dr. berlian i. idris, spjp(k), fiha, mph, dscidicabangtangerang.org/upload/20190209112507-stemi pit...
TRANSCRIPT
dr. Berlian I. Idris, SpJP(K), FIHA, MPH, DSc
• Dokter Umum: FKUI 1995-2002
• Master of Public Health (MPH) - Doctor of Science
(DSc): Belanda 2003-2006
• Spesialis Jantung dan Pembuluh Darah (SpJP):
FKUI - Pusat Jantung Nasional Harapan Kita 2007-
2011
• Pendidikan Konsultan (K) Intervensi Kardiologi:
Vietnam & Thailand 2012 – 2013
• Dokter di RSUD Kota Tangerang
Berlian I. Idris
RSUD Kota Tangerang
Fibrinolytic for STEMI patients:
How we could save lives
Disclaimer
• This is a sponsored lecture by Dexa
Medica (Fibrion, streptokinase)
Acute coronary syndrome
A spectrum of clinical syndromes due to
sudden, significantly compromised coronary
circulation ranging from unstable angina to
NSTEMI and STEMI.
Further stages of stable angina pectoris
Topol EJ, ed. Textbook of cardiovascular medicine 2007.
DEFINITION
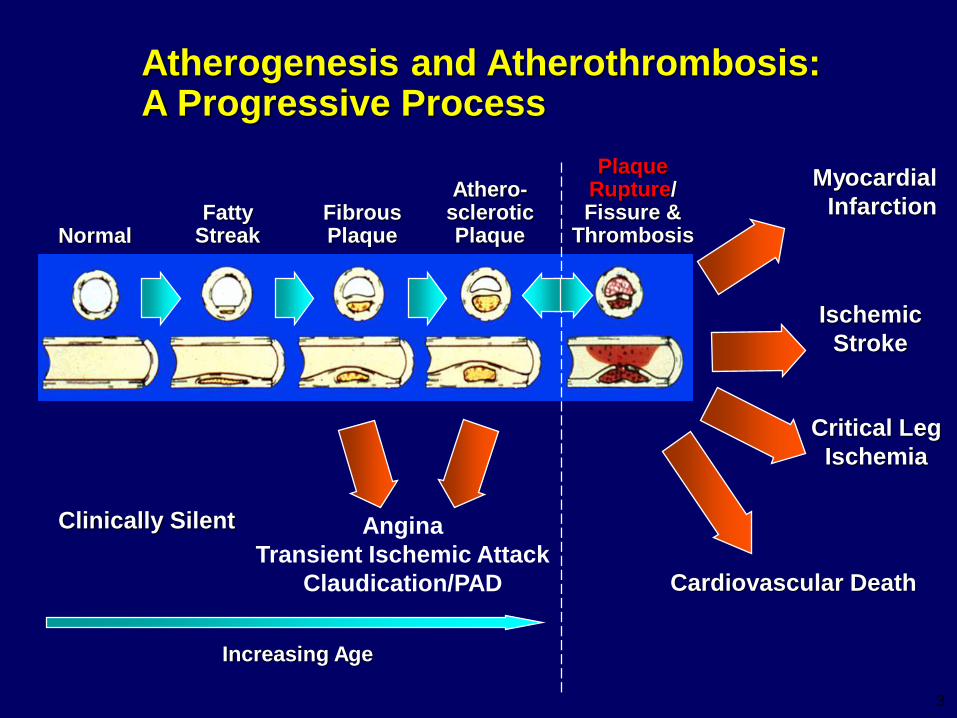
Atherogenesis and Atherothrombosis: A Progressive Process
NormalFatty
StreakFibrousPlaque
Athero-scleroticPlaque
PlaqueRupture/Fissure &
Thrombosis
Myocardial
Infarction
Ischemic
Stroke
Critical Leg
Ischemia
Clinically Silent
Cardiovascular Death
Increasing Age
Angina
Transient Ischemic Attack
Claudication/PAD
3
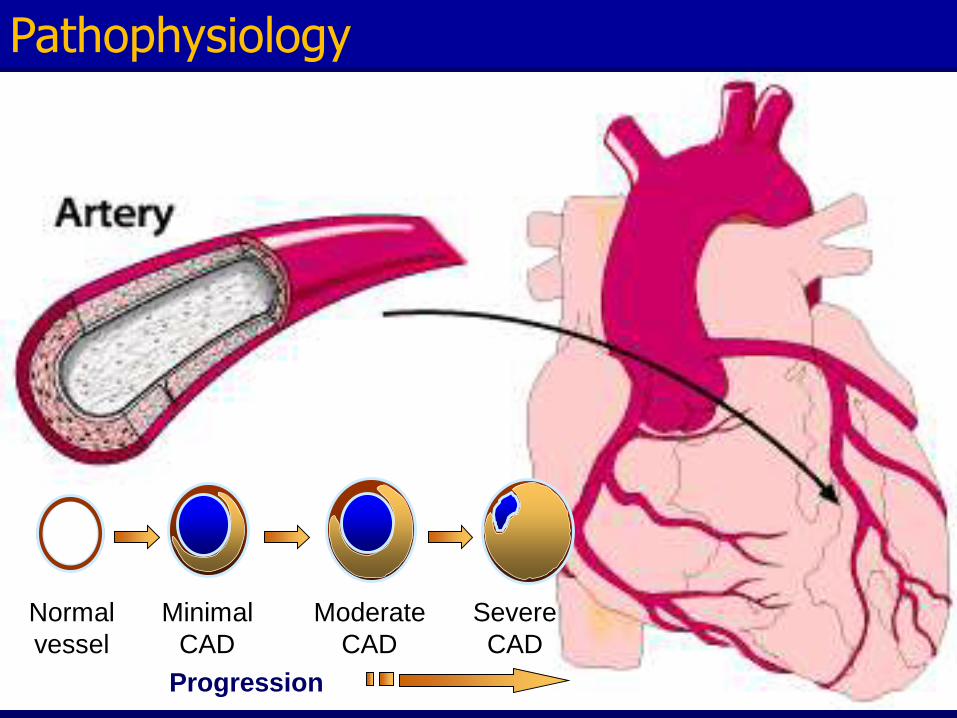
Normal
vessel
Minimal
CAD
Severe
CAD
Moderate
CAD
Progression
Pathophysiology
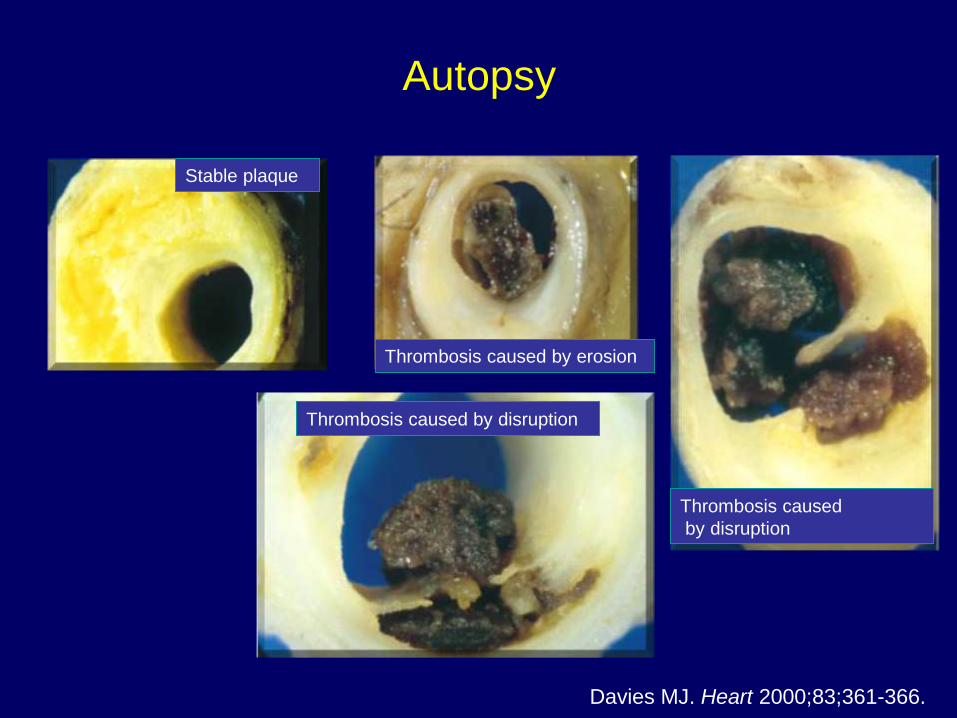
Autopsy
Stable plaque
Davies MJ. Heart 2000;83;361-366.
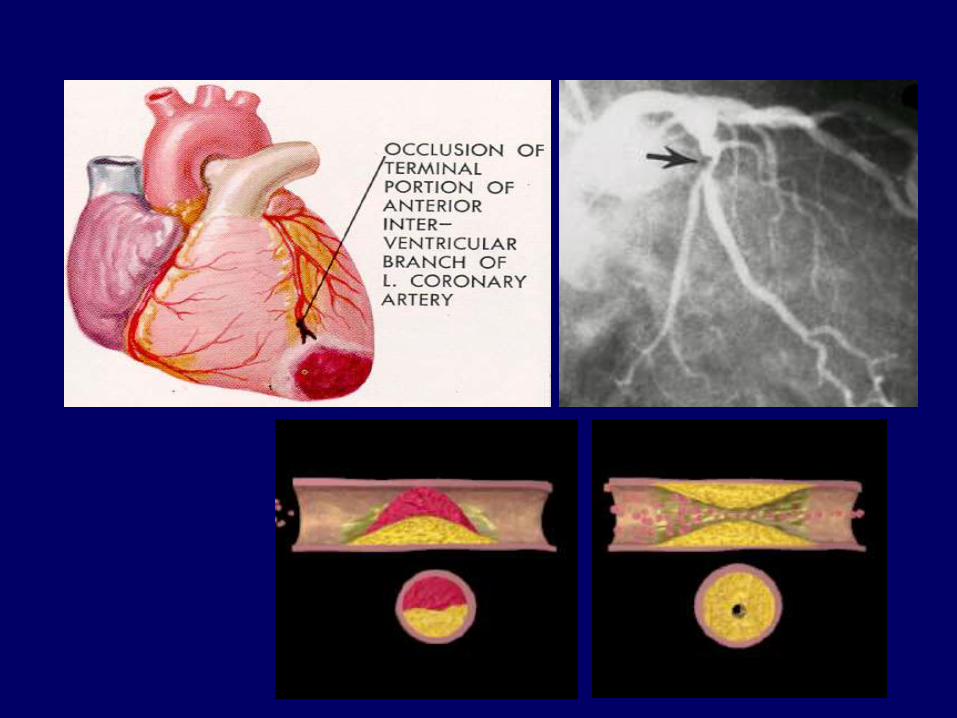
Thrombosis caused by erosion
Thrombosis caused by disruption
Thrombosis caused
by disruption
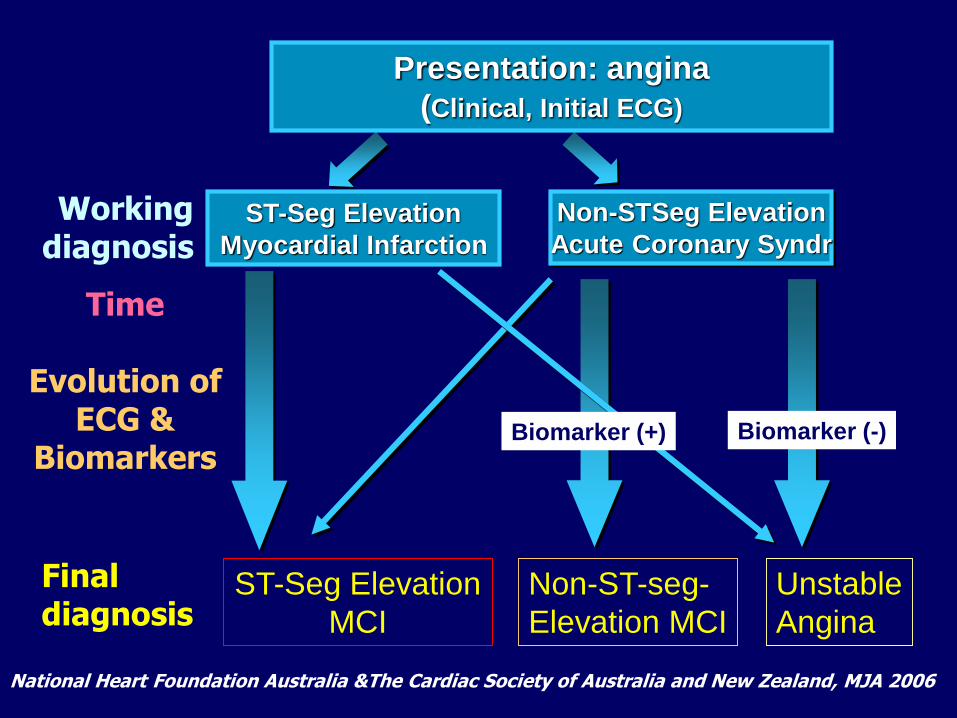
Presentation: angina
(Clinical, Initial ECG)
ST-Seg Elevation
Myocardial Infarction
Non-STSeg Elevation
Acute Coronary Syndr
ST-Seg Elevation
MCI
Non-ST-seg-
Elevation MCI
Unstable
Angina
Workingdiagnosis
Time
Evolution ofECG &
Biomarkers
Finaldiagnosis
National Heart Foundation Australia &The Cardiac Society of Australia and New Zealand, MJA 2006
Biomarker (-)Biomarker (+)
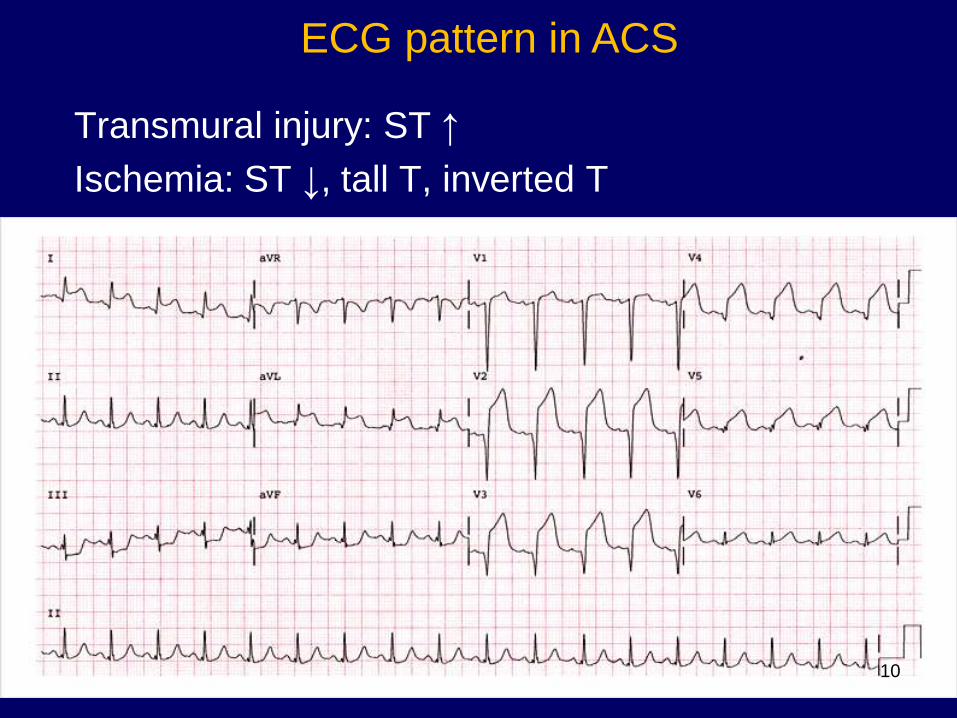
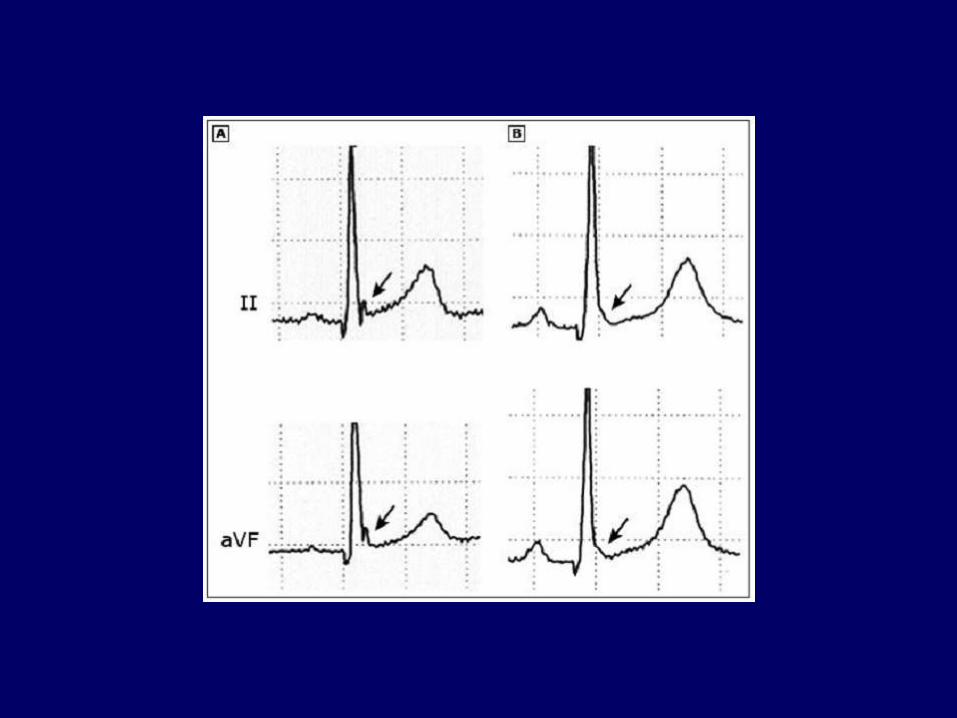
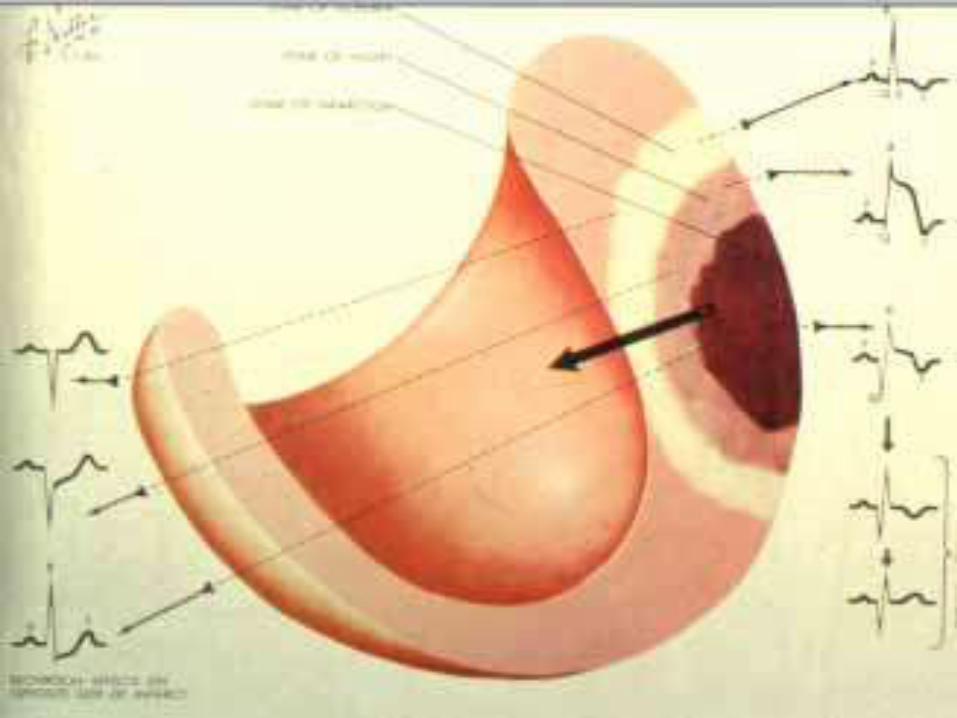
Transmural injury: ST ↑
Ischemia: ST ↓, tall T, inverted T
ECG pattern in ACS
10
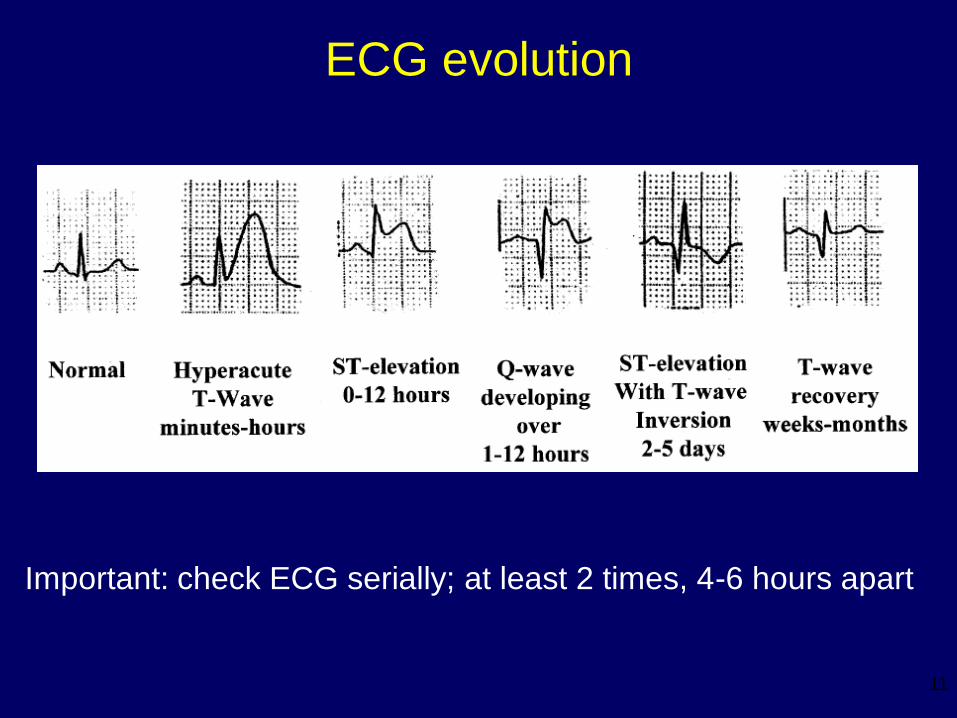
ECG evolution
Important: check ECG serially; at least 2 times, 4-6 hours apart
11
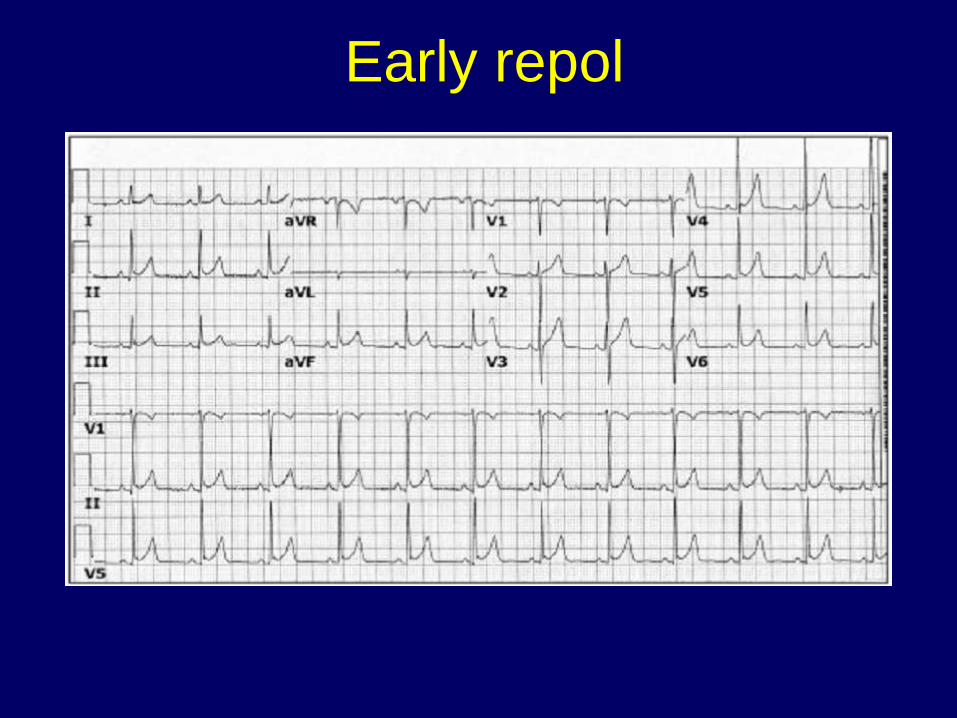
Early repol
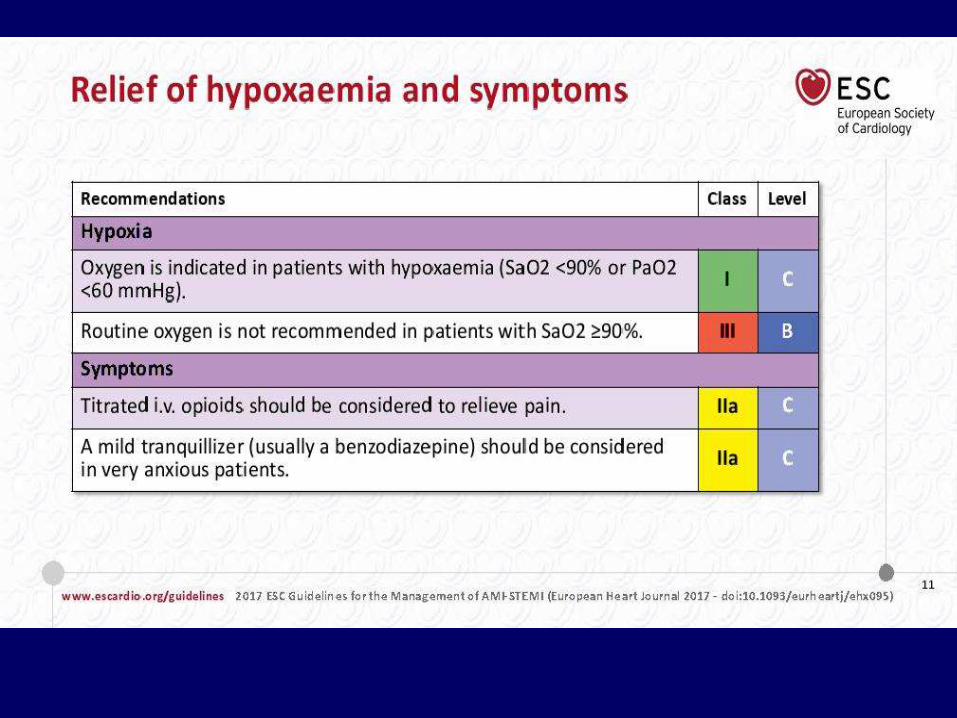
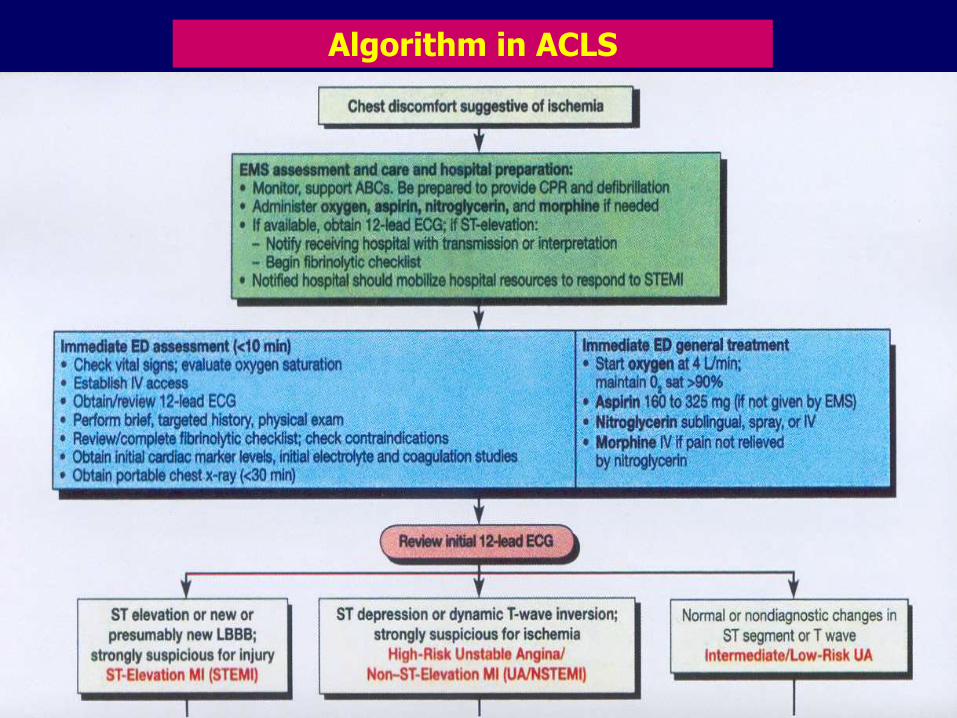
• Monitor and support ABCs
• Check vital signs, incl oxygen saturation
• Establish IV access
• Administer– Oxygen 2-4L/min
– Aspirin 160-325 mg chewed
– Clopidogrel loading dose 300 mg, or ticagleror 180 mg
– Statin loading dose
– Nitrate (ISDN) sublingual
– Morphine if pain not relieved with NTG
Initial management

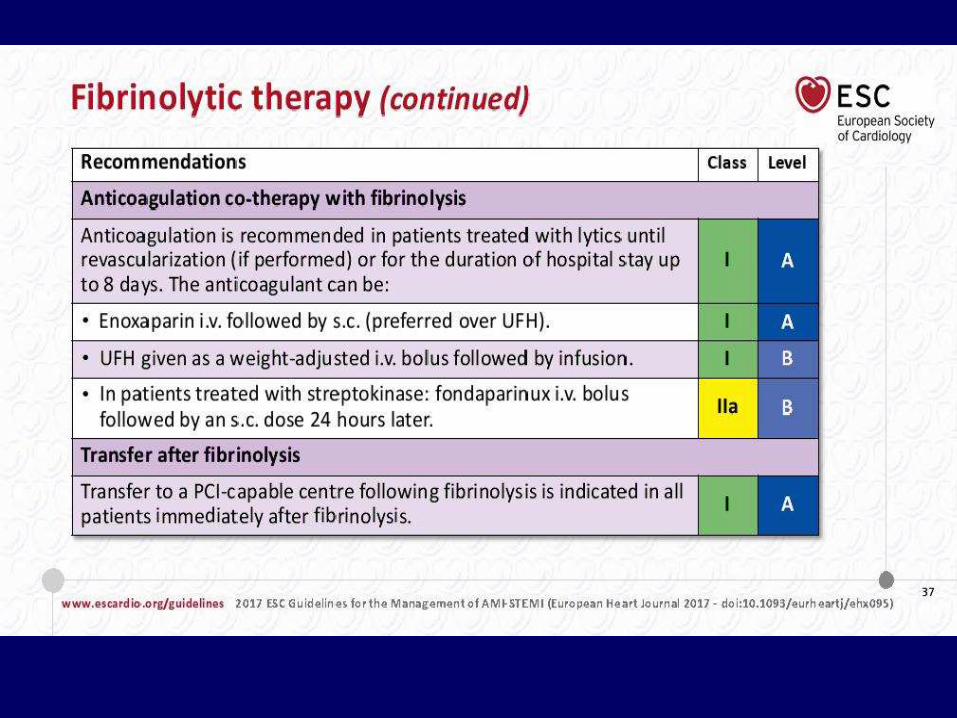
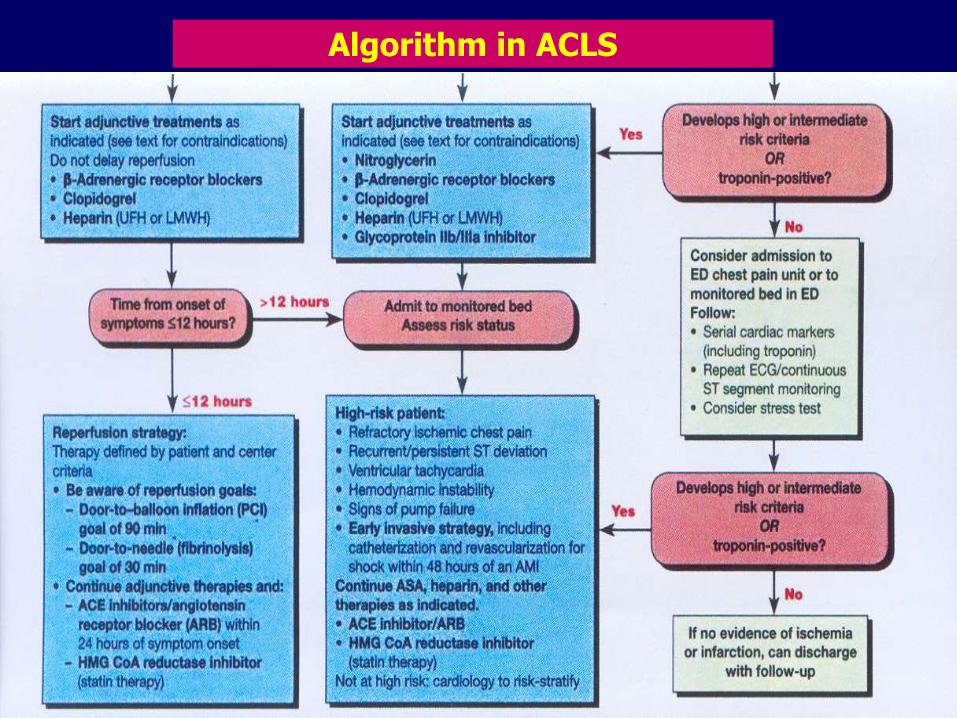
Anticoagulation & reperfusion
• Heparin administration (LMWH enoxaparine, fondaparinux or UFH)
• Reperfusion in STEMI
– Fibrinolysis or primary percutaneous coronary intervention (PCI)
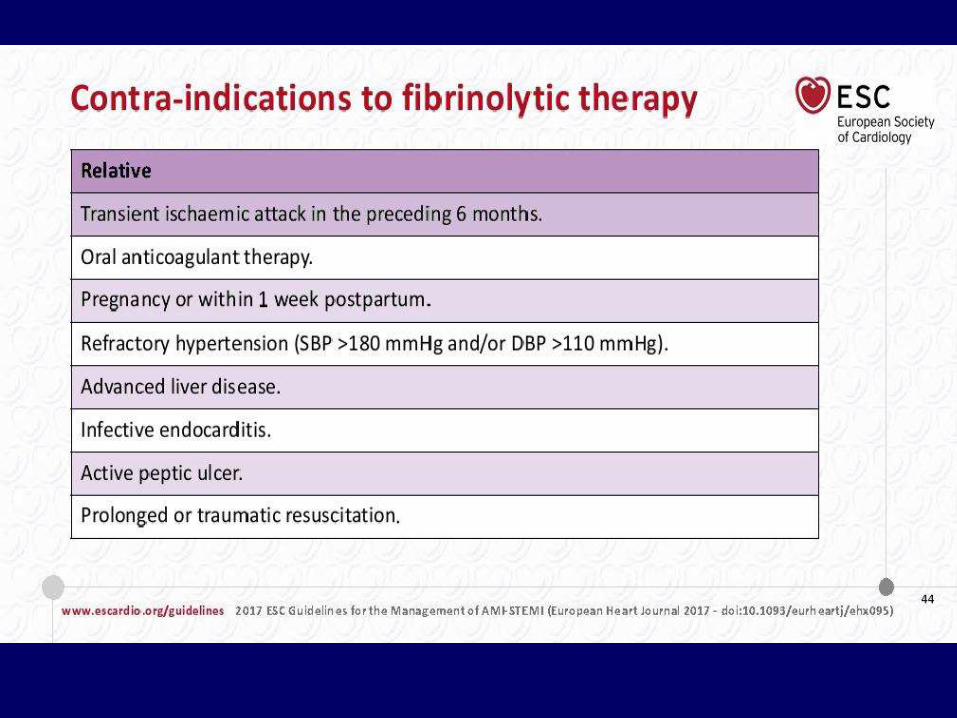
– Assess onset & contraindication
Indication • Typical symptom: angina
• ST elevation in 2 or more related leads/ new or presumably newLBBB baru
• Chest pain onset < 12 hours, most effective <2h after onset.1
Preparation• Contraindication check list
• Informed consent
• Resuscitation personnel and equipments
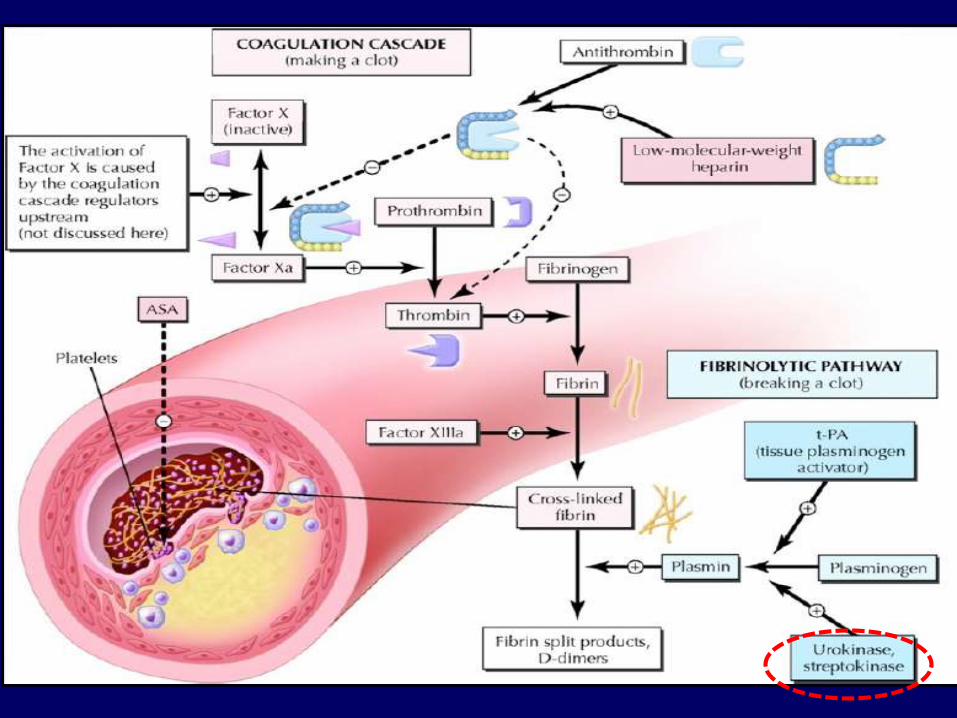
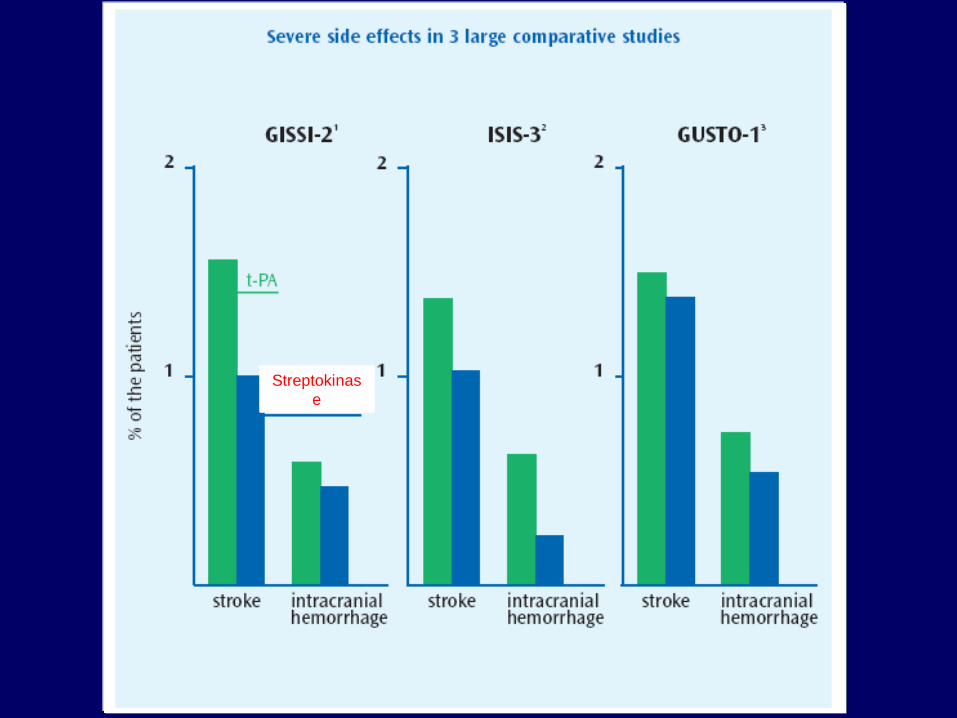
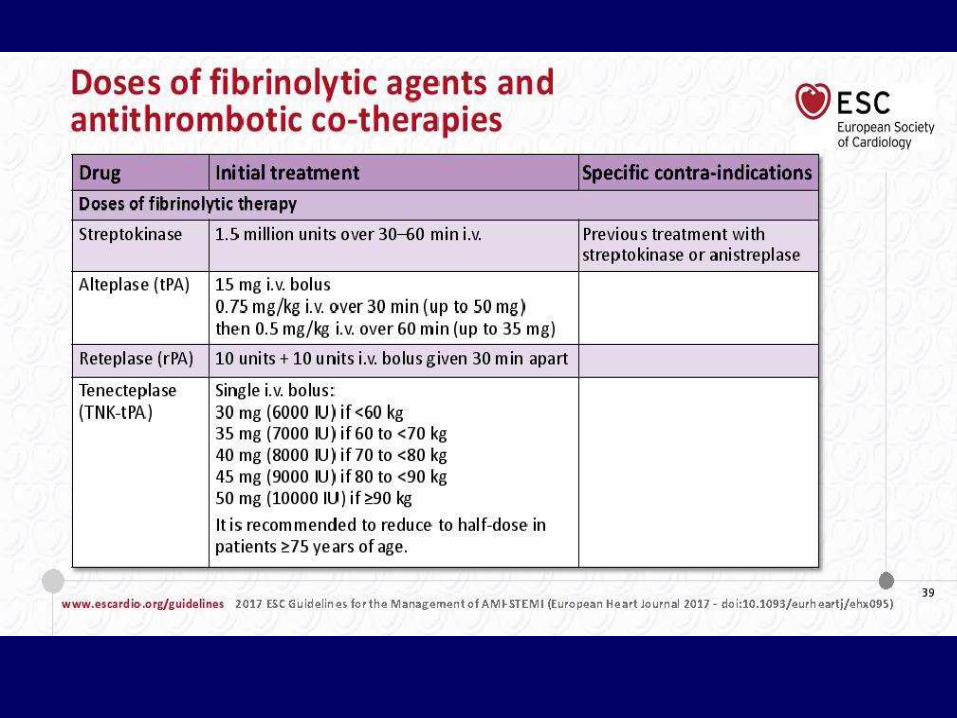
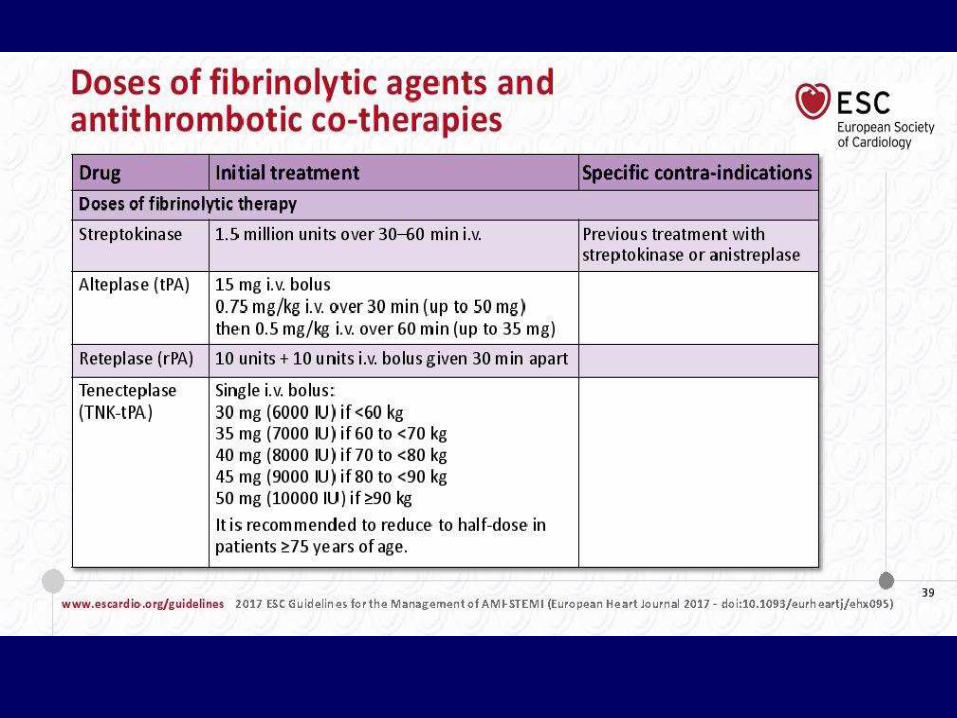
Fibrinolytic drugs• Streptokinase
• Tissue Plasminogen Activator
• Tenecteplase (TNK-tPA)
Fibrinolytic therapy
1Boersma E, et al. Lancet 1996;348(9030):771–775
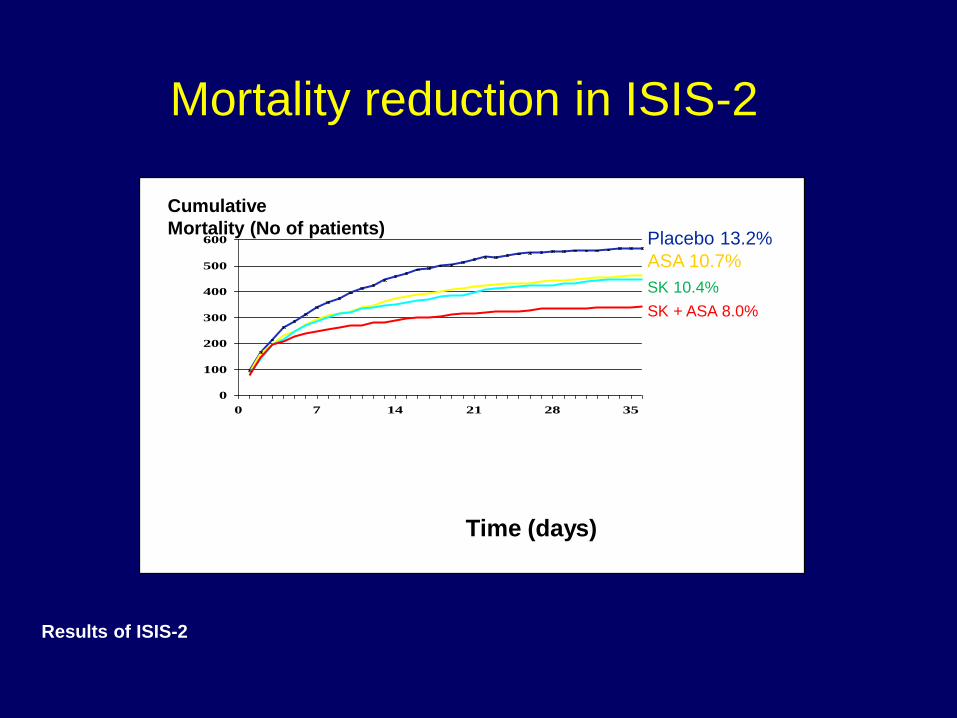
Mortality reduction in ISIS-2
0
100
200
300
400
500
600
0 7 14 21 28 35
Placebo 13.2%
ASA 10.7%
SK 10.4%
SK + ASA 8.0%
Time (days)
Cumulative
Mortality (No of patients)
Results of ISIS-2

Streptokinas
e
Event
SK
n=13,607
tPA
13,569
APSAC
13,599
Thrombo-
lysis +
heparin
20,400
Thrombo-
lysis alone
20,375
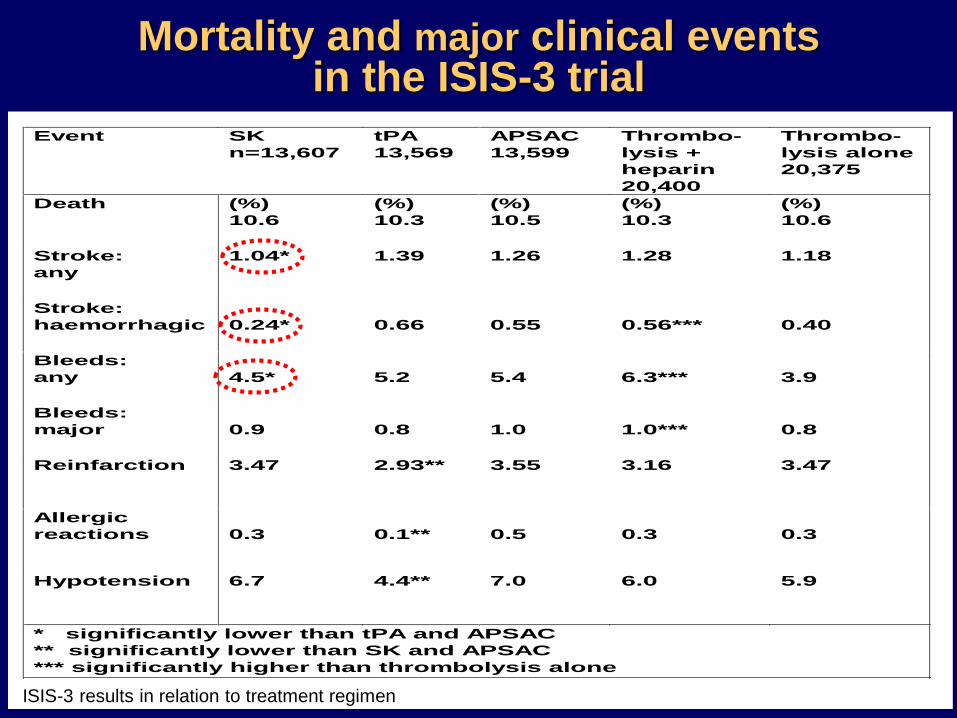
Death (%)
10.6
(%)
10.3
(%)
10.5
(%)
10.3
(%)
10.6
Stroke:
any
1.04* 1.39 1.26 1.28 1.18
Stroke:
haemorrhagic
0.24*
0.66
0.55
0.56***
0.40
Bleeds:
any
4.5*
5.2
5.4
6.3***
3.9
Bleeds:
major
0.9
0.8
1.0
1.0***
0.8
Reinfarction 3.47 2.93** 3.55 3.16 3.47
Allergic
reactions
0.3
0.1**
0.5
0.3
0.3
Hypotension 6.7 4.4** 7.0 6.0 5.9
* significantly lower than tPA and APSAC
** significantly lower than SK and APSAC
*** significantly higher than thrombolysis alone
ISIS-3 results in relation to treatment regimen
Mortality and major clinical eventsin the ISIS-3 trial
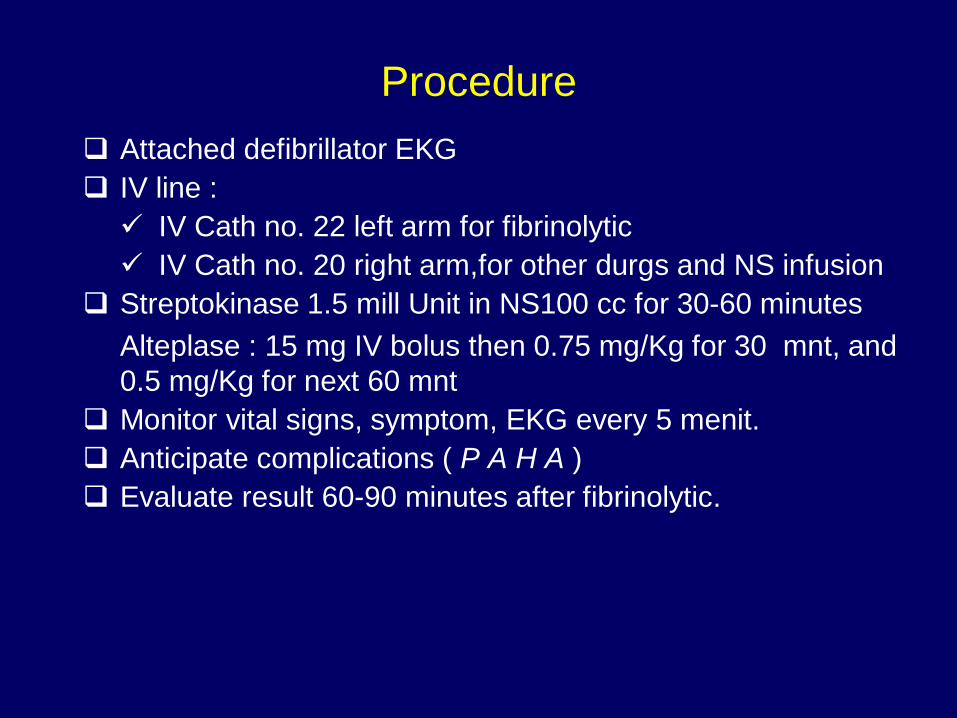
Procedure
Attached defibrillator EKG
IV line :
IV Cath no. 22 left arm for fibrinolytic
IV Cath no. 20 right arm,for other durgs and NS infusion
Streptokinase 1.5 mill Unit in NS100 cc for 30-60 minutes
Alteplase : 15 mg IV bolus then 0.75 mg/Kg for 30 mnt, and
0.5 mg/Kg for next 60 mnt
Monitor vital signs, symptom, EKG every 5 menit.
Anticipate complications ( P A H A )
Evaluate result 60-90 minutes after fibrinolytic.
• Significant symptomatic relieve
• ECG: decrease in ST elevation >50%
Success criteria
Perdarahan (bleeding)
Minor : observe, slow infusion rate.
Major : stop, transfusion if necessary
Alergy
Stop fibrinolytic, antihistamin / cortikosteroid iv
Hipotension
Withhold fibrinolytic
Tredelenburg position
Loading 100-250 cc Nacl 0,9%
Start again, slow the rate
Arrhythmia
Benign: observe
Malignant: treat accordingly
Complications
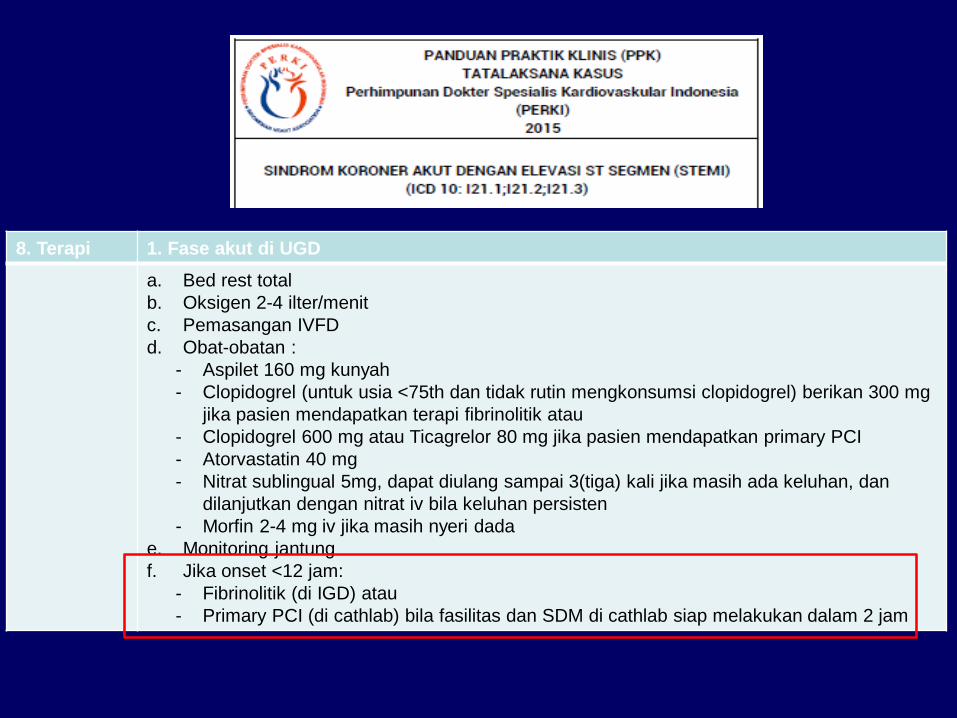
8. Terapi 1. Fase akut di UGD
a. Bed rest total
b. Oksigen 2-4 ilter/menit
c. Pemasangan IVFD
d. Obat-obatan :
- Aspilet 160 mg kunyah
- Clopidogrel (untuk usia <75th dan tidak rutin mengkonsumsi clopidogrel) berikan 300 mg
jika pasien mendapatkan terapi fibrinolitik atau
- Clopidogrel 600 mg atau Ticagrelor 80 mg jika pasien mendapatkan primary PCI
- Atorvastatin 40 mg
- Nitrat sublingual 5mg, dapat diulang sampai 3(tiga) kali jika masih ada keluhan, dan
dilanjutkan dengan nitrat iv bila keluhan persisten
- Morfin 2-4 mg iv jika masih nyeri dada
e. Monitoring jantung
f. Jika onset <12 jam:
- Fibrinolitik (di IGD) atau
- Primary PCI (di cathlab) bila fasilitas dan SDM di cathlab siap melakukan dalam 2 jam
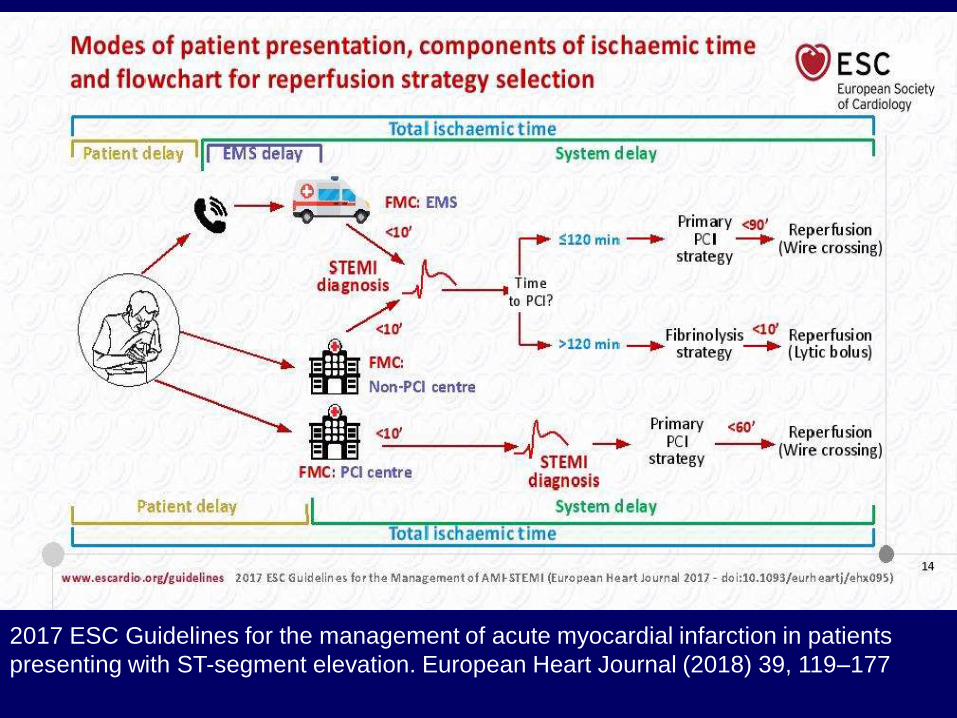
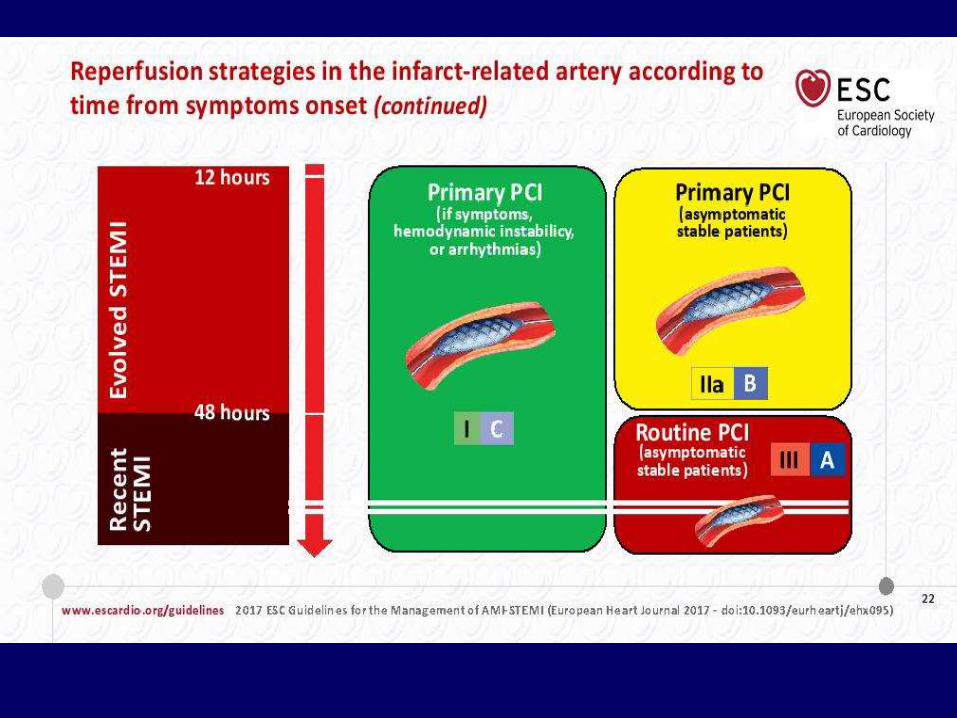
2017 ESC Guidelines for the management of acute myocardial infarction in patients
presenting with ST-segment elevation. European Heart Journal (2018) 39, 119–177
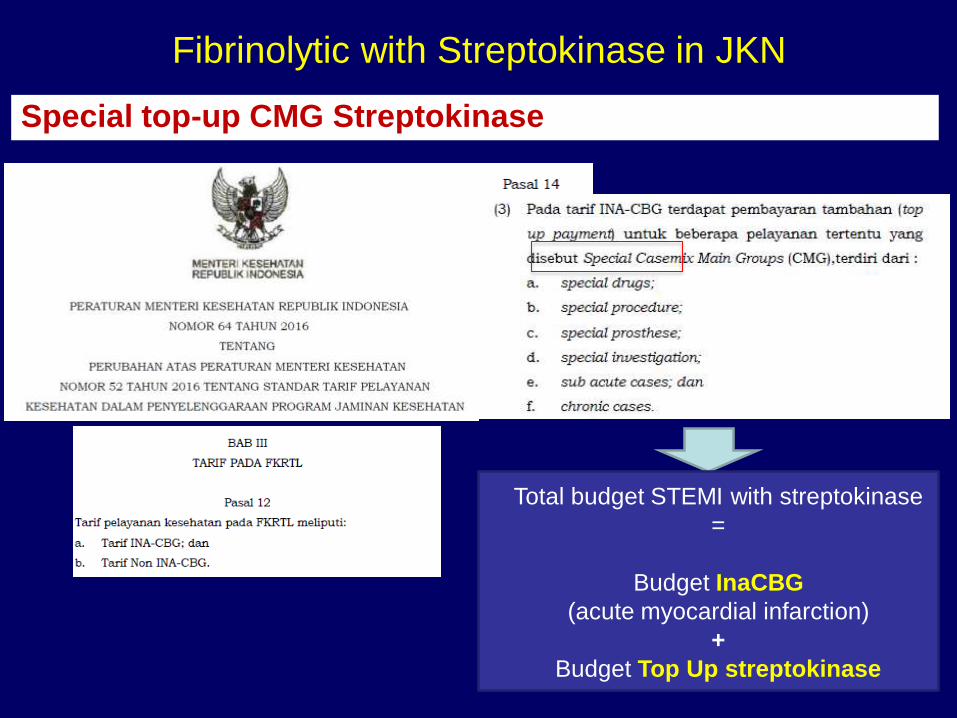
Fibrinolytic with Streptokinase in JKN
Special top-up CMG Streptokinase
Total budget STEMI with streptokinase
=
Budget InaCBG
(acute myocardial infarction)
+
Budget Top Up streptokinase
Thank you
Thank you

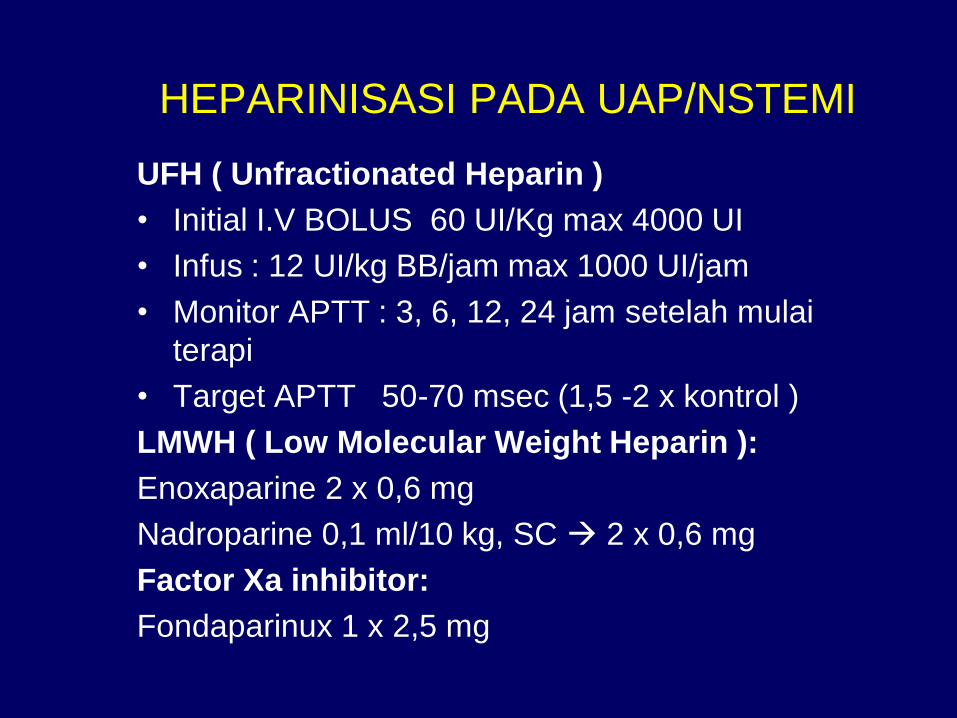
HEPARINISASI PADA UAP/NSTEMI
UFH ( Unfractionated Heparin )
• Initial I.V BOLUS 60 UI/Kg max 4000 UI
• Infus : 12 UI/kg BB/jam max 1000 UI/jam
• Monitor APTT : 3, 6, 12, 24 jam setelah mulai
terapi
• Target APTT 50-70 msec (1,5 -2 x kontrol )
LMWH ( Low Molecular Weight Heparin ):
Enoxaparine 2 x 0,6 mg
Nadroparine 0,1 ml/10 kg, SC 2 x 0,6 mg
Factor Xa inhibitor:
Fondaparinux 1 x 2,5 mg
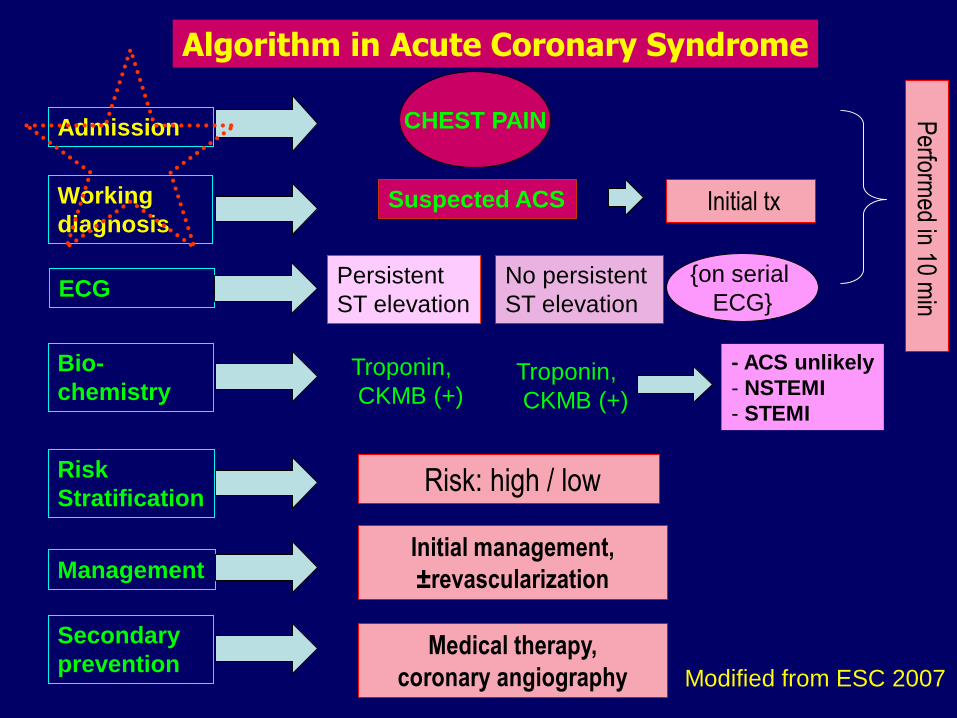
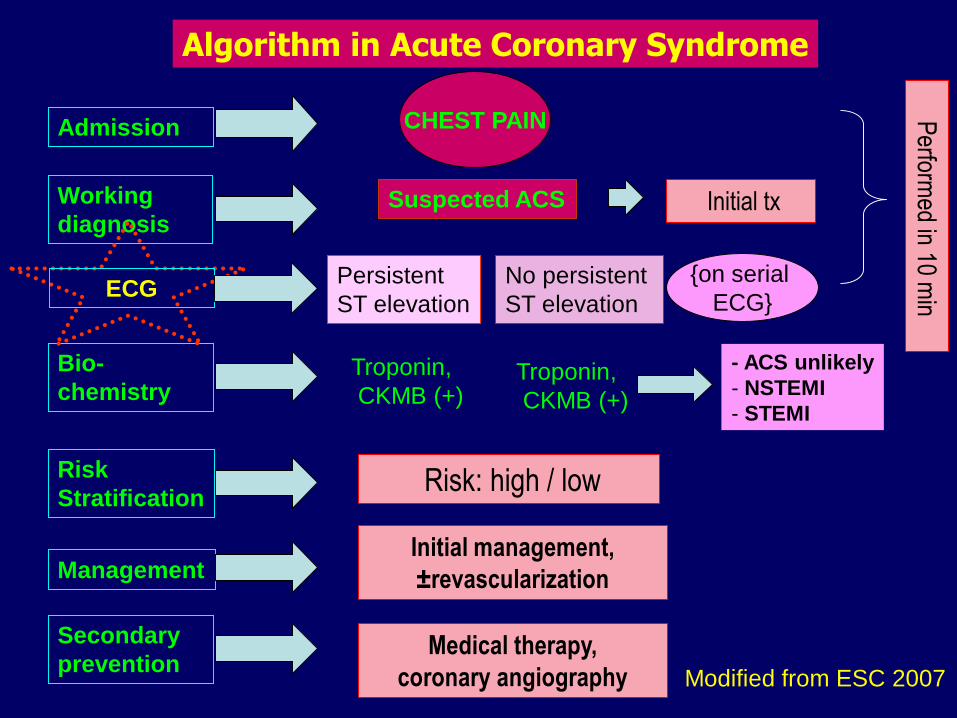
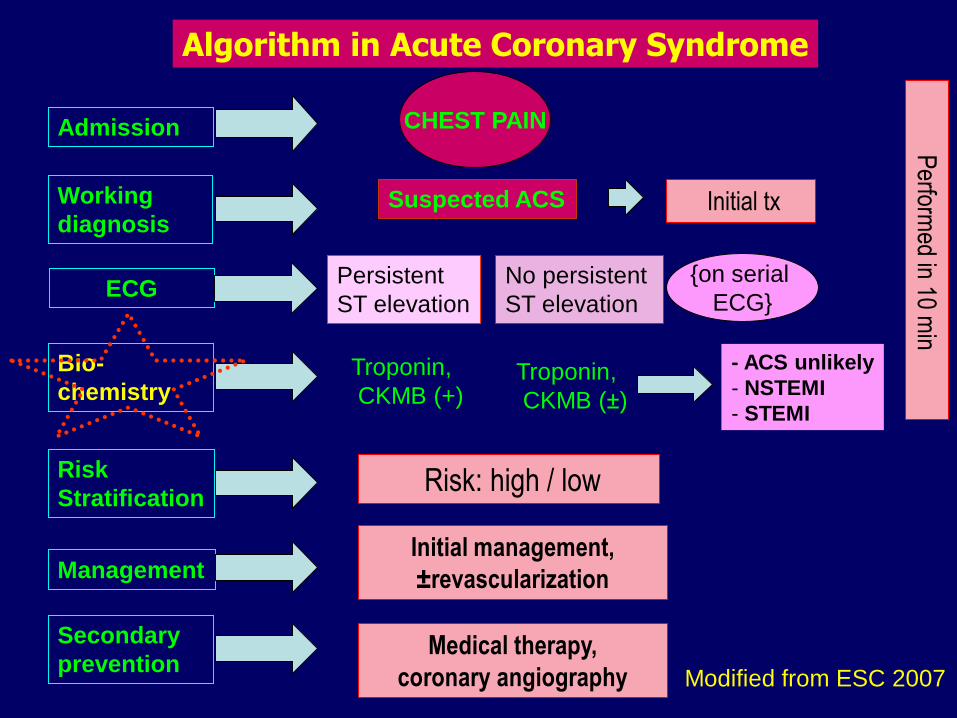
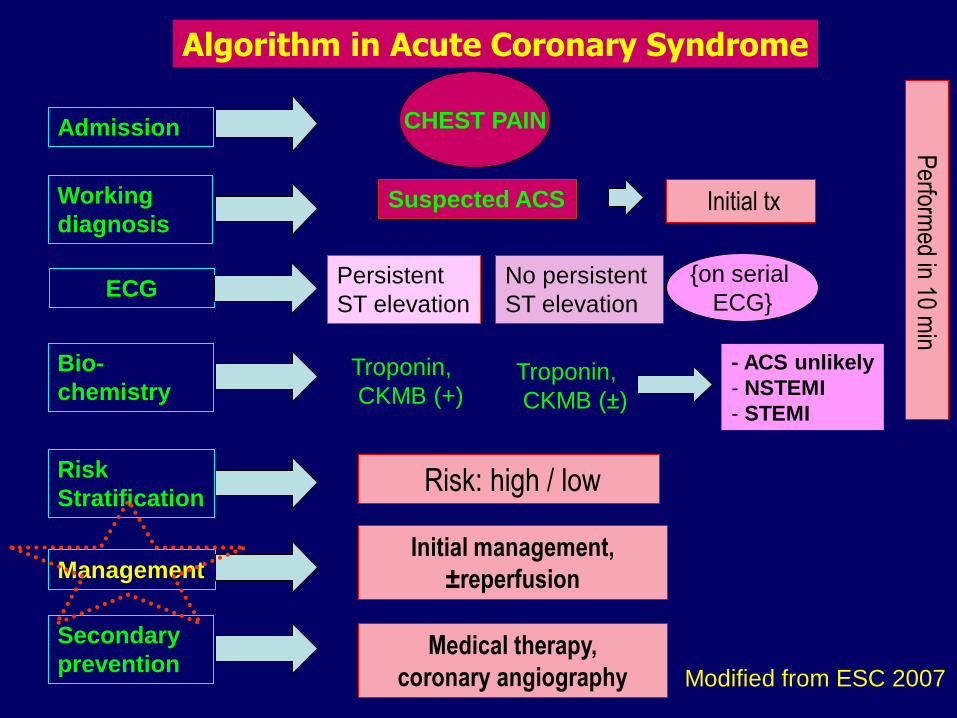
CHEST PAINAdmission
Working
diagnosis
Bio-
chemistry
Risk
Stratification
Management
Secondary
prevention
Suspected ACS
Persistent
ST elevation
No persistent
ST elevation
Troponin,
CKMB (+)
Risk: high / low
Algorithm in Acute Coronary Syndrome
Modified from ESC 2007
- ACS unlikely
- NSTEMI
- STEMI
ECG
Initial management,
±revascularization
Medical therapy,
coronary angiography
Perform
ed in 10 min
{on serial
ECG}
Troponin,
CKMB (+)
Initial tx
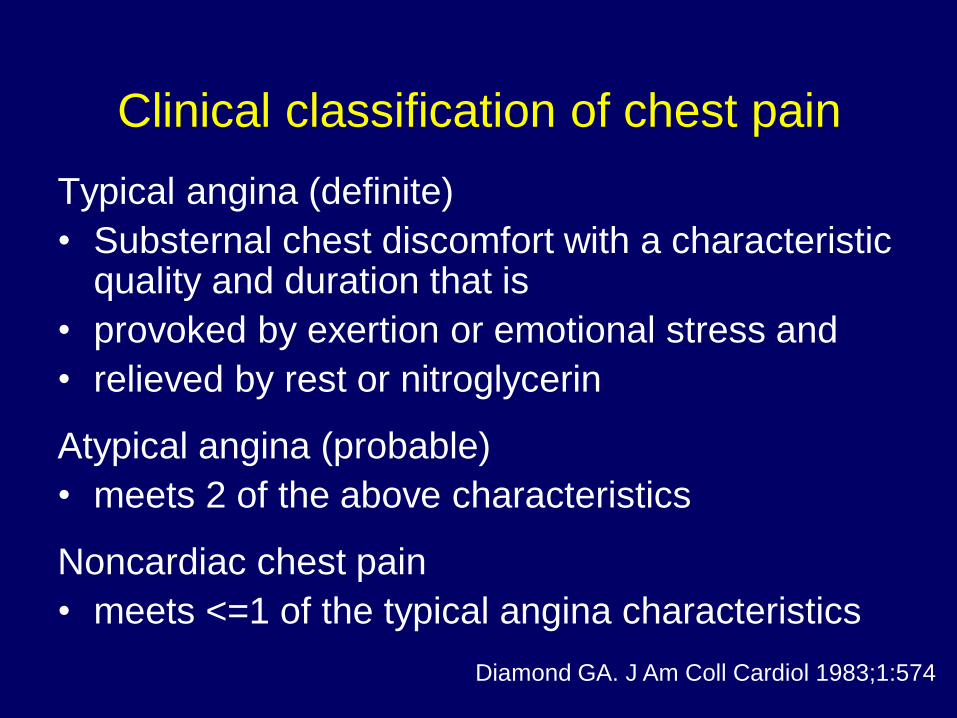
Clinical classification of chest pain
Typical angina (definite)
• Substernal chest discomfort with a characteristic quality and duration that is
• provoked by exertion or emotional stress and
• relieved by rest or nitroglycerin
Atypical angina (probable)
• meets 2 of the above characteristics
Noncardiac chest pain
• meets <=1 of the typical angina characteristics
Diamond GA. J Am Coll Cardiol 1983;1:574
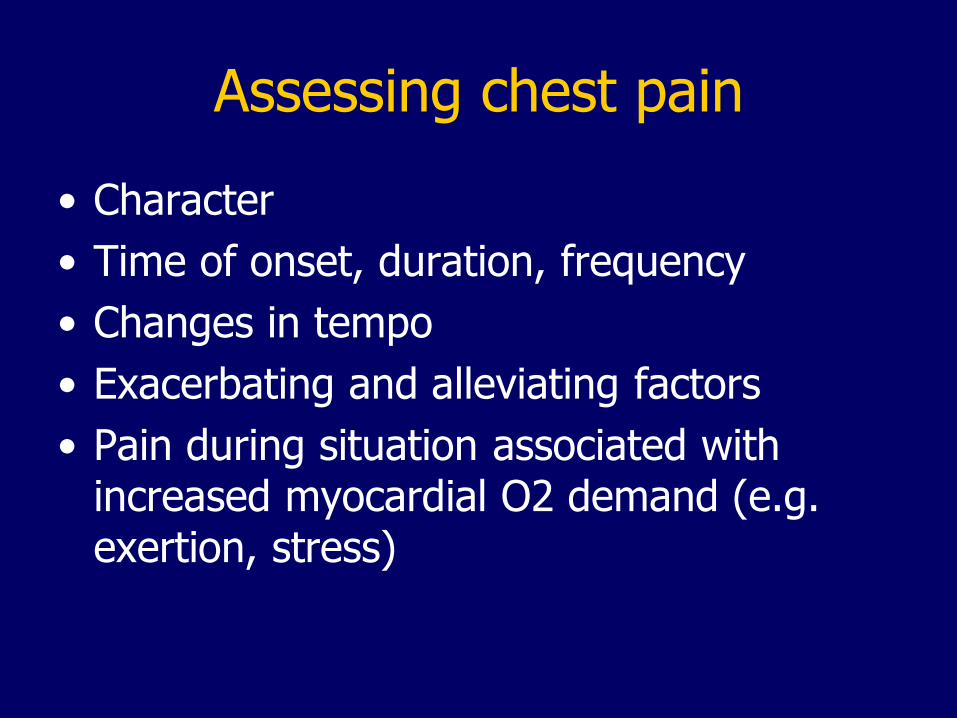
Assessing chest pain
• Character
• Time of onset, duration, frequency
• Changes in tempo
• Exacerbating and alleviating factors
• Pain during situation associated with increased myocardial O2 demand (e.g. exertion, stress)
Character of anginal pain
• Localized usually at precordium
• Radiate to arm, neck, shoulder, back or epicardium
• Feels like being pressed by heavy object, orconstricting or crushing.
• Concomitant systemic symptoms: dyspnea, dizziness, nausea, diaphoresis
• Not related to movement/body position, cough, other obvious cause e.g. herpes, trauma
Character of anginal pain
• Some feels epigastrial pain, similar to gastritis• Only 54% report typical angina• 34% “burning”, or “indigestion”• 32% chest pain • 20% stabbing, sharp pain• 42% undescribable• Can be atypical in the elderly, diabetic• Patient without CAD: sharp localized pain,
pleuritic, positional, increased with tactile pressure almost always not ischemia.
Classification of Angina
• Typical vs atypical angina vs non cardiac• Angina equivalent• Stable Angina• Unstable angina
– Angina in myocardial infarct
Stable Angina Pectoris
• Provoked by exertion or emotional stress; increasing demand triggers ischemia
• Relieved by rest or nitroglycerin
Pedoman tatalaksana SKA tanpa ST elevasi, PERKI 2008
Severity in Stable Angina
• I : angina occurring with strenous but not ordinary physical activity
• II : Slight limitation of ordinary physical activity
• III : Marked limitation of ordinary physical activity
• IV : Inability to carry on any physical activity without discomfort, symptoms may be present at rest.
Unstable angina
1. Angina at rest
2. Angina first onset
3. Progressive anginaSignificant worsening of stable angina, increasingintensity/frequency, longer duration, triggeredeasier, harder to alleviate
4. Angina after infarctAngina after infarct recovery
Pedoman tatalaksana SKA tanpa ST elevasi, PERKI 2004
Differential Diagnosis
of Chest Pain
Cardiac• ACS : Infarct,angina
• MVP
• Aortic Stenosis
• Hypertrophic cardio-
myopathy
• Pericarditis
Lungs • Lung Emboli
• Pnemonia
• Pneumothorax
• Pleuritis
Gastrointestinal•Reflux esofagus
•Ruptur esofagus
•Gall bladder disease
•Peptic Ulcer
•Pancreatitis
Vascular•Aortic dissection/aneurysma
Others•Musculoskeletal
•Herpes zoster
CHEST PAINAdmission
Working
diagnosis
Bio-
chemistry
Risk
Stratification
Management
Secondary
prevention
Suspected ACS
Persistent
ST elevation
No persistent
ST elevation
Troponin,
CKMB (+)
Risk: high / low
Algorithm in Acute Coronary Syndrome
Modified from ESC 2007
- ACS unlikely
- NSTEMI
- STEMI
ECG
Initial management,
±revascularization
Medical therapy,
coronary angiography
Perform
ed in 10 min
{on serial
ECG}
Troponin,
CKMB (+)
Initial tx
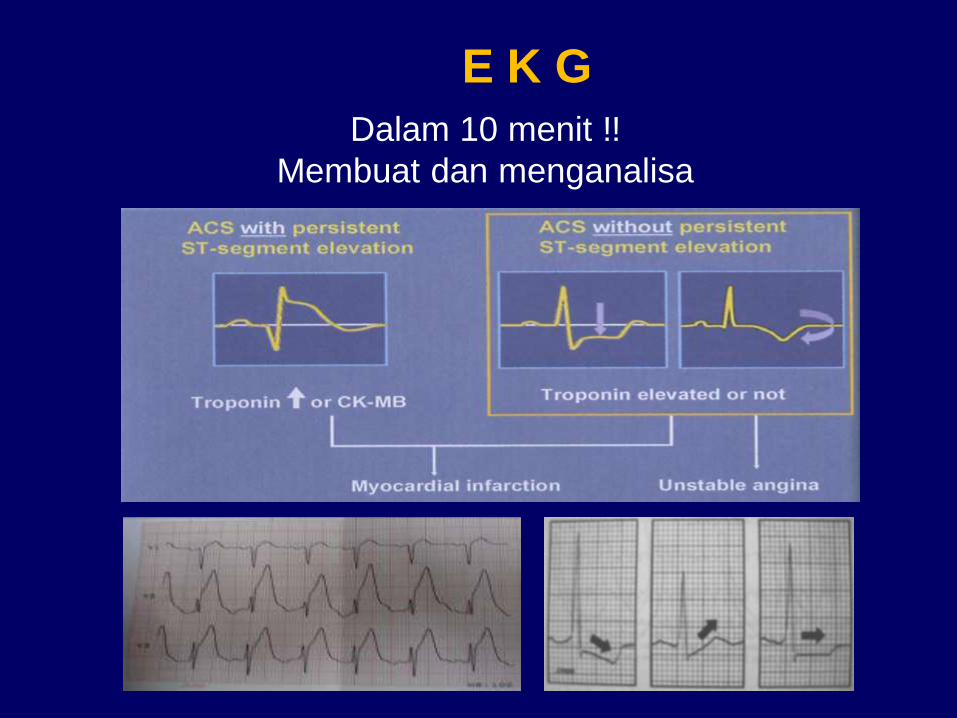
Dalam 10 menit !!
Membuat dan menganalisa
E K G
Case
• Tn mahmudin 50th..os merasa lemas pada sisi
kiri tubuh sejak 1 hari yg lalu secara
mendadak..mulut mencong (-), bicara pelo (-),
minum tersedak (-), nyeri dada (-)..riwayat
merokok sejak remaja 1-2 bungkus sehari,
berhenti sejak 10 thn yll..riwayat HT (+), tidak
terkontrol, DM (-), riwayat serangan jantung 10
thn yll..KU baik, kes CM, GCS 15, TD 150/90, N
90, RR 20, suhu 37, 9..motorik 5/5, 5/5. CKMB
16, serial ecg N
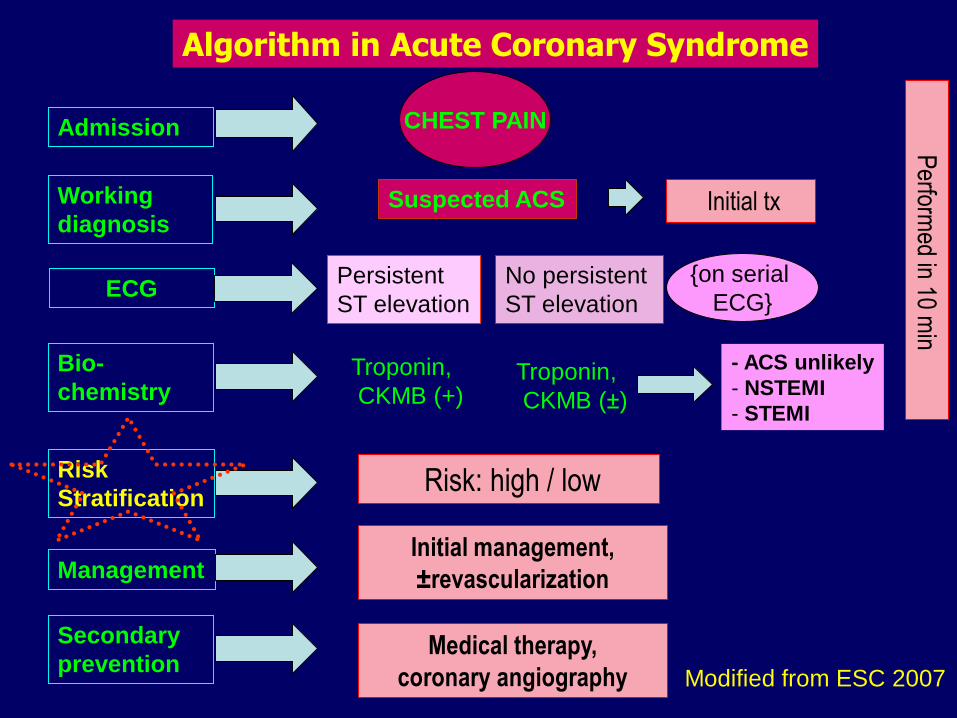
CHEST PAINAdmission
Working
diagnosis
Bio-
chemistry
Risk
Stratification
Management
Secondary
prevention
Suspected ACS
Persistent
ST elevation
No persistent
ST elevation
Troponin,
CKMB (+)
Risk: high / low
Algorithm in Acute Coronary Syndrome
Modified from ESC 2007
- ACS unlikely
- NSTEMI
- STEMI
ECG
Initial management,
±revascularization
Medical therapy,
coronary angiography
Perform
ed in 10 min
{on serial
ECG}
Troponin,
CKMB (±)
Initial tx
• Recommendation: CK, CKMB & Troponin upon admission and serial in 4-6 hours if initially normal
• LDH, SGOT/SGPT and other enzymes not recommended
• Increase of plasma CK plasma & CK-MB happens early, but less specific
• Increase of TnI & TnT are more specific in diagnosingmarker MI; level corresponds with prognosis.
Biomarkers
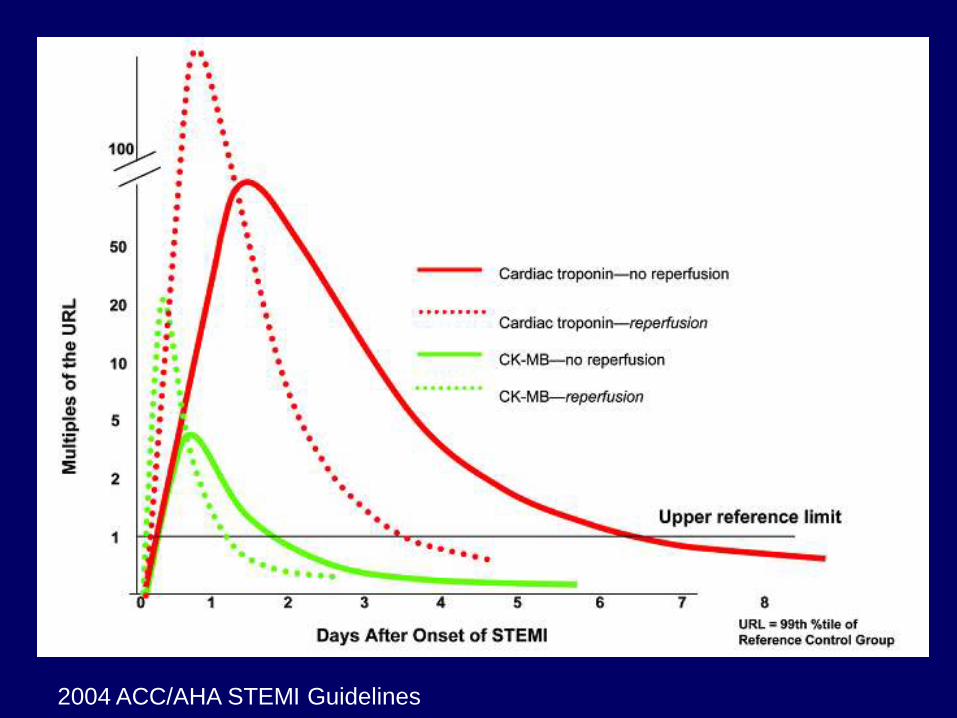
2004 ACC/AHA STEMI Guidelines
CHEST PAINAdmission
Working
diagnosis
Bio-
chemistry
Risk
Stratification
Management
Secondary
prevention
Suspected ACS
Persistent
ST elevation
No persistent
ST elevation
Troponin,
CKMB (+)
Risk: high / low
Algorithm in Acute Coronary Syndrome
Modified from ESC 2007
- ACS unlikely
- NSTEMI
- STEMI
ECG
Initial management,
±revascularization
Medical therapy,
coronary angiography
Perform
ed in 10 min
{on serial
ECG}
Troponin,
CKMB (±)
Initial tx
High risk
• Repetitive or prolonged (> 10 minutes) ongoing
chest pain;
• Elevated level of at least one cardiac biomarker
(troponin or creatine kinase-MB isoenzyme);
• Persistent or dynamic ST depression 0.5 mm or
new T-wave inversion
• Transient ST-segment elevation ( 0.5 mm) in
more than two contiguous leads;
Guideline ACS 2006 National Heart Foundation Australia
High risk (2)
• Haemodynamic compromise — Syst. BP< 90 mmHg, cool peripheries, diaphoresis, Killip Class > I, and/or new-onset mitral regurgitation;
• Sustained ventricular tachycardia;
• Syncope;
• LV syst dysfunction (ejection fraction < 0.40);
• Prior PCI or CABG within 6 months or prior
• Diabetes;
• Chronic kidney disease (estimated GFR< 60 mL/minute)
Guideline ACS 2006 National Heart Foundation Australia
Intermediate risk
• Chest pain within 48 hours that occurred at rest, or was repetitive or prolonged (but currently resolved)
• Age >65 years
• Known CAD — prior infarction withEF>0.40, or known 50% coronary stenosis
• No high-risk changes on ECG
Guideline ACS 2006 National Heart Foundation Australia
Intermediate risk (2)
• Two or more of risk factors: hypertension, family history, active smoking or hyperlipidemia
• Diabetes (with atypical symptoms of ACS);
• Chronic kidney disease (estimated GFR<60 mL/minute) (with atypical symptoms of ACS)
• Prior aspirin use
Guideline ACS 2006 National Heart Foundation Australia
Low risk
• Acute coronary syndrome without
intermediate-risk or high-risk features.
• This includes
– onset of angina within the last month,
– worsening in severity or frequency of angina,
– lowering of anginal threshold
Guideline ACS 2006 National Heart Foundation Australia
CHEST PAINAdmission
Working
diagnosis
Bio-
chemistry
Risk
Stratification
Management
Secondary
prevention
Suspected ACS
Persistent
ST elevation
No persistent
ST elevation
Troponin,
CKMB (+)
Risk: high / low
Algorithm in Acute Coronary Syndrome
Modified from ESC 2007
- ACS unlikely
- NSTEMI
- STEMI
ECG
Initial management,
±reperfusion
Medical therapy,
coronary angiography
Perform
ed in 10 min
{on serial
ECG}
Troponin,
CKMB (±)
Initial tx
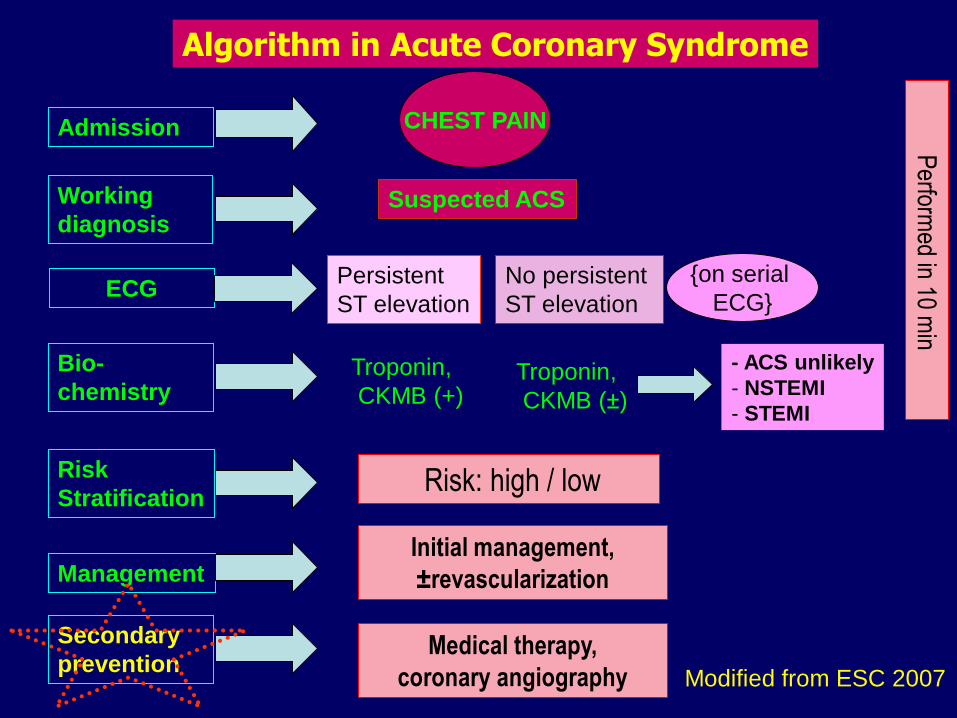
CHEST PAINAdmission
Working
diagnosis
Bio-
chemistry
Risk
Stratification
Management
Secondary
prevention
Suspected ACS
Persistent
ST elevation
No persistent
ST elevation
Troponin,
CKMB (+)
Risk: high / low
Algorithm in Acute Coronary Syndrome
Modified from ESC 2007
- ACS unlikely
- NSTEMI
- STEMI
ECG
Initial management,
±revascularization
Medical therapy,
coronary angiography
Perform
ed in 10 min
{on serial
ECG}
Troponin,
CKMB (±)
A Aspirin and Anticoagulants
B Beta blockers and Blood Pressure
C Cholesterol and Cigarettes
D Diet and Diabetes
E Education and Exercise
F Fun and Faith
Secondary prevention strategy
• Rawat tirah baring
• Puasa 8 jam
• IVFD NaCl 0,9% atau D5W% 1 kolf/24 jam
• Aspirin 160 mg dikunyah,selanjutnya 1 x 80 mg ( besok )
• Clopidogrel 4 tab ( 300 mg ), selanjutnya 1 x 75 mg ( besok )
• ISDN 3 x 5 mg
• Atorvastatin 1 x 40 mg
• Bisoprolol 1 x 2,5 mg
• Diazepam 1 x 5 mg / Clobazam 1 x 10 mg / Alprazolam 1 x 0,5 mg
• Laxadine syrup 1 x CI
• Heparin dg UFH / LMWH selama 5 hari
• Rontgen torak
• EKG tiap hari
• Cek Profil lipid, GDS, Ureum, Kreatinin, elektrolit besok
• ACE inhibitor ( bila ada hipertensi )
CONTOH INSTRUKSI DOKTER
UAP / NSTEMI
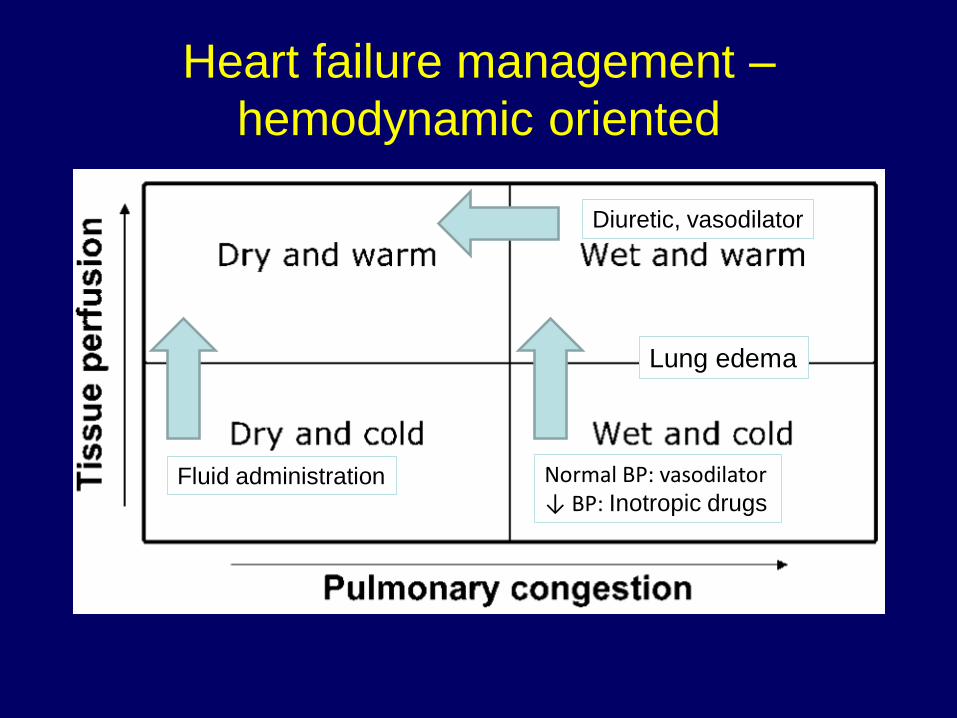
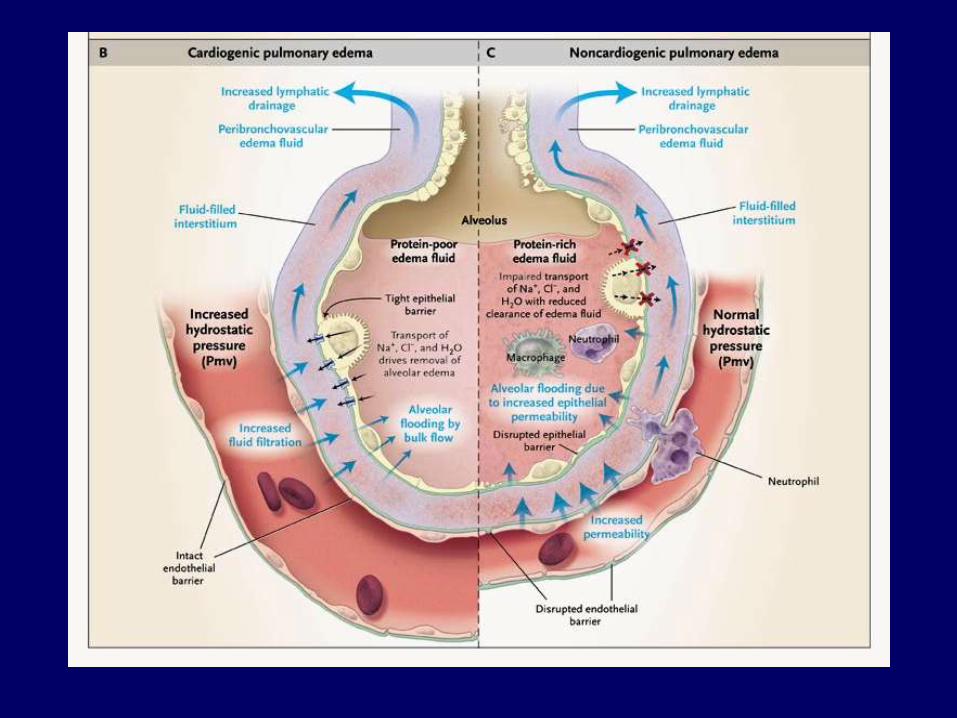
Heart failure management –
hemodynamic oriented
Fluid administration Normal BP: vasodilator↓ BP: Inotropic drugs
Diuretic, vasodilator
Lung edema
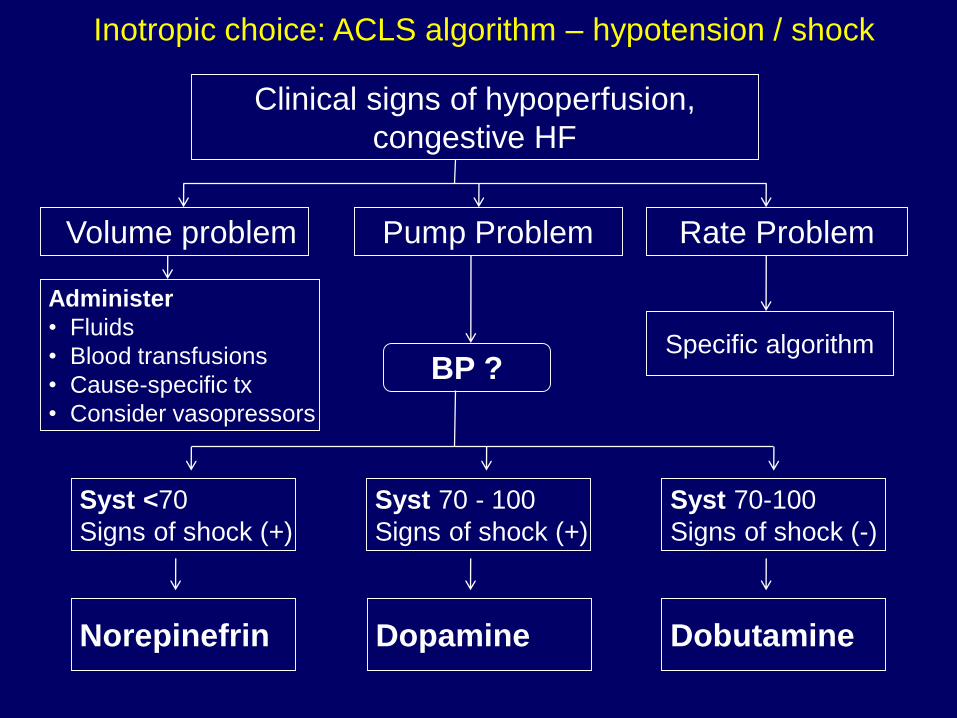
Volume problem
Administer
• Fluids
• Blood transfusions
• Cause-specific tx
• Consider vasopressors
Rate ProblemPump Problem
Specific algorithm
Clinical signs of hypoperfusion,
congestive HF
BP ?
Syst 70 - 100
Signs of shock (+)
Syst 70-100
Signs of shock (-)
Syst <70
Signs of shock (+)
Norepinefrin Dopamine Dobutamine
Inotropic choice: ACLS algorithm – hypotension / shock
Algorithm in ACLS
Algorithm in ACLS
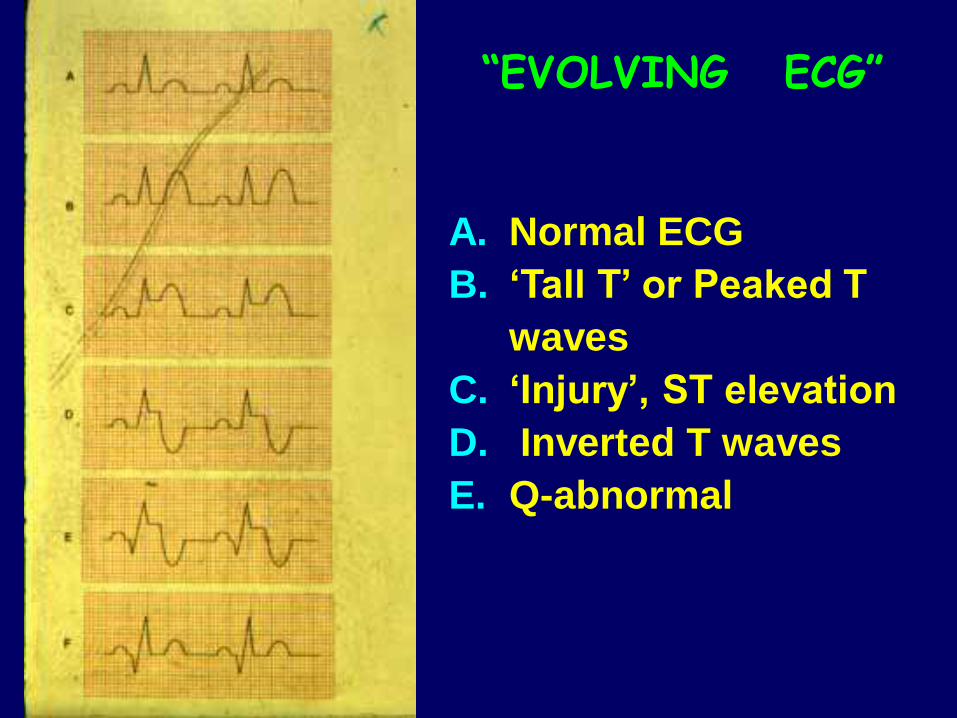
A. Normal ECG
B. ‘Tall T’ or Peaked T
waves
C. ‘Injury’, ST elevation
D. Inverted T waves
E. Q-abnormal
“EVOLVING ECG”
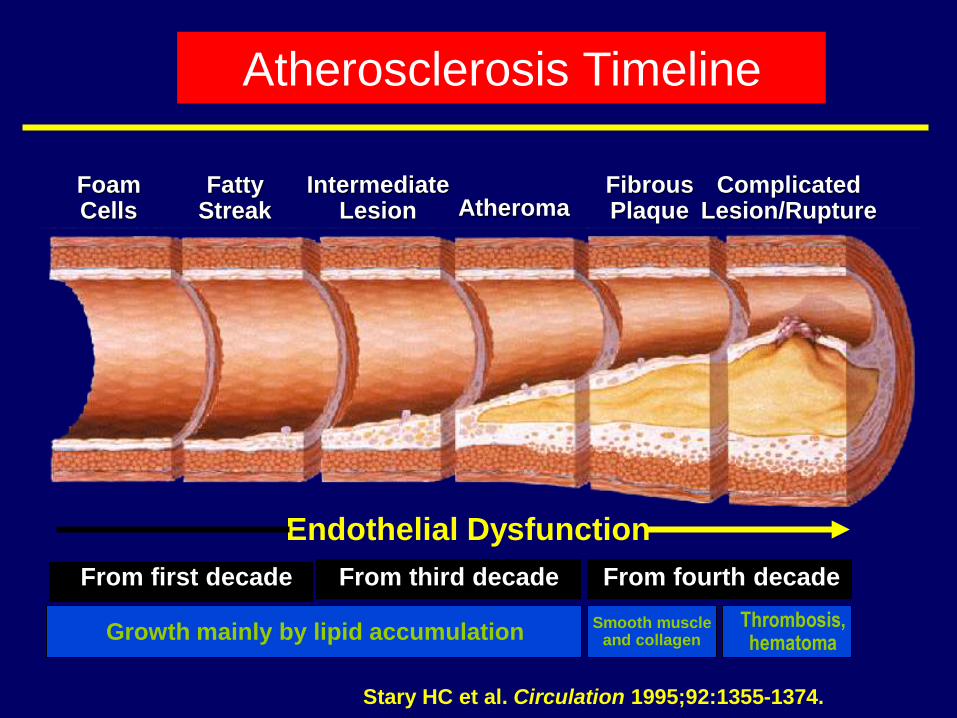
FoamCells
FattyStreak
IntermediateLesion Atheroma
FibrousPlaque
ComplicatedLesion/Rupture
Endothelial Dysfunction
Smooth muscleand collagen
From first decade From third decade From fourth decade
Growth mainly by lipid accumulationThrombosis,hematoma
Stary HC et al. Circulation 1995;92:1355-1374.
Atherosclerosis Timeline
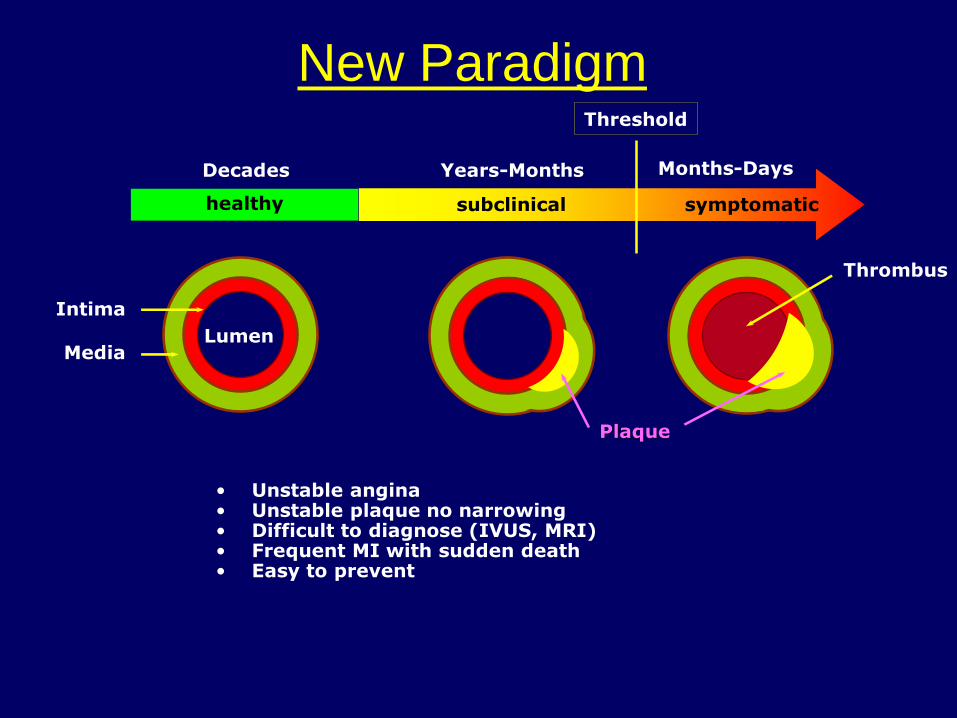
New Paradigm
healthy subclinical symptomatic
Threshold
Decades Years-Months Months-Days
Intima
Media
Plaque
Thrombus
Lumen
• Unstable angina• Unstable plaque no narrowing• Difficult to diagnose (IVUS, MRI)• Frequent MI with sudden death• Easy to prevent