belajar ekg yuk
DESCRIPTION
bnTRANSCRIPT
BELAJAR EKG YUK
Kebanyakan para perawat kita ahli dalam pemasangan EKG, tapi sebagian besar dari mereka tidak tahu apa itu EKG, cara membaca dan bahkan lokasi pemasangan yang benar. Berikut sedikit tutorial yang dapat di berikan.
Hal ini disajikan dalam bahasa sederhana, sehingga mudah dipahami, untuk mempelajari lebih mendalam silahkan baca buku dan jangan tidak semangat untuk membaca.
Modul lengkap EKG dalam English ada di terakhir halaman, silahkan di Download (Gratis).
1. Pendahuluan
Elektrokardiografi adalah ilmu yang mempelajari aktifitas listrik jantung. Sedangkan Elektrokardiogram (EKG) adalah suatu grafik yang menggambarkan rekaman listrik jantung. Kegiatan listrik jantung dalam tubuh dapat dicatat dan direkam melalui elektroda-elektroda yang dipasang pada permukaan tubuh.
Prinsip utama belajar EKG adalah mengetahui anatomi fisiologi jantung, dan persyarafan jantung sehingga pada saat belajar EKG sudah dapat membayangkan keadaan jantung.
2. Anatomi Fisiologi Jantung
Jantung terdiri dari 4 bagian yaitu atrium (dextra & sinistra) & ventrikel (dextra & sinistra). Jantung mempunyai aktifitas listrik meliputi: Sino Atrio Nodus, Atrio Ventrikuler Nodus, Berkas His dan Serabut Purkinje, inilah point penting dalam pembacaan EKG.
Lihat gambar dibawah bagaimana aktifitas listrik jantung bekerja:
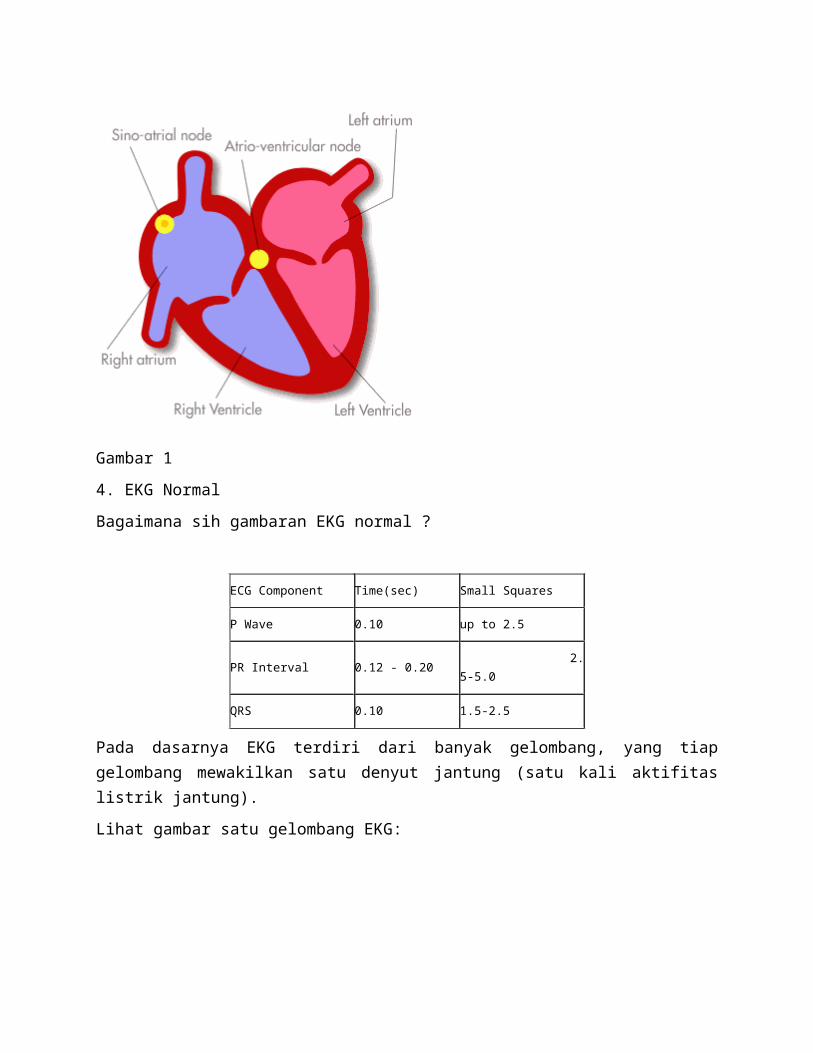
Gambar 1
4. EKG Normal
Bagaimana sih gambaran EKG normal ?
ECG Component Time(sec) Small Squares
P Wave 0.10 up to 2.5
PR Interval 0.12 - 0.20 2.5-5.0
QRS 0.10 1.5-2.5
Pada dasarnya EKG terdiri dari banyak gelombang, yang tiap gelombang mewakilkan satu denyut jantung (satu kali aktifitas listrik jantung).
Lihat gambar satu gelombang EKG:
Gambar 2
Dalam satu gelombang EKG terdiri ada yang disebut titik (lihat gambar), interval dan segmen. Titik terdiri dari titik P, Q, R, S, T dan U (kadang sebagian referensi tidak menampilkan titik U) sedangkan Interval terdiri dari PR interval, QRS interval dan QT interval dan Segmen terdiri dari PR segmen, dan ST segmen.
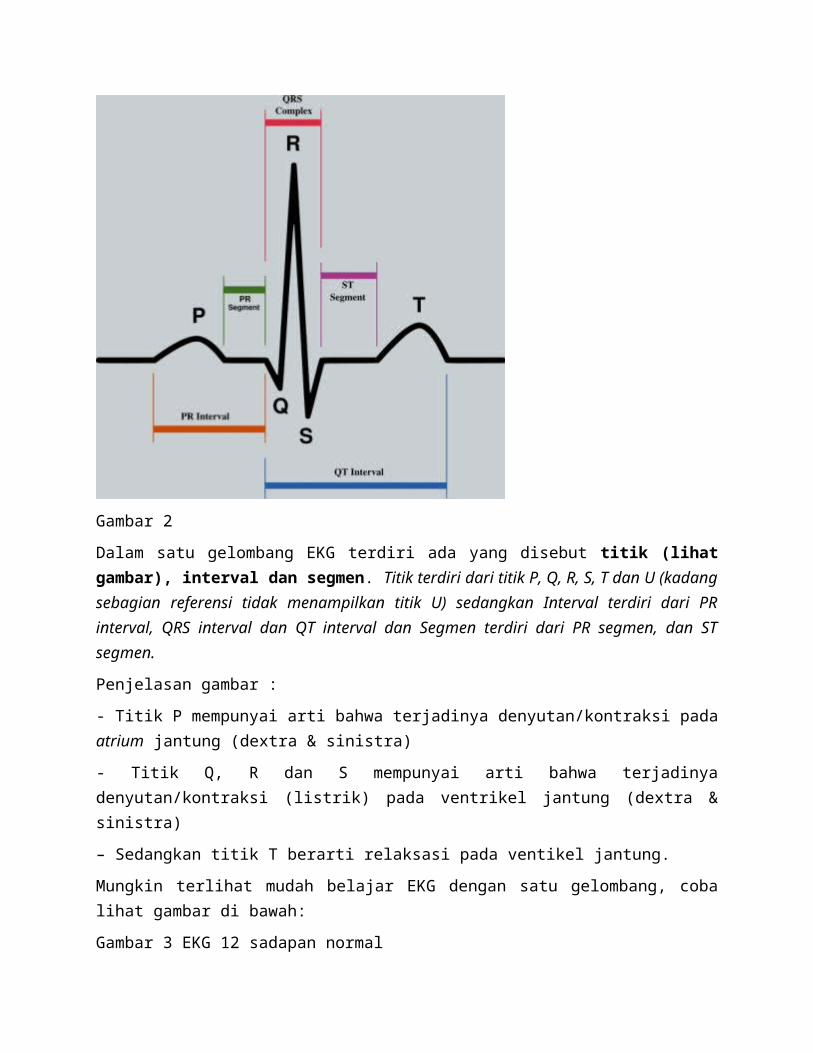
Penjelasan gambar :
- Titik P mempunyai arti bahwa terjadinya denyutan/kontraksi pada atrium jantung (dextra & sinistra)
- Titik Q, R dan S mempunyai arti bahwa terjadinya denyutan/kontraksi (listrik) pada ventrikel jantung (dextra & sinistra)
– Sedangkan titik T berarti relaksasi pada ventikel jantung.
Mungkin terlihat mudah belajar EKG dengan satu gelombang, coba lihat gambar di bawah:
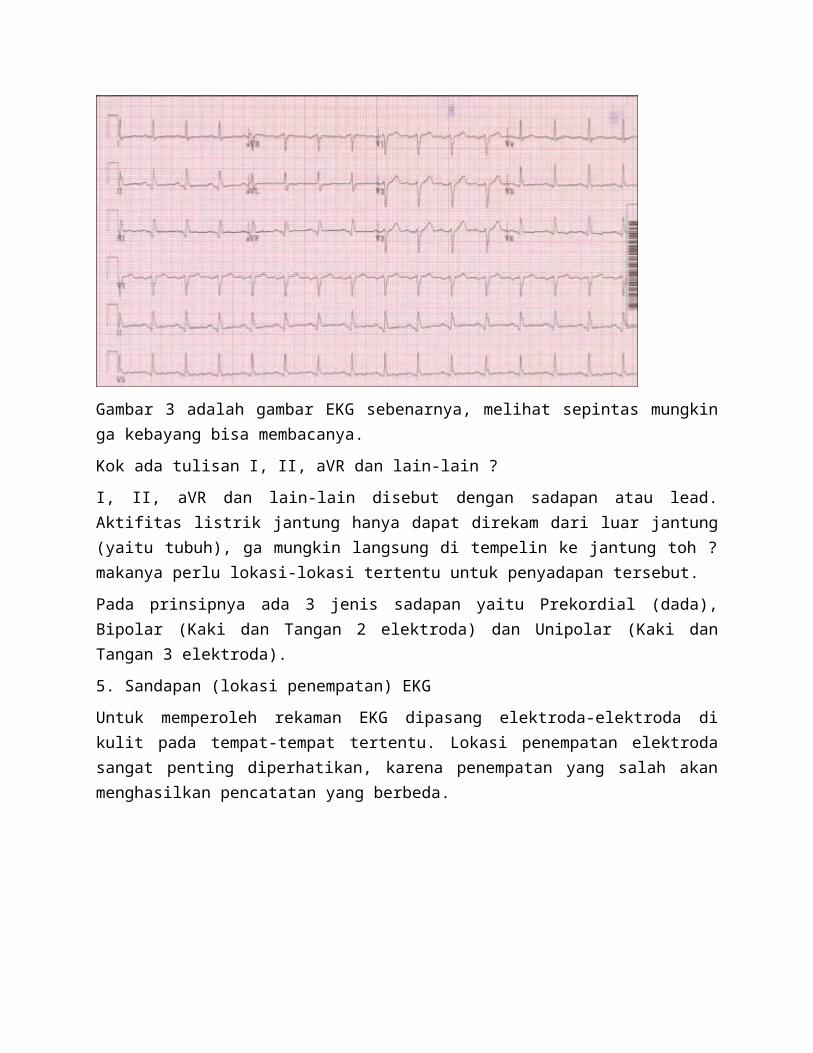
Gambar 3 EKG 12 sadapan normal
Gambar 3 adalah gambar EKG sebenarnya, melihat sepintas mungkin ga kebayang bisa membacanya.
Kok ada tulisan I, II, aVR dan lain-lain ?
I, II, aVR dan lain-lain disebut dengan sadapan atau lead. Aktifitas listrik jantung hanya dapat direkam dari luar jantung (yaitu tubuh), ga mungkin langsung di tempelin ke jantung toh ? makanya perlu lokasi-lokasi tertentu untuk penyadapan tersebut.
Pada prinsipnya ada 3 jenis sadapan yaitu Prekordial (dada), Bipolar (Kaki dan Tangan 2 elektroda) dan Unipolar (Kaki dan Tangan 3 elektroda).
5. Sandapan (lokasi penempatan) EKG
Untuk memperoleh rekaman EKG dipasang elektroda-elektroda di kulit pada tempat-tempat tertentu. Lokasi penempatan elektroda sangat penting diperhatikan, karena penempatan yang salah akan menghasilkan pencatatan yang berbeda.
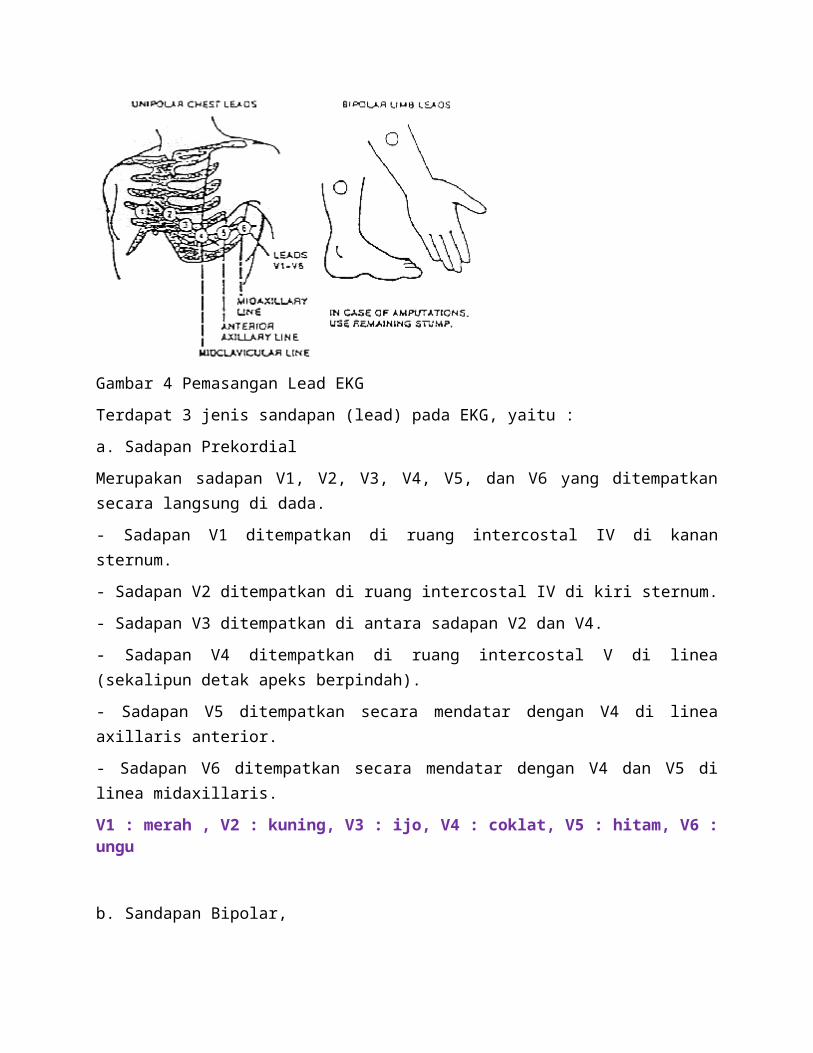
Gambar 4 Pemasangan Lead EKG
Terdapat 3 jenis sandapan (lead) pada EKG, yaitu :
a. Sadapan Prekordial
Merupakan sadapan V1, V2, V3, V4, V5, dan V6 yang ditempatkan secara langsung di dada.
- Sadapan V1 ditempatkan di ruang intercostal IV di kanan sternum.
- Sadapan V2 ditempatkan di ruang intercostal IV di kiri sternum.
- Sadapan V3 ditempatkan di antara sadapan V2 dan V4.
- Sadapan V4 ditempatkan di ruang intercostal V di linea (sekalipun detak apeks berpindah).
- Sadapan V5 ditempatkan secara mendatar dengan V4 di linea axillaris anterior.
- Sadapan V6 ditempatkan secara mendatar dengan V4 dan V5 di linea midaxillaris.
V1 : merah , V2 : kuning, V3 : ijo, V4 : coklat, V5 : hitam, V6 : ungu
b. Sandapan Bipolar,
Merekam perbedaan potensial dari 2 elektroda, yang ditandai dengan angka romawi I, II dan III
a) Sandapan I : merekam beda potensial antara tangan kanan (RA) yang bermuatan negatif (-) tangan kiri bermuatan positif (+).
b) Sandapan II : merekam beda potensial antara tangan kanan (-) dengan kaki kiri (LF) yang bermuatan (+)
c) Sandapan III : merekam beda potensial antara tangan kiri (LA) yang bermuatan (-) dan kaki kiri (+).
b. Sandapan Unipolar
a) Sandapan Unipolar Ekstremitas
· aVR : merekam potensial listrik pada tangan kanan (RA) yang bermuatan (+), dan elektroda (-) gabungan tangan kiri dan kaki kiri membentuk elektroda indifiren.
· aVL : merekam potensial listrik pada tangan kiri (LA) yang bermuatan (+), dan muatan (-) gabungan tangan kanan dan kaki kiri membentuk elektroda indifiren.
· aVF : merekam potensial listrik pada kaki kiri (LF) yang bermuatan (+) dan elektroda (-) dari gabungan tangan kanan dan kaki kiri membentuk elektroda indifiren.
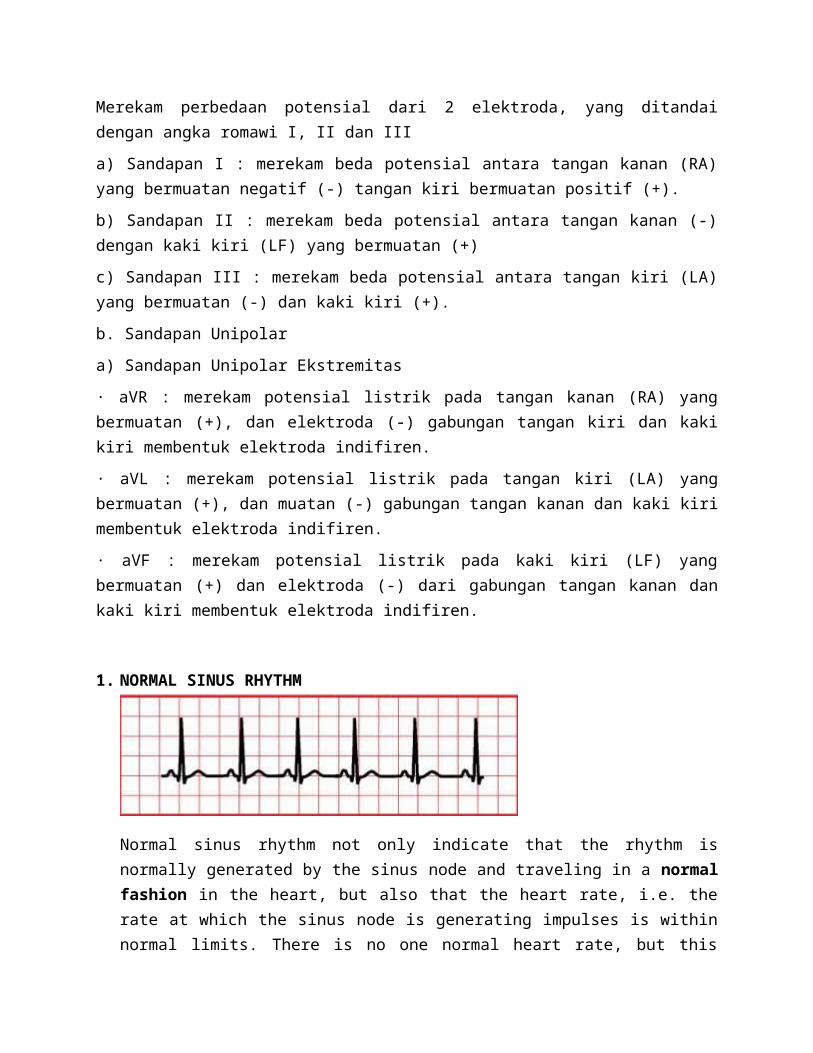
1. NORMAL SINUS RHYTHM
Normal sinus rhythm not only indicate that the rhythm is normally generated by the sinus node and traveling in a normal fashion in the heart, but also that the heart rate, i.e. the rate at which the sinus node is generating impulses is within normal limits. There is no one normal heart rate, but this varies by age. It is normal for a newborn to have a heart rate up to 150 beats per minute, while a child of five years of age may have a heart rate of 100 beats per minute. The adult's heart rate is even slower at about 60-80 beats per minute.
1. What is the rate and is it regular?
The heart rate is normal and the rhythm is regular.
2. Is the QRS wide or narrow?
The QRS complex is usually narrow, but it can be wide
if there is a conduction delay.
The QRS complex is normally less than 0.10 seconds.
QRS duration greater than 0.12 seconds is prolonged.
Rhythms with a narrow QRS are almost always supra-
ventricular. Wide QRS rhythms may originate in the
ventricle or be supraventricular with abnormal conduction.
3. Are P waves present and upright?
P waves are present and upright.
4. How are the P waves related to the QRS complex?
There is a fixed, 1-to-1 relationship between the
P waves and QRS complexes.
The impulse in normal sinus rhythm arises in the
SA node and spreads through the atria to the AV node.
The impulse then travels down the conducting system
and spreads through the ventricles. The P wave is
followed by a narrow QRS complex. The QRS complex can
be wide if there is aberrant conduction.
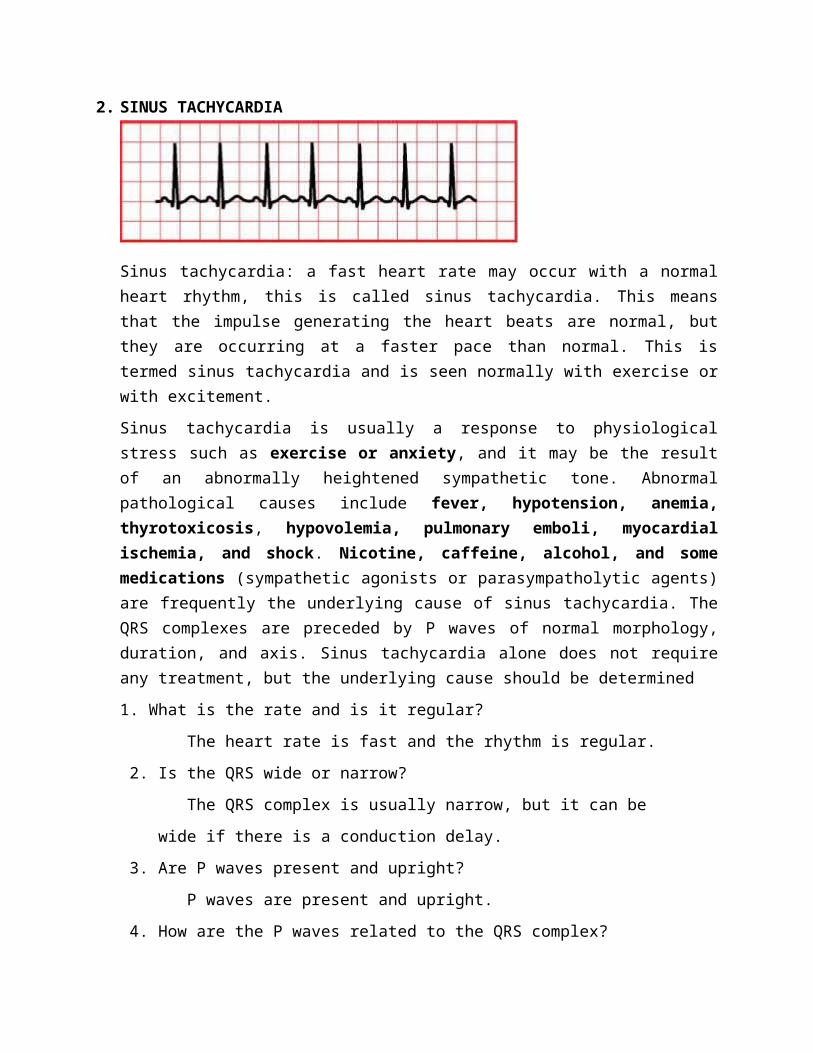
2. SINUS TACHYCARDIA
Sinus tachycardia: a fast heart rate may occur with a normal heart rhythm, this is called sinus tachycardia. This means that the impulse generating the heart beats are normal, but they are occurring at a faster pace than normal. This is termed sinus tachycardia and is seen normally with exercise or with excitement.
Sinus tachycardia is usually a response to physiological stress such as exercise or anxiety, and it may be the result of an abnormally heightened sympathetic tone. Abnormal pathological causes include fever, hypotension, anemia, thyrotoxicosis, hypovolemia, pulmonary emboli, myocardial ischemia, and shock. Nicotine, caffeine, alcohol, and some medications (sympathetic agonists or parasympatholytic agents) are frequently the underlying cause of sinus tachycardia. The QRS complexes are preceded by P waves of normal morphology, duration, and axis. Sinus tachycardia alone does not require any treatment, but the underlying cause should be determined
1. What is the rate and is it regular?
The heart rate is fast and the rhythm is regular.
2. Is the QRS wide or narrow?
The QRS complex is usually narrow, but it can be
wide if there is a conduction delay.
3. Are P waves present and upright?
P waves are present and upright.
4. How are the P waves related to the QRS complex?
There is a fixed, 1-to-1 relationship between the
P waves and QRS complexes.
The impulse in normal sinus rhythm arises in the
SA node and spreads through the atria to the AV node.
The impulse then travels down the conducting system and
spreads through the ventricles. The P wave is followed
by a narrow QRS complex, unless there is aberrant
conduction.
In sinus tachycardia, the heart rate is greater than
100 beats per minute.
Sinus tachycardia can be difficult to distinguish
from atrial tachycardia. Heart rate greater than 150
beats per minute and an abnormal P wave favor atrial
tachycardia. P waves may be superimposed on T waves
or U waves and be difficult to recognize.
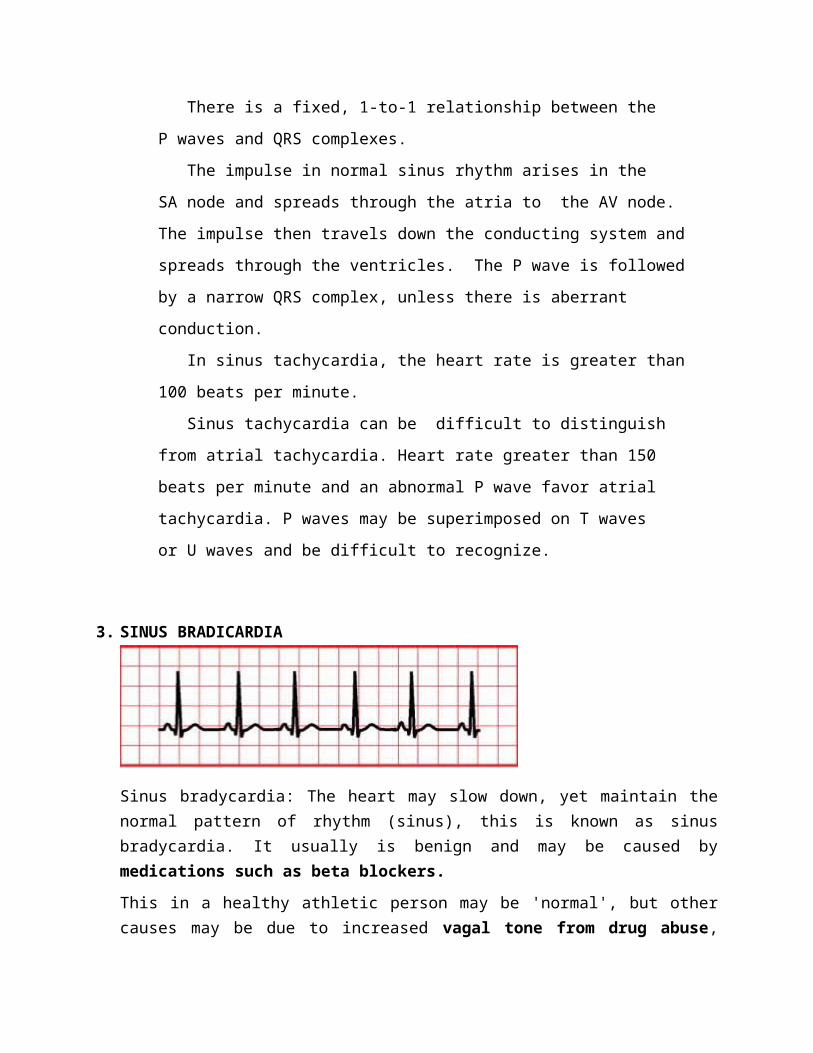
3. SINUS BRADICARDIA
Sinus bradycardia: The heart may slow down, yet maintain the normal pattern of rhythm (sinus), this is known as sinus bradycardia. It usually is benign and may be caused by medications such as beta blockers.
This in a healthy athletic person may be 'normal', but other causes may be due to increased vagal tone from drug abuse, hypoglycaemia and brain injury with increase intracranial pressure (ICP) as examples
1. What is the rate and is it regular?
The heart rate is slow and the rhythm is regular.
2. Is the QRS wide or narrow?
The QRS complex is usually narrow, but it can be
wide if there is a conduction delay.
3. Are P waves present and upright?
P waves are present and upright.
4. How are the P waves related to the QRS complex?
There is a fixed, 1-to-1 relationship between the
P waves and QRS complexes.
The impulse in sinus rhythm arises in the SA node
and spreads through the atria to the AV node. The
impulse then travels down the conducting system and
spreads through the ventricles. The P wave is followed
by a narrow QRS complex, unless there is aberrant
conduction.
In sinus bradycardia, the heart rate is less than
60 beats per minute
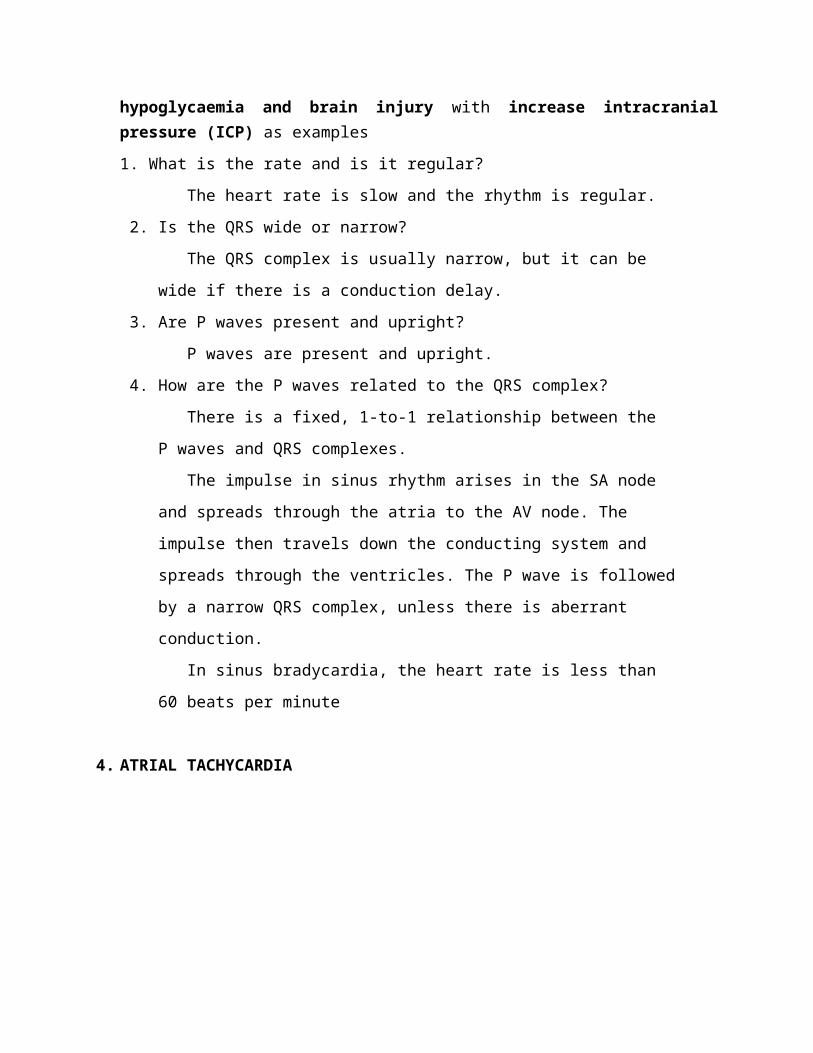
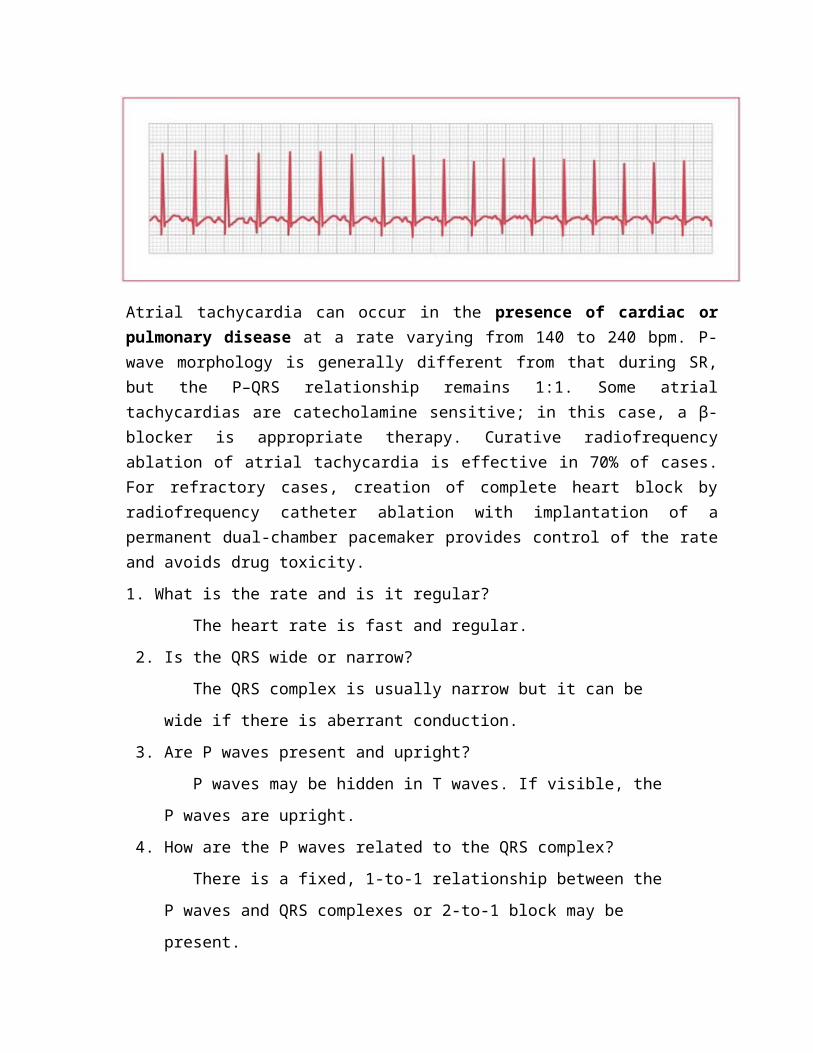
4. ATRIAL TACHYCARDIA
Atrial tachycardia can occur in the presence of cardiac or pulmonary disease at a rate varying from 140 to 240 bpm. P-wave morphology is generally different from that during SR, but the P–QRS relationship remains 1:1. Some atrial tachycardias are catecholamine sensitive; in this case, a β-blocker is appropriate therapy. Curative radiofrequency ablation of atrial tachycardia is effective in 70% of cases. For refractory cases, creation of complete
heart block by radiofrequency catheter ablation with implantation of a permanent dual-chamber pacemaker provides control of the rate and avoids drug toxicity.
1. What is the rate and is it regular?
The heart rate is fast and regular.
2. Is the QRS wide or narrow?
The QRS complex is usually narrow but it can be
wide if there is aberrant conduction.
3. Are P waves present and upright?
P waves may be hidden in T waves. If visible, the
P waves are upright.
4. How are the P waves related to the QRS complex?
There is a fixed, 1-to-1 relationship between the
P waves and QRS complexes or 2-to-1 block may be
present.
The impulse in atrial tachycardia arises in the
atria and spreads to the AV node. The impulse travels
down the conducting system and spreads through the
ventricles resulting in a narrow QRS complex. If
aberrant conduction is present, the QRS will be wide.
The heart rate in atrial tachycardia is 150 to 250
beats per minute. A QRS follows every P wave or 2-to-1
block may occur. The P wave may be superimposed on the
T wave and be difficult to identify.
Atrial tachycardia can be difficult to distinguish
from sinus tachycardia. Heart rate greater than 150
beats per minute and an abnormal P wave favor atrial
tachycardia.
It can be difficult to distinguish ventricular
tachycardia from supraventricular tachycardia with
aberrant conduction. The presence of P waves or
irregularity in rate favor supraventricular
tachycardia. When in doubt assume the rhythm is
ventricular tachycardia.
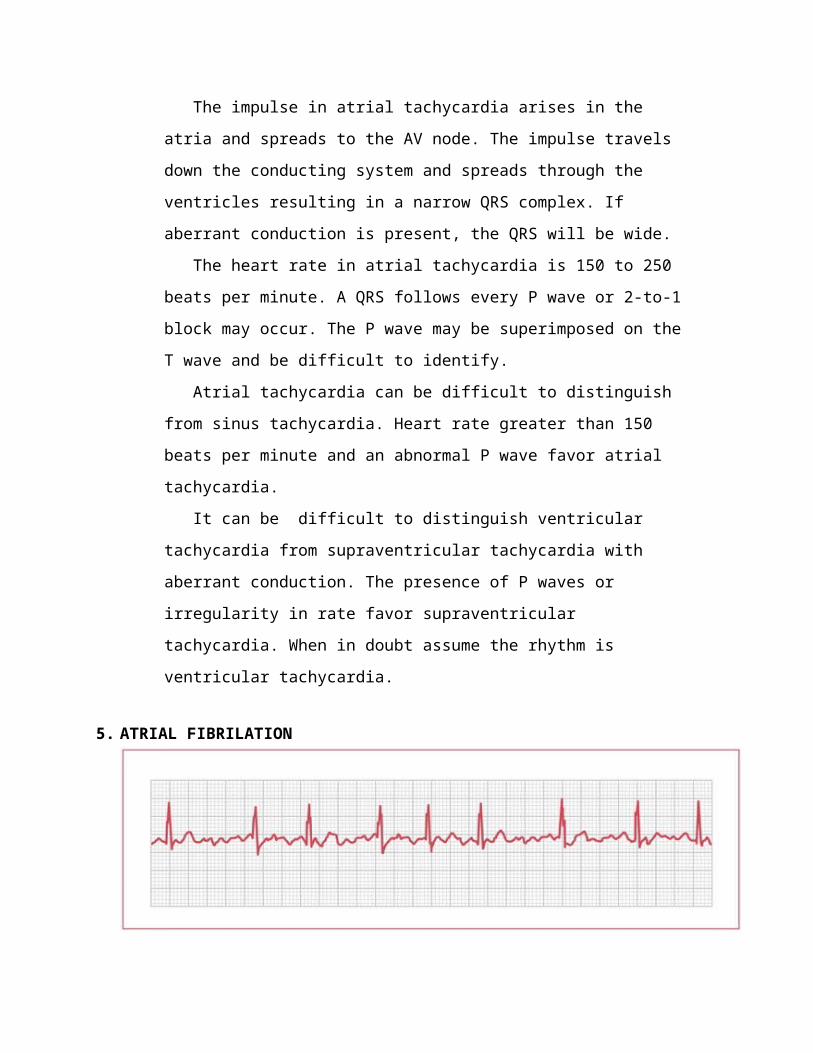
5. ATRIAL FIBRILATION
The clinical manifestations of AF range from a complete absence of symptoms (usually in the young and fit) to hemodynamic collapse (in the elderly or those with systolic dysfunction). In addition to symptoms of palpitations, patients with AF have an increased risk of stroke and may also develop decreased exercise tolerance and LV dysfunction. The incidence of AF increases with age and its development is concentrated in patients with hypertensive heart disease, congestive heart failure, and rheumatic heart disease; the association with coronary artery disease is not as strong as with these other conditions. Among the noncardiac causes of AF, the association is strongest with hyperthyroidism, electrolyte abnormalities, and alcohol excess.
1. What is the rate and is it regular?
The heart rate is variable with an irregularly irregular
rhythm.
2. Is the QRS wide or narrow?
The QRS complex is narrow.
3. Are P waves present and upright?
P waves are not present, but fibrillatory waves may be
present.
4. How are the P waves related to the QRS complex?
There is no relationship between the P waves and
QRS complexes.
Atrial fibrillation is chaotic. The atrial muscle is
depolarizing very rapidly in a disorganized fashion. There
are no P waves since each depolarization involves little
muscle mass, but oscillations can sometimes be seen in the
baseline. Impulses are irregularly conducted to the AV node
which conducts depending on its refractory state. The
resulting QRS complexes are narrow with irregular R-R
intervals.
The rhythm is atrial fibrillation if there are no
P waves and the QRS's are irregularly irregular.
If there is abnormal conduction with wide QRS
complexes and a rapid ventricular rate, atrial
fibrillation can look like ventricular tachycardia. The
irregular rhythm is the key to diagnosis of atrial
fibrillation with abnormal conduction.
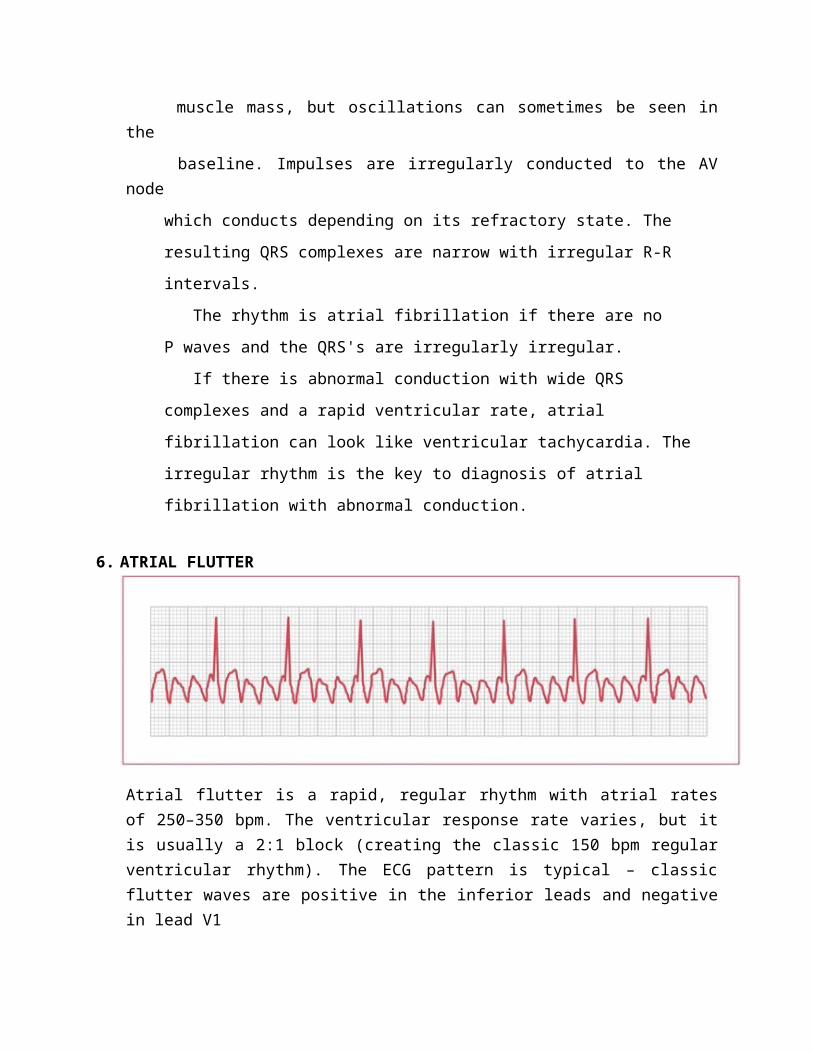
6. ATRIAL FLUTTER
Atrial flutter is a rapid, regular rhythm with atrial rates of 250–350 bpm. The ventricular response rate varies, but it is usually a 2:1 block (creating the classic 150 bpm regular ventricular rhythm). The ECG pattern is typical – classic flutter waves are positive in the inferior leads and negative in lead V1
1. What is the rate and is it regular?
The heart rate is fast and the rhythm is usually
regular.
2. Is the QRS wide or narrow?
The QRS complex is narrow.
3. Are P waves present and upright?
The P waves are the sum of a positive and negative
component and have a sawtooth appearance.
4. How are the P waves related to the QRS complex?
Frequently there are more flutter waves than QRS
complexes so some degree of AV block can be present.
The impulse in atrial flutter travels around the atrium
in a circular fashion. The atrial activity is regular,
usually with a rate between 240 and 360 per minute. The
QRS complexes may not be regular since variable AV block
is often present.
The most common presentation of atrial flutter is an
atrial rate of 300 with 2:1 block.
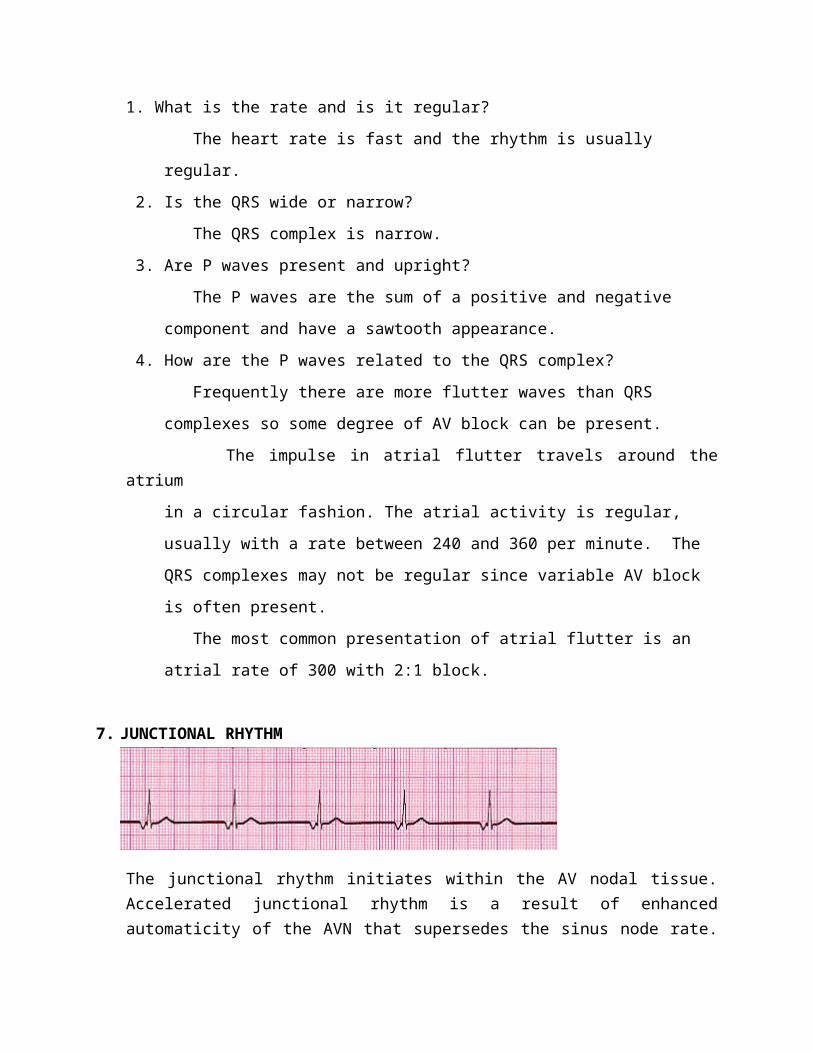
7. JUNCTIONAL RHYTHM
The junctional rhythm initiates within the AV nodal tissue. Accelerated junctional rhythm is a result of enhanced automaticity of the AVN that supersedes the sinus node rate. During this rhythm, the AVN is firing faster than the sinus node, resulting in a regular narrow complex rhythm. These rhythms may demonstrate retrograde P waves on ECG findings, and the rates can vary from 40-60 beats per minute.
Changes in autonomic tone or the presence of sinus node disease that is causing an inappropriate slowing of the sinus node may exacerbate this rhythm. Young healthy individuals, especially those with increased vagal tone during sleep, are often noted to have periods of junctional rhythm that is completely benign, not requiring any intervention.
Rarely, the AVN develops enhanced automaticity and overtakes a "normal" sinus node. This occasionally is observed in digitalis toxicity, following cardiac surgery (typically valve replacement), during acute myocardial infarction, or during isoproterenol infusion.
Junctional bradycardia due to profound sinus node dysfunction. No atrial activity is apparent
junctional tachycardias are most often observed in the setting of digitalis toxicity, recent cardiac surgery, acute myocardial infarction, or isoproterenol infusion.
1. What is the rate and is it regular?
The heart rate is normal and the rhythm is regular.
2. Is the QRS wide or narrow?
The QRS complex is narrow.
3. Are P waves present and upright?
P waves are absent or negative.
4. How are the P waves related to the QRS complex?
In high junctional rhythm inverted P waves come before
the QRS, in mid-junctional rhythm there are no P waves,
and in low junctional rhythm an inverted P wave follows
the QRS.
In junctional rhythms the impulse arises in or near the
AV node. The rhythm is regular. If the impulse arises high
in the junction, an inverted P wave precedes the QRS. The
P wave is inverted since the impulse is conducted retro-
grade through the atria.
If the impulse arises in the middle of the junction, the
P wave is not present. It is either buried in the QRS or
the impulse was not conducted to the atria.
If the impulse arises low in the junction, the impulse
takes a long time to pass through the node and retrograde
through the atria. The P wave is inverted and follows the
QRS complex.
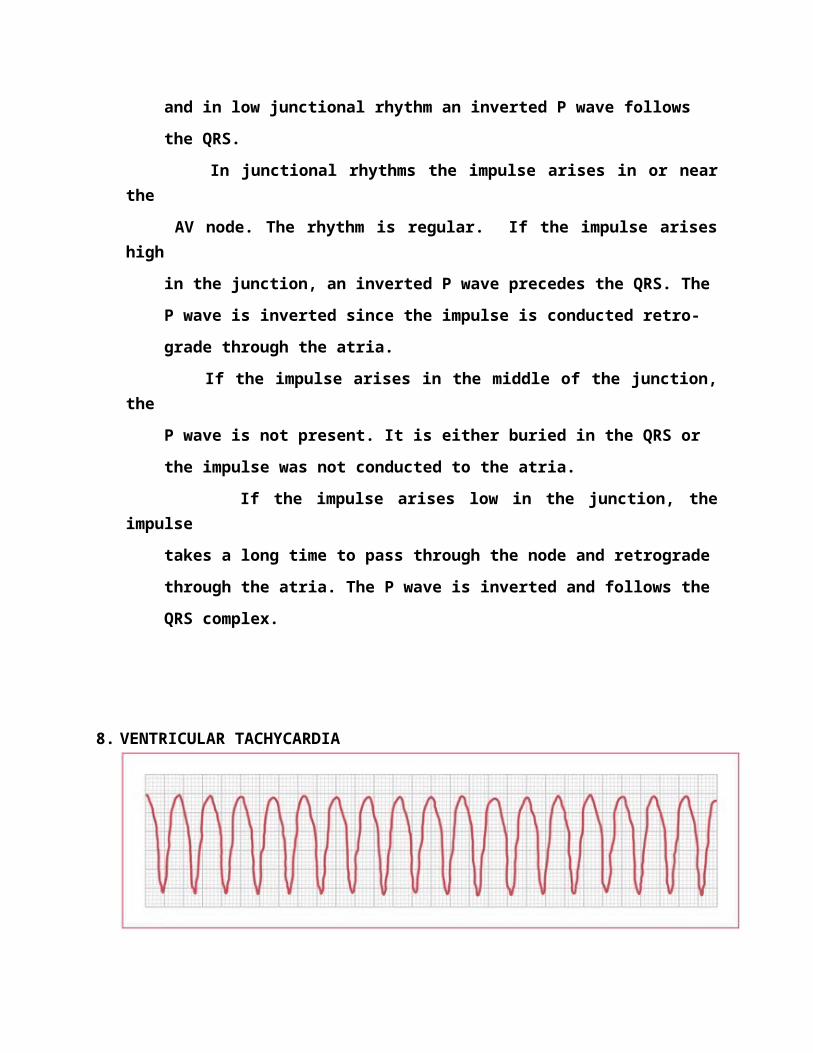
8. VENTRICULAR TACHYCARDIA
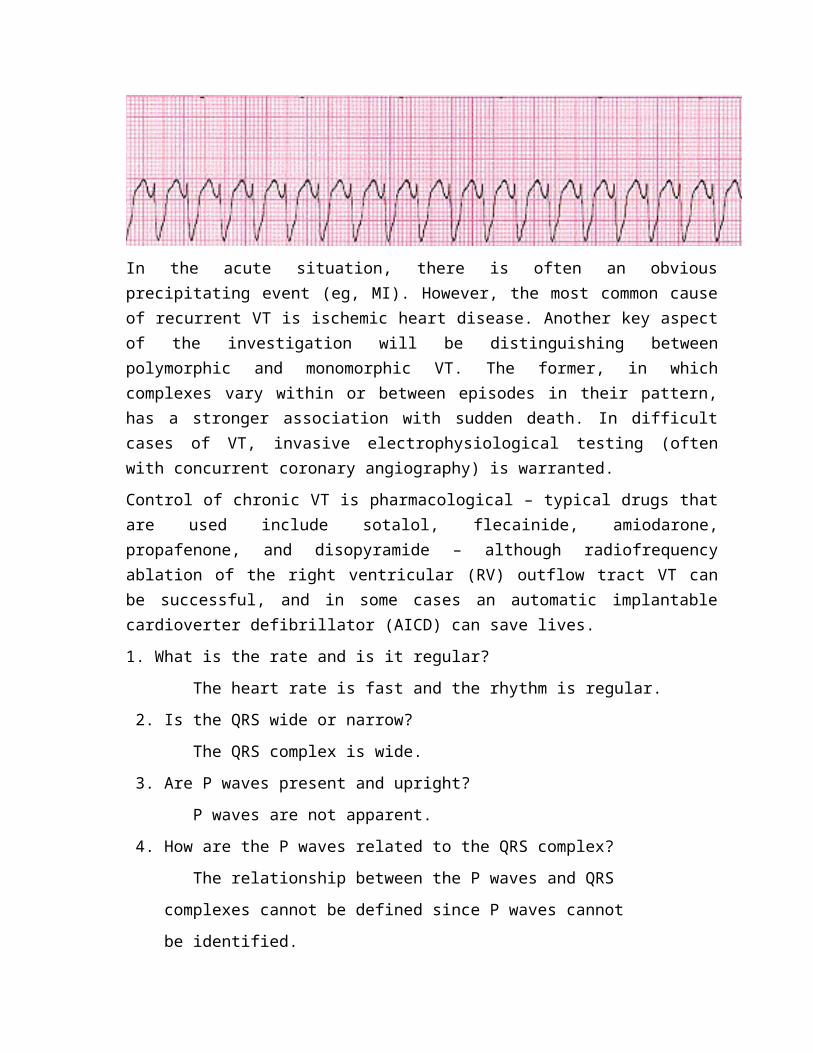
In the acute situation, there is often an obvious precipitating event (eg, MI). However, the most common cause of recurrent VT is ischemic heart disease. Another key aspect of the investigation will be distinguishing between polymorphic and monomorphic VT. The former, in which complexes vary within or between episodes in their pattern, has a stronger association with sudden death. In difficult cases of VT, invasive electrophysiological testing (often with concurrent coronary angiography) is warranted.
Control of chronic VT is pharmacological – typical drugs that are used include sotalol, flecainide, amiodarone, propafenone, and disopyramide – although radiofrequency ablation of the right ventricular (RV) outflow tract VT can be successful, and in some cases an automatic implantable cardioverter defibrillator (AICD) can save lives.
1. What is the rate and is it regular?
The heart rate is fast and the rhythm is regular.
2. Is the QRS wide or narrow?
The QRS complex is wide.
3. Are P waves present and upright?
P waves are not apparent.
4. How are the P waves related to the QRS complex?
The relationship between the P waves and QRS
complexes cannot be defined since P waves cannot
be identified.
Ventricular tachycardia is present with three or more
beats of ventricular origin in a row. Ventricular
tachycardia is usually regular but it can be irregular.
The QRS complexes are wide. P waves are sometimes
identifiable but they bear no relationship to the
QRS complexes.
It can be difficult to distinguish ventricular
tachycardia from supraventricular tachycardia with
aberrant conduction. When in doubt assume the rhythm
is ventricular tachycardia.
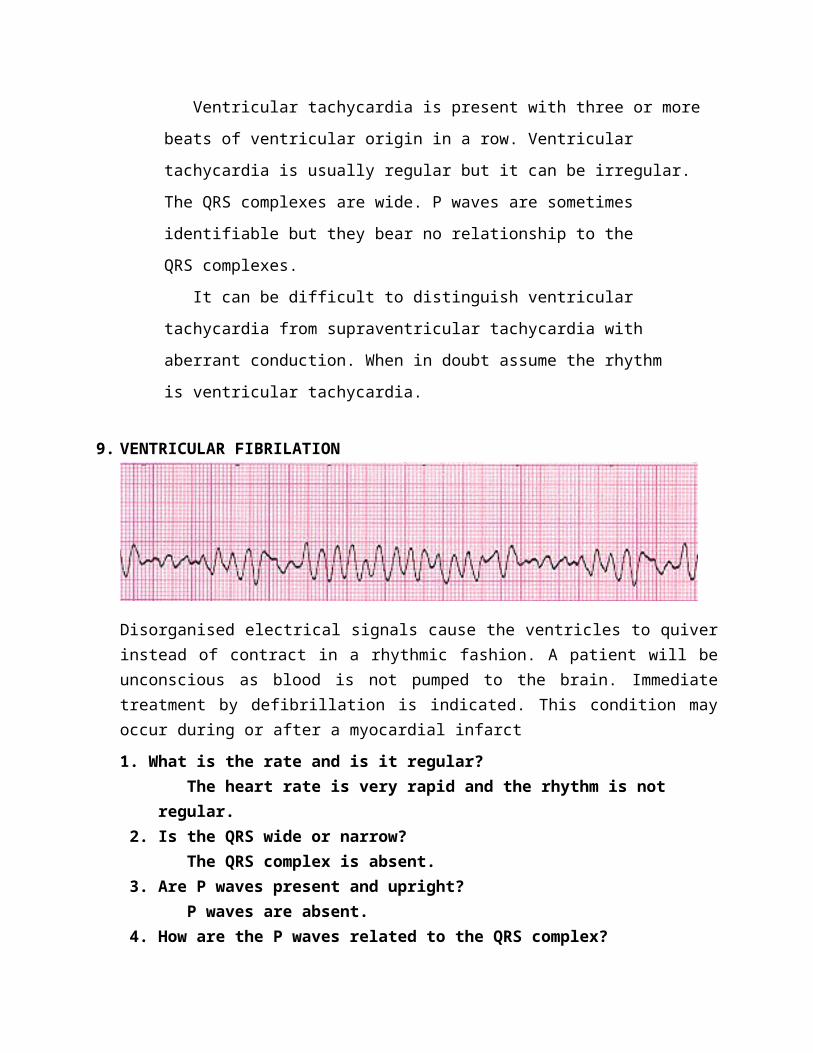
9. VENTRICULAR FIBRILATION
Disorganised electrical signals cause the ventricles to quiver instead of contract in a rhythmic fashion. A patient will be unconscious as blood is not pumped to the brain. Immediate treatment by defibrillation is indicated. This condition may occur during or after a myocardial infarct
1. What is the rate and is it regular? The heart rate is very rapid and the rhythm is not regular. 2. Is the QRS wide or narrow? The QRS complex is absent. 3. Are P waves present and upright? P waves are absent. 4. How are the P waves related to the QRS complex? There are no P waves or QRS complexes so there is no relationship between them. In ventricular fibrillation areas of the ventricles are depolarizing and repolarizing in a completely disorganized fashion. All pumping function of the ventricles is lost.
The electrocardiogram may show voltage fluctuations. The amplitude of these waves is described by the terms "coarse" and "fine"
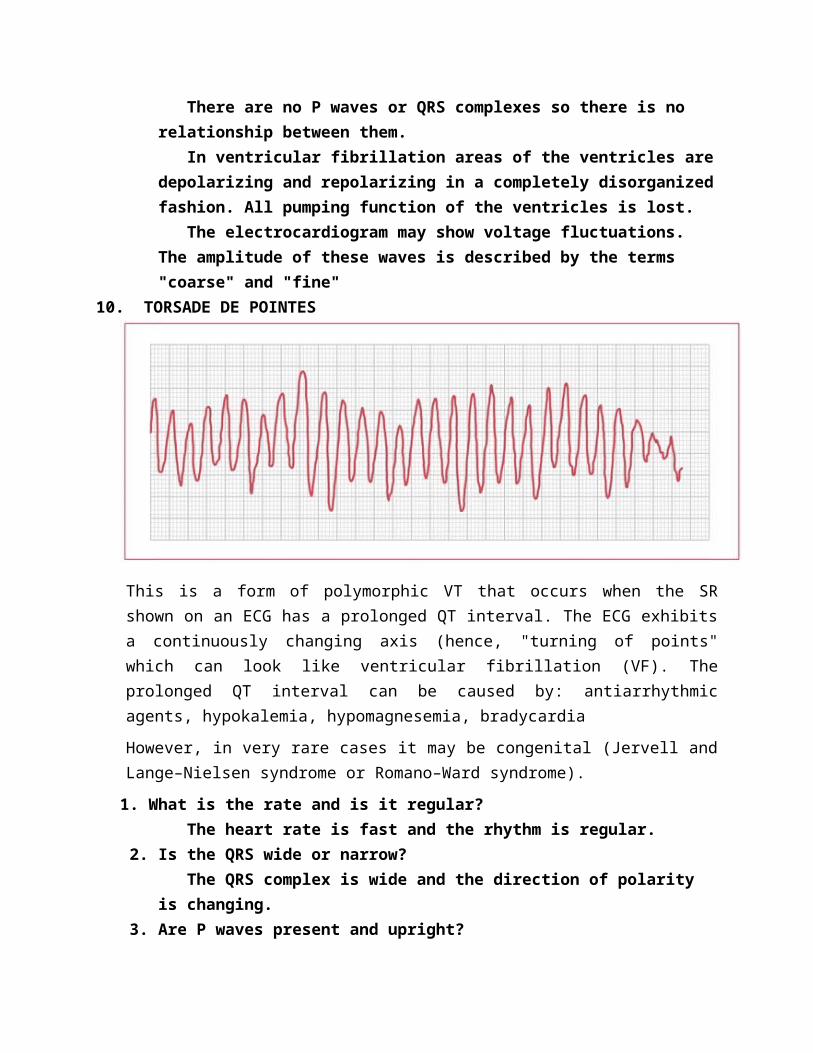
10. TORSADE DE POINTES
This is a form of polymorphic VT that occurs when the SR shown on an ECG has a prolonged QT interval. The ECG exhibits a continuously changing axis (hence, "turning of points" which can look like ventricular fibrillation (VF). The prolonged QT interval can be caused by: antiarrhythmic agents, hypokalemia, hypomagnesemia, bradycardia
However, in very rare cases it may be congenital (Jervell and Lange–Nielsen syndrome or Romano–Ward syndrome).
1. What is the rate and is it regular? The heart rate is fast and the rhythm is regular. 2. Is the QRS wide or narrow? The QRS complex is wide and the direction of polarity is changing. 3. Are P waves present and upright? P waves are not apparent. 4. How are the P waves related to the QRS complex? The relationship between the P waves and QRS complexes is not defined since the P waves are not identifiable. Torsades de Pointes is a variant form of ventricular tachycardia in which the polarity periodically changes from positive to negative. The name means twisting of the points. The rhythm is usually regular but it can be irregular. The QRS complexes are wide. P waves are sometimes
identifiable but they bear no relationship to the QRS complexes. It is important to distinguish Torsade de Pointes from ventricular tachycardia since the treatment is different. Torsades de Pointes is associated with a long QT interval. Agents such as quinidine and procainamide can prolong the QT interval and worsen the arrhythmia. Overdrive pacing and magnesium are the treatments of choice for Torsade de Pointes.
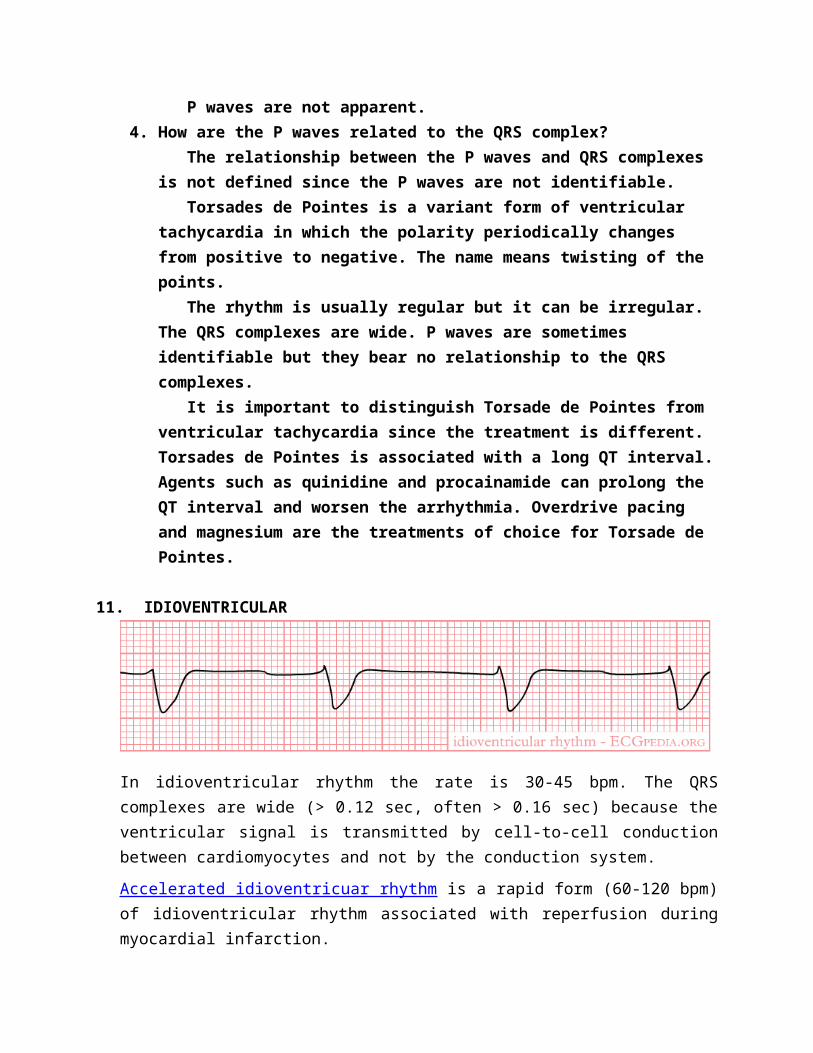
11. IDIOVENTRICULAR
In idioventricular rhythm the rate is 30-45 bpm. The QRS complexes are wide (> 0.12 sec, often > 0.16 sec) because the ventricular signal is transmitted by cell-to-cell conduction between cardiomyocytes and not by the conduction system.
Accelerated idioventricuar rhythm is a rapid form (60-120 bpm) of idioventricular rhythm associated with reperfusion during myocardial infarction.
1. What is the rate and is it regular? The heart rate is slow and the rhythm is regular. 2. Is the QRS wide or narrow? The QRS complex is wide. 3. Are P waves present and upright? P waves are not apparent. 4. How are the P waves related to the QRS complex? The relationship between the P waves and QRS complexes cannot be defined since P waves cannot be identified. Accelerated idioventricular rhythm arises from the regular firing of a ventricular site. The rate is typically 40 to 99 beats per minute with wide and bizarre complexes.
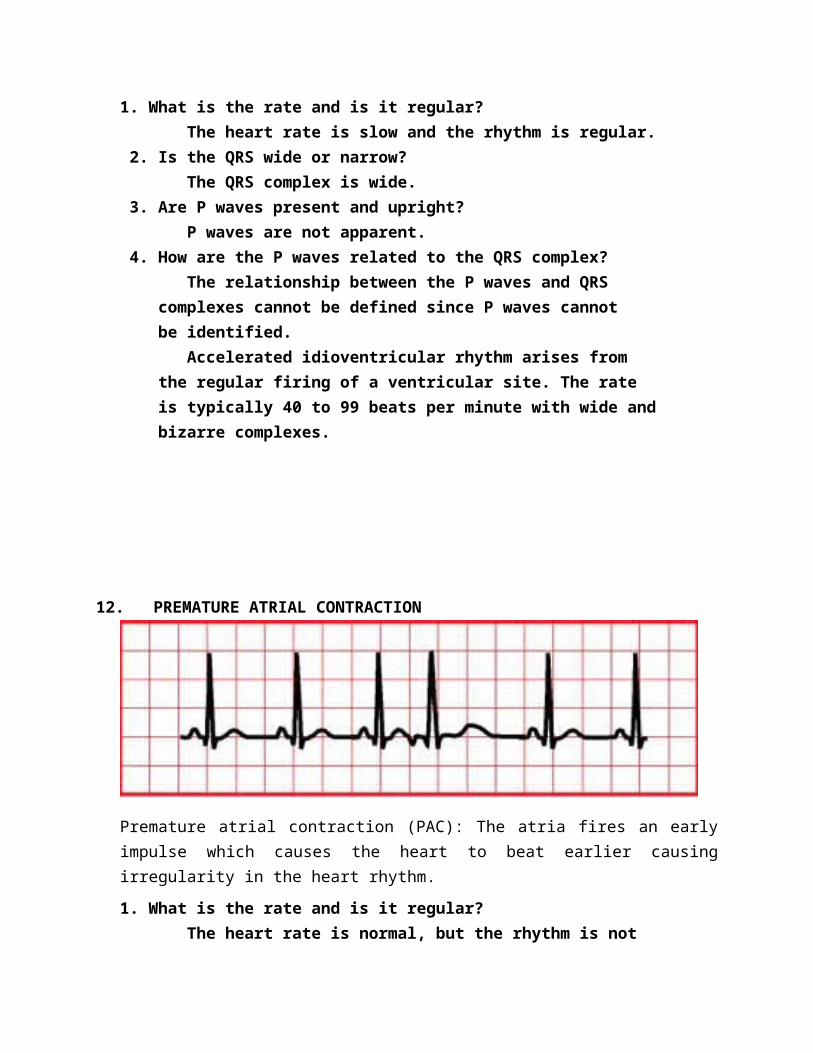
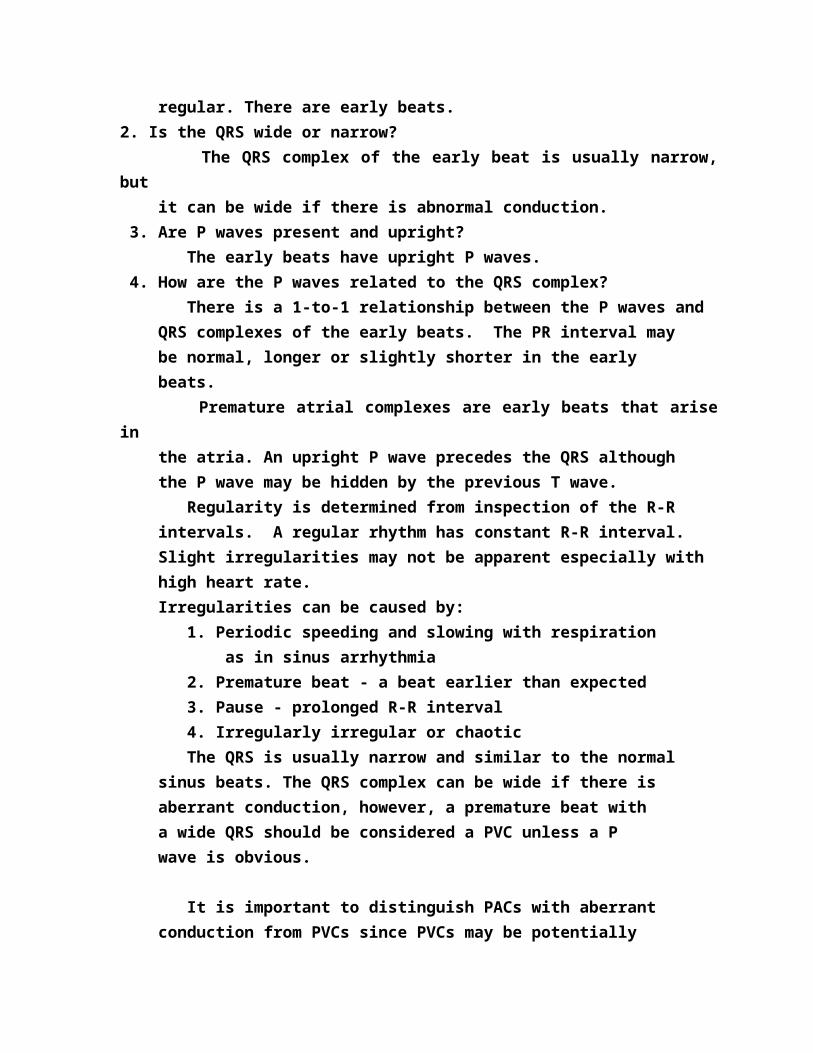
12. PREMATURE ATRIAL CONTRACTION
Premature atrial contraction (PAC): The atria fires an early impulse which causes the heart to beat earlier causing irregularity in the heart rhythm.
1. What is the rate and is it regular? The heart rate is normal, but the rhythm is not regular. There are early beats.2. Is the QRS wide or narrow? The QRS complex of the early beat is usually narrow, but it can be wide if there is abnormal conduction. 3. Are P waves present and upright? The early beats have upright P waves. 4. How are the P waves related to the QRS complex? There is a 1-to-1 relationship between the P waves and QRS complexes of the early beats. The PR interval may be normal, longer or slightly shorter in the early beats. Premature atrial complexes are early beats that arise in the atria. An upright P wave precedes the QRS although the P wave may be hidden by the previous T wave. Regularity is determined from inspection of the R-R intervals. A regular rhythm has constant R-R interval. Slight irregularities may not be apparent especially with high heart rate. Irregularities can be caused by:
1. Periodic speeding and slowing with respiration as in sinus arrhythmia 2. Premature beat - a beat earlier than expected 3. Pause - prolonged R-R interval 4. Irregularly irregular or chaotic The QRS is usually narrow and similar to the normal sinus beats. The QRS complex can be wide if there is aberrant conduction, however, a premature beat with a wide QRS should be considered a PVC unless a P wave is obvious.
It is important to distinguish PACs with aberrant conduction from PVCs since PVCs may be potentially dangerous and supraventricular beats are usually benign. When in doubt assume the beat is a premature ventricular contraction.
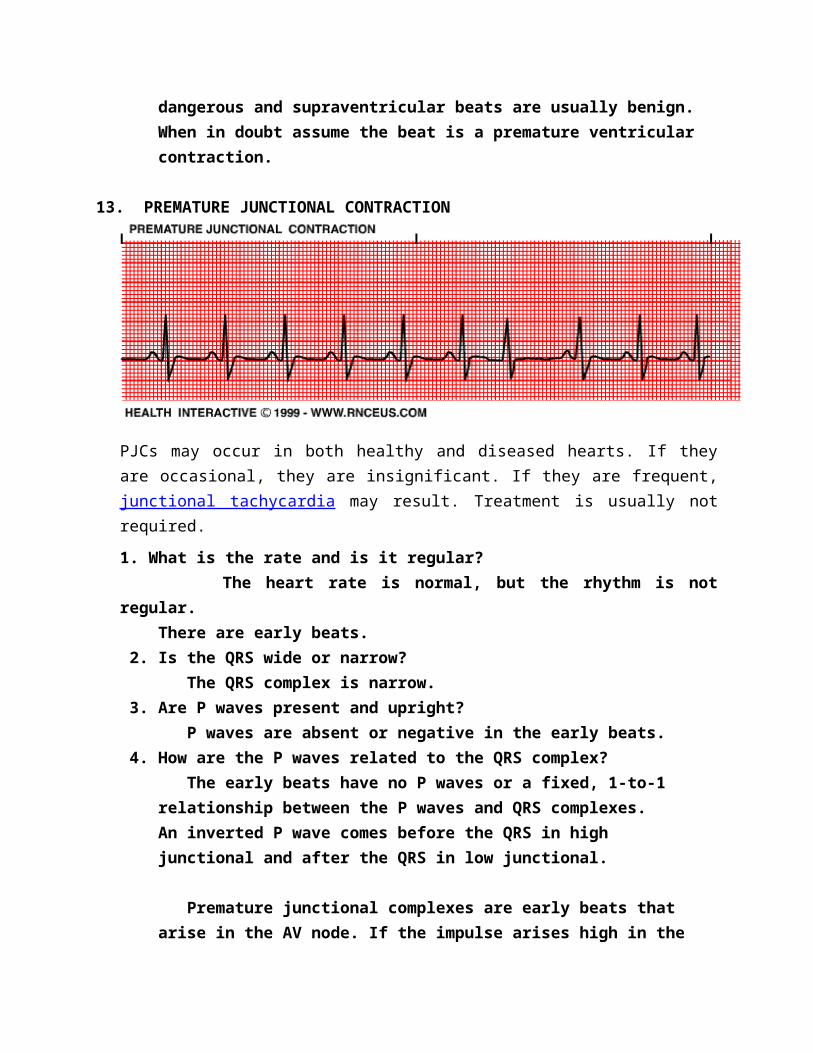
13. PREMATURE JUNCTIONAL CONTRACTION
PJCs may occur in both healthy and diseased hearts. If they are occasional, they are insignificant. If they are frequent, junctional tachycardia may result. Treatment is usually not required.
1. What is the rate and is it regular? The heart rate is normal, but the rhythm is not regular. There are early beats. 2. Is the QRS wide or narrow? The QRS complex is narrow. 3. Are P waves present and upright? P waves are absent or negative in the early beats.
4. How are the P waves related to the QRS complex? The early beats have no P waves or a fixed, 1-to-1 relationship between the P waves and QRS complexes. An inverted P wave comes before the QRS in high junctional and after the QRS in low junctional.
Premature junctional complexes are early beats that arise in the AV node. If the impulse arises high in the junction, an inverted P wave precedes the QRS. The P wave is inverted since the impulse is conducted retrograde through the atria. If the impulse arises in the middle of the junction, the P wave is not present. It is either buried in the QRS or the impulse was not conducted to the atria. If the impulse arises low in the junction, the impulse takes a long time to pass through the node and retrograde through the atria. The P wave is inverted and follows the QRS complex.
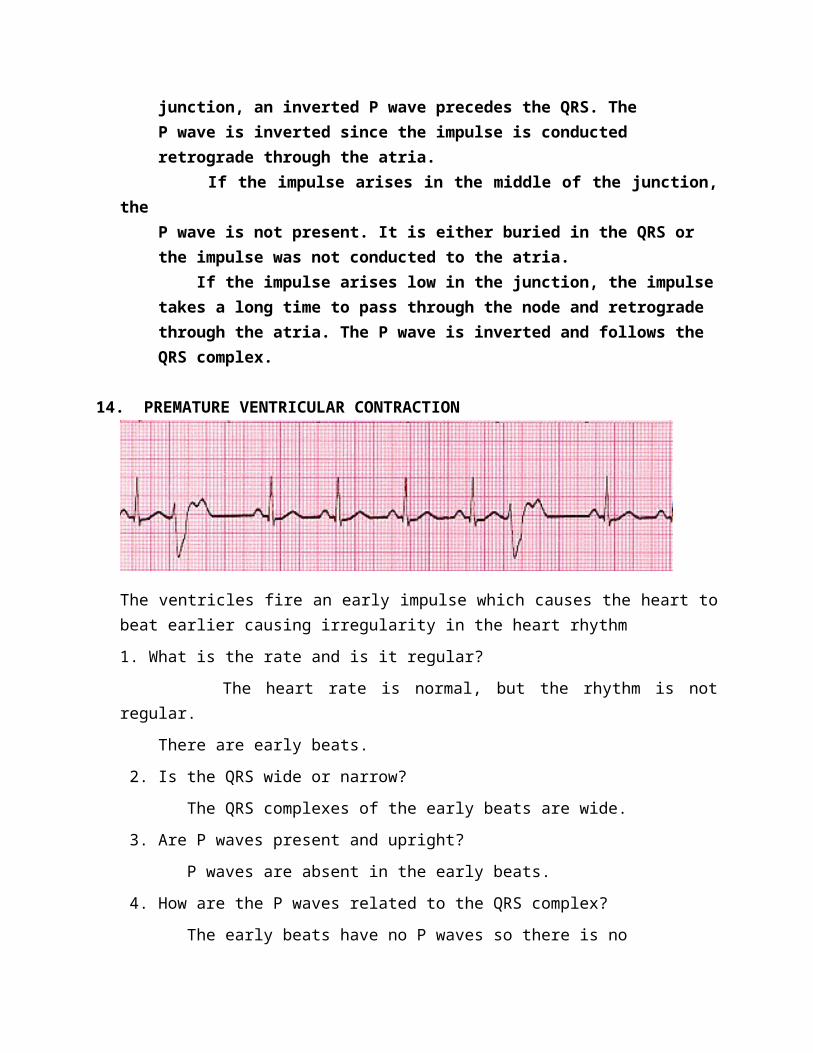
14. PREMATURE VENTRICULAR CONTRACTION
The ventricles fire an early impulse which causes the heart to beat earlier causing irregularity in the heart rhythm
1. What is the rate and is it regular?
The heart rate is normal, but the rhythm is not regular.
There are early beats.
2. Is the QRS wide or narrow?
The QRS complexes of the early beats are wide.
3. Are P waves present and upright?
P waves are absent in the early beats.
4. How are the P waves related to the QRS complex?
The early beats have no P waves so there is no
relationship to the QRS.
Premature ventricular complexes are early beats that
arise in the ventricle. They are conducted through the
ventricle and have a wide, often bizarre QRS complex.
It is important to distinguish PVCs from supra-
ventricular beats with aberrant conduction since PVCs
may be potentially dangerous and supraventricular beats
are usually benign. When in doubt assume the beat is a
premature ventricular contraction.
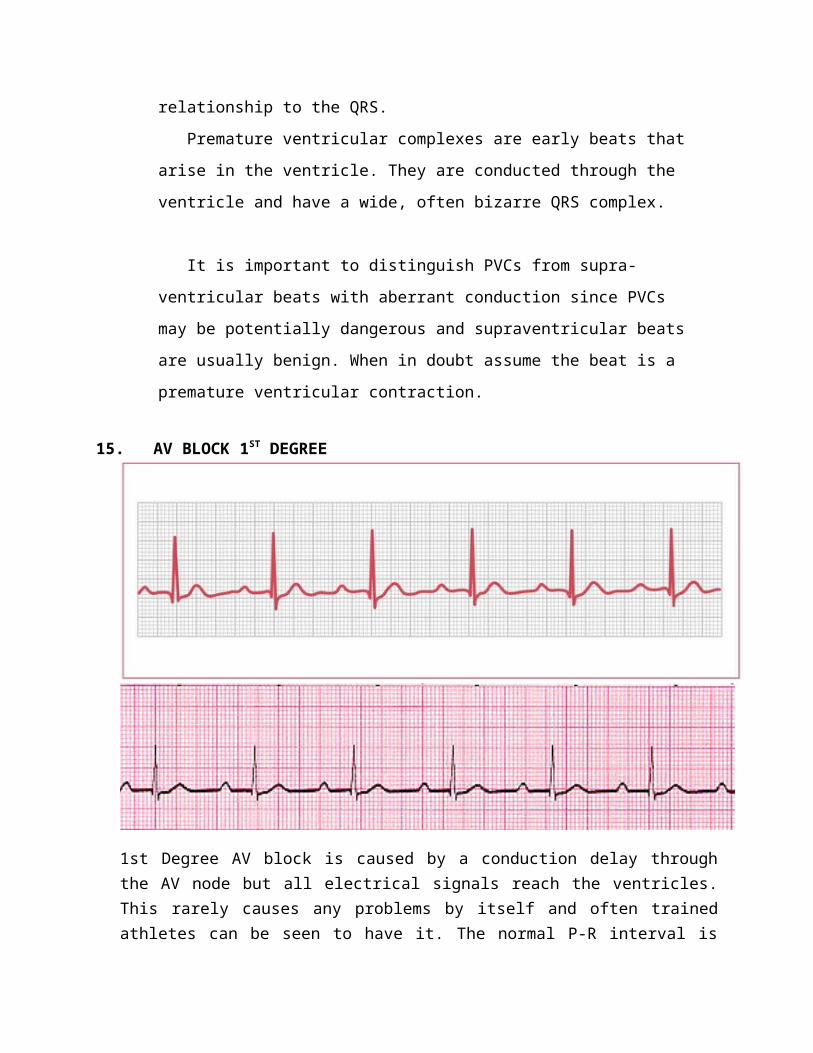
15. AV BLOCK 1ST DEGREE
1st Degree AV block is caused by a conduction delay through the AV node but all electrical signals reach the ventricles. This rarely causes any problems by itself and often trained athletes can be seen to have it. The normal P-R interval is between 0.12s to 0.20s in length, or 3-5 small squares on the ECG.
This is where there is a prolonged PR interval of >200 milliseconds (5 small squares; see No specific therapy is required and the prognosis is excellent. However, it can be a marker for an underlying problem such as myocarditis, MI, degenerative disease, or, most commonly, a drug effect (eg, tricyclic antidepressants).
1. What is the rate and is it regular?
The heart rate is slow to normal and the rhythm is
regular.
2. Is the QRS wide or narrow?
The QRS complex is narrow.
3. Are P waves present and upright?
The P waves are upright.
4. How are the P waves related to the QRS complex?
There is a fixed, 1-to-1 relationship between the P
waves and QRS complexes, but the PR interval is
prolonged.
Every P wave causes a QRS complex in first degree AV
block. The PR interval is fixed, but it is greater than
0.2 seconds.
16. AV BLOCK 2ND DEGREE TYPE 1
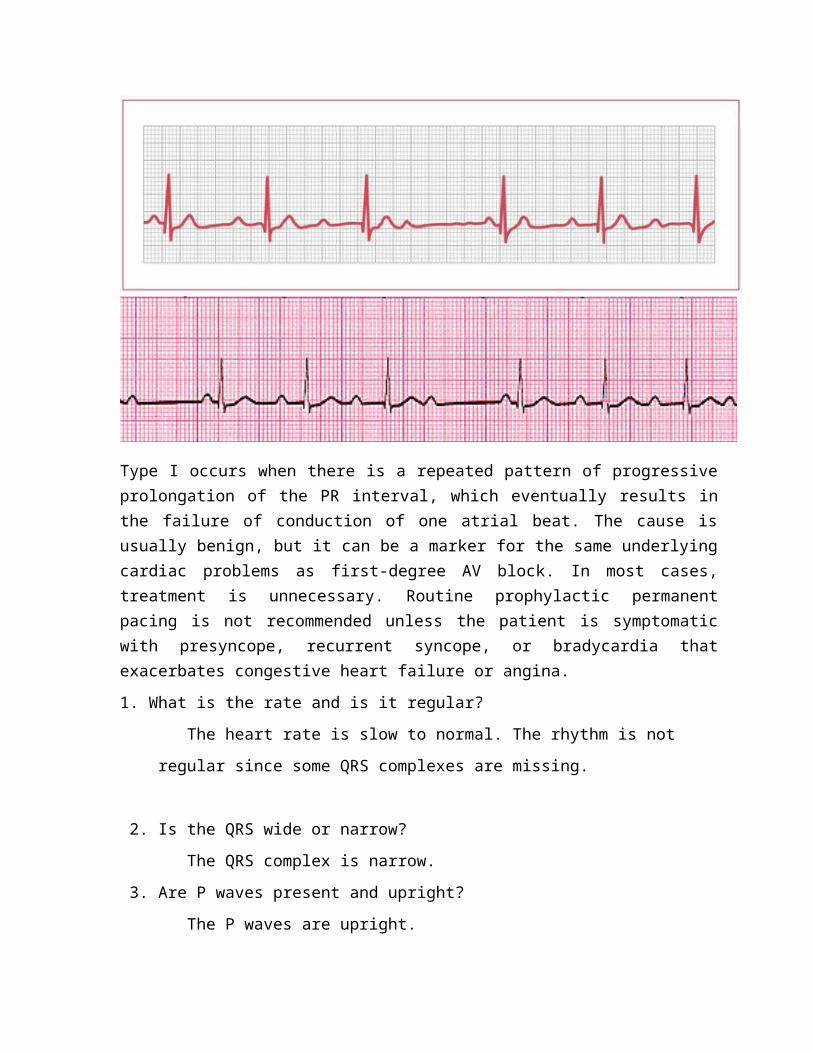
Type I occurs when there is a repeated pattern of progressive prolongation of the PR interval, which eventually results in the failure of conduction of one atrial beat. The cause is usually benign, but it can be a marker for the same underlying cardiac problems as first-degree AV block. In most cases, treatment is unnecessary. Routine prophylactic permanent pacing is not recommended unless the patient is symptomatic with presyncope, recurrent syncope, or bradycardia that exacerbates congestive heart failure or angina.
1. What is the rate and is it regular?
The heart rate is slow to normal. The rhythm is not
regular since some QRS complexes are missing.
2. Is the QRS wide or narrow?
The QRS complex is narrow.
3. Are P waves present and upright?
The P waves are upright.
4. How are the P waves related to the QRS complex?
There are more P waves than QRS complexes. The PR
interval progressively lengthens until a QRS complex
is dropped. The shortest PR interval follows the
dropped beat.
Second degree type I AV block is also known as Mobitz
Type I or Wenkebach. The conduction block occurs in the
AV node. The PR interval progressively lengthens until the
impulse is not conducted to the ventricles.
Second degree type I AV block is most commonly
associated with right coronary artery occlusion with
inferior wall infarctions. This block generally has a
good prognosis.
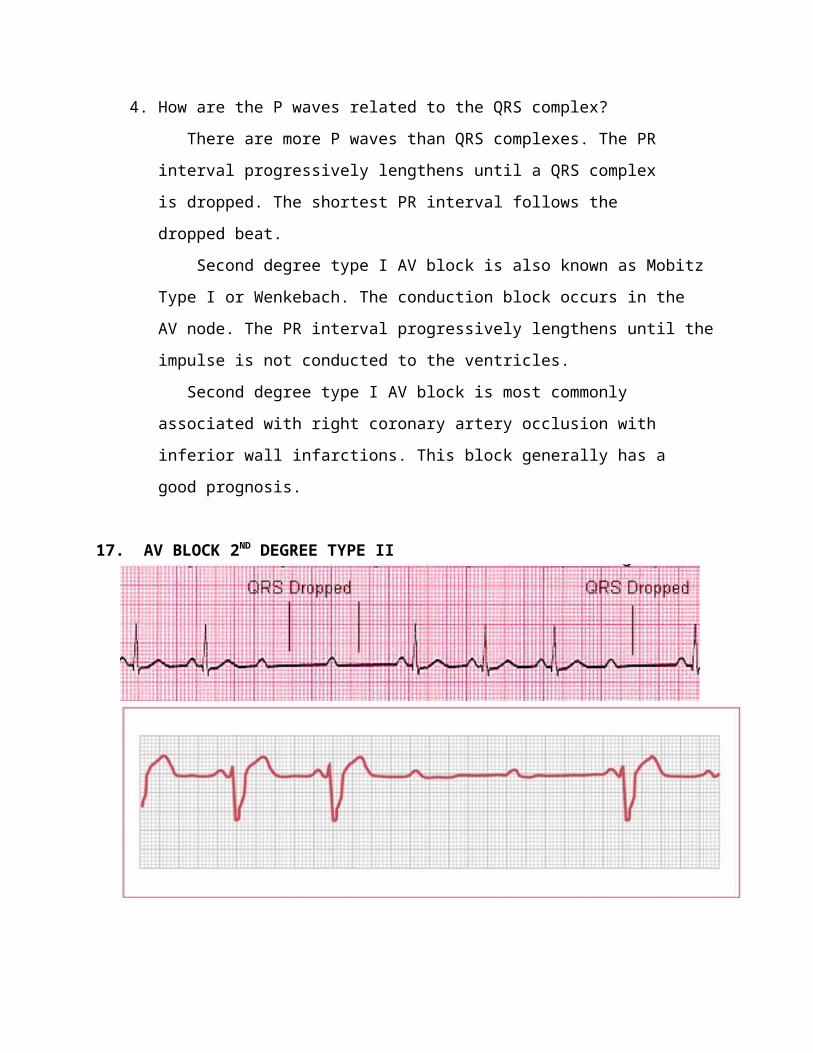
17. AV BLOCK 2ND DEGREE TYPE II
In type II, most beats are conducted with a constant PR interval, but occasionally atrial depolarization is not followed by ventricular depolarization Type II is pathological and indicates disease of the conduction system distal to the AV node. It can frequently lead to complete AV block, causing Stokes–Adams attacks. Therefore, temporary and then permanent pacing (DDD) is indicated in most patients, even those who initially present without symptoms.
1. What is the rate and is it regular?
The heart rate is slow to normal and the rhythm is not
regular. QRS complexes are missing.
2. Is the QRS wide or narrow?
The QRS complex is usually wide.
3. Are P waves present and upright?
The P waves are upright.
4. How are the P waves related to the QRS complex?
There are more P waves than QRS complexes. The PR
interval is fixed and usually has normal duration.
Second degree type II AV block is also known as Mobitz
Type II. The conduction block is infranodal. The PR
interval is fixed duration until the impulse is not
conducted to the ventricles.
Second degree type II AV block is most commonly
associated with anterior wall infarctions. This block
has a propensity to progress to third degree AV block.
18. AV BLOCK 3RD DEGREE
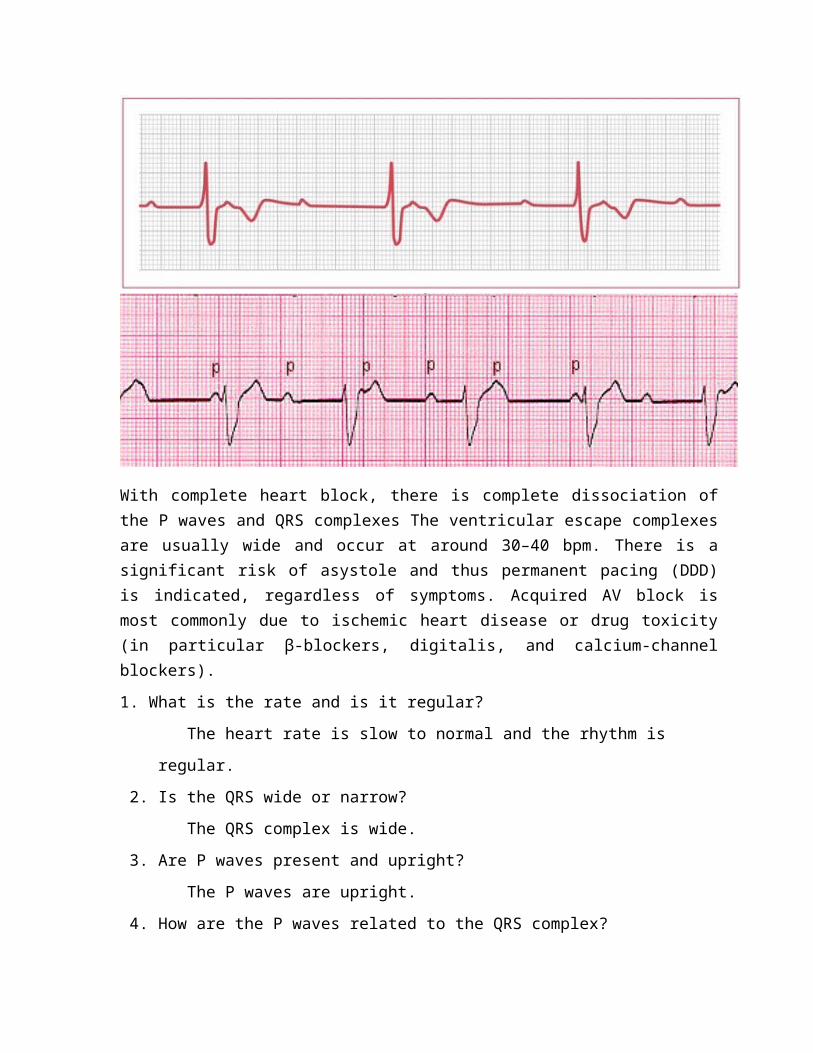
With complete heart block, there is complete dissociation of the P waves and QRS complexes The ventricular escape complexes are usually wide and occur at around 30–40 bpm. There is a significant risk of asystole and thus permanent pacing (DDD) is indicated, regardless of symptoms. Acquired AV block is most commonly due to ischemic heart disease or drug toxicity (in particular β-blockers, digitalis, and calcium-channel blockers).
1. What is the rate and is it regular?
The heart rate is slow to normal and the rhythm is
regular.
2. Is the QRS wide or narrow?
The QRS complex is wide.
3. Are P waves present and upright?
The P waves are upright.
4. How are the P waves related to the QRS complex?
There are usually more P waves than QRS complexes.
There is usually atrial and ventricular regularity,
but they are independent of each other. P waves march
through QRS complexes.
Third degree AV block is complete heart block. The
atria beat at their rate while the ventricular rate is
determined by a junctional or ventricular pacemaker.
P waves "march through" or are unrelated to QRS
complexes.
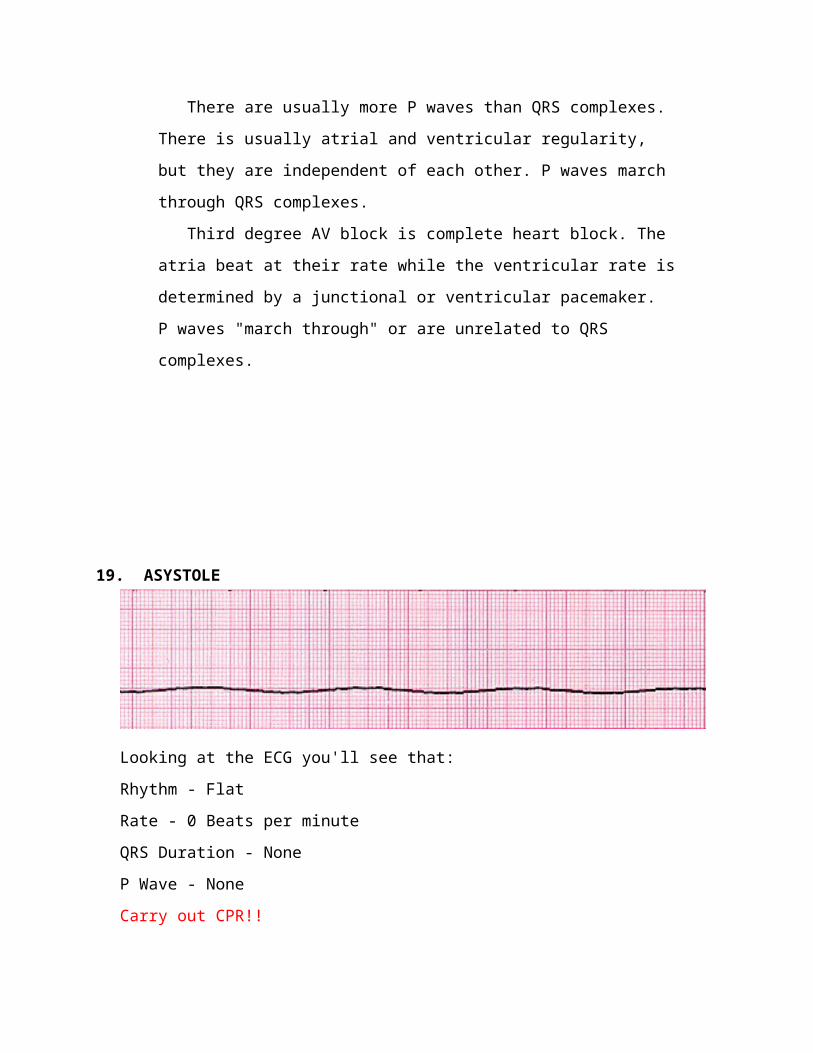
19. ASYSTOLE
Looking at the ECG you'll see that:
Rhythm - Flat
Rate - 0 Beats per minute
QRS Duration - None
P Wave - None
Carry out CPR!!
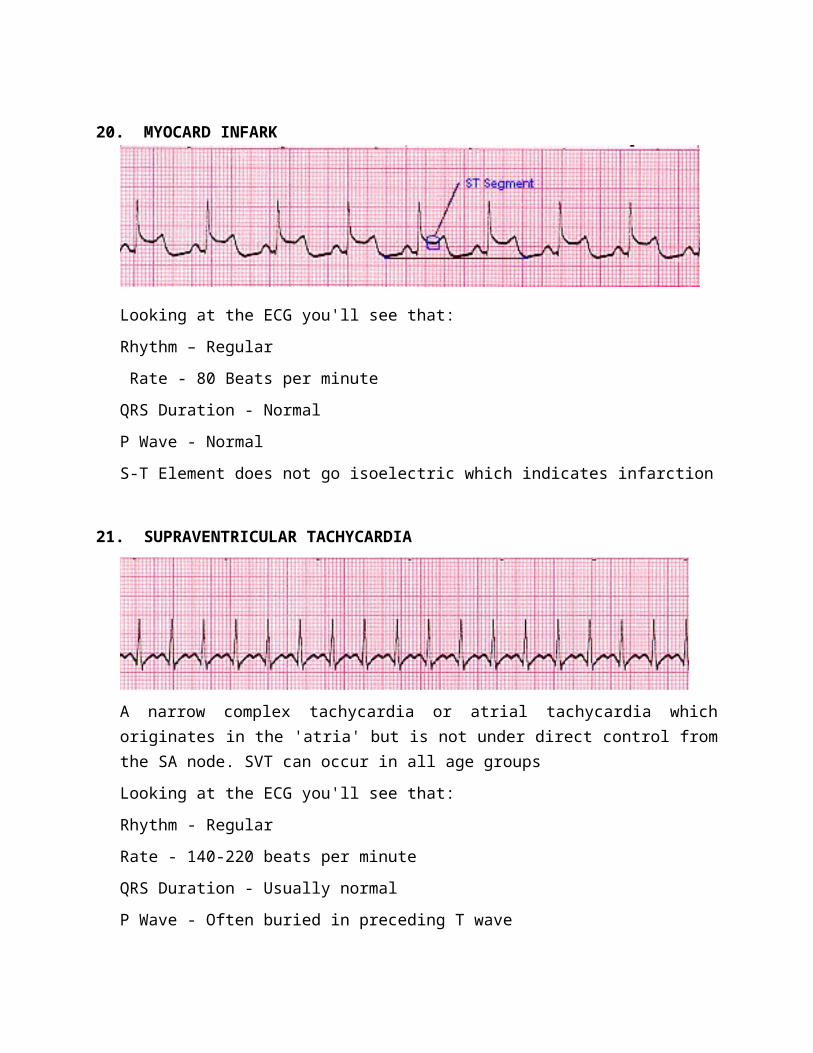
20. MYOCARD INFARK
Looking at the ECG you'll see that:
Rhythm – Regular
Rate - 80 Beats per minute
QRS Duration - Normal
P Wave - Normal
S-T Element does not go isoelectric which indicates infarction
21. SUPRAVENTRICULAR TACHYCARDIA
A narrow complex tachycardia or atrial tachycardia which originates in the 'atria' but is not under direct control from the SA node. SVT can occur in all age groups
Looking at the ECG you'll see that:
Rhythm - Regular
Rate - 140-220 beats per minute
QRS Duration - Usually normal
P Wave - Often buried in preceding T wave
P-R Interval - Depends on site of supraventricular pacemaker Impulses stimulating the heart are not being generated by the sinus node, but instead are coming from a collection of tissue around and involving the atrioventricular (AV) node
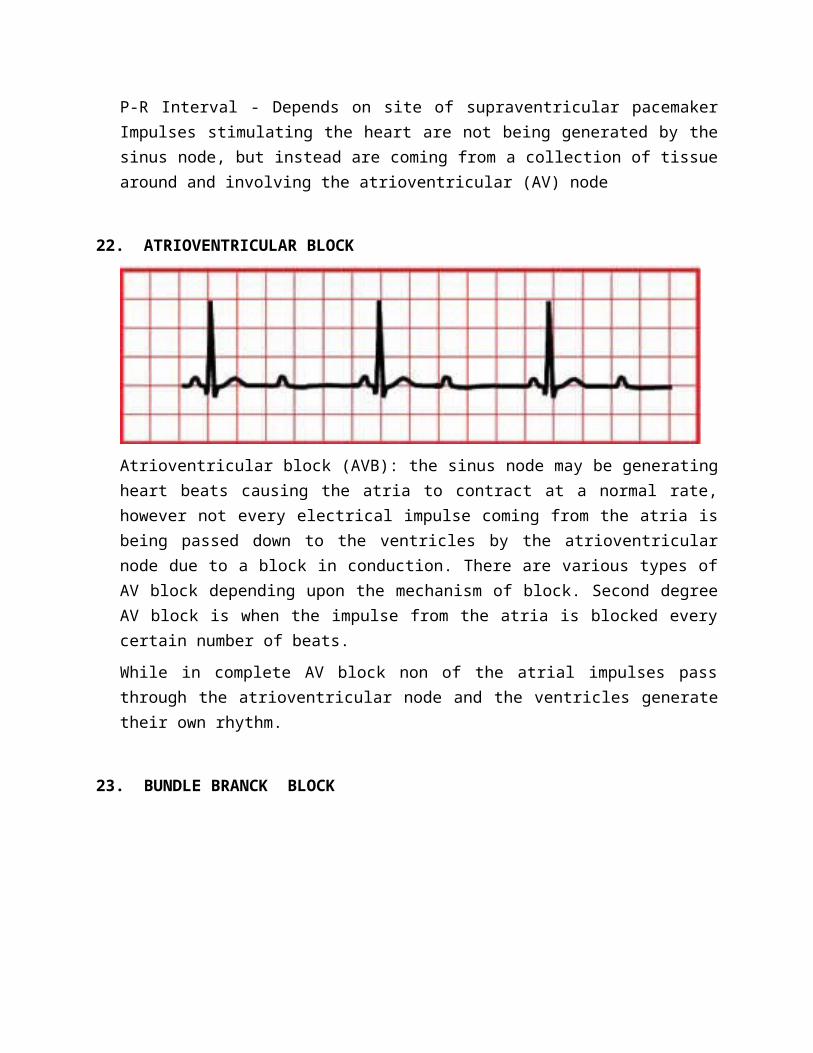
22. ATRIOVENTRICULAR BLOCK
Atrioventricular block (AVB): the sinus node may be generating heart beats causing the atria to contract at a normal rate, however not every electrical impulse coming from the atria is being passed down to the ventricles by the atrioventricular node due to a block in conduction. There are various types of AV block depending upon the mechanism of block. Second degree AV block is when the impulse from the atria is blocked every certain number of beats.
While in complete AV block non of the atrial impulses pass through the atrioventricular node and the ventricles generate their own rhythm.
23. BUNDLE BRANCK BLOCK
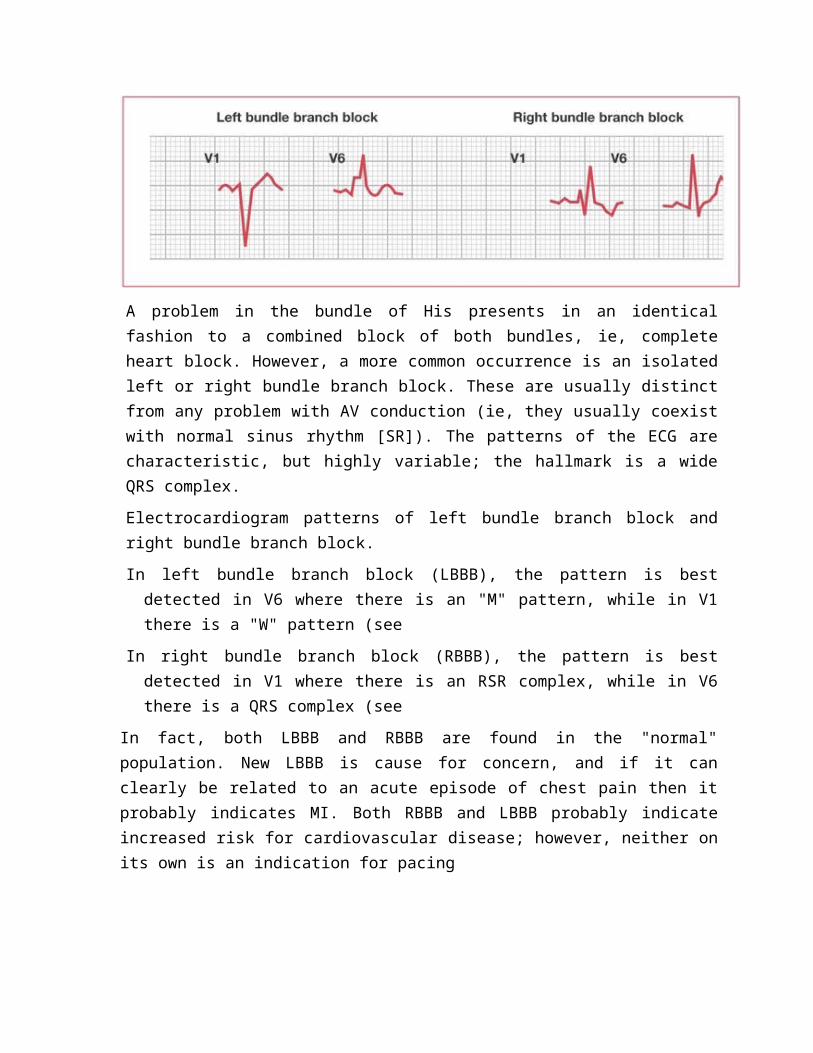
A problem in the bundle of His presents in an identical fashion to a combined block of both bundles, ie, complete heart block. However, a more common occurrence is an isolated left or right bundle branch block. These are usually distinct from any problem with AV conduction (ie, they usually coexist with normal sinus rhythm [SR]). The patterns of the ECG are characteristic, but highly variable; the hallmark is a wide QRS complex.
Electrocardiogram patterns of left bundle branch block and right bundle branch block.
In left bundle branch block (LBBB), the pattern is best detected in V6 where there is an "M" pattern, while in V1 there is a "W" pattern (see
In right bundle branch block (RBBB), the pattern is best detected in V1 where there is an RSR complex, while in V6 there is a QRS complex (see
In fact, both LBBB and RBBB are found in the "normal" population. New LBBB is cause for concern, and if it can clearly be related to an acute episode of chest pain then it probably indicates MI. Both RBBB and LBBB probably indicate increased risk for cardiovascular disease; however, neither on its own is an indication for pacing
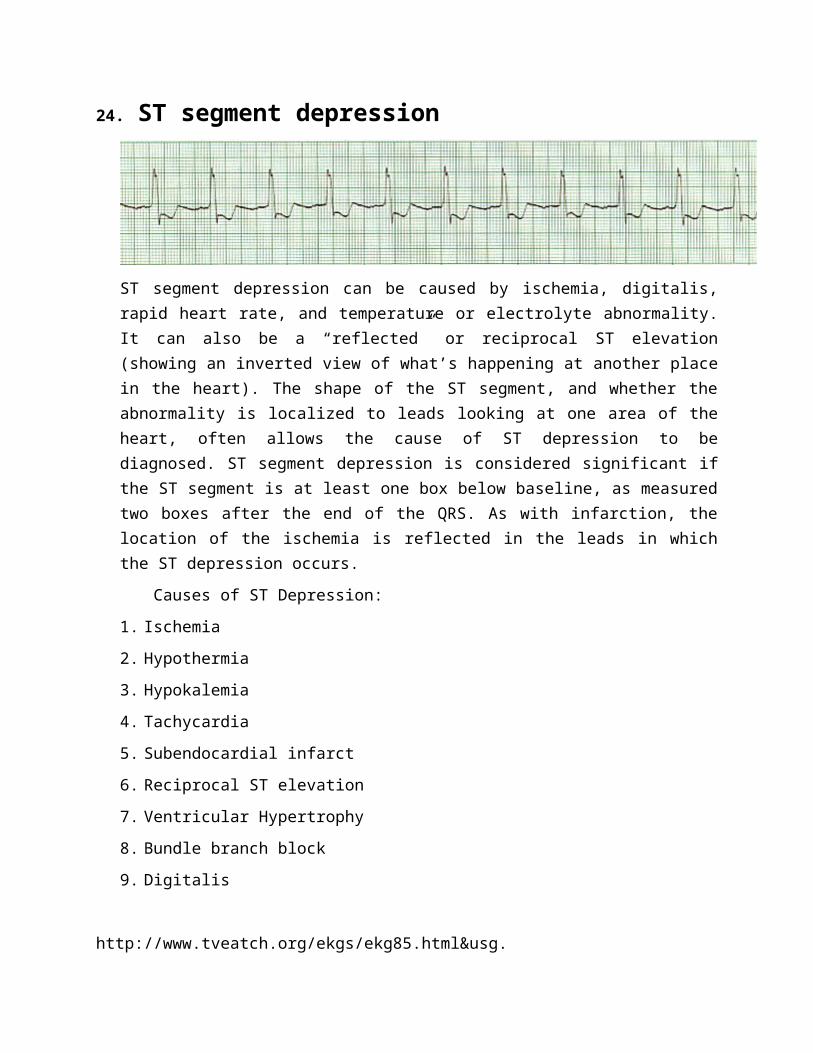
24. ST segment depression
ST segment depression can be caused by ischemia, digitalis, rapid heart rate, and temperature or electrolyte abnormality. It can also be a “reflected” or reciprocal ST elevation (showing an inverted view of what’s happening at another place in the heart). The shape of the ST segment, and whether the abnormality is localized to leads looking at one area of the heart, often allows the cause of ST depression to be diagnosed. ST segment depression is considered significant if the ST segment is at least one box below baseline, as measured two boxes after the end of the QRS. As with infarction, the location of the ischemia is reflected in the leads in which the ST depression occurs.
Causes of ST Depression:
1. Ischemia
2. Hypothermia
3. Hypokalemia
4. Tachycardia
5. Subendocardial infarct
6. Reciprocal ST elevation
7. Ventricular Hypertrophy
8. Bundle branch block
9. Digitalis
http://www.tveatch.org/ekgs/ekg85.html&usg.
1. NORMAL SINUS RHYTHM
2. SINUS TACHYCARDIA
3. SINUS BRADICARDIA
4. ATRIAL TACHYCARDIA
5. ATRIAL FIBRILATION
6. ATRIAL FLUTTER
7. JUNCTIONAL RHYTHM
8. VENTRICULAR TACHYCARDIA
9. VENTRICULAR FIBRILATION
10. TORSADE DE POINTES
11. IDIOVENTRICULAR
12. PREMATURE ATRIAL CONTRACTION
13. PREMATURE JUNCTIONAL CONTRACTION
14. PREMATURE VENTRICULAR CONTRACTION
15. AV BLOCK 1ST DEGREE
16. AV BLOCK 2ND DEGREE TYPE 1
17. AV BLOCK 2ND DEGREE TYPE II
18. AV BLOCK 3RD DEGREE
19. ASYSTOLE
20. MYOCARD INFARK
21. SUPRAVENTRICULAR TACHYCARDIA
22. ATRIOVENTRICULAR BLOCK
23. BUNDLE BRANCK BLOCK