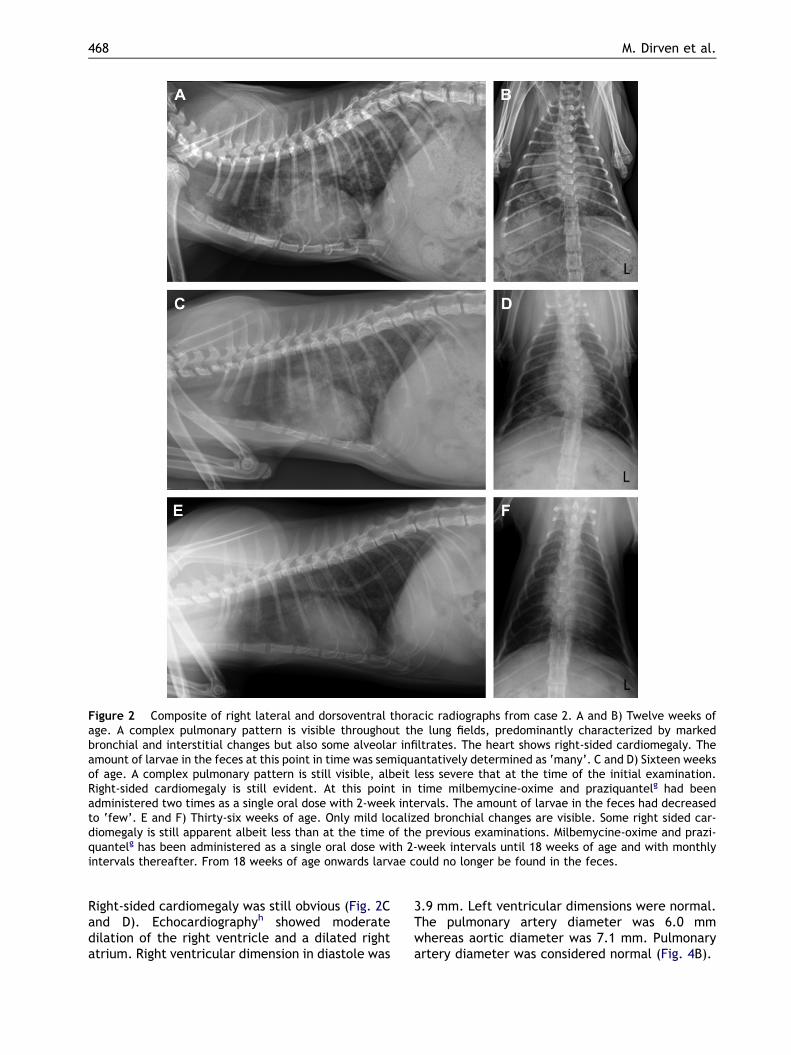
Figure 2 Composite of right lateral and dorsoventral thoracic radiographs from case 2. A and B) Twelve weeks ofage. A complex pulmonary pattern is visible throughout the lung fields, predominantly characterized by markedbronchial and interstitial changes but also some alveolar infiltrates. The heart shows right-sided cardiomegaly. Theamount of larvae in the feces at this point in time was semiquantatively determined as ‘many’. C and D) Sixteen weeksof age. A complex pulmonary pattern is still visible, albeit less severe that at the time of the initial examination.Right-sided cardiomegaly is still evident. At this point in time milbemycine-oxime and praziquantelg had beenadministered two times as a single oral dose with 2-week intervals. The amount of larvae in the feces had decreasedto ‘few’. E and F) Thirty-six weeks of age. Only mild localized bronchial changes are visible. Some right sided car-diomegaly is still apparent albeit less than at the time of the previous examinations. Milbemycine-oxime and prazi-quantelg has been administered as a single oral dose with 2-week intervals until 18 weeks of age and with monthlyintervals thereafter. From 18 weeks of age onwards larvae could no longer be found in the feces.
468 M. Dirven et al.
Right-sided cardiomegaly was still obvious (Fig. 2Cand D). Echocardiographyh showed moderatedilation of the right ventricle and a dilated rightatrium. Right ventricular dimension in diastole was
3.9 mm. Left ventricular dimensions were normal.The pulmonary artery diameter was 6.0 mmwhereas aortic diameter was 7.1 mm. Pulmonaryartery diameter was considered normal (Fig. 4B).
Lungworm associated pulmonary hypertension 469
Color Doppler echocardiography showeda moderate systolic tricuspid regurgitation. A smalldiastolic jet of pulmonic insufficiency was stillnoticed. Spectral Doppler evaluation of thetricuspid regurgitation showed a maximal regur-gitant velocity of 2.55 m/s (Fig. 5B). The diastolicjet of pulmonic insufficiency had a maximalvelocity of 0.56 m/s. The pulmonary outflowvelocity was 0.83 m/s with an acceleration time of33 ms and an ejection time of 133 ms (ReR interval239 ms) resulting in an acceleration time to ejec-tion time ratio of 0.25 (Fig. 6B). The estimatedsystolic right ventricular to right atrial pressuregradient was at least 26 mmHg.
Fifteen days later clinical and radiographicfindings were the same. The amount of A.abstrusus larvae had decreased to ‘few’.
Four months later the kitten was reassessed. Itwas 36 weeks old. The owner had not observed anyrespiratory or other abnormalities. The kitten hadgrown normally. Physical examination did notreveal any abnormalities. Respiratory sounds werenormal. A heart murmur could not be identified.Some local mild bronchial changes were noted onthoracic radiographs. Right sided cardiomegalywas still apparent, albeit less than originally(Fig. 2E and F).
Echocardiographyh showed normal left ventric-ular dimensions and a mildly dilated right ventricleand right atrium. The pulmonary artery was notdilated (Fig. 4C). Color Doppler echocardiographyshowed a very small physiologic low velocitysystolic regurgitant jet originating from thetricuspid valve. Pulmonic insufficiency could notbe identified. Spectral Doppler evaluation of thetricuspid and pulmonic valves did not reveala measurable regurgitant blood flow (Fig. 5C). Thepulmonary outflow velocity was 0.98 m/s with anacceleration time of 67 ms and an ejection time of162 ms (ReR interval 315 ms), resulting ina acceleration time to ejection time ratio of 0.41(Fig. 6C).
Figure 3 Composite of right parasternal two-dimensional and M-mode images from case 2 (A and C)and an age, weight and size matched kitten without clin-ical signs or echocardiographic abnormalities forcomparison (B andD).A) Twelveweeks of age. Severe rightventricular dilatation is present. B) Age, weight and sizematched healthy kitten showing normal right ventriculardimensions. C) Twelve weeks of age. Due to dilation of theright ventricle the internal diameter is increased anda papillary muscle is visible in the middle of the ventricle.The right atrium is enlarged compared to the left atrium.D) Age, weight and size matched healthy kitten. Normaldimensions of the both ventricles and atria.
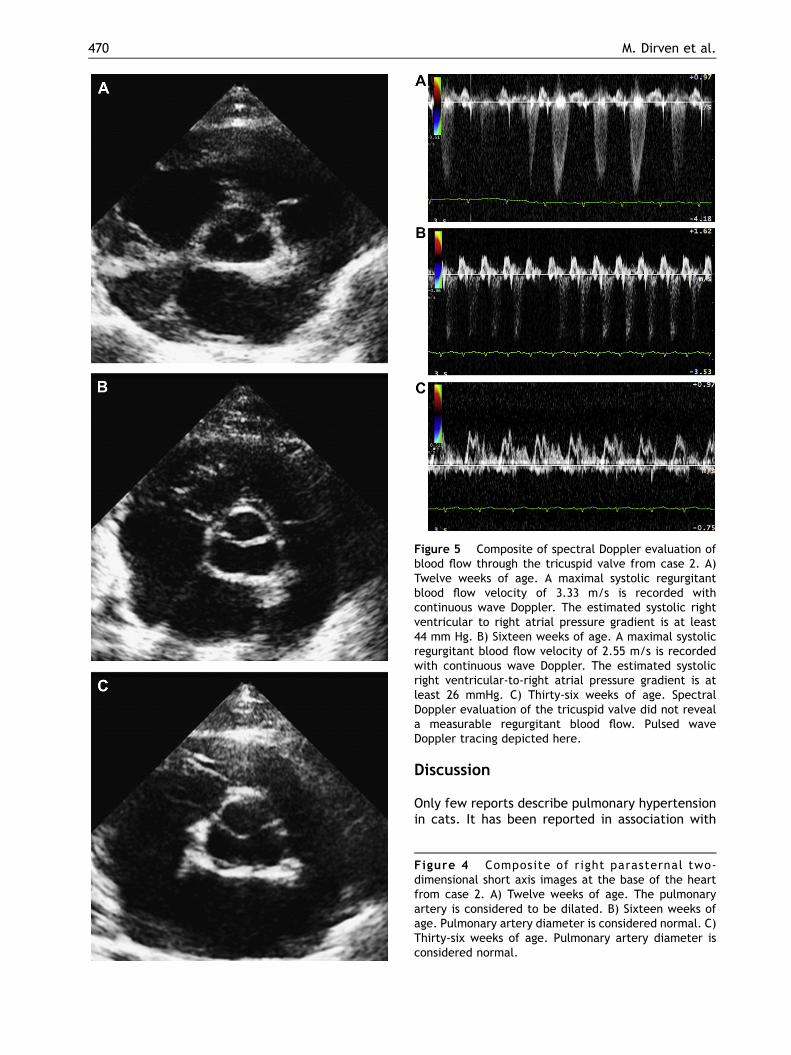
Figure 5 Composite of spectral Doppler evaluation ofblood flow through the tricuspid valve from case 2. A)Twelve weeks of age. A maximal systolic regurgitantblood flow velocity of 3.33 m/s is recorded withcontinuous wave Doppler. The estimated systolic rightventricular to right atrial pressure gradient is at least44 mm Hg. B) Sixteen weeks of age. A maximal systolicregurgitant blood flow velocity of 2.55 m/s is recordedwith continuous wave Doppler. The estimated systolicright ventricular-to-right atrial pressure gradient is atleast 26 mmHg. C) Thirty-six weeks of age. SpectralDoppler evaluation of the tricuspid valve did not reveala measurable regurgitant blood flow. Pulsed waveDoppler tracing depicted here.
470 M. Dirven et al.
Discussion
Only few reports describe pulmonary hypertensionin cats. It has been reported in association with
Figure 4 Composite of right parasternal two-dimensional short axis images at the base of the heartfrom case 2. A) Twelve weeks of age. The pulmonaryartery is considered to be dilated. B) Sixteen weeks ofage. Pulmonary artery diameter is considered normal. C)Thirty-six weeks of age. Pulmonary artery diameter isconsidered normal.
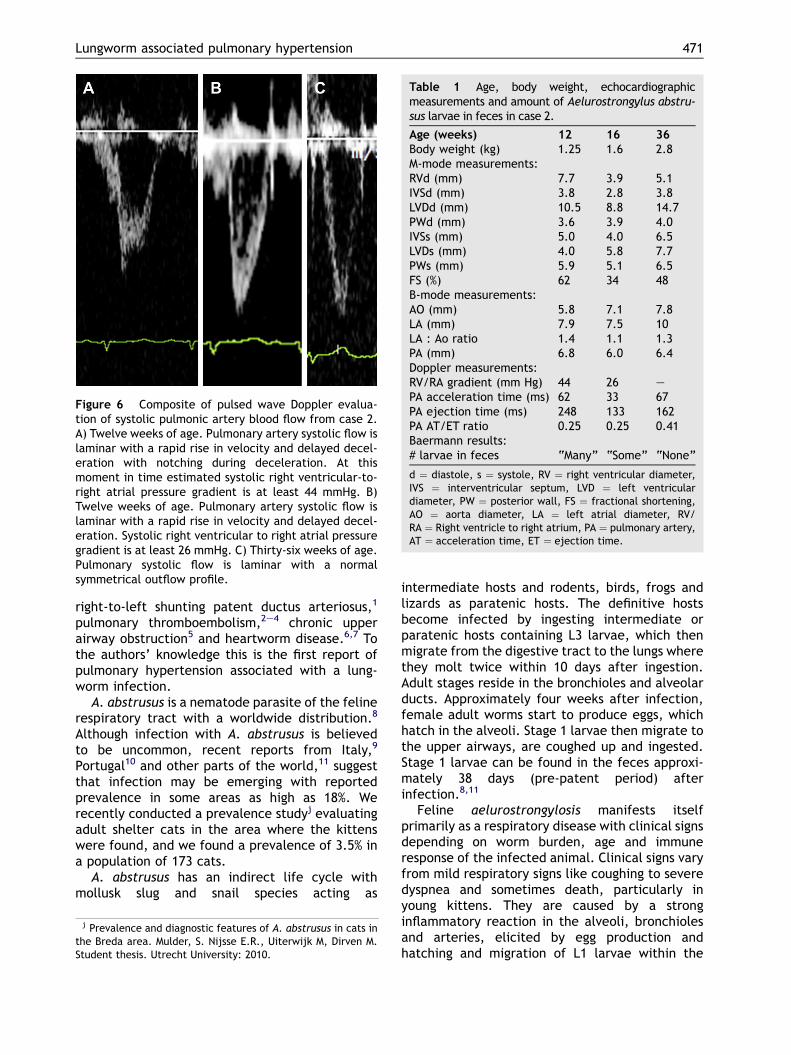
Figure 6 Composite of pulsed wave Doppler evalua-tion of systolic pulmonic artery blood flow from case 2.A) Twelve weeks of age. Pulmonary artery systolic flow islaminar with a rapid rise in velocity and delayed decel-eration with notching during deceleration. At thismoment in time estimated systolic right ventricular-to-right atrial pressure gradient is at least 44 mmHg. B)Twelve weeks of age. Pulmonary artery systolic flow islaminar with a rapid rise in velocity and delayed decel-eration. Systolic right ventricular to right atrial pressuregradient is at least 26 mmHg. C) Thirty-six weeks of age.Pulmonary systolic flow is laminar with a normalsymmetrical outflow profile.
Table 1 Age, body weight, echocardiographicmeasurements and amount of Aelurostrongylus abstru-sus larvae in feces in case 2.
Age (weeks) 12 16 36Body weight (kg) 1.25 1.6 2.8M-mode measurements:RVd (mm) 7.7 3.9 5.1IVSd (mm) 3.8 2.8 3.8LVDd (mm) 10.5 8.8 14.7PWd (mm) 3.6 3.9 4.0IVSs (mm) 5.0 4.0 6.5LVDs (mm) 4.0 5.8 7.7PWs (mm) 5.9 5.1 6.5FS (%) 62 34 48B-mode measurements:AO (mm) 5.8 7.1 7.8LA (mm) 7.9 7.5 10LA : Ao ratio 1.4 1.1 1.3PA (mm) 6.8 6.0 6.4Doppler measurements:RV/RA gradient (mm Hg) 44 26 ePA acceleration time (ms) 62 33 67PA ejection time (ms) 248 133 162PA AT/ET ratio 0.25 0.25 0.41Baermann results:# larvae in feces “Many” “Some” “None”
d ¼ diastole, s ¼ systole, RV ¼ right ventricular diameter,IVS ¼ interventricular septum, LVD ¼ left ventriculardiameter, PW ¼ posterior wall, FS ¼ fractional shortening,AO ¼ aorta diameter, LA ¼ left atrial diameter, RV/RA ¼ Right ventricle to right atrium, PA ¼ pulmonary artery,AT ¼ acceleration time, ET ¼ ejection time.
Lungworm associated pulmonary hypertension 471
right-to-left shunting patent ductus arteriosus,1
pulmonary thromboembolism,2e4 chronic upperairway obstruction5 and heartworm disease.6,7 Tothe authors’ knowledge this is the first report ofpulmonary hypertension associated with a lung-worm infection.
A. abstrusus is a nematode parasite of the felinerespiratory tract with a worldwide distribution.8
Although infection with A. abstrusus is believedto be uncommon, recent reports from Italy,9
Portugal10 and other parts of the world,11 suggestthat infection may be emerging with reportedprevalence in some areas as high as 18%. Werecently conducted a prevalence studyj evaluatingadult shelter cats in the area where the kittenswere found, and we found a prevalence of 3.5% ina population of 173 cats.
A. abstrusus has an indirect life cycle withmollusk slug and snail species acting as
j Prevalence and diagnostic features of A. abstrusus in cats inthe Breda area. Mulder, S. Nijsse E.R., Uiterwijk M, Dirven M.Student thesis. Utrecht University: 2010.
intermediate hosts and rodents, birds, frogs andlizards as paratenic hosts. The definitive hostsbecome infected by ingesting intermediate orparatenic hosts containing L3 larvae, which thenmigrate from the digestive tract to the lungs wherethey molt twice within 10 days after ingestion.Adult stages reside in the bronchioles and alveolarducts. Approximately four weeks after infection,female adult worms start to produce eggs, whichhatch in the alveoli. Stage 1 larvae then migrate tothe upper airways, are coughed up and ingested.Stage 1 larvae can be found in the feces approxi-mately 38 days (pre-patent period) afterinfection.8,11
Feline aelurostrongylosis manifests itselfprimarily as a respiratory disease with clinical signsdepending on worm burden, age and immuneresponse of the infected animal. Clinical signs varyfrom mild respiratory signs like coughing to severedyspnea and sometimes death, particularly inyoung kittens. They are caused by a stronginflammatory reaction in the alveoli, bronchiolesand arteries, elicited by egg production andhatching and migration of L1 larvae within the

472 M. Dirven et al.
respiratory tract.11e13 Radiographic pulmonaryabnormalities caused by A. abstrusus infectionvary depending on worm burden and elapsed timeafter infection. Peribronchial thickening andlocalized interstitial changes are apparent in earlydisease followed by generalized alveolar diseaseduring L1 production 5e21 weeks after infection.After resolution of alveolar disease, bronchial wallthickening and increased interstitial opacity mayremain visible for months.14,15
The response of the right heart and pulmonaryvasculature to infection with A. abstrusus wasstudied by Rawlings et al in the early 1980’s. Theyevaluated experimentally infected cats withthoracic radiographs, electrocardiograms,ventricular weights and pulmonary artery cathe-terization for pressure determination and arterio-grams. Remarkably no signs of pulmonaryhypertension or an associated right ventricularresponse were found in that study.16
The appearance of a heart murmur, rightventricular and pulmonary artery dilation and anincreased systolic right ventricular-to-right atrialpressure gradient in case 2 are compatible withpulmonary hypertension. At the time of the initialinvestigation, clinical and radiological findingscombined with the results from the Baermannexamination in case 2 and the histopathologyresults in case 1, show that severe A. abstrususinfection was present. The resolution of the heartmurmur and echocardiographic abnormalities withtreatment of A. abstrusus, suggest that pulmonaryhypertension was associated with A. abstrususinfection.
Many classification schemes exist to categorizepulmonary hypertension. A frequently used clinicalclassification in man categorizes pulmonaryhypertension as either pulmonary arterial hyper-tension, pulmonary hypertension owing to leftheart disease, pulmonary hypertension owing tolung diseases and/or hypoxemia, chronic throm-boembolic pulmonary hypertension and pulmonaryhypertension with unclear multifactorial mecha-nisms.17 Via this classification pulmonary hyper-tension in case 2 may be associated with eitherpulmonary arterial changes as well as lung diseaseand/or hypoxemia.
Changes in the pulmonary arteries subsequentto A. abstrusus infection have been welldescribed.13,18 Hyperplasia and hypertrophy of thesmooth muscle cells of the media and intimalproliferation are common features and result innarrowing of the lumen of pulmonary vasculature.These changes are apparent approximately 12weeks post-infection and resemble vascularchanges as seen in human pulmonary arterial
hypertension.19 Medial hypertrophy is not specificto A. abstrusus infection. It may be associatedwith Dirofilaria immitis infection but is alsoconsidered to be a spontaneous lesion in cats,occurring in both conventional and specific-pathogen-free cats.20 However in case 1 nochanges in the media and intima were noted.Given the age of the animal, infection could nothave been present for more than 4e6 weeks,which could explain the absence of vascularchanges. Therefore it is possible that suspectedpulmonary hypertension occurred secondary tolung disease and/or hypoxemia. Diffuse alveolardisease possibly will lead to impaired oxygenexchange in the lungs.15 It remains speculativethat hypoxemia was the cause of pulmonaryhypertension in case 2 as arterial blood gas anal-ysis was not performed. Alternatively, A. abstrususinfection may cause prolonged vasoconstrictionmediated by mast cells and histamine release16
triggering increased pulmonary vascular resis-tance and pulmonary hypertension. Exactly how A.abstrusus causes pulmonary hypertension remainsto be elucidated.
As only few reports describe pulmonary hyper-tension in cats, clinical characteristics of pulmo-nary hypertension remain ill defined. Dyspnea,jugular venous distension and a systolic heartmurmur best heard on the right side of the thoraxhave all been reported.1e6 Clinical signs in dogswith symptomatic pulmonary hypertension includedyspnea, cough, lethargy, syncope, exerciseintolerance and ascites.21e24 In case 1 and 2 severedyspnea and a heart murmur was observed. In ourcase dyspnea may have been attributable topulmonary disease, yet dyspnea and pulmonaryhypertension decreased within two weeks aftertreatment, whereas radiographic pulmonaryabnormalities remained apparent much longer.
In the present case report pulmonary hyperten-sion was suspected based on the echocardiographicfindings in case 2. In dogs echocardiographicfeatures of pulmonary hypertension include eccen-tric and concentric right ventricular hypertrophy,main pulmonary artery dilation, diastolic pulmonicvalve insufficiency with a maximum regurgitantvelocity >2.2 m/s, pulmonary outflow profileshowing rapid rise in pulmonary flow and delayeddeceleration with or without midsystolic notching,and an acceleration time to ejection time ratio lessthan 0.3 and systolic tricuspid regurgitation witha maximum regurgitant velocity >2.8 m/s.21e24
Although specific echocardiographic characteris-tics in cats have not been widely reported, anec-dotal findings suggest that the same criteria mayapply to cats.1e6 In case 2 we describe all of the
Lungworm associated pulmonary hypertension 473
previously stated criteria. Furthermore weobserved a resolution of pulmonary artery dilationand tricuspid regurgitation and a normalization ofthe pulmonary artery outflow profile and accelera-tion time to ejection time ratio, suggesting thatpulmonary hypertension in case 2 was the cause ofthe echocardiographic changes.
In the Netherlands no drug is licensed specifi-cally for treatment of A. abstrusus. Some evidencesuggests that avermectines including milbemycinmay be effective for treatment of cardiopulmo-nary parasites.25e27 As milbemycine-oxime andpraziquantelg matched the animal sheltersanthelmintic protocol, it was selected for treat-ment. In case 2 repeated administration ofmilbemycine-oxime and praziquantelg with twoweek intervals resulted in cessation of L1-sheddingand resolution of clinical signs over a period of sixweeks. No specific treatment for pulmonaryhypertension was instigated. With treatmenteventually clinical signs of dyspnea, estimatedpulmonary artery pressure and radiographicpulmonary abnormalities normalized.
In conclusion, severe A. abstrusus infection maylead to acquired heart disease in cats as young as12 weeks of age. Exactly how A. abstrusus causespulmonary hypertension remains to be elucidated.A. abstrusus bronchopneumonia and associatedpulmonary hypertension resolved after repeatedtreatment with milbemycine-oxime.
Conflict of interest
There are no conflicts of interest.
Acknowledgment
The authors would like to thank Sander de Kock forhis help with the manuscript.
References
1. Connolly DJ, Lamb CR, Boswood A. Right-to-left shuntingpatent ductus arteriosus with pulmonary hypertension ina cat. J Small Anim Pract 2003;44:184e188.
2. Baron Toaldo M, Guglielmini C, Diana M, Giunti M, Dondi F,Cipone M. Reversible pulmonary hypertension in a cat. JSmall Anim Pract 2011;52:271e277.
3. Pouchelon JL, Chetboul V, Devauchelle P, Delisle F, Mai W,Vial V. Diagnosis of pulmonary thromboembolism in a catusing echocardiography and pulmonary scintigraphy. J SmallAnim Pract 1997;38:306e310.
4. Sottiaux J, Franck M. Pulmonary embolism and cor pulmo-nale in a cat. J Small Anim Pract 1999;40:88e91.
5. MacPhail CM, Innocenti CM, Kudnig ST, Veir JK,Lappin MR. Atypical manifestations of feline inflamma-tory polyps in three cats. J Feline Med Surg 2007;9:219e225.
6. Small MT, Atkins CE, Gordon SG, Birkenheuer AJ, Booth-Sayer MA, Keene BW, Fujii Y, Miller MW. Use of a nitinolgooseneck snare catheter for removal of adult Dirofilariaimmitis in two cats. J Am Vet Med Assoc 2008;233:1441e1445.
7. Rawlings CA. Pulmonary arteriography and hemodynamicsduring feline heartworm disease. Effect of aspirin. J VetIntern Med 1990;4:285e291.
8. Anderson RC. The superfamily metastrongyloidea. In:Nematode parasites of vertebrates. Their development andtransmission. 2nd ed. Guildford UK: Cabi Publishing; 2000.p. 162e163.
9. Traversa D, Lia RP, Iorio R, Boari A, Paradies P,Capelli G, Avolio S, Otranto D. Diagnosis and risk factorsof Aelurostrongylus abstrusus (Nematoda, Strongylida)infection in cats from Italy. Vet Parasitol 2008;153:182e186.
10. Payo-Puente P, Botelho-Dinis M, Carvaja Uruena AM, Payo-Puente M, Gonzalo-Orden JM, Rojo-Vazquez FA. Prevalencestudy of the lungworm Aelurostrongylus abstrusus in straycats of Portugal. J Feline Med Surg 2008;10:242e246.
11. Traversa D, Guglielmini C. Feline aelurostrongylosis andcanine angiostrongylosis: a challenging diagnosis for twoemerging verminous pneumonia infections. Vet Parasitology2008;157:163e174.
12. Pechman RD. Respiratory parasites. In: Sherding RD, editor.The cat: diseases and clinical management. New York:Churchill Livingstone; 1995. p. 613e622.
13. Stockdale PH. The pathogenesis of the lesions elicited byAelurostrongylus abstrusus during its prepatent period. VetPath 1970:102e115.
14. Losonsky JM, Thrall DE, Prestwood AK. Radiographic eval-uation of pulmonary abnormalities after Aelurostrongylusabstrusus inoculation in cats. Am J Vet Res 1983;44:478e482.
15. Mahaffey MB. Radiographic-pathologic findings in experi-mental Aelurostrongylus abstrusus infection in cats. J AmVet Rad Soc 1979;20:81.
16. Rawlings CA, Losonsky JM, Lewis RE, Hubble JJ,Prestwood AK. Response of the feline heart to Aeluros-trongylus abstrusus. J AmAnimHosp Assoc 1980;16:573e578.
17. Simonneau G, Robbins IM, Beghetti M, Channick RN,Delcroix M, Denton CP, Elliott CG, Gaine SP, Gladwin MT,Jing ZC, Krowka MJ, Langleben D, Nakanishi N, Souza R.Updated clinical classification of pulmonary hypertension. JAm Coll Cardiol 2009;30:43Se54S.
18. Naylor JR, Hamilton JM, Weatherley AJ. Changes in theultrastructure of feline pulmonary arteries followinginfection with the lungworm Aelurostrongylus abstrusus. BrVet J 1984;140:181e190.
19. Rich S, McLaughlin VV. Pulmonary hypertension. In: Libby P,Bonow RO, Mann DL, Zipes DP, editors. Braunwald’s heartdisease, a textbook of cardiovascular medicine. 8th ed.Philadelphia: Saunders Elsevier; 2008. p. 1891.
20. McCracken, Patton S. Pulmonary arterial changes in felineDirofilariasis. Vet Pathol 1993;30:64e69.
21. Johnson L, Boon J, Orton EC. Clinical characteristics of 53dogs with Doppler-derived evidence of pulmonary hyper-tension: 1992-1996. J Vet Intern Med 1999;13:440e447.
22. Bach JF, Rozanski EA, MacGregor J, Betkowski JM, Rush JE.Retrospective evaluation of sildenafil citrate as a therapyfor pulmonary hypertension in dogs. J Vet Intern Med 2006;20:1132e1135.

474 M. Dirven et al.
23. Schober KE, Baade H. Doppler echocardiographic predictionof pulmonary hypertension in West Highland White Terrierswith chronic pulmonary disease. J Vet Intern Med 2006;20:912e920.
24. Pyle RL, Abbott J, MacLean H. Pulmonary hypertension andcardiovascular sequelae in 54 dogs. Intern J Appl Res VetMed 2004;2:99.
25. Traversa D, Di Cesare A, Milillo P, Lohr B, Iorio R,Pampurini F, Schaper R, Paoletti B, Heine J. Efficacy andsafety of imidacloprid 10%/moxidectin 1% spot-on
formulation in the treatment of feline aelurostrongylosis.Parasitol Research 2009;105:S55eS62.
26. Genchi C, Cody R, Pengo G, Buscher G, Cavalleri D, Bucci V,Junquera P. Efficacy of a single milbemycin oxime admin-istration in combination with praziquantel against experi-mentally induced heartworm (Dirofilaria immitis) infectionin cats. Vet Parasitol 2004;122:287e292.
27. Conboy G. Natural infections of Crenosoma vulpis andAngiostrongylus vasorum in dogs in Atlantic Canada and theirtreatment with milbemycin oxime. Vet Rec 2004;155:16e18.
Available online at www.sciencedirect.com