forame oval para epilepsia temporal mesial.pdf
TRANSCRIPT

8/11/2019 Forame Oval para Epilepsia temporal mesial.pdf
http://slidepdf.com/reader/full/forame-oval-para-epilepsia-temporal-mesialpdf 1/8
Epilepsia, 47(8):1300–1307, 2006Blackwell Publishing, Inc.C 2006 International League Against Epilepsy
Foramen Ovale Electrodes Can Identify a Focal Seizure Onset
When Surface EEG Fails in Mesial Temporal Lobe Epilepsy
∗Tonicarlo R. Velasco, ∗Americo C. Sakamoto, ∗Veriano Alexandre Jr., ∗Roger Walz, ∗Charles L.
Dalmagro, ∗Marino M. Bianchin, ∗†David Araujo, ∗†Antonio C. Santos, †Joao P. Leite, ‡Joao A.
Assirati, and ‡Carlos Carlotti Jr.
∗CIREP, Centro de Cirurgia de Epilepsia, Faculdade de Medicina de Ribeir ˜ ao Preto, †Departamento de Neurologia, Psiquiatria e
Psicologia M edica, and ‡Departamento de Anatomia e Cirurgia, Universidade de S ˜ ao Paulo, S ao Paulo, Brazil
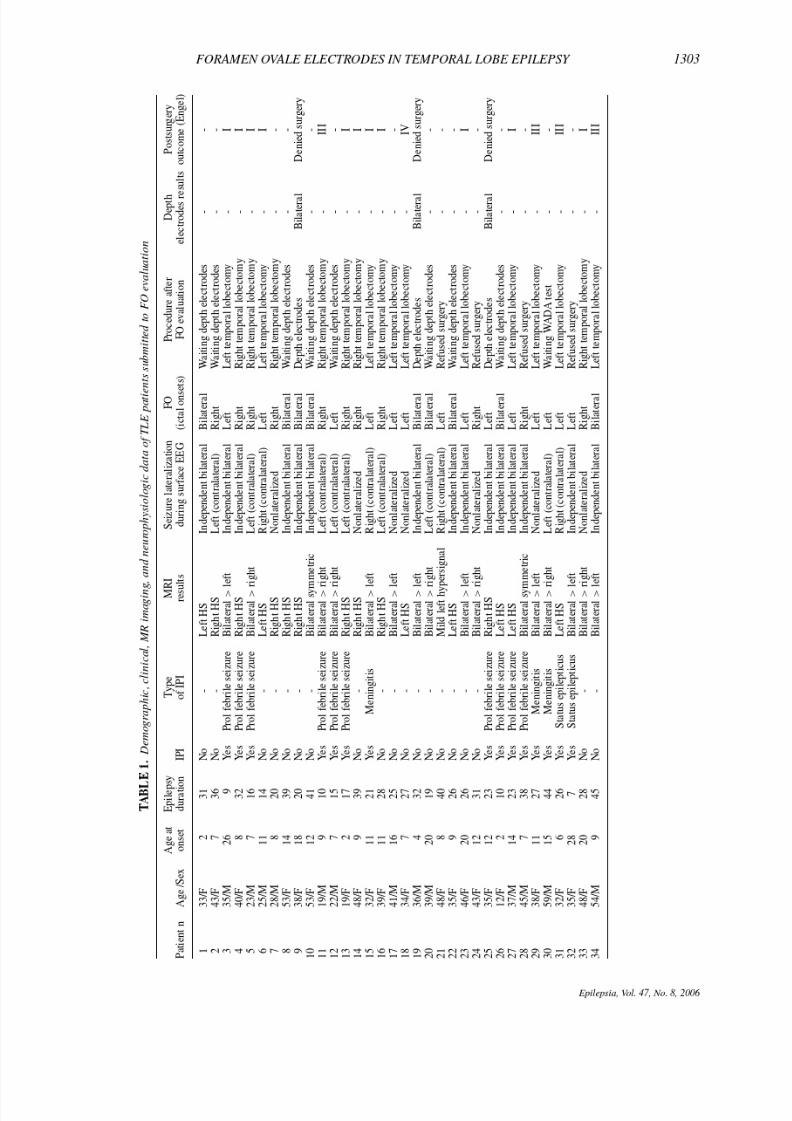
Summary: Purpose: We analyze a series of patients with
mesial temporal lobe epilepsy (MTLE) associated with hip-pocampal sclerosis (HS) submitted to presurgical investigationwith scalp sphenoidal, followed by foramen ovale electrodes(FO), and, when necessary, with depth temporal electrodes. Wesought to evaluate the clinical utility of FO in patients withMTLE-HS.
Methods: We included patients who had phase I investigationwith bitemporal independent seizures, nonlateralized ictal on-sets, or ictal onset initiating in the side contralateral to the sideof hippocampal sclerosis. Patients whose implanted FO failedto demonstrate an unambiguous unilateral ictal onset were laterevaluated with depth hippocampal electrodes.
Results: Between May 1994 and December 2004, 64 patientsmet our inclusion criteria: 33 female (51.5%) and 31 male sub-
jects (48.5%). The mean age at enrollment was 37.66 ± 10.6
years (range, 12–56 years). The groups with nonlateralized sur-face ictal EEG onsets and contralateral EEG onsets had a greaterchance of lateralization with FO when compared with the groupwith bilateral independent seizures on surface EEG (p < 0.01).Foramen ovale electrodes lateralized the seizures in 60% of pa-tients. Seventy percent of patients became seizure free after tem-poral lobectomy. Five patients were implanted with depth tem-poral electrodes after FO video-EEG monitoring. The depth-electrode EEG onsets confirmed the results of FO video-EEGmonitoring in all patients, and the surgery was refused.
Conclusions: In MTLE-HS, FO is a reliable method for lat-eralization of seizures that are not clearly recorded by sur-face EEGs. Key Words: Epilepsy—Mesial temporal lobeepilepsy—Epilepsy surgery—Foramen ovale electrodes—EEG.
Mesial temporal lobe epilepsy associated with hip-
pocampal sclerosis (MTLE-HS) is the commonest type
of pharmacologically intractable epilepsy. However, after
a careful preoperative evaluation, 60–70% of MTLE-HS
patients can be rendered seizure free after temporal lobec-
tomy (1).
In many candidates for temporal lobe resection, the
seizure focus can be accurately lateralized and patients
selected for surgery by using noninvasive investiga-
tions, such as high-resolution magnetic resonance imaging
(MRI), noninvasive video-EEG monitoring, and positron
emission tomography (PET) and single-photon emission
computed tomography (SPECT) studies (2). Surface inter-
ictal and ictal EEG recordings remain an essential element
of the presurgical evaluation in patients with MTLE-HS
to demonstrate the presence of unilateral epileptogene-
Accepted February 6, 2006.
Address correspondence and reprint requests to Dr. T.R. Velasco atCIREP 4◦ andar, Hospital das Clinicas de Ribeirao Preto, Universidadede Sao Paulo 14.048-900, SP, Brasil. E-mail: [email protected]
doi: 10.1111/j.1528-1167.2006.00547.x
sis. Notably, the definition of the seizure-onset zone by
surface ictal EEG generally provides an accurate estima-
tion of the epileptogenic zone, defined as the area of cor-
tex necessary and sufficient for the generation of clinical
seizures (3).
However, in ∼30% of MTLE-HS patients, scalp-
sphenoidal EEG recordings fail to demonstrate an un-
ambiguous unilateral ictal onset, showing contralateral,
bitemporal independent, and nonlateralized ictalonsets, or
the surface EEG recordings are not interpretable because
of movement artifacts (4,5). Conversely, a bilateral scalp
onset is still compatible with a unilateral mesial temporal
onset and should not deter further surgical assessment (6).
When noninvasive studies remain nonconcordant or un-
certain regarding the localization of seizure onset, invasive
studies such as those with depth electrodes may be needed
(7). Nevertheless, the proportion of patients evaluated with
depth electrodes has decreased over the last decade, be-
cause of our increasing ability to localize epileptogenic
lesions such as HS with high-resolution MRI, and because
invasive electrodes carry considerable costs and risks of
complications (3).
1300

8/11/2019 Forame Oval para Epilepsia temporal mesial.pdf
http://slidepdf.com/reader/full/forame-oval-para-epilepsia-temporal-mesialpdf 2/8
FORAMEN OVALE ELECTRODES IN TEMPORAL LOBE EPILEPSY 1301
To record from the mesiobasal aspect of the temporal
lobe, Wieser et al. (8–10) developed a subdural electrode
inserted through the foramen ovale (FO). This procedure
is safe and can be an alternative to invasive implantation
of depth electrodes in MTLE patients who are candidates
for temporal lobectomy.
Here we describe a series of patients with MTLE-HSsubmitted to a progressive presurgical investigation with
scalp sphenoidal, followedby FO anddepthtemporalelec-
trodes when necessary. Our findings agreed with previous
descriptions showing that, in patients whose surface EEG
fails to demonstrate an unequivocal unilateral ictal onset,
FO might provide relevant and sufficient information to
give an indication for resective surgery.
METHODS
Subjects
Patients with suspected MTLE-HS evaluated at the
Ribeirao Preto Epilepsy Surgery Center at University of Sao Paulo School of Medicine, between January 1996 and
June 2004, were included in the study. The presurgical
protocol was approved by our University Hospital Ethics
Committee, and an informed consent was obtained from
all subjects.
Phase I investigation for epilepsy surgery consisted
of an assessment made by a neurologist with expertise
in epileptology, structural and functional neuroimaging,
neuropsychological examination, and scalp-sphenoidal
video-EEG monitoring.
The decision to implant FO was based on the results of
the phase I investigation. Patients with a clear hypothesisregarding the location of the epileptogenic zone in mesial
temporal lobes, but whose surface EEGs failed to demon-
strate unilateral ictal onsets, were submitted to investiga-
tion with FO. When implanted FO also failed to demon-
strate an unambiguous unilateral ictal onset, patients were
further evaluated with depth temporal electrodes.
The inclusion criteria were (a) medical history and
seizure semiology consistent with intractable MTLE, usu-
ally with epigastric, autonomic, or psychic auras, followed
by behavioral arrest, progressive clouding of conscious-
ness, oroalimentary and manual automatisms, and auto-
nomic phenomena; (b) no other lesion than the presence of
atrophy or hippocampal signal changes at high-resolution
MRI; and (c) ictal EEG with bitemporal independent ic-
tal EEG onsets, nonlateralized ictal onsets, or ictal onsets
initiating contralateral to the temporal lobe with focal ab-
normalities detected on high-resolution MRI.
Vıdeo-EEG monitoring
Video-EEG analysis
EEG signals were obtained by using a digital video-
EEG system (Vangard Systems, Cleveland Clinic Foun-
dation, Cleveland, OH, U.S.A.). Surface electrodes were
placed over the scalp according to the international 10–20
system, added by temporal electrodes positioned accord-
ing to the “10–10 system” plus bilaterally placed sphe-
noidal electrodes. At least two events similar to the pa-
tient’s habitual seizures were recorded.
Interictal spikes
The frequency, lateralization ratio, and localization of
interictal spikes (ISs) were visually assessed by board-
certified electroencephalographers.For the analysis of ISs,
5-min EEG samples were collected every hour, 24 h/day.
Spikes and sharp waves were defined according to the In-
ternationalFederationof Clinical Neurophysiology guide-
lines.
Ictal-onset zone
The ictal-onset zone (IOZ) was independently assessed
on ictal video-EEG by two investigators, and when the
results were discordant, they were reviewed together to
achieve agreementaboutthe localization and lateralizationof seizure onset.
Foramen ovale electrodes insertion
Commercially available FOs (AdTech) with four con-
tacts at 5-mm intervals were implanted percutaneously
with the aid of a fluoroscope under light general anesthe-
sia. Electrodes were positioned in such way that the tip
(contact 1) was located at the end of the ambient cistern,
with contact 4 placed just above the level of the foramen
ovale. Immediately after the procedure, a skull radiograph
was taken to confirm whether the FO implantation posi-
tions were adequate and bilaterally symmetrical.
MRI-guided stereotactic depth electrode implantation
A surgical plan based on an entry and target points on
axial and sagittal images was defined for the insertion of
depth electrodes. Navigational views, using three-planar
images, were performed to determine which structures the
electrodes would pass through to be correctly placed in
the amygdala and hippocampus. The correct site of depth
electrode implantation was confirmed by MRI.
Neuroimaging
Neuroimaging studies included high-resolution MRI
(1.5-T Siemens Magneton Vision, Erlangen, Germany)
with special protocols for epilepsy and interictal and ictalSPECT. Based on visual analysis of MRI, the neuro-
radiologists classified hippocampal sclerosis as (a) uni-
lateral, when hippocampal atrophy (on T1-weighted 1-
mm isotropic-voxel SPGR sequence) or increased signal
(on T2-weighted sequences: turbo-spin echo and fluid-
attenuated inversion recovery sequences) were observed
in oneside;or (b) bilateral, when thehippocampalchanges
were observed on both sides.
If the abnormality was increased signal intensity with-
out hippocampal atrophy, the radiologists did not clas-
sify it as HS. However, increased hippocampal signal
Epilepsia, Vol. 47, No. 8, 2006

8/11/2019 Forame Oval para Epilepsia temporal mesial.pdf
http://slidepdf.com/reader/full/forame-oval-para-epilepsia-temporal-mesialpdf 3/8
1302 T. R. VELASCO ET AL.
intensities were considered abnormal for the lateraliza-
tion of neuroimaging features and for the correlation with
ictal studies.
Surgical outcome was defined according to the classi-
fication proposed by Engel (11).
Statistical analysis
The χ2 test or Fisher’s exact test was used to establish
correlation between categoric variables. A t test or Mann–
Whitney test was used to analyze numeric variables, such
as age at seizure onset, age, or epilepsy duration.
RESULTS
Clinical and demographic data
The clinical, demographic, MRI, and neurophysiologic
data are summarized in Table 1. Between 1996 and 2004,
65 patients were submitted to evaluation with FO and
were included in the analysis: 35 female (53.8%) and
30 male patients (46.2%). The mean age at enrollment
was 37.8 ± 10.1 years (range, 12–59 years). The mean
age at epilepsy onset was 12.2 ± 6.9 years (range, 1–
36 years). The epilepsy duration was 25.5 years ± 9.8
years (range, 4–45 years). The mean seizure frequency be-
fore surgery was 6.8± 7.5 seizures per month. Thirty-five
(53.8%) patients had initial precipitant insults (IPIs), and
prolonged febrile seizure was the most common type of
IPI (60%). The mean age at IPI was 3.2± 4.7 years (range,
1–28 years).
MRI findings
Thirty-one (47.6%) had bilateral abnormalities, 25 with
bilateral asymmetrical and six with bilateral symmetri-cal abnormalities. Thirty-four patients had unilateral MRI
findings: 18 (27.7%) patients had right HS, 15 (26.2%)
patients had left HS, and mild left increased hippocampus
signal intensity without hippocampal atrophy was found
in one (1.5%) patient.
EEG data
The mean duration of video-EEG monitoring (VEEG)
with scalp-sphenoidal electrodes was 6.0± 2 days (range,
2–13 days). The median of recorded seizures was five
seizures (range, 2–17 seizures). The most frequent reason
for FO implantation was independent bilateral seizures re-
vealed by surface EEG in 26 (40.0%) patients, followedbysurface EEG onsets contralateral to the side of hippocam-
pal atrophy in 23 (35.4%) patients, and nonlateralized ictal
discharge onsets in 16 (24.6%) patients. In the nonlateral-
ized group, eight (50%) patients had bilateral HS.
FO evaluation revealedunilateral EEG onsets ipsilateral
to the side of HS in 19 patients with unilateral HS and
ipsilateral to the side of the more intense HS in 14 patients
with bilateral asymmetrical HS.
In the nonlateralized group by surface EEG, 14 (87.5%)
of 16 patients had lateralized EEGs during FO evaluation.
In the group with contralateral surface EEG onsets, the
proportion of patients with lateralized EEGs was 52.2%
(12 of 23 patients). These groups had a greater chance of
lateralization with FO when compared with the group with
bilateral independent seizures on surface EEG (34.6%,
nineof 26; p< 0.01). In eight patients, the FO EEG onsets
were unilateral but contralateral to the side of HS, and
depth electrodes were indicated.In relation to the lateralization of HS, 10 (32.2%) of 31
patients with bilateral HS revealed bilateral EEG onsets
during FO recording, and 10 (29.41%) of 34 patients with
unilateral HS had bilateral EEG onsets (p= 0.66, Fisher’s
Exact test).
Five patients were submitted to implantation of depth
temporal electrodes after FO video-EEG monitoring. The
indications for depth electrodes were bilateral EEG onsets
(four patients) and seizures contralateral to the side of HS
(one patient) revealed during FO evaluation. The depth-
electrode evaluation results yielded findings very similar
to the results of FO VEEG monitoring in all patients, and
the surgery was refused. Fifteen (23%) patients who had
bilateral or contralateral EEG onsets on FO recordings are
currently waiting for depth-electrode evaluation.
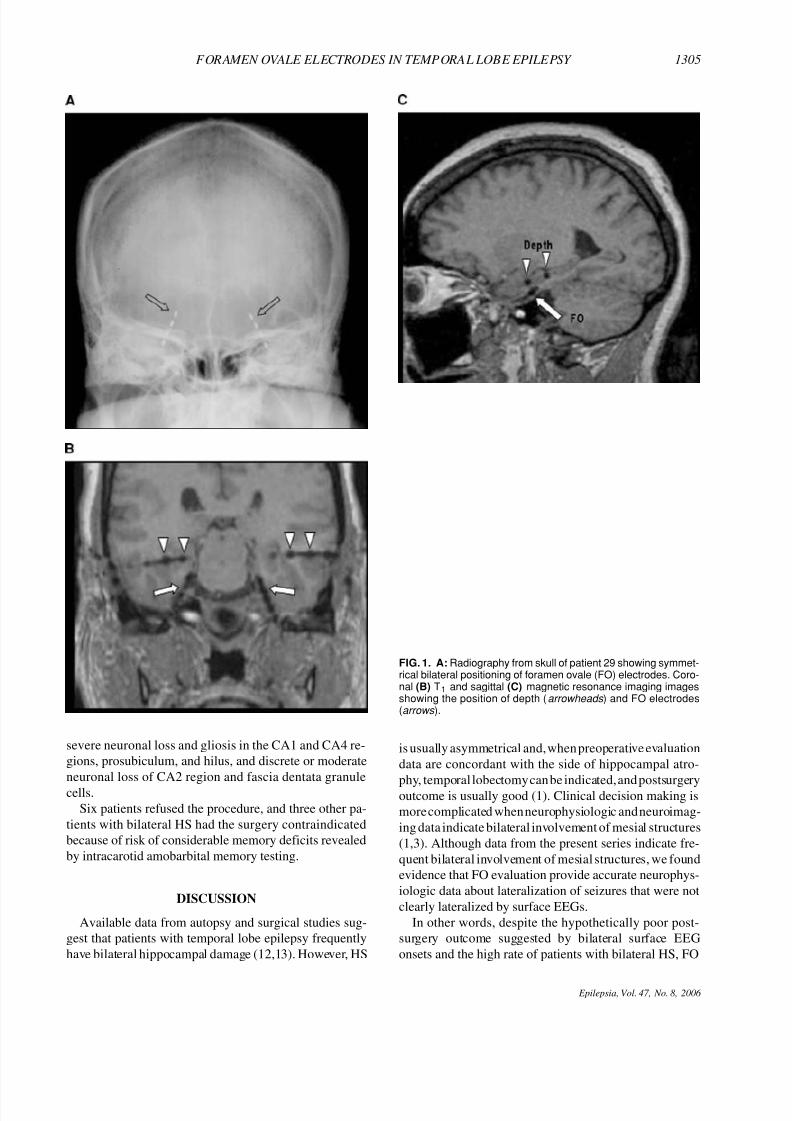
In one patient, the FO electrode had bilateral indepen-
dent EEG onsets and depth electrodes were added, allow-
ing simultaneous FO and depth-electrode recordings. MR
imaging of implanted electrodes revealed that the FO elec-
trodes were in close relation to the parahippocampal gyrus
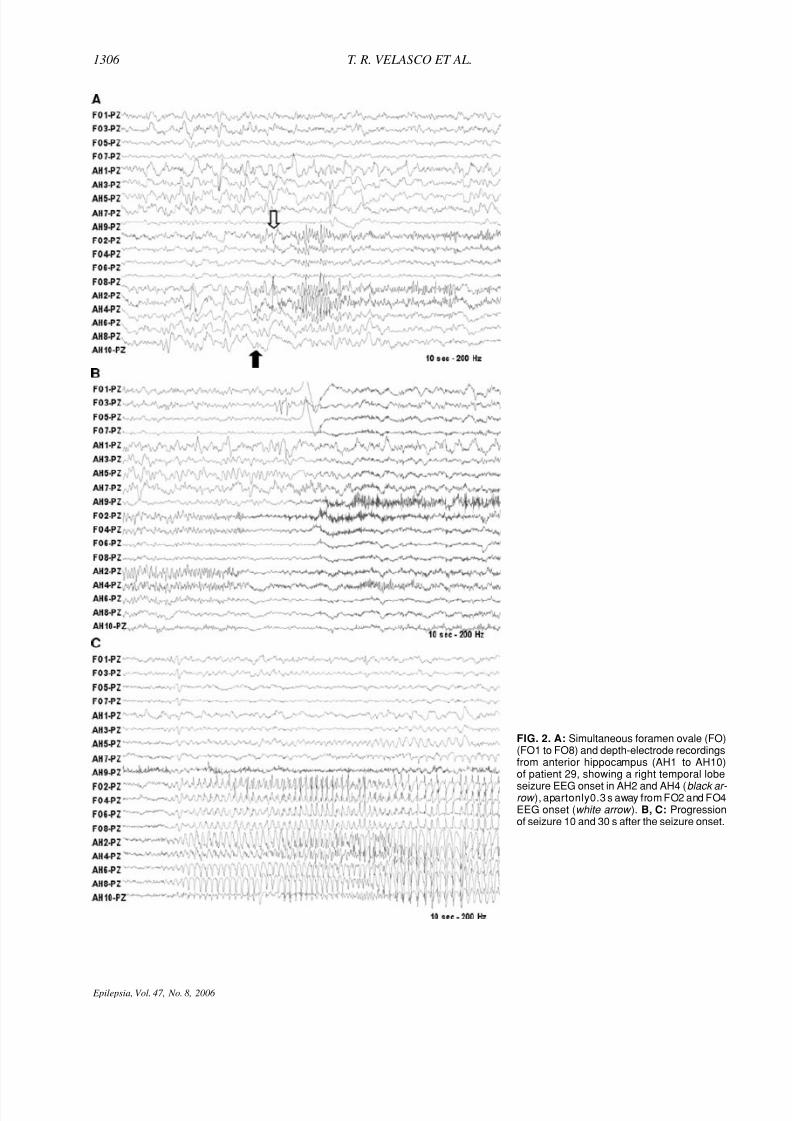
(Fig. 1B and C). The EEG recordings in this patient re-
vealed that the time of EEG onsets in FO electrodes were
within 0.3 to 1.7 s apart from the EEG onsets in depth
hippocampal electrodes (Fig. 2A).
Complications
The complications related to FO implantation were
transitory, as follows: (a) temporary facial pain (12 pa-
tients); (b) hypoesthesia in trigeminal territory (three
patients); (c) temporomandibular joint dysfunction (two
patients); (d) recurrence of labial herpes (two patients); (e)
retromandibular hematoma (one patient); and (f) transient
complete atrioventricular block induced by FO insertion,
despite premedication with atropine (one patient). In three
patients, the insertion of FO was difficult, and the record-
ings revealed asymmetry of the background EEG.
Postsurgical dataIn 31 (47.7%) patients,the results of FO revealed unilat-
eral EEG onsets, and temporal lobectomy was performed.
Two additional patients with>90% of seizures originating
from the side of unilateral HS underwent temporal lobec-
tomy. Twenty-three(70%) of 33 patients had good postsur-
gical outcome after temporal lobectomy (Engel classes I
andII). Theproportion of patients with Engel I seizure out-
come was 80% in patients with unilateral HS in compar-
ison with 53.8% in patients with bilateral HS (p = 0.05).
In all patients who underwent temporal lobectomy, patho-
logic examination of the resected temporal tissue revealed
Epilepsia, Vol. 47, No. 8, 2006
8/11/2019 Forame Oval para Epilepsia temporal mesial.pdf
http://slidepdf.com/reader/full/forame-oval-para-epilepsia-temporal-mesialpdf 4/8

8/11/2019 Forame Oval para Epilepsia temporal mesial.pdf
http://slidepdf.com/reader/full/forame-oval-para-epilepsia-temporal-mesialpdf 5/8
8/11/2019 Forame Oval para Epilepsia temporal mesial.pdf
http://slidepdf.com/reader/full/forame-oval-para-epilepsia-temporal-mesialpdf 6/8
FORAMEN OVALE ELECTRODES IN TEMPORAL LOBE EPILEPSY 1305
severe neuronal loss and gliosis in the CA1 and CA4 re-
gions, prosubiculum, and hilus, and discrete or moderate
neuronal loss of CA2 region and fascia dentata granule
cells.
Six patients refused the procedure, and three other pa-
tients with bilateral HS had the surgery contraindicated
because of risk of considerable memory deficits revealed
by intracarotid amobarbital memory testing.
DISCUSSION
Available data from autopsy and surgical studies sug-
gest that patients with temporal lobe epilepsy frequently
have bilateral hippocampal damage (12,13). However, HS
FIG. 1. A: Radiography from skull of patient 29 showing symmet-rical bilateral positioning of foramen ovale (FO) electrodes. Coro-nal (B) T1 and sagittal (C) magnetic resonance imaging imagesshowing the position of depth (arrowheads ) and FO electrodes(arrows ).
is usually asymmetrical and, when preoperative evaluation
data are concordant with the side of hippocampal atro-
phy, temporal lobectomy can be indicated, and postsurgeryoutcome is usually good (1). Clinical decision making is
more complicated when neurophysiologic and neuroimag-
ing data indicate bilateral involvement of mesial structures
(1,3). Although data from the present series indicate fre-
quent bilateral involvement of mesial structures, we found
evidence that FO evaluation provide accurate neurophys-
iologic data about lateralization of seizures that were not
clearly lateralized by surface EEGs.
In other words, despite the hypothetically poor post-
surgery outcome suggested by bilateral surface EEG
onsets and the high rate of patients with bilateral HS, FO
Epilepsia, Vol. 47, No. 8, 2006
8/11/2019 Forame Oval para Epilepsia temporal mesial.pdf
http://slidepdf.com/reader/full/forame-oval-para-epilepsia-temporal-mesialpdf 7/8
1306 T. R. VELASCO ET AL.
FIG. 2. A: Simultaneous foramen ovale (FO)(FO1 to FO8) and depth-electrode recordingsfrom anterior hippocampus (AH1 to AH10)of patient 29, showing a right temporal lobe
seizure EEG onset in AH2 and AH4 (black ar- row ), apartonly0.3 s away from FO2 and FO4EEG onset (white arrow ). B, C: Progressionof seizure 10 and 30 s after the seizure onset.
Epilepsia, Vol. 47, No. 8, 2006

8/11/2019 Forame Oval para Epilepsia temporal mesial.pdf
http://slidepdf.com/reader/full/forame-oval-para-epilepsia-temporal-mesialpdf 8/8
FORAMEN OVALE ELECTRODES IN TEMPORAL LOBE EPILEPSY 1307
evaluation substantially affected the presurgical evalua-
tion, indicating the side of temporal lobectomy in two
thirdsof these MTLE patients.It is importantto emphasize
that this proportion was similar in patients with bilateral
and unilateral HS revealed by MRI.
The signal-to-noise ratio of FO is better than that in the
scalp-sphenoidal electrode recordings (7–10). Thereforemany electrophysiologic events with lateralizing value are
detected by FO but remainundetected by scalp-sphenoidal
contacts (14,15). In our series, this permitted the indica-
tion of temporal lobectomy in 60% of cases that were
not lateralized by scalp-sphenoidal electrodes, with the
great advantages of being nontraumatic to the brain and
of carrying much less risk for the patient than the more-
invasive depth electrodes. Moreover, even in a sample of
patients with bilateral HS on MRI and apparent bilateral
surface ictal EEG onsets, 70% of the patients had good
postsurgical outcome after temporal lobectomy, provided
that unilateral EEG onsets were defined by FO. This pro-
portion is very similar to previous descriptions of patients
with MTLE (1,10,11).
It should be stressed, however, that the FO recording
technique addresses only specific questions:if the seizures
originate in the mesiobasal temporal lobe structures and
if they are consistently lateralized. In other words, a
clear hypothesis should exist regarding the location of the
epileptogenic zone, derived from noninvasive studies. In
previous descriptions of FO, it has been stated that, in
comparison to the presurgical examination using intrac-
erebral depth recordings, the information gained by FO
electrode recording is limited, and that the FO technique
cannot substitute for a proper depth-electrode evaluation(9). However, this conclusion was drawn before the recent
advances of neuroimaging. The advent of high-resolution
MRIhas allowed theproper selectionof patients that might
benefit from FO recordings, namely MTLE patients, ex-
cluding those patients with epileptogenic lesions outside
the mesiobasal structures.
In all the five patients in whom the result of FO elec-
trodesshowed bilateral independent or nonlateralized ictal
onsets, further recordings with depth electrodesconfirmed
the findings. This can be explained by the evidence of
the intimate relation of the properly placed FO electrode
with the parahippocampal gyrus, uncus, and lingual gyrus(Fig. 1C), and by the good correlation between the ictal
onsets in FO and depth electrodes (Fig. 2A).
In conclusion, our results indicate that, in properly se-
lected patients, FO is a reliable method for lateraliza-
tion of seizures that are not clearly recorded by surface
EEGs, usually providing sufficient information to indicate
epilepsy surgery. In addition, FO implantation is relatively
simple, well tolerated, and can substantially facilitate the
presurgical evaluation of patients who are candidates for
temporal lobectomy surgery by decreasing the risks of in-
vasive neurophysiologic evaluation without excessive loss
of information.Acknowledgment: This work was supported by FAPESP/
CINAPCE Project 0556447-7. Roger Walz was supportedby CNPq (472840/2004-5 and 301379/2005-0). Marino M.Bianchin was supported by FAPESD Project (02103743-0).
REFERENCES
1. Engel J Jr, Wiebe S, French J, et al. Practice parameter: tempo-ral lobe and localized neocortical resections for epilepsy. Epilepsia2003;44:741–751.
2. Kilpatrick C, Cook M, Kaye A, et al. Non-invasive investigations
successfully select patients for temporal lobe surgery. J Neurol Neu-rosurg Psychiatry 1997;63:327–333.
3. Rosenow F, Luders H. Presurgical evaluation of epilepsy. Brain2001;124:1683–1700.4. Pataraia E, Lurger S, Serles W, et al. Ictal scalp EEG in unilateral
mesial temporal lobe epilepsy. Epilepsia 1998;39:608–614.5. Serles W, Li LM, Antel SB, et al. Time course of postoperative
recovery of N -acetyl-aspartate in temporal lobe epilepsy. Epilepsia2001;42:190–197.
6. Alarcon G, Kissani N, Dad M, et al. Lateralizing and localizing val-ues of ictal onset recorded on the scalp: evidence from simultane-ous recordings with intracranialforamen ovale electrodes. Epilepsia2001;42:1426–1437.
7. Diehl B, Luders HO. Temporal lobe epilepsy: when are invasiverecordings needed? Epilepsia 2000;41(suppl 3):S61-S74.
8. Siegfried J, Wieser HG, Stodieck SR. Foramen ovale elec-trodes: a new technique enabling presurgical evaluation of pa-tients with mesiobasal temporal lobe seizures. Appl Neurophysiol1985;48:408–417.
9. Wieser HG, Elger CE, Stodieck SR. The “foramen ovale elec-trode”: a new recording method for the preoperative evaluation of patients suffering from mesio-basal temporal lobe epilepsy. Elec-troencephalogr Clin Neurophysiol 1985;61:314–322.
10. Wieser HG, Siegel AM. Analysis of foramen ovale electrode-recorded seizures and correlation with outcome following amyg-dalohippocampectomy. Epilepsia 1991;32:838–850.
11. Engel J Jr.Outcome with respect to epilepticseizures.In: Engel J Jr,ed. Surgical treatment of epilepsies. New York: Raven, 1987;553–571.
12. Falconer MA, Serafetinides EA, Corsellis JA. Etiology And patho-genesis of temporal lobe epilepsy. Arch Neurol 1964;10:233–248.
13. Margerison JH, Corsellis JA. Epilepsy and the temporal lobes: aclinical,electroencephalographicand neuropathologicalstudy of thebrain in epilepsy, with particular reference to the temporal lobes.
Brain 1966;89:499–530.14. Fernandez Torre JL, Alarcon G, Binnie CD, et al. Comparison of
sphenoidal, foramen ovale and anterior temporal placements for de-tecting interictal epileptiform discharges in presurgical assessmentfor temporal lobe epilepsy. Clin Neurophysiol 1999;110:895–904.
15. Kissani N, Alarcon G, Dad M, et al. Sensitivity of recordings atsphenoidal electrode site for detecting seizure onset: evidence fromscalp, superficial and deep foramen ovale recordings. Clin Neuro-
physiol 2001;112:232–240.
Epilepsia, Vol. 47, No. 8, 2006