dr. andriana purnama, spb-kbd alamat kantor : divisi bedah digestif fk unpad/rshs jl. pasteur no. 38...
TRANSCRIPT
Dr. Andriana Purnama, SpB-KBDAlamat Kantor : Divisi Bedah Digestif FK UNPAD/RSHS
Jl. Pasteur No. 38 Bandung 40161Telp/Fax Kantor : 022-2034574Alamat Rumah : Jl. Babakan Jeruk III No. 23 BandungTelp/Fax rumah : -No.HP : 08122025557Tempat/Tgl Lahir: Bandung, 09 Juni 1972Email : -Profesi : Dokter Konsultan Bedah DigestifJabatan :
1. Staf Divisi Bedah Digestif RSHS 2. -
Penetrating Abdominal Trauma: Guidelines For
Evaluation
Andriana PurnamaDepartment of SurgeryHasan Sadikin Hospital
Faculty of Medicine Padjadjaran UniversityBandung
HOT TOPICS
Interest in selective non-operative management(SNOM) of PAI began to increase.
SNOM for stab wounds is now common
SNOM for gunshot wounds remains controversial
The doctor should answer 2 questions :
1. Is there intra abdominal injury ?2. Does this injury require operative
repair ?

DO It or not???

Risks of Operative Management of Abdominal Trauma
Higer Unnecessary Laparatomy RateMorbidityMortalityLonger Hospital StaysIncreased Hospital Costs
Mc.Connell DB & Trunkey .DD : Nonoperative Management of Abdominal Trauma, in Surg.Clin.North Am, 1990 (70) :3, 679.
Risks of NOM of Abdominal Trauma
Missed injuryMorbidityMortalityContinued bleedingTransfusion riskAbdominal Compartment Syndrome
Mc.Connell DB & Trunkey .DD : Nonoperative Management of Abdominal Trauma, in Surg.Clin.North Am, 1990 (70) :3, 678.
History Until the early 1900s, PAI was managed
conservatively.World War I :
patients who underwent mandatory operative exploration had a better chance of survival, Laparotomy became the standard of care.
World War II : early laparotomy improved survival.
1950, laparotomy was the standard treatment of PAI pts
1960, Shaftan : high rate of negative laparotomies published a report on the Non Operative Management of abdominal injury He had managed 125 of 180 PAI patients
without surgery, with a mortality rate < 1 %
Introduction
Recent guidelines have recommended :
* Observation for haemodynamically stable patients
with no evidence of peritonitis for stab wounds and tangential GSW
* Up to 30 % of anterior abdominal GSW & 67 % of gunshot injuries to the back, can be managed safely without operative
interventionZafar NS, Rushing A, Haut ER, Kisat MT, Villegas CV, Chi A et al, Outcome of selective non-operative management of penetrating abdominal injuries from the North American National Trauma Database, British Journal of Surgery 2011; 99(Suppl 1): 155–165
Mechanism of injury
Low velocityKnife wound/stab woundsDisrupts only structures penetrated
Medium velocityHandguns and pellet guns
High velocityMilitary weapons and rifles
Gunshot Wound VS Stab Wound
GSW SW
The most commonly injured organs
1. Small bowel (50%)2. Colon (40%)3. Liver (30%)4. Abdominal vascular
structures (25%)
The most commonly injured organs
1. Liver (40%)2. Small bowel (30%)3. Diaphragm (20%)4. Colon (15%)
Stab WoundDemetriades and Rabinowitz 1987 :
Prospective study of 651 patients with stab wounds to the anterior abdomen treated with SNOM
Based mainly on serial physical examinations. Half cases were successfully managed without laparotomy. Eleven (1.6%) patients who were initially observed,
required a laparotomy later, No mortality among them. The accuracy of the initial physical examination was
93.9% (false negative initial exam 3.2%, false negative exam 2.9%).
Demetriades D, Velmahos GC, Indications for & Techniques of Laparotomy, in Feliciano DV, Mattox KL, Moore EE, Trauma, 7th ed, 2013
Stab Wound
Shorr et al 1988 :330 patients with abdominal stab
wounds :32% of had a therapeutic laparotomy 14% a non therapeutic laparotomy. 53% were discharged without an
operation.Demetriades D, Velmahos GC, Indications for & Techniques of Laparotomy, in Feliciano DV, Mattox KL, Moore EE, Trauma, 7th ed, 2013
Stab WoundIndications for laparotomy such as :
peritoneal penetration, omental evisceration, free air on abdominal radiographs, blood on abdominal paracentesis are debated.1. 69% associated with significant intra-abdominal
injuries, even in the absence of generalized abdominal tenderness
2. Others have found no such association : continue to use SNOM avoid routine operation
SNOM should be considered only in centers with experience & appropriate in-house staffing by trauma surgeons.
Stab Wound
In most patients :Decision to operate or not, should be based on1. serial physical exams and 2. close hemodynamic monitoring.
Demetriades D, Velmahos GC, Indications for & Techniques of Laparotomy, in Feliciano DV, Mattox KL, Moore EE, Trauma, 7th ed, 2013
Gunshot Wound
Abdominal GSW are treated by routine laparotomy in most trauma center
GSWs to the abdomen are still commonly treated with mandatory exploration because of multiple reports emphasizing a high incidence of intra-abdominal injuries
GSWs1. Demetriades D, Velmahos GC, Cornwell EE III
1997 : ⅓ GSW to anterior abdomen ⅔ GSW to the back No significant intra abdominal injury safe to SNOM
2. Velmahos GC, Demetriades D, Toutouzas KG 2001 : 1856 GSW pts : 1405 anterior / 451 posterior –
8 yr period 47% : no significant abdominal injury
39% anterior / 74% posterior GSW 80 pts ( 4% ) developed signs delayed
laparotomy 5 pts (0.3%) : complications managed
successfully
Demetriades D, Velmahos GC, Indications for & Techniques of Laparotomy, in Feliciano DV, Mattox KL, Moore EE, Trauma, 7th ed, 2013
G S WsBased on these observations
Selected patients with : isolated gunshot wounds to solid organs (liver, spleen,
kidney) hemodynamically stable no peritoneal signs,
may be managed nonoperatively
In a study of 152 patients with gunshot injuries to the liver, 21% of cases with isolated liver injury were successfully managed non operatively
Demetriades D, Velmahos GC, Indications for & Techniques of Laparotomy, in Feliciano DV, Mattox KL, Moore EE, Trauma, 7th ed, 2013
Serial Physical Examination
A careful initial physical examination followed by serial examinations :Are the most
important tool to set the indications for laparotomy after abdominal stab wounds.
Realible in detecting significant Injuries
after PAI, if performed by experienced
clinicans and preferably by the same team
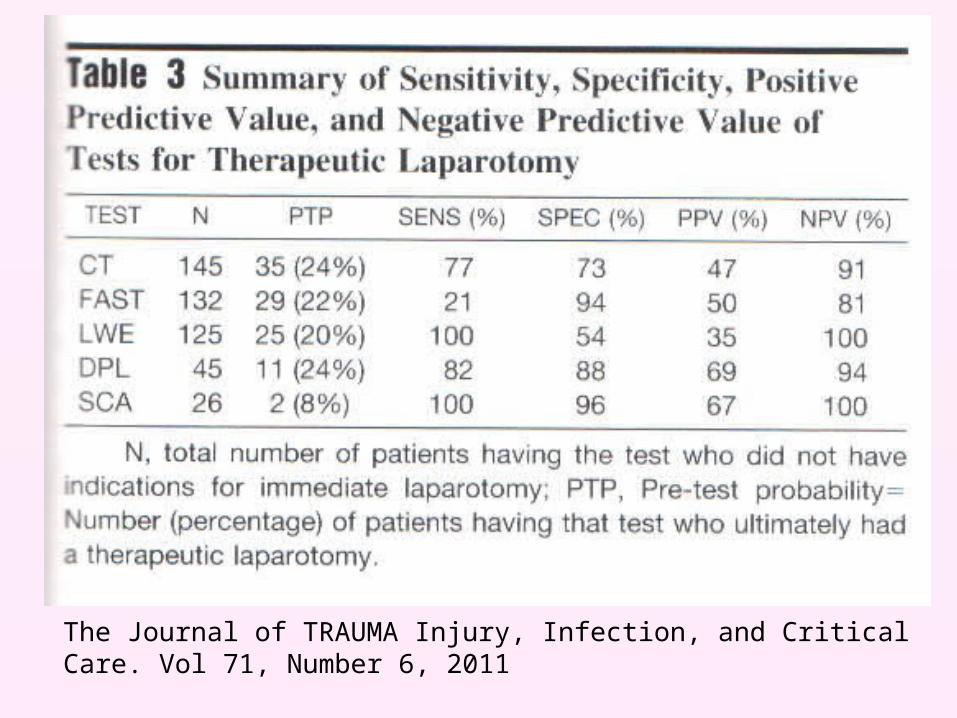
The Journal of TRAUMA Injury, Infection, and Critical Care. Vol 71, Number 6, 2011
Serial Physical Examination
Diagnostic Peritoneal Lavage
DPL has been used to identify significant peritoneal injury after PAI for at least 30 years and still has arole in Trauma Care
DPL reduced unnecessary LAP, Rapid, Safe and Highly cost-effective
Diagnostic Peritoneal Lavage
When the Concept of Selective Management rather than Mandatory LAP began to receive more attention, The Non Invasive Tools become more popular adjuncts
The more recent literatur Suggest that DPL now seems to be Increasingly replaced by the use of other diagnostic modalities
The Journal of TRAUMA Injury, Infection, and Critical Care. Vol 71, Number 6, 2011
Diagnostic Peritoneal Lavage - DPL
For hemodynamically stable patients CT scan For hemodynamically unstable patients FAST DPL is used predominantly when :
1. CT or FAST are not available, 2. No sufficient expertise to make decisions based
on the FAST results, 3. FAST results are negative, but there is no other
source to account for the hemodynamic instability.
Local Wound Exploration
LWE has been used in a number of series to rule out penetration of the Anterior Fascia
If the patient has no penetration of the anterior Fascia, the patient may be safely discharged from the ED
When LWE is used alone to determine Laparatomy there will be a high unnecessary Laparatomy Rate
Even the peritoneum is penetrated were used as a Cutt- Off, many patients will have no intra peritoneal Injury, or an Injury that does not require surgical Intervention
Most Commonly: Omental Laceration, Mesenteric Laceration or Liver tears that have stopped Bleeding
Most Authors have Investigated; LWE (+), Laparatomy Negative almost 50%
Management Guidelines for Penetrating Abdominal Trauma. Current Opinion in Critical Care 2010, 16:609-617
Local Wound Exploration

Ultrasonography - FASTExcellent sensitivity in identifying intra-
abdominal fluidEase of use, repeatability, and avoidance of
radiationThe most significant contribution of the
FAST is : detection of intra-abdominal fluid in the : hemodynamically unstable and clinically unevaluable blunt trauma victim. immediate exploratory laparotomy
Negative FAST further evaluation - most commonly CT
Abdominal Computed Tomography
Show accurate imaging of solid parenchymal injury
Major role in decision to manage the injured spleen, liver & kidney nonoperatively
Increase use in blunt traumaUse in evaluation of abdominal GSW,
selected for nonoperative management ( SNOM )
Abdominal CT has become an indispensable tool in the evaluation of abdominal trauma.
Diagnostic Laparoscopy
Major limitation : Inability to :1. “ Run “ the bowel2. Diagnose retroperitoneal injuries3. Expose adequately deep lying organs4. Estimate accurately the quantity of
hemoperitoneum
≈ ½ existing injuries can be missed by laparoscopy
Vilavicencio RT, Aucar JA, Analysis of laparoscopy in trauma, J Am Coll Surg 189:11, 1999
Diagnostic LaparoscopyAdvantages :Excellent ( > 95% ) Sensitivity &
Specifity to establish :1. Peritoneal violation2. Hemoperitoneum3. Enteric content spillage
Peritoneal penetration or hemoperitoneum :not always associated with therapeutic laparotomy the information provided by laparoscopy ???
Diagnostic Laparoscopy
It does not appear that laparoscopy has a role in the management of patients with PAI
The procedure does not appear to be cost effective, because it is rarely theurapeutic
(only 1 of 24 patients in WTA trials)
CURRENT MANAGEMENT OF PENETRATING ABDOMINAL INJURY (PAI)
Review of published literatures
Validating the Western Trauma Association Algorithm For Managing Patients With Anterior Abdominal Stab Wounds: A Western Trauma Association Multicenter Trial
The Journal of TRAUMA Injury, Infection, and Critical Care. Vol 71, Number 6, 2011
Western Trauma Association
Six Center of TraumaMay 2008-Nov 2010222 Pts PAI62 Pts had immediate LAP160 Pts Stable and Asymptomatic20 Pts D/C form ED after LWE (-)11 Pts Lap, When their clinical condition
changed
The Journal of TRAUMA Injury, Infection, and Critical Care. Vol 71, Number 6, 2011
The WTA proposed algorithm is designed for cost-effectiveness. Serial Clinical Assessments can be performed without the added
expense of CT, DPL or Laparoscopy
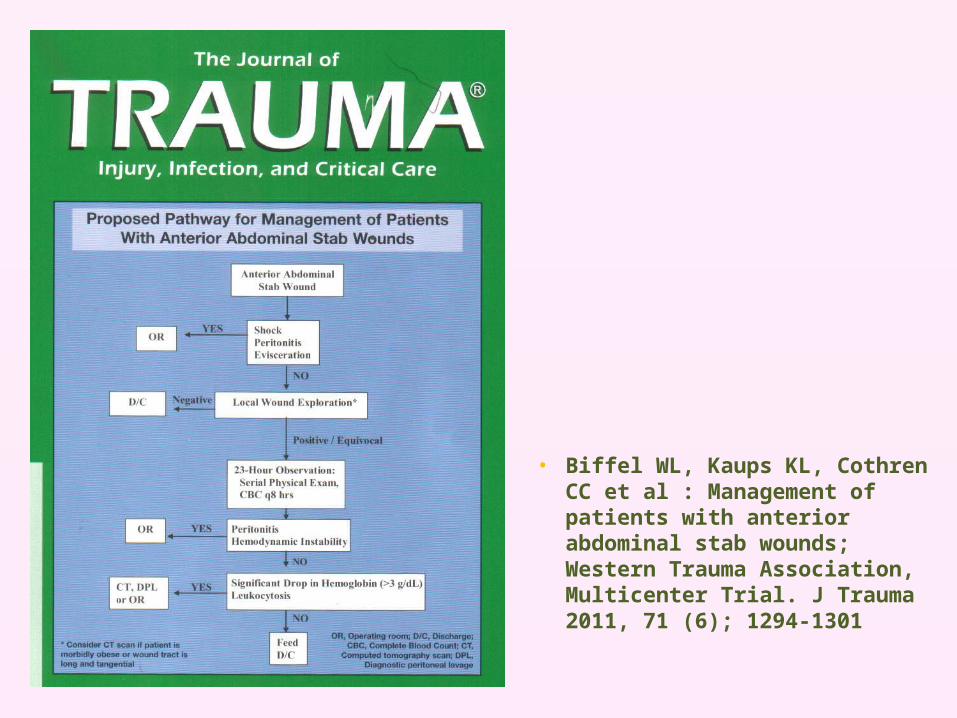
• Biffel WL, Kaups KL, Cothren CC et al : Management of patients with anterior abdominal stab wounds; Western Trauma Association, Multicenter Trial. J Trauma 2011, 71 (6); 1294-1301
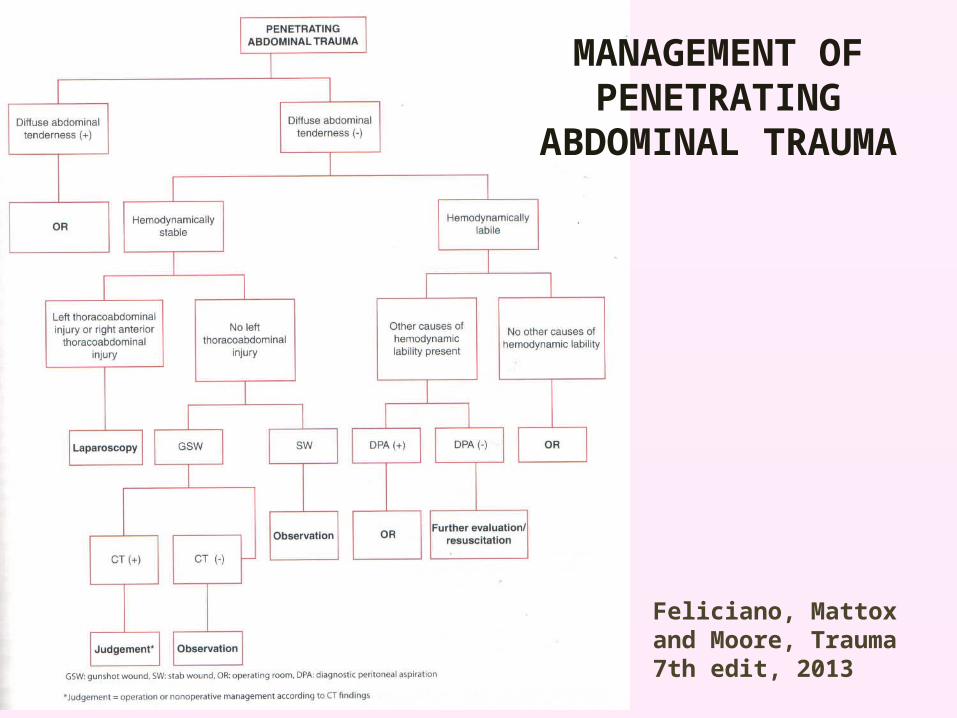
Feliciano, Mattox and Moore, Trauma 7th edit, 2013
MANAGEMENT OF PENETRATING
ABDOMINAL TRAUMA
Conditions for SNOM of PAI
How about practicing SNOM in trauma centers with a :1. Low volume of penetrating trauma 2. Inadequate resources to provide 24-hour in-house
coverage. 3. The inability to do serial physical examinations by
physicians with reasonable experience
prohibits the practice of SNOM
It may be safer for small trauma centers with limited exposure to GSW victims to retain a policy of routine laparotomy.
Conditions for SNOM of PAI
SNOM of PAI is recommended in :1. Facilities with the resources and experience to
select and monitor patients with PAI carefully,
2. Capability to provide immediate surgical intervention to those who need it.
Zafar SN, et al, Outcome of selective non-operative management of penetrating abdominal injuries from the North American National Trauma Database, BJS 2011; 99(Suppl 1): 155–165
SNOM : Success & FailureSuccess rate is 75–80 %
and improved over the time interval
Failure rate 10–20 % Failed SNOM is associated with :
- longer hospital stays & costs Failed SNOM ≈ mortality has not been
documented
Como J.J et al J Trauma, 2010, 68:721-733
RECOMMENDATIONS
a. Pts who are hemodynamically unstable or who have diffuse abdominal tenderness should be taken emergently for laparotomy (level 1)
b. Pts who are hemodynamically stable with an unrealable clinical examination ( i.e. brain injury, spinal cord injury, intoxication, or need for sedation or anesthesia). Should have further diagnostic investigation performed for intra peritoneal injury or undergo exploratory laparotomy (level 1)
c. A routine laparotomy is not indicated is hemodynamically stable pts with abdominal SWs without signs of peritonitis or diffuse abdominal tenderness (away from the wounding site) in centers with expertise (level 2).
d. A routine laparotomy is not indicated in hemodynamically stable pts with abdominal GSWs if the wounds are tangential and there are no peritoneal signs (level 2)
RECOMMENDATIONS
e. Serial physical examination is reliable in detecting significant injuries after penetrating trauma to the abdomen, if performed by experienced clinicians and preferable by the same team (level 2)
f. In pts selected for initial NOM, abdomino pelvic CT should be strongly considered as a diagnostic tool to fasicilitate initial management decision (level2)
RECOMMENDATIONS
g. Pts with penetrating injury isolated to the right upper quadrant of the abdomen may be managed without laparotomy in the presence of stable vital signs, reliable examination, and minimal to no abdominal tenderness (level 3)
h. The majority of pts with penetrating abdominal trauma managed non operatively may be discharged after 24 hours of observation in the presence of a reliable abdominal examination and minimal to no abdominal tenderness (level 3)
i. Diagnostic laparoscopic may be considered as a tool to evaluate diaphragmatic lacerations and peritoneal penetration (level 2)
RECOMMENDATIONS
Conclusion
The rate of Unnecessary Laparatomy should be minimized
NOM should never be at the expense of a delay in the diagnosis and tratment of Injury
A part of anterior stab wound and GSW victims can be managed non operatively safely
